
Abstract
Keywords
Traumatic brain injury (TBI) among underserved populations is an increasing global health concern and a silent epidemic with devastating consequences (Webster et al., 2015). The rate of TBI amongst racial and ethnic minorities indicates that Black people sustain moderate to severe TBI at increasingly higher rates Brenner et al., 2012; Bruns & Hauser, 2003; Jager et al., 2000). Amongst underserved populations, Black people living with TBI have unmet and unaddressed needs along the continuum of care (Heinemann et al., 2002) and are more vulnerable to the impacts of occupational deprivation (Lowe, 2015; Mensah, 2010), defined as the prevention of opportunities to participate in meaningful occupation (Whiteford, 2004). The aftermath of TBI has shown to affect occupational participation due to changes in physical, psychosocial, emotional, and cognitive functioning (Draper et al., 2007; Wheeler et al., 2016). This often requires a long, arduous process to recovery and rehabilitation.
The U.S. Center for Disease Control and Prevention (CDC) defines TBI as a “disruption in the normal function of the brain that can be caused by a bump, blow, or jolt to the head or penetrating head injury” (Center for Disease Control and Prevention [CDC)], 2019, What is a TBI? section, para. 1). TBI remains one of the largest contributors to trauma-related deaths and disability around the world, collectively producing substantial social and economic impacts (Dewan et al., 2018; Pinggera et al., 2020). Approximately 43.1% of people who are hospitalized for TBI develop long-term disability (Iaccarino et al., 2018). Reintegration into the community and participation in life and meaningful occupation is the ultimate goal of rehabilitation for persons with TBI. An essential criterion along the care journey for persons with TBI is that pathways provide the tools and resources that lead to participation and engagement in occupation and ultimately live a meaningful life.
Racial and ethnic minorities, especially Black people, are at an increased risk for hospitalization due to TBI and have been reported to use health care services less frequently and experience poorer health outcomes than white people (Gao et al., 2018). Black people have less health coverage, are less likely to be covered through private insurance, more likely to be covered through public health insurance, access care through emergency departments, and lack continuity of care across the care continuum (Kirby & Kaneda, 2010). It is well known that TBI can result from several mechanisms, including motor vehicle collisions, sports injuries, work-related trauma, falls, being struck by an object or person (Faul & Coronado, 2015). The intersection of TBI and violence has been gaining more attention over the years (Colantonio et al., 2014; Kim & Colantonio, 2008). TBI resulting from violence is associated with poorer health outcomes (Kim et al., 2013; Shafi et al., 2019). One population vulnerable to the intersections of violence, TBI, and poorer health and rehabilitation outcomes is Black people living with a TBI (Banksm & Ackerman, 2002; Linton & Kim, 2014).
Previous reviews of the literature have highlighted racial and ethnic disparities in care and rehabilitation outcomes (Gary et al., 2009) and the use of rehabilitation support services (Gao et al., 2018). In these reviews, racial and ethnic disparities were described to be related to insurance coverage (Gao et al., 2018) and likely the result of patient, provider, and institutional factors such as diversity, prejudice, stereotypes, and diversity of health providers and health teams (Gary et al., 2009). One of the challenges and limitations of rehabilitation and care pathways is a one-size-fits-all approach that overlooks intersecting vulnerabilities based on race, racialization, racism, disability, gender, culture, and socioeconomic disparities. To this extent, previous reviews to date have not challenged or explicitly recognized the pervasive nature of structural violence in TBI care. Structural violence demarcates how institutionalized forms of anti-Black racism are enacted in subtle and invisible ways along the care pathway through human practices that determine care outcomes and life experiences which hold material consequences for Black populations Hamed et al., 2020; Wendel et al., 2021).
Being Black and experiencing TBI can lead to inadequate treatment, limited opportunities to engage in occupation, and institutional violence. Although racism and its related intersections such as sex, gender, and disability produce differential outcomes and experiences along the care pathway and continuum, there has not been a review to date investigating or highlighting integrated care under these considerations for Black people experiencing TBI. Effort that attempts to frame the struggle of all underserved populations, including racial minorities, as a single and isolated initiative in addressing health inequities is limited in its analysis and impact. To bridge this gap, this scoping review was undertaken to address the following objectives: (a) to summarize the extent, nature, and range of care pathways that consider Black populations, (b) summarize how Blackness, race, and racism are conceptualized in the literature, (c) determine how Black people come to access care pathways, and (d) identify how care pathways consider the mechanism of injury and implications for human occupation (Omar et al., 2020). Addressing the scope of the literature also involved consideration for how concepts of sex and gender were positioned and applied in the included studies.
Methods
This scoping review was informed by a critical transdisciplinary lens and developed under the methodological guidance of Arksey and O’Malley (2005), later refined by Levac et al. (2010), and further guided by the Joanna Briggs Institute (2015). The Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) checklist was used in the reporting of this review (Tricco et al., 2018).
Identifying the Search Strategy
The search strategy for this review was developed through an iterative process in collaboration with an Information Specialist. The search strategy was guided by the following primary research question: what is the extent, nature, and range of the literature on integrated care for Black people experiencing TBI? The search strategy included the application of text words and subject headings (e.g., MeSH, Emtree) consistent with the following fundamental word categories: traumatic brain injury (TBI), integrated care, and Black populations. To identify relevant peer-reviewed literature, six databases were systematically searched: MEDLINE (In-Process and Other Non-Indexed Citations), EMBASE, Cochrane Central Register of Controlled Trials, Cumulative Index to Nursing and Allied Health Literature (CINAHL), PsycINFO, and Sociological Abstracts. Books or grey literature was not included in this scoping study. These databases were searched up to November 2020 to retrieve articles indexed since September 2019 which resulted in no additional articles. The reference lists of identified literature were hand-searched to identify additional key sources of information that might not have been captured in the search strategy. Limits were placed on the search strategy to restrict studies to published literature from 1980 and onwards, as this is when the term integrated care first appeared in health literacy (Shaw et al., 2011). The searches were also limited to English language publications. No restrictions were applied to the geographical location as one of the goals of this review was to map the scope of the literature. The complete and final search strategy in MEDLINE can be found in Appendix A.
