
Abstract
Background
The current study addresses the issue of societal stigma attached to mental health issues of college students, which strongly suppress their attempts at help-seeking.
Focus of the Article
✓We design a meso-level midstream intervention to effect a behavior change of mentally depressed students, who, due to internalized societal stigma attached to mental health issues, strongly evade help-seeking.
✓We use theoretical arguments and formative research to design a shadow social marketing (SSM) meso-intervention to normalize help-seeking behavior of individuals suffering from mental health issues.
✓We perform field-testing of our intervention to ascertain its comparative efficacy against two competing micro-interventions.
Research Question
To address a complex problem that does not have a direct, clear-cut solution at either the micro or the macro level, we investigate, in this study, whether an SSM meso-intervention performs better than micro-interventions in alleviating social stigma attached to mental health issues. Its primary benefit is to establish a connection between the micro and the macro levels.
Importance to the Social Marketing Field
Social marketing scholarship underscores a number of undesirable consequences of micro-level social marketing interventions that directly target individuals who suffer from mental depression, because their attempts at help-seeking are grossly suppressed by societal stigma attached to mental health issues. Our study contributes to the understanding of how the SSM meso-intervention could serve as a better alternative to direct interventions in normalizing help-seeking behaviour of affected individuals. We hope that changes of social norms at the community level can eventually lead to societal macro-level changes with modification and enhancement of institutional norms.
Methods
We use an SSM approach to design a meso-level, midstream intervention to alleviate societal stigma that deters help-seeking of mentally depressed students in an educational institution. We use survey methods for data collection and Tobit regression for data analysis to empirically test our meso-intervention against two other micro-level interventions.
Results
Our hypothesis that stigmatized individuals are more likely to avail of wellbeing-related services offered by a platform based on an SSM, meso-intervention rather than by one that does not adopt such a strategy is empirically supported strongly (
Recommendations for Research or Practice
A meso-level intervention is an essential prerequisite to bring about macro-level changes to address stigma attached to mental health issues. As a practical matter, changes of social norms at the community level have a strong potential for bringing about societal macro-level changes with modifications and enhancements of institutional norms and eventual micro-level help-seeking behavior.
“There is a girl who smiles all the time, to show the world that she is fine. A boy who surrounds himself with friends, wishes that his life would end. For those that say they never knew — the saddest leave the least of clues.” ― Lang Leav (Leav, 2016, p. 48)
Introduction
Depression among college students is a complex problem in general that is further exacerbated by extreme reluctance to seek external help due primarily to perceived stigma attached to mental health issues (Vidourek et al., 2014). External societal stigma leaves those suffering from such conditions to be in denial and averse to seeking help. In India, studies on mental health stigma among young people are rather scanty (Kaur et al., 2021). On the practical side, the need for efficient mental health services is dire and requires immediate attention.
Most social marketing interventions target depression directly rather than address societal stigma that deters help-seeking at the individual level (DeBate & Gato, 2021). Prior studies have emphasized the inadequacy of micro-level social marketing interventions targeting individuals where the root cause of issues lies at the macro level (Kennedy, 2016). To address this problem, we adopt, in this work, a shadow social marketing (SSM) approach (Roy & Goswami, 2020) to design and develop a meso-level, midstream intervention platform called Cocoon to alleviate the deleterious effects of the perception of societal stigma that deter help-seeking among mentally depressed undergraduate (UG) students in an educational institution. SSM essentially involves camouflaging the real offering – mental health services – with a shadow offering. For Cocoon, it was career guidance.
To be sure, this is a wicked problem. Such problems lack clarity in definition and scope and are symptomatic of other deeper problems involving multiple stakeholders with conflicting interests (Rittel & Weber, 1973). They involve “complex, multi-layered issues which have multiple causes, perpetuating factors, and solutions” (Kennedy, 2019, p. 1) with “multiple institutionalized causes beyond the behaviour of individuals” (Barrios, 2021, p. 513).
Scholars in the human sciences and medical sociology have established that people attempt to make sense of their social identity by constructing images of themselves (Williams, 1984). Mentally depressed individuals frequently attempt to divest themselves of a negative identity by a practice referred to as distancing (Gibson et al., 2004; Neale et al., 2011). It involves self-criticising or belittling themselves with respect to others in the society. In turn, they are viewed as “dangerous, unpredictable, violent and bizarre,” with “weak morals, poor character, malingering, lack of self-control or bad breeding” (Ross & Goldner, 2009, p. 560). This vicious circle oftentimes makes it difficult for them to find employment if their conditions are known to prospective employers. The fear of adverse consequences in terms of poor employability, “spoiled identity,” 1 and societal stigma (Goffman, 1963) forces denial of their misery and discourages them from seeking professional help.