Identifying Relevant Studies
The search yielded a total of 178 articles after removing duplicates. Empirical studies such as reviews were used to check for additional references at the level of full-text review. As a result, 27 articles were selected, after which 16 more were identified from the reference lists of the 27 papers. A total of 43 articles met the inclusion criteria. A full description of the search results including excluded and included articles is described in the PRISMA diagram and shown in Figure 1. Preferred reporting items for systematic reviews and meta-analyses (PRISMA) diagram of the search results.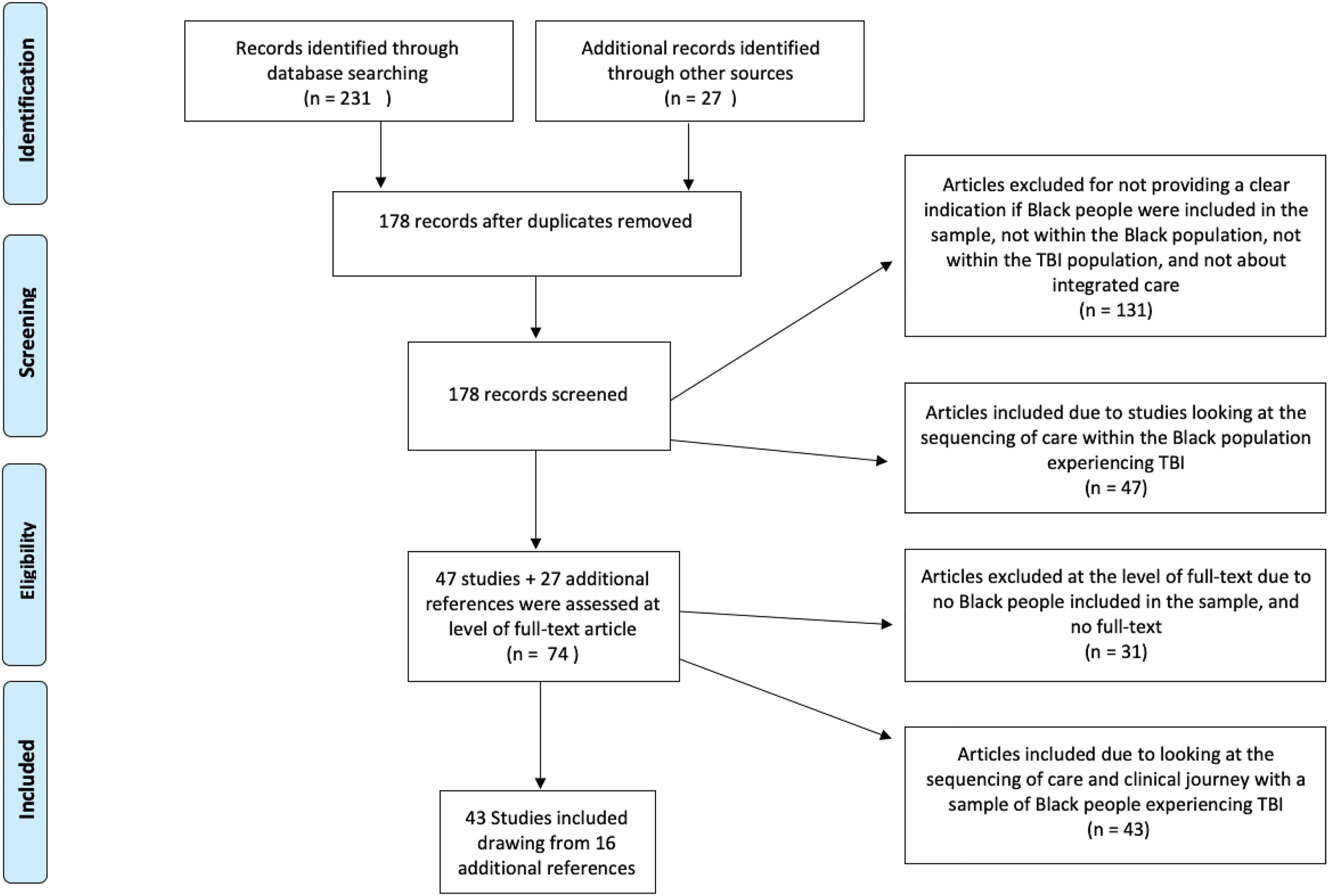
Study Selection
All texts included a description of an integrated care pathway or integrated care, which may be a plan, model, protocol, or intervention that maps onto the pre-identified definition. Campbell et al. (1998) define integrated care pathways as “the tasks to be carried out together with the timing and sequence of these tasks and the discipline” (p.133) for a specific clinical condition across all service delivery settings (e.g., community-based care, community-based agencies, community-based organizations, acute/subacute care institutions, and rehabilitation hospitals). The integrated care pathway must have been described within the context of persons with a primary diagnosis of TBI of any severity level, including Black persons in the sample or as part of the text for non-empirical articles or any of the words race, racism, racialization, and Blackness. Lastly, all texts were published in English and peer-reviewed.
Two independent reviewers screened a sample of 20 abstracts against the criteria to compare and discuss any discrepancies in understanding the criteria and definitions and to increase consistency. The inter-related reliability was over 80% between both reviewers using the kappa statistic at the title and abstract screening and full-text review of articles during pilot testing. Subsequently, the two reviewers independently reviewed the first level of title and abstracts against the inclusion and exclusion criteria. All articles that met the criteria above were included for the second level of full-text review against the predetermined inclusion criteria. In this second level, two independent reviewers independently reviewed and discussed the rationale for the inclusion and exclusion of articles at the level of full-text. A third reviewer was consulted to reach a consensus where differences or discrepancies arose after discussion between any of the two reviewers. This was a global search where are all identified literature were from the United States.
Data Charting
Data chart of included studies.

Data Analysis and Synthesis
A narrative synthesis was conducted to further distill the breadth of the literature on care pathways for Black people experiencing TBI. Narrative synthesis is a form of analysis that uses text and words primarily to compile and summarize the findings of the synthesis (Popay et al., 2006). This form of synthesis uses a textual approach to tell a story from the collective findings of the studies in the review (Popay et al., 2006). Narrative synthesis is particularly useful when a broad range of objectives and research questions are being explored in a systematic review of the literature (Popay et al., 2006).
Results
Extent of the Literature
Forty-three studies met the eligibility criteria and were included in this review. Table 1 presents characteristics of the included studies.
Geographical location and publication years
All of the 43 studies included in this review were based in the United States. The earliest publication capturing care pathways for Black people experiencing TBI dated back to the year 1984. This article was a population-based comparative study on head trauma in two communities in Chicago that differed on the basis of socioeconomic status and race (Whitman et al., 1984). This was the only study that provided analysis that is contingent on the geographical location of interest.
Study design and population characteristics
Over 90% of the articles (n = 41) were quantitative in nature. The majority of these studies drew from databases across the nation with many stemming from the TBI Model Systems (TBIMS) program. Burnett et al. (2000) expressed that the majority of the TBIMS programs were based near urban centers. The two qualitative studies used focus groups and interviews to understand the service needs of persons with TBI (Leith et al., 2004) and factors that contribute to the use of standard clinical procedures (Melnick et al., 2015).
Eighty-four percent of the studies described severity of TBI in the sample, including mild TBI (n = 4) and moderate (n = 1). Most studies included a range of mild to severe (n = 18) TBI. Fourteen studies focused only on moderate and severe TBI. Six studies (16%) did not specify or report on the severity of TBI in the sample. Adults made up the most common sample of participants included in the studies (n = 29, 67%), with nine studies also including the pediatric population. Seven studies (16%) sampled from the pediatric population only, four studies included older adults in the sample, and two studies were unclear. One study included a mix of children, adolescents, adults, and older adults. In more than 70% of the studies, white participants accounted for greater than 70% of the sample. Three studies were found where Black people made up over 87% of the sample. One study had a sample that was 51% Black people (Hart et al., 2005). In one study, Black people represented one percent of the sample (Kane et al., 2014).
Range of the Literature
Title of articles and focus of the care pathway
Sixty percent (n = 26) of the articles made direct reference to race and ethnicity in the title. Three studies identified the inclusion of Black participants in the title of the article. Twenty-one (81%) of the article titles explicitly highlighted racial and ethnic disparities across TBI-related outcomes such as community integration, medical disposition, and differential care and treatment.
The most common focus of care pathways for Black people experiencing TBI was on racial and ethnic disparities in care, screening, access, treatment, and disposition. However, none of these studies identified the source of existing disparities. For instance, in “Black children experience worse clinical and functional outcomes after traumatic brain injury: An analysis of the National Pediatric Trauma Registry” p. 1259), Haider et al. (2007) documented disparities in trauma care and related outcomes for persons experiencing TBI and described Black children as the population who underperformed and faced the worse outcomes using a national trauma database.
Settings of the care pathway and providers
Included studies were conducted with samples within emergency departments (n = 11), hospitals (n = 7), and post-hospitalization care such as acute inpatient rehabilitation (n = 18), outpatient rehabilitation (n = 2), community settings (n = 10), vocational rehabilitation (n = 1), and a skilled nursing facility (n = 1). Two studies were located within clinical care settings for veterans. The majority of the included literature in this review did not report which designated or non-designated providers were involved in the clinical care journey for Black people experiencing TBI.
Locating Institutional Racism as Institutionalized Inclusion: Framings of Race, Sex, Gender, and Blackness in the Literature
Terms used to describe race and the sample of Black people in the studies
Twelve studies used the term race in the methodology of the paper. Thirty-three percent (n = 14) of the studies used the terms race and ethnicity interchangeably. Others used ethnicity (n = 4) and minority (n = 7) in the place of race where minority accounted for all the racial categories that were considered to be non-white. Only two studies explicitly defined race as a socially constructed phenomenon (Howard et al., 2005; Yeates et al., 2002).
All the studies in this review homogenized Black people under the one category of “Black” or African American. A total of 33% (n = 14) of the included articles described the sample of Black people in the study as being Black and over 55% (n = 25) of the studies described their sample as African American. Four studies used the term non-Hispanic Black. Seven studies methodologically grouped Black people under the category of minority to compare differences between Black and white people making it more difficult to determine outcomes among Black participants. Two studies explicitly controlled for race and ethnicity in the analysis (Pappadis et al., 2012; Sander et al., 2012). In earlier studies, the term race is used where ethnicity shows up in the early 2000s, becomes more popular over time, and is used interchangeably. The term Black is used to designate Black people. It is not until the early 2000s where African American and other indicators of ethnicity are used to describe populations of Black people. In 2011, the designation of non-Hispanic Black began to show up in the literature. In every study, white participants were the reference group. Lastly, one study stated that participants in the study were matched for race (Couch & Stewart, 2016).
In over 80% (n = 35) of the studies, race was routinely used as an independent variable for understanding the differences in outcomes, treatment, discharge destinations, and mortality in the literature on integrated care for persons with TBI. For instance, Yeates et al. (2002) articulated race as a moderator and stated that “race consistently moderated outcomes independent from SES [socioeconomic status]” (p. 400). Similarly, Selassie et al. (2004) stated race and gender have independent effects that influence and account for hospital admission.
Language used to engage with sex and gender in the studies
A total of 49% (n = 21) of the studies used the term sex, 44% (n = 19) used gender, and two studies did not report on either sex- or gender-specific data in their papers. Three studies used the terms sex and gender interchangeably (Arango-Lasprilla et al., 2009; Arango-Lasprilla et al., 2007; Dams-O’Connor et al., 2017). Over 40% (n = 18) of the studies used sex to refer to males and females. Over 40% of the studies misapplied the term gender to refer to dichotomous sex differences, such as male and female. Only one study used the correct pairing of gender with the terms man and woman (Bazarian et al., 2003). All of the included studies in this review viewed sex or gender as a dichotomous construct despite the existence of multiple gender identities.
Most studies did not report stratified data on the basis of gender and/or race. Four studies disaggregated the data to create more than one group to represent the participants in the sample. Many of these studies displayed the data in two groups typically representing whites and minorities, respectively, and one study only provided data for the white participants (Yeates et al., 2002). A total of seven studies reported data for Black participants.
Considering intersections of race, sex, and gender
Ten studies (23%) provided an analysis on the intersections of race and sex or gender, particularly towards Black people. For instance, it is unveiled that Black females received less standard treatment procedures (Selassie et al., 2004). Studies that articulated analysis for race and gender often stated that Black males with TBI were typically older than the average clinical population (Gary et al., 2009; Hanks et al., 2003) and represented the majority of the sample (Hart et al., 2005; Kennepohl et al., 2004). Sander et al. (2009) articulated that Black men scored lower on social integration than Black women, who often take on home roles that require them to do meal preparation and homework.
Conceptualizations of Blackness
Blackness and the care pathway are portrayed in several ways, including the mechanism of injury, education, and productivity. For instance, six studies emphasized that Black people had an increased risk of obtaining a TBI through violent mechanisms such as assault. Hank et al. (2003) examined the occurrence and characteristics of persons with violent-related TBI and reported that single, African American males who were unemployed pre-injury and with a history of TBI were at greater risk. Intentionality is associated with what is understood to be violent mechanisms of injury. In particular, two studies explicitly report that African Americans were more likely to be injured intentionally (Haider et al., 2007; Hart et al., 2005). Further, Haider et al. (2007) reported that 50% of Black trauma patients with penetrating injuries were classified as intentional. Moreover, Whitman et al. (1984) described interpersonal violence such as gunshot wounds, as one of the leading causes of injury for Black people in inner-city Chicago.
Black people were described as unproductive compared to white people (Sherer et al., 2003) and less integrated into the community (Sander et al., 2009). Black people were labeled to display less independence in productivity (Sander et al., 2009). Race and productivity were linked by Sherer et al. (2003) who articulated that “race is significantly associated with productivity outcomes” (p. 415) where African Americans were twice as likely to be unproductive at follow-up than white people. Gary et al. (2009) reported that Black people were at increased odds for not being competitively employed and had worse employment outcomes.
Five studies explicitly articulated the socioeconomic status of Black people with particular emphasis on marital status and education (Burnett et al., 2000; Gary et al., 2009; Hart et al., 2005, 2007; Sherer et al., 2003). Burnett et al. (2000) articulate that African Americans with TBI were high school educated, expelled, dropped out before graduation, labeled as special needs, and failed a grade at some point during their school education. Additionally, Burnett et al. (2000) provide more details about Black people in the study regarding substance abuse, previous encounters with the police, and resulting arrests. However, Burnett et al. (2000) did not justify the reasoning behind providing those details about Black people.
Gary et al. (2009) caution rehabilitation professionals to direct greater attention towards the unique needs of Black people. Gary et al. (2009) describe Black males as more likely to have lower levels of competitive employment pre-injury, less than high school education, unmarried, and lower Glasgow Coma Scale measures. In Haider et al. (2007), Black children were labeled as an at-risk population for poor outcomes post-TBI and were more prone to injuries that produce worse clinical outcomes than white children. Johnstone et al. (2003) reported that Black people were at increased odds of being in the groups that scored low on the Functional Independence Measure (FIM). The authors further articulated that Black people were typically younger than 45 years of age, received support through Medicaid, lived in Atlanta and San Francisco, and experienced comorbidity. Rumalla et al. (2018) reported that the racial category of Black was an independent risk factor for post-traumatic amnesia. Additionally, Dams-O’Connor et al. (2017) provided an illustrative hypothetical case example of how demographics and injury characteristics served as a risk factor for rehospitalization. The authors articulated that being a “Black female, aged 70 years, unemployed pre-injury, received insurance coverage through Medicaid and Medicare were at increased risk” (p. 7). However, there were no indicators as to why this example was chosen as the authors stated that the provided example was one of many to choose from.