We draw from stakeholder theory (Hult et al., 2011) to develop a value proposition based on SSM to include multiple stakeholders in our study. They include, for instance, faculty, general students, educational administrators, wellbeing experts, and affected students, all with their own, and frequently, conflicting interests. To empirically assess the efficacy of the SSM-based Cocoon intervention platform, we compare it, from the students’ perspective, with two competing micro-level offerings.
The Indian Context, Perceived Stigma, the Wicked Problem, and the Logic of Cocoon
The Indian Context
Formal studies of perceived stigma among students affected with mental health issues in India are few (Kaur et al., 2021). Surprisingly, while 20% of global youth reported mental health issues, only 7.3% of the India’s 365 million in this demography reported it (Gaiha et al., 2020). According to a report by WHO, India has the highest number of depressed people in the world (Garg, 2022). The Global Burden of Disease Study also reported that depression contributed primarily to total mental disorders in terms of disability-adjusted life-years (India State-Level Disease Burden Initiative Mental Disorders Collaborators, 2020). Deb et al. (2016) further reported that 37% of university students in India suffers from moderate depression, and the figure is 13% for severe depression. Furthermore, the 2021 UNICEF and Gallup survey reported that although one in seven in the 15–24 age group often felt depressed in India, it was the only country among the 21 surveyed in which a minority of 41% of young people felt that those suffering from mental health issues should seek help, which amounted to 83% worldwide (Garg, 2022).
Different Approaches to Stigma
Anti-stigma interventions involve handling of public stigma as well as internalized self-stigma. Public stigma interventions for college students include mental health education and/or direct contact with individuals suffering from mental health issues. Such efforts are conspicuous by their absence in low and middle-income countries (Clement et al., 2013; Thornicroft et al., 2016). Meta-analysis results show that education is more effective than contact-based approaches, especially in the medium to long term, and mass media interventions are likely to reduce stigma (Clement et al., 2013; Corrigan et al., 2012; Mehta et al., 2015).
Another approach focuses on promoting the idea of mental health-mental illness as a continuum. This proves to be better in reducing stigma compared to a dichotomous approach to having or not having a certain mental health condition (Schomerus et al., 2016). Self-stigma interventions include, among others, psycho-social intervention involving individual and group sessions and peer-led, group-based intervention with disclosure as primary mode of countering stigma (Yanos et al., 2015).
Mental Depression: A Wicked Problem
Earlier scholars have shown that a macro-level social marketing approach, facilitated by changes in public policies including governmental rules and regulations, is essential to address wicked problems, without which micro-level changes are infeasible (Brennan et al., 2016; Wymer, 2015). In our view, however, only macro-level policy changes are insufficient to bring about the desired micro-level behavior. To be effective, a meso-level intervention is an essential prerequisite for an individual-level effect to fructify. Extant literature has somewhat under-emphasized the crucial role that meso-level interventions play in addressing wicked problems. We address this gap by empirically evaluating the efficacy of a meso-intervention in comparison with two other micro-interventions, in an environment where societal stigma dissuades help-seeking for mental health issues. Additionally, we answer the call to focus on wicked problems unique to the global south that is missing from mainstream literature (Gordon et al., 2016), as well as the appeal by Wilner and Huff (2016) for more research on legitimization of tabooed products and services.
The wicked problem of mental depression is recognized as one of the major causes of suicide ideation. In India, suicide attempts were a criminal offense until about 2017 (Bekedam, 2016; Sneha et al., 2018). Furthermore, adequate public policy measures by the government for promoting mental health and wellbeing were missing. To make matters worse, there was no requirement on educational institutions to implement any well-defined mental health policies for students. This disconcerting state of affairs confronts us with the critical need for meso-level interventions to address societal stigma attached to depression, help change public opinion, and raise increasing public awareness through effective ideation and implementation of public policies. Huff et al. (2017) proposed that consumer interest groups helped to change institutional norms and indirectly influenced policy makers to deal with wicked problems. Indeed, for such problems, small, incremental improvements by multiple interventions prepare the ground for bringing about long-lasting, macro-level social changes (Termeer & Dewulf, 2019).
Hoek and Jones (2011: 41) calls for “rapprochement between upstream and downstream social marketers.” Russell-Bennett et al. (2013) emphasize the influential role of “others” involving community, organizations, and friends through mid-stream efforts. Kennedy (2016) contends that macro social marketing should involve not only downstream and upstream interventions but midstream ones as well. Nevertheless, midstream meso interventions have remained relatively under-researched, and little attention has been paid to the actual development of value propositions for targeting multiple stakeholders with conflicting interests (Pettigrew et al., 2014). This is where we contribute. Specifically, we evaluate the efficacy of a meso-level SSM intervention and examine whether it works better than direct ones in alleviating individual stigma attached to seeking help from mental health professionals or peers.