Anti-Black racism displayed as symptoms of an unnamed problem
Differential clinical outcomes between racial groups were sometimes suggested to be shaped by the biological inferiority of Black people and other people of color and symptoms of anti-Black racism. For instance, Rumalla et al. (2018) suggested that Black people had worse TBI-related outcomes due to predisposing factors such as socioeconomic deprivation, differential treatment, unequal access to care, and notably, genetic variations. Haider et al. (2007) questioned if the reason why Black children produced worse functional outcomes was due to a “race associated disadvantage” (p. 1261). In another study, Bell et al. (2011) suggested that racial differences between Black people, other minorities, and white people in the sample may have accounted for why the phone intervention was unsuccessful: “we reasoned that perhaps the current study showed negative findings because of the much larger proportion of nonwhite participants” (p. 1558).
In other instances, health disparities for Black people are described as the result of systemic inequalities and differential access to treatment and rehabilitation. For instance, Howrey et al. (2017) reported that Black people were more likely to have poorer functional trajectory due to disparities resulting from differential access to care and quality of care across the care continuum. Howrey et al. (2017) suspected that Black people received rehabilitation of lower quality than white people, and this is also reported in Selassie et al. (2004) and Sherer et al. (2003). Even more, Howard et al. (2005) explicitly articulated that prejudiced beliefs against Black people may account for differential outcomes that result in the observable differences that are noticed. Shafi et al. (2007) expressed that differential access to care and rehabilitation may be the result of systemic inequalities that are faced by Black people including those that are perpetuated through geographical location (Piatt & Neff, 2012; Shafi et al., 2007).
Bazarian et al. (2003) stated that African Americans were three times more likely to receive care from a resident physician than a white doctor. Bazarian et al. (2003) further described that this disparity could be the result of a number of factors including the white resident feeling more comfortable and less likely to be scrutinized by a Black patient, intentionally selecting the charts of Black patients as they were perceived to be easier and require less attention thereby limiting white physicians from having contact with Black patients. Furthermore, in some papers, authors attributed lack of employment and productivity levels to the job market (Sherer et al., 2003), exclusive opportunities for employment, and the impact of racial prejudice that limits the potential for Black people (Gary et al., 2009; Sander et al., 2009). Haider et al. (2007) speculated that the top cause of disparities for Black people was bias in the health-care system. Additionally, Shafi et al. (2007) articulated that health disparities could be shaped by geographical location and religious beliefs. Moreover, in all of the examples, the authors described instances of racial discrimination towards Black people that is typically described as anti-Black racism. However, none of the studies explicitly named racism.
Nature of the Literature on Anti-Black Racism in TBI Care Pathways: Narrative Findings
A narrative analysis led to four themes encompassing the nature of anti-Black racism in the literature on care pathways for studies that include Black people experiencing TBI, including how care pathways are accessed, how they account for the mechanism of injury and the implications for occupation. These four themes are defined as the following: accessing clinical care pathways; mechanism of injury and other factors contributing to the clinical care journey for Black people; functional outcomes of anti-Black racism in the clinical care pathway; and long-term occupational impacts of the clinical care pathway. Below we present the narrative findings.
Accessing clinical care pathways
Arbogast et al. (2016) described where youth with concussion seek care as their initial point of contact in the children hospital of Philadelphia network which serves a socioeconomically, racially, and ethnically diverse population and insurance coverage that goes beyond primary care clinicians to also specialty services. Seventy-one percent (n = 5729) of the study sample were identified as being white whereas 17.1% (n = 1383) were Black children. As such, 42.4% of Black children sought care for their concussion in emergency departments compared to 5% of white patients many of which who sought care from primary care clinicians. Arbogast et al. (2016) stated that greater efforts are required to educate primary care clinicians as that is where most people go to seek care. McCarthy et al. (2002) reported that race influenced hospital admission even after controlling for other factors such as gender, income, and insurance coverage. Participants were categorized as white, African American, or other. Non-white children such as African American children were 20% less likely to be admitted to hospital than white children (McCarthy et al., 2002). Black patients who presented themselves to the hospital were reported to have received lower rates of major procedures than all other racial groups in the study sample (Piatt & Neff, 2012).
Shafi et al. (2007) examined potential disparities and differential access to diagnostic assessments and treatment at inner-city hospitals that are poorly funded and did not find any ethnic disparities in the assessment and management of patients who present themselves to a trauma center. However, despite lack of any ethnic disparities in the management, authors suggested looking at the quality of care that is received at the level of inpatient and the type of procedures including where patients go after discharge from acute care facilities. For example, Melnick et al. (2015) conducted a qualitative study exploring what non-clinical human factors encourage or discourage the appropriate use of CT scans for patients that present themselves to the emergency department for mild head injury and reported themes such as establishing trust, patient expectations, and influence of others. While the study authors expressed that the study sample contained a representative make-up of the patient population and emergency department physicians, the results were displayed according to patients and providers with little indication for their intersections such as race and what information may lay bare as a result. Under those circumstances, African Americans were more likely than white patients to receive emergency department care from a resident than a staff physician, technician specialist, or another type of designated provider even after controlling for other potential confounding variables (Bazarian et al., 2003). Consequently, racial disparities in emergency department care resulted in lack of follow-up after discharge from emergency department that is faced by African American patients experiencing TBI (Bazarian et al., 2003) and lack of access to trauma care (Bowman et al., 2007).
Racial and ethnic disparities persist in access to rehabilitation discharge from trauma care. Shafi et al. (2007) reported that ethnic minorities (60% African American) were less likely to be placed in acute rehabilitation after being discharged from trauma centers which is a finding that remained consistent after controlling for other variables such as the uniqueness of their injury, severity level, and status of insurance coverage. Black patients are more likely to receive less intensive and high-level rehabilitation regardless of insurance coverage compared to white patients who were matched on other variables such as age, sex, insurance, mechanism of injury, and injury severity. Black patients were more likely to be discharged home compared to white patients (Meagher et al., 2015). One study concluded that there were no racial and ethnic disparities in medical disposition in emergency department care regardless of severity such as being admitted to the intensive care unit, routine care, and hospital admission versus discharge. This study sample consisted of 49% African American. For the purposes of explaining these findings, study authors expressed that the study sample is a training site for residents from a collaborating historically Black college comprised of health providers who were experienced with serving racial and ethnically diverse patients which represented a large number of the patients (Howard et al., 2005).
Selassie et al. (2004) examined the effects of race, gender, and insurance coverage in post-hospitalization care for individuals that presented themselves to an emergency department at a non-federal hospital in South Carolina. In this study, Black patients made up a total of 33% of the sample of persons with TBI, 41% of those who were not covered by insurance, and 63% of those who were covered by Medicaid, which is a state federal program to help cover the cost of care for those with limited income and resources. Black females were 21% less likely to be hospitalized compared with white females even after controlling for other covariates including insurance status (Selassie et al., 2004). In one study, African Americans who were privately insured were less likely to be placed in rehabilitation compared to white patients (de la Plata et al., 2007). Although African Americans were less likely to have private insurance, those with federally funded insurance coverage were provided with rehabilitation at higher rates than white patients (de la Plata et al., 2007). Similarly, Kane et al. (2014) examined disparities in discharge destination in patients according to race/ethnicity and type of insurance coverage. African Americans made up 1% (N = 76) of the study population (N = 6061). Only 17% of Black patients were discharged to post-hospitalization care. However, insurance coverage was not stratified by race.
Mechanism of injury and other factors contributing to the clinical care journey for Black people
In Hank et al. (2003), African Americans made up 86% of the sample of minority participants who were 3.1 times more likely to sustain a violent-related TBI than persons who were white. Being a single African American male was reported to be a risk factor for violence-related TBI. Similarly, minority participants were 77% Black and were more likely to receive a TBI through violent mechanisms (Arango-Lasprilla et al., 2007). In Howard et al. (2005), Black participants made up 49% of the study sample. While grouped under the category of minority patients, they were more likely to have sustained their TBI by being hit by a car while walking. When the mechanism of injury for Black people is considered according to geographical location, Black males and females living in the inner city of Chicago were more likely to sustain a head injury at 30 years of age (Whitman et al., 1984). Vehicle accidents were the leading cause of head injury for Black children living in a suburban area, and the second leading cause was interpersonal assaults (Whitman et al., 1984). In contrast, it was falls and recreational injuries for white children (Whitman et al., 1984). However, interpersonal attacks were the leading cause of head injury for Black people living in the inner-city community (Whitman et al., 1984). One study reported that being African American was seen as an independent risk factor for post-traumatic seizures in children with TBI (Rumalla et al., 2018). Another study reported that being an older Black Hispanic female was a risk factor for rehospitalization for moderate to severe TBI 1–10 years post-injury (Dams-O’Connor et al., 2017).
Functional outcomes of anti-Black racism in the clinical care pathway
The aftermath of rehabilitation varied for Black participants experiencing TBI, with most studies reporting poorer outcomes. For instance, Haider et al. (2007) noted that Black children, while more likely to be referred to inpatient rehabilitation were at an increased odds of having a functional deficit in locomotion, expression, and feeding at the time being discharged without any worsening injuries of the extremity. Howrey et al. (2017) reported that Black patients in the study were more likely to have poorer functional outcomes in cognition and motor functioning even at admission to rehabilitation. African Americans spent nearly three times more as unemployed than white participants (Johnstone et al., 2003). Johnstone et al. (2003) found no significant differences in vocational outcomes but that African Americans using these services would benefit from vocational rehabilitation consistent with their natural environments. However, African Americans were reported to experience difficulty accessing vocational rehabilitation services and waited for an average of 11.4 years post-TBI (Johnstone et al., 2003). Similarly, Burnett et al. (2000) examined functional outcomes and reported no differences between minorities and non-minorities regarding disability rating scales and functional independence measures. However, a total of 94.3% of the study participants were African American (Burnett et al., 2000).
Warren et al. (2016) explored the occurrences of psychological distress in families of persons experiencing TBI and reported that 39% of family remembers indicated positive for depressive symptoms and 24.3% for post-traumatic stress and exhibited higher levels at three-month follow-up. Above all, the findings were not stratified according to the different study participants, making it increasingly challenging to determine Black family members' outcomes. Kennepohl et al. (2004) reported that lack of acculturation and cultural factors impact outcomes on neuropsychological assessments for African Americans experiencing TBI.
Long-term occupational impacts of anti-Black racism in the clinical care journey
Black persons experienced poorer outcomes in functional independence, recovery, and community integration at the one-year follow-up mark (Rosenthal et al., 1996). African Americans were reported to experience lower scores on community integration, such as home integration and productivity, a decline in income, and unemployment (Sander et al., 2009). Similarly, Gary et al. (2009) reported that Black people experienced unfavorable employment outcomes at one, two, and five years post-TBI. At one year follow-up, minorities had lower community integration scores, particularly in productivity and social integration. The authors reported that a likely explanation might be since minorities were single and living alone, and 46% were not employed before the TBI. Black participants experienced lower social integration (Pappadis et al., 2012). At one-year post-injury, African Americans experienced significantly lower social integration levels such as engaging in leisure activities, having a best friend, and were more likely to participate alone (Hart et al., 2005). In fact, 35% reported never hanging out with friends and were dissatisfied with life (Hart et al., 2005). African Americans were three times more likely to be unproductive, which was impacted by the etiology of TBI and pre-injury productivity (Sherer et al., 2003). At the time of their TBI, participants in the violent etiology group, consisting of 37% African Americans, were less likely to be employed competitively and experienced poorer community integration outcomes (Schoop et al., 2006).
While Dahlberg et al. (2006) examined social and communication skills for persons with TBI, the findings were not stratified, making it challenging to unveil Black participants' outcomes. Leith et al. (2004) collected information about race in the demographic characteristics and explored the service needs and experiences of persons experiencing TBI and their families. Similarly, the results were not stratified or interpreted using an intersectional approach that considers the unique perspectives of both Black and white participants. Race was applied as a demographic variable.
Discussion
One of the central findings of this review, as demonstrated by the limited literature available, is that care pathways are non-integrated, inequitable, and limited for Black people living with TBI. The patient care pathway is not a guaranteed predefined standard protocol or written process. Rather, it is the actual unplanned journey of a Black patient seeking health care and rehabilitation services to address their TBI and other related health concerns. A significant finding in this review is the application of race as a biological construct in this literature on integrated care pathways which consider Black people in the sample. Race-based data is not disclosed or collected in many health systems around the world which can be seen in the limited literature included in this review that all originate from studies based in the United States. This is the first systematic scoping review to apply a critical lens to identify and challenge how Black people are displayed in the literature on care pathways for persons with TBI and what becomes visible about how human occupation is supported across the life trajectory. There is a lack of research on integrated care and TBI that considers Black populations outside of the United States, which is a significant gap in the literature. By considering the breadth of the literature by way of non-exclusionary geographical limitations, this review provides a comprehensive scope of the literature displaying that racism remains unchallenged.