SSM and the Logic of Cocoon
External, societal stigma attached to mental illness leaves affected individuals to be in denial and averse to seeking help. In the SSM approach, the intervention’s real intention to promote help-seeking behavior of the affected individuals is camouflaged. This “shadowing” is particularly effective and beneficial in situations where perceived stigma strongly dissuades individuals from seeking external support. It helps individuals to develop and nurture a different and optimistic outlook on the offered products or services that does not, in any way, evoke the underlying fear of perceived stigma attached to mental health problems.
We adopted this approach by attempting to alter the community-level, stigmatized perception of mental health issues in offering the services of Cocoon, which were well integrated with many services students commonly avail of as they pursue a UG degree in a higher educational institution. Most micro-level interventions promote mental health services directly. By contrast, Cocoon offered them as a part of its full set of services, with the primary focus being on achievable career goals and placements of students by encouraging them to develop practical or technical skills to ensure better employment prospects. The idea is that college life and the journey in pursuance of a suitable career are naturally stressful periods of student life, and mental health support is a perfectly “normal” need during this phase. It is in this way that Cocoon was able to normalize help-seeking for mental health services. A similar approach was proposed by Gaddis et al. (2018).
Specifically, we targeted all individuals in the student community rather than only those suffering from mental health problems. This is directly in line with the approach adopted in meso-level interventions to reduce stigma attached to mental health issues (Cook et al., 2014; Corrigan & Fong, 2014; Kosyluk et al., 2016; Thornicroft et al., 2016). Pescosolido & Martin (2015) propose that stigma can operate at micro (self-stigma), meso (public stigma) and macro (structural stigma) levels. In particular, public or meso-level stigma captures stigma in the general population (Livingston & Boyd, 2010). This is operationalized almost uniformly as perceived stigma (Link et al., 1991); in other words, how members of the public community perceive the individuals suffering from mental ailments. Studies have also established the relationships between community-level stigma and mental health outcomes in university campuses. In this regard, it has been found that addressing both individual and institutional level stigma is the best way to tackle the situation (Byrd & McKinney, 2012).
Theoretical Framework
Stigma
Young people suffering from depression or other mental health problems are frequently in denial of their debilitating mental conditions (Yusoff & Esa, 2015). This arises from deeply ingrained sociocultural prejudices that generate large-scale, external stigma attached to mental health issues. They are ostracized, avoided, rejected, feared, and discriminated against (Hogan, 2003). A large number of the affected young people live in constant fear of societal judgment passed upon them and avoid seeking help from mental health professionals to ameliorate their mental conditions (Bakan, 2016; Phillipson et al., 2009). Indeed, the stigma is so deep-rooted that even healthcare professionals are known to harbor it (Knaak et al., 2017).
Although the external stigma forces the sufferers to hide their deteriorating mental conditions, it frequently becomes impossible to do so, and inadvertent signs become apparent (Goffman, 1963; Henderson et al., 2013). In this situation, severe self-harm or even suicidal attempts are common. Indeed, the extreme reluctance or fear of the affected individuals in seeking help even in an emergency is undeniably linked directly to external stigma (Wyllie & Carlson, 2019). In India, because of a lack of serious public health policies of the government, it became difficult, historically, culturally, or administratively, to develop interventions to reduce stigma or encourage self-help in mental health issues.
Macro-Meso-Micro Lens of Social Marketing Interventions and Help-Seeking
The majority of the common social-marketing interventions that attempted to facilitate help-seeking by targeting depressed individuals have inadvertently put the carriage before the horse. While interventions should target external stigma that causes the reluctance to seek help, most interventions suffer, in practice, from the neo-liberal tendency of putting the responsibility on the suffering individual vis-à-vis the societal stigma that forces this behavior of shying away from help-seeking (Crawshaw, 2012). Macromarketing scholars have argued that social marketing must shift its focus from responsibilization of individuals with downstream micro-marketing interventions targeting individuals to examining and addressing societal root-causes that cause problematic behaviors at the individual level (Brennan et al., 2016). Specifically, Brennan et al. (2016) call for moving beyond the macro-micro dyad and propose a synthesis at the meso level.