Considerations for Naming and Addressing Anti-Blackness
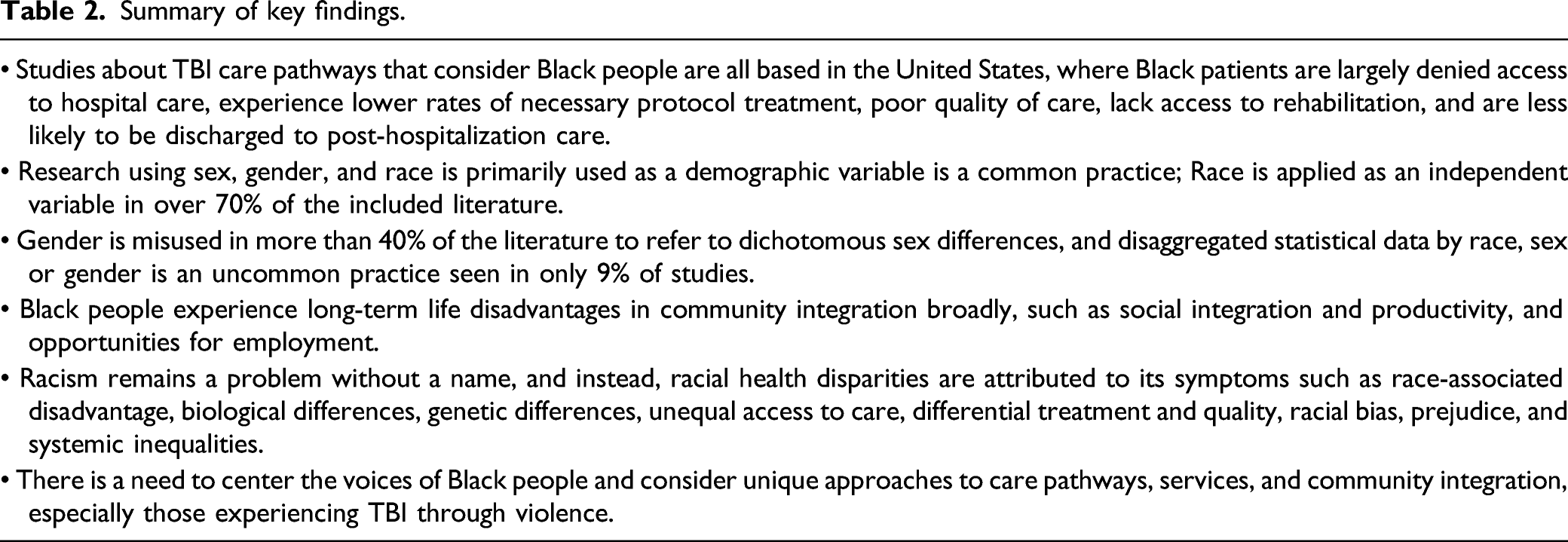
Summary of key findings.
This review highlights the overpopulation of research spotlighting racial and ethnic disparities and the lack of studies exploring solutions to poor treatment, health inequities, access to care, and how to address goals related to participation in occupation, community integration, and other related outcomes. Most concerning is how authors discuss racial health disparities as symptoms of racism without invoking racism. White supremacy and racism are the underlying processes that produce differential outcomes based on racialization, and not solely on race. Authors discuss racial health disparities as being attributed to bias, prejudice, and systemic barriers. For instance, Bazarian et al. (2003) described how racial bias determines care pathways as it limits access to care and rehabilitation for persons with TBI who are Black. As such, anti-Black racism becomes unchallenged, normalized, and understood as symptoms of a problem without a name.
Camara Phyllis Jones (2002) in a seminal piece titled Confronting Institutionalized Racism described the importance of centering racism in public health, naming its existence, understanding how it shapes health and life outcomes, and taking action to dismantle its impacts. Nearly two decades later and the conversation largely remains unchanged. By explicitly acknowledging and naming institutionalized racism in literature about the TBI care pathway, researchers can spotlight how injustice and discrimination have been normalized, institutionalized, and reinforced in research and health systems. The dominant approaches to using racial statistics and addressing racial health disparities function to only legitimate existing practices rooted in anti-Blackness and the perpetuation of dominant narratives where race is not used as a social construct in application and interpretation. The blind misuse of racial statistics where race is used as a biological construct reinforces the status quo. Research on health disparities is a significant vehicle in its reproduction as the root issues are not acknowledged or addressed. Rather, disparities are magnified.
The Dangers of Using and Interpreting Racial Statistics
The National Institute of Health (NIH) has been challenged to reconsider the application of race in science (Yudell et al., 2020). Race-based data is essential for transparency to understand better how practices and policies impact different communities of people. However, race has been misused in research and clinical practice to perpetuate biological differences between categories of humans based on race (Cerdena et al., 2020; Yudell et al., 2020) even by those who are well intentioned. We wish to draw attention to the application of race in TBI research. Zuberi (2001) clearly articulated that the purpose of producing racial statistics should be to help others understand the mechanism of racial stratification, not to legitimize its existence through interpretation. How race is conceptualized and applied in the literature is shaped in part by the research design in quantitative and qualitative studies. Angela James (2008) in her writing critically examines the application of race and how it could be effectively used in research and notes that the study of race can be divided into two categories, “those who study race and racial dynamics, and those who routinely use the concept of race in their studies” (p. 42). Applying race as a social construct entail examining race as a social process with material consequences. James (2008) expresses that “explicit arguments about the presumed biological or genetic basis of race are not normally articulated” (p. 43). In over 90% of the quantitative research in this review, it is unclear if race is used as a social construct, which may reinforce the assumption that race is equated to biological differences.
Research questions or hypotheses are meant to be educated guesses about the outcome based on the relationship between different interest variables. The relationship between variables is often underpinned by particular theories or frameworks that acknowledge how these variables operate in society, which validates the findings. Research about TBI and the clinical care journey, including rehabilitation outcomes and community integration, includes race in ways that are not underpinned and explained through theories of racism, racialization, disability, and related intersections suggesting that resulting interpretations are incomplete, unsubstantiated, and holding exclusionary benefits. There is a significant gap in the theorization of institutional racism in TBI rehabilitation and the care continuum. In these studies, 70% of the time, race is either applied as an independent, moderating, control, or demographic variable in functional outcomes, treatment along the care continuum, access to rehabilitation and discharge destinations, mortality, and mechanism of injury. Using race as an independent, moderating, control, or demographic variable has particular implications as it may erase how racism shapes access, treatment, experiences, outcomes, and long-term opportunities for Black patients with TBI. Studying race as a variable independent of these structures dismisses the very same structures that hold racial hierarchies and reproduce harmful impacts (Zubari & Bonilla-Silva, 2008). For best practices, an important step is to raise the question of what purpose race and ethnicity-based data serves. The collection of race-based data must be completed in a meaningful way that asks about racism and brings light to the consequences of institutional policies and practices beyond identifying racial health disparities, differential health outcomes, and naming racism as a potential contributing factor.
Within this literature, racism becomes institutionalized through inclusion such as differential access to power and voice. Ninety-five percent of the articles included in the review were quantitative, and 65 percent of the studies largely recruited participants from national and local databases. It is unclear if informed consent is provided as a part the inclusion criteria for some of these databases and if individuals are aware of how their data will be used, interpreted, and disseminated in future research outputs. Within this context, Black people enter health service-related research primarily based on studies in which it is unclear if informed consent was provided. More specifically, there is a question about whether Black people were informed about the exact purpose of the research and whether they were aware of how their data will be analyzed and interpreted.
The collection of race-based data is the first step as this information is important for practice and policy changes. However, collecting data on race alone will not provide solutions to the aftermaths of institutional racism. Addressing root causes of inequities such as racism at all levels of functioning including interpersonal, personal, and institutional is a significant consideration in TBI research about the care continuum. For example, statistical data can be used to measure perceived racism, racial discrimination, and unconscious bias instead of reinforcing racial disparities. Different techniques and strategies have been reported on how to capture and measure institutional racism at the perceived, individual, intra-organizational, and extra-organizational level (Adkins-Jackson et al., 2021; Groos et al., 2018).
Additionally, institutional racism is also ingrained in how data is collected. The included literature displayed aggregated data as a common practice whereby study authors lump Black people under broad categories of minority, socioeconomic status, and sex or gender-specific stratification. Aggregated data is an example of how institutional racism is practiced and normalized. One of the components of this theoretical approach is intersectionality which refers to how multiple interlocking forms of social categories such as race, gender, class, and socioeconomic status including income, education, and occupation intersect with one another through racialized hierarchies, power, and systems of discrimination, thereby creating differential forms of oppression for different people (Crenshaw, 1989). This intersectionality of social categories magnifies health disparities and provides a lens to spotlight how Black populations are disadvantaged, and considers the overlapping impact of other social identities, including gender and sex. Systemic and institutional racism further magnify these disparities creating marginalization that disproportionately impacts Black people Aggregated data perpetuates the erasure of Black people and is dangerous as it distorts and loses data in the process, making it difficult to infer how Black people are doing (Sharpe, 2019) in relation to various outcomes in care. Few studies provided an intersectional interpretation such as the intersection of race, sex or gender for Black people experiencing TBI. Disaggregated data is needed for effective practice and policy changes and intersectionality provides a valuable tool to consider how multiple identities and systems of oppression create unique and distinct forms of discrimination that shape how data is collected and interpreted (Sharpe, 2019). Even more, in the qualitative research, the voices of Black participants are silenced as the data lacks consideration for intersectionality when reporting the findings. The question remains, what conclusions can be made about Black people in the absence of knowing which Black populations are being studied?
Dismantling Hidden Socio-Political Assumptions in Language
Language is political and can shape perspective and narratives. The discourses evoked in the title of articles suggest that race and ethnicity evoke significant impact across TBI-related outcomes such as community integration, medical disposition, and care and treatment. Titles are important in drawing attention to and increasing readability and knowledge translation. The titles alone may, in turn, reinforce invalid claims of race not being socially constructed. For instance, the use of race as a moderating variable in Yeates et al. (2002) can portray the essentialization of race as a racial category that causes differential outcomes despite the authors' positioning race as a social construct. Language can be used as an invisible tool to idealize whiteness and normalize anti-Black racism. The underlying assumption is that the white group represents a standard from which all racialized minorities deviate from, and that deviation is measured and interpreted (Whitfield et al., 2008). There is a dire need to explore how racism is operating in these institutional spaces as opposed to reproducing literature about racial disparities (Jones, 2002). Specific consideration for addressing institutional anti-Black racism involves addressing racial bias and its related intersections in the clinical care setting and what type of research questions are prioritized. The studies included in this review reflect geographical locations that are all based in the United States. Future research reflecting different social, historical, political, and economic contexts, particularly a publicly funded health care model, is needed to provide diverse contextual understandings.
Institutional anti-Black racism shapes care pathways, outcomes, and human occupation for Black people experiencing TBI. A lack of consideration for how institutional racism operates and manifests may lead to color-blind approaches to clinical care and inequitable opportunities to participate in occupation. For instance, Arbogast et al. (2016) expressed that Black youth often seek care in emergency departments and subsequently stated that greater efforts are required to educate primary care clinicians as that is where most people go to seek care. This color-blind approach undermines where Black patients seek support for their TBI and instead reinforces inequitable change. Despite the best intentions, many of the included studies in this review failed to consider intersectionality. Multiple intersecting identities such as race, gender, and class including the impacts of these structures determine which populations benefit from particular care pathways. In adopting this lens, what does it mean for Black people to continuously face differential treatment and poor outcomes? Objectivity is not synonymous with color-blindness. Color-blindness is a counterproductive mechanism that supports the institutionalization of racism and thereby the perpetuation of whiteness. This may lead to policies that unfairly treat Black people. The lens that is applied to research reflects the way that the problem is operationalized. Further, how can racial bias and racism be comforted in research and clinical practice, and how can issues of racial stratification and their consequences be acknowledged and addressed? For example, Paradies et al. (2014) published a systematic review of various measures of health care provider racism targeting racial bias, stereotypes, and discrimination.
Rethinking Racial Capitalism and the (re)production of Anti-Blackness
One of the more obvious research gaps revealed by this review is the scarce research available on interventions and programs along the care pathway. Many studies acknowledged the importance of exploring, examining, and eradicating the underlying factors for racial health disparities in TBI outcomes (Bowman et al., 2007; Burnett et al., 2000; Egede et al., 2012; Hart et al., 2003, 2007; Howrey et al., 2017; Kane et al., 2014; Piatt & Neff, 2012; Shafi et al., 2007; Sherer et al., 2003; Yeates et al., 2002). Although many studies highlighted racial and ethnic disparities, assessing racial health disparities may be complicated by the lack of attention paid to the impacts of unconscious bias. Interventions addressing the underlying mechanisms of racial disparities is key and has been identified in recommendations for future research by other study authors (Kane et al., 2014; Shafi et al., 2007; Warren et al., 2016; Yeates et al., 2002). Interventions and programs to support the unique needs of Black persons experiencing TBI are fundamental to participation in activities of everyday living and the more long-term rehabilitation goals for community integration. In doing so, it is increasingly important to adopt an anti-racist lens that acknowledges the realities of Black people and moves away from a one-size-fits-all approach.
Disparities in funding levels from large national funding agencies have been found to underfund health equity-focused research and Black scholars in particular (Ginther et al., 2011; Hoppe et al., 2019). It is important to recognize that this negatively contributes to the lack of tenure positions in academia for Black faculty and the type of research that is prioritized (Stevens et al., 2021). The underfunding of health equity research and the rise of racial funding disparities disproportionately impacting Black faculty continue into the present day (Stevens et al., 2021). A paradigm shift away from positivist world views and towards onto-epistemological views that reflect Black people’s realities is needed to make visible racial oppression and how intersectional issues of health inequities can be understood and addressed (Telhan et al., 2020). Critical qualitative research has the potential to challenge taken-for-granted assumptions and foreground how institutional racism has been normalized through the erasure of voice and first-hand Black experiences in these spaces. Exploring the experiences, understandings, and expectations that Black people have of accessing and or receiving health care for TBI could provide the required information to create accessible pathways to access appropriate care to meet their needs in living fulfilling lives.
Lastly, racism becomes institutionalized as violent narratives of Black people that become reproduced in research and clinical practice. Anti-Black racism can be displayed as racial bias, whether it is conscious or unconscious. Over 95% of the articles in this review applied the category of white as a reference group. In these articles, Blackness becomes associated with negative portrayals, including being unmarried, less educated, prone to intentional violent-related injuries, at-risk population, and unproductive (Gary et al., 2009; Sander et al., 2009; Schoop et al., 2006; Sherer et al., 2003). Opportunities to further discuss intersections of violence, human occupation, and considerations for ethical, appropriate, and relevant support services are missed. While some studies reported that violent etiology impacts employment and community integration (Schoop et al., 2006; Sherer et al., 2003), there were no reported interventions, programs, pathways, or unique considerations to support those experiencing TBI as a result of violence and the lack of opportunities to engage in occupation.
The need to consider appropriate care pathways that consider the mechanism of injury and particularly, the needs of those experiencing TBI as a result of violence has been acknowledged (Hank et al., 2003). The importance of acknowledging the racial trauma of inequities (Telhan et al., 2020) and deprived opportunities to live a life worth living is significant in the road towards an equitable system of care and rehabilitation. A racial trauma-informed approach that considers the structural and institutional consequences of racism such as differential disparities, inequitable access, outcomes, and treatment (Telhan et al., 2020) is critical. Furthermore, ensuring that the voices of Black people are heard, especially in regard to research that impacts them, is not only important in devising interventions, programs, and models of care that meets their unique needs but also in preventing anti-Black narratives that reproduce material consequences in clinical care and life. This moment in time calls for a new era of social accountability, one that considers and takes action against the aftermaths of institutional violence by diagnosing and treating racism (Evans et al., 2020).