The micro level examines individual behavior, and the macro level focuses on the juridical or policy environment. By contrast, the meso level promotes collaboration among market actors rather than targeting end-consumers directly (Karpen et al., 2012). While social marketing efforts at the macro level are upstream and those at the micro level downstream, the meso level establishes a rapprochement between the two and is, therefore, identified as mid-stream (Hoek & Jones, 2011; Russell-Bennett et al., 2013). Brofenbrenner (1979) stressed that individuals are influenced at multiple levels: macro (distant from person); exo (external to person, such as the legal system); meso (between the person and his social environment that subjects them to injunctive norms); micro (individual in close societal circle). Brennan et al. (2016), however, argue that at least a synthesis of the micro-macro layers is necessary with the evoking of meso-interventions.
While peers might erroneously perceive the depressed ones to be prone to violence, administrators might blame them for promoting the erroneous perception of a difficult academic environment, and recruiters might altogether avoid such individuals with apprehensions about work productivity. A meso intervention addresses this problem by attempting to bring a change in the social environment, so that help-seeking at the micro level becomes feasible. With such interventions, the overall social environment of stigma attached to mental health problems causing the individual-level avoidance of help-seeking can be addressed. It, therefore, has the promise to create a strong foundation for long-term productive “social good” that social marketing aims to promote. Cocoon was designed and developed from this perspective.
A Meso-Level SSM Intervention
In this study we design a meso-level intervention devoted to reducing the deleterious effects of external stigma without introducing direct educational messages into the mental health awareness of the affected individuals. The intervention’s primary objective is to positively influence the layer below it – the micro-environment. This is in line with Kennedy’s (2016) view to alter institutional norms with macro-level social marketing interventions that promise to bring about a long-term societal change, reducing external stigma attached to depression. We argue that modifying macro-level institutional norms requires prior meso-level interventions. Consequently, the stigma effect is significantly reduced.
We further argue that interventions framed principally as mental health educational messages might not work effectively on the implicit attitude that drives stigmatizing beliefs and convictions (Banaji & Greenwald, 1994). We designed and developed our intervention in the setting of a residential Indian university (henceforth, University X or UX) located in a semi-urban area to examine whether stigma in help-seeking is better addressed at a meso level compared to more direct micro-level interventions that target individual-level changes without attempting to address the issue of external stigma. To this effect, we designed a web-based intervention platform named “Cocoon” 2 to provide a common ground for all individuals, depressed and not-depressed, to interact in a common arena of concern for both groups – their overall career progress and development. The underlying principle is to normalize students’ help-seeking behavior as a natural remedy for their academic stress.
Following the approach of Wilner and Huff (2016), we avoid focusing on the tabooed consumption of services, such as seeking help from mental health professionals or wellbeing experts. Instead, we attempt a design reframe to normalize the stigma attached to depression in students, who are the users of Cocoon. The services offered by the intervention are carefully designed not to explicitly mention any mental health problems to the users. Following SSM (Roy & Goswami, 2020), the strategy here is to “shadow” an intervention’s blatant explicitness that might trigger stigmatized feelings in affected individuals. This normalizes the necessity of taking care of mental health as a natural outcome of the competitive and stressful environment. Although it may not immediately motivate depressed students to directly seek external help, the normalization encourages help-seeking behavior without manifest exposure to mental health issues, which are “normal” in an academically competitive environment. Moreover, it implicitly promotes inclusivity through the apparent offering of career services that normalizes mental health challenges. This includes, among others, competitions to target, courses of study, extracurricular activities, and so forth.
Given that students have a common superordinate goal of career success that can often be stressful, Cocoon, as an SSM web-intervention, essentially camouflages the real offering of stigma reduction in help-seeking with an apparent offering of career development and academic advancement. The features include, for instance, talking to a teacher; participating in competitions; resources for courses; taking a wellbeing challenge; talking to a friend or wellbeing professional, without any explicit mention of depression or mental health problems (Figure 1). Prototype of the Cocoon web-based intervention platform.
Prior research has shown that audiences create meanings and draw inferences from indirect claims made through images, text, and metaphors, among others. This process has proved to be more persuasive and effective than direct claims (Amar et al., 2021). Our web-intervention has the image of cocoons and butterflies in the foreground. Adopting the metaphor of a caterpillar using a cocoon as a passage to transform itself into a beautiful butterfly, our intervention offers students a space for finding ways to elevate the self to explore a purposeful existence that transcends the travails of everyday life full of anxiety, stress, hopelessness, or depression. Cocoon includes the following tabs: (a) Home, (b) Competitor’s Arena, (c) Placement Prospect, (d) Podcast, (e) Alternate Guide to College, (f) Take a Challenge and (g) Talk to Someone. A short description of each of the tabs is presented below: (a) Home: Describes how the site is a safe space to find one’s purpose, try new pursuits and get support from faculty and peers, accept wellbeing challenges