Clinical and Public Health Implications for Practice, Policy, and Research
Towards the end of Thicker Than Blood: How Racial Statistics Lie, Zuberi (2001) questions how the logic of social statistics shaped and influenced by white logic can be deracialized? White logic refers to the “content in which white supremacy has defined the techniques and processes of reasoning and facts” (Zuberi, 2001, p. 17) where the methods are the tools used to support and reproduce a mirrored image of the racial stratification of society. To this extent, all researchers, clinical care providers, and policymakers must practice critical self-reflexivity and revisit onto-epistemological commitments to consider the social, historical, political, and economic realities that govern Black life in various geographical locations. Table 1 provides recommendations for future research provided by all studies included in this review.
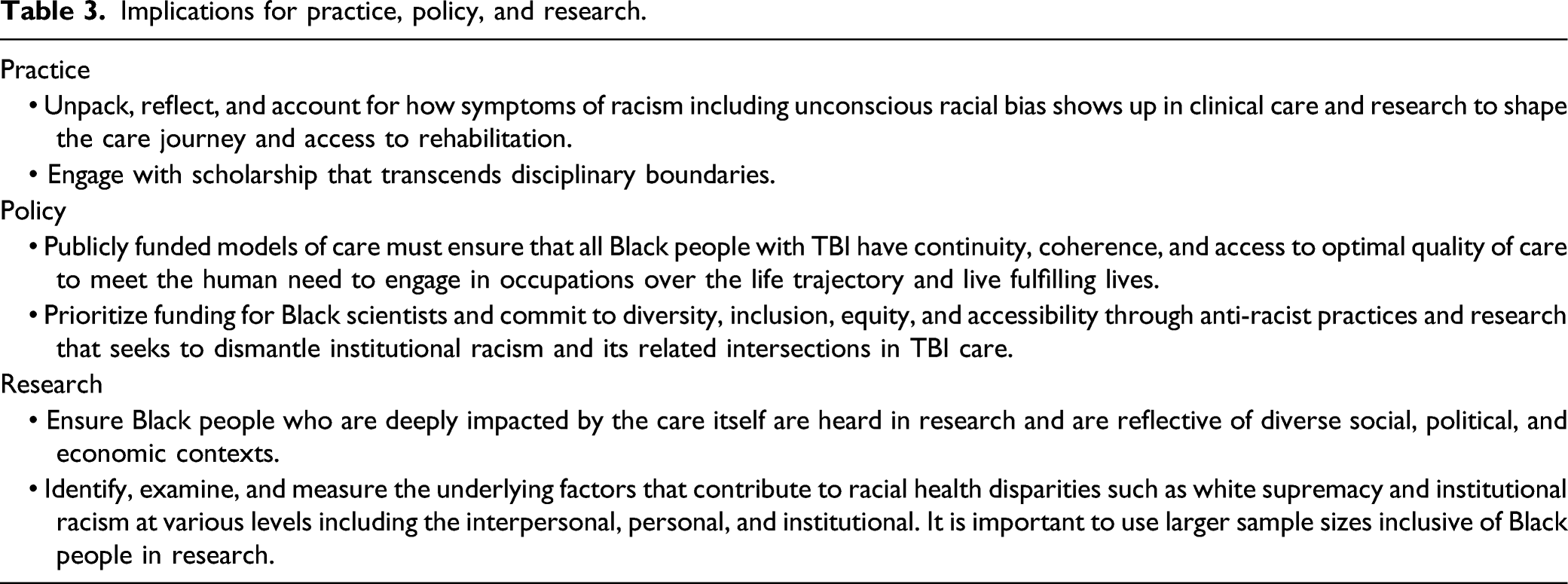
Implications for practice, policy, and research.
Gillborn (2010) highlights the importance that numbers are not neutral and hold meaning based on social categories of identities and discriminatory systems of oppression. How can quantitative research capture the everyday experiences of Black persons with TBI and the impact of the clinical care pathway? One of the tenants of CTD is critical race theory, which is a body of literature that foregrounds racism and the subtle ways it shows up in society, including legislation, research, and practice (Delgado & Stefancic, 1998). A critical race lens can reveal how racism can be embedded in quantitative methods and challenge dominant application and interpretation of numbers (Gillborn, 2010). Gillborn et al. (2018) provided five principles for qualitative methods informed through a critical theory lens. These principles can be expressed as the following: “(1) the centrality of racism, (2) numbers are not neutral, (3) categories are neither “natural” nor given: for “race” read “racism,” (4) voice and insight: data cannot “speak for itself,” and (5) using numbers for social justice” (p. 169). These principles can be approached as a starting place to consider the clinical and public health implications of race-based data by centering racism and how this reinforces whiteness and produces material consequences for Black persons experiencing TBI.
Limitations
One limitation is the lack of quality assessment applied for this review. Although quality assessment is not a necessary component of scoping reviews (Arksey & O’Malley, 2005; Levac et al., 2010; Peters et al., 2015), the decision to not include such an appraisal may be viewed as a limitation of this review. However, the goal of this review was to map the scope of the literature and provide a comprehensive critical analysis. Future research applying quality assessment for studies in this area of work will be a significant consideration to understanding the literature on care pathways for Black people experiencing TBI. This review was limited to the English language only and did not include grey literature. By nature, other relevant studies published in different languages and other information sources may have been overlooked. However, these limitations do not lessen the significance of the results reported.
Conclusion
This is the first scoping review of the academic literature conducted to adopt a critical lens to spotlight what can be understood about taken-for-granted assumptions and practices around integrated care pathways that consider Black people living with a TBI. This review illustrates that anti-Black racism becomes institutionalized in subtle ways that render it normal, invisible, and a problem that remains unchallenged and unnamed. Instead, symptoms of racism are named as potentially contributing to racial health disparities such as bias, prejudice, and systemic barriers. A significant finding is that this research is dominated by quantitative approaches that use race as a biological construct in analysis and interpretation. Future research that acknowledges and prioritizes addressing the institutional forms of anti-Black racism and its related intersections along the care pathway is important in working towards a vision of care that meets the unique needs of Black people living with a TBI. This responsibility must also be reflected in funding agencies. By conducting this review, our intentions are to invite researchers in the area of TBI and care pathways to consider and question how dominant paradigms, methodologies, and narratives make it easier to keep the racial order in place. We hope that by conducting a review that centers Black life as the focus, care and rehabilitation can be reimagined to meet the needs of Black people experiencing TBI to live fulfilling lives.
Footnotes
Acknowledgments
We would like to thank Ms. Jessica Babineau for assistance in developing the search strategy for this review, Ms. Andrea D’Souza for assisting with first level title and abstract screening, and Ms. LLana James for contributions to the critical transdisciplinarity framework and the protocol for this review.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This review was supported by the Health System Research Fund Program Awards, “Integrating Brain Injury, Mental Health, and Addictions”, Ministry Grant No. 267. The views expressed in this publication are those of the authors and do not necessarily reflect those of the Ministry of Health and Long-Term Care. Samira Omar was supported by a Toronto Rehabilitation Student Scholarship and a University of Toronto Fellowship. Dr. Angela Colantonio was supported in part by the Canada Research Chair Programs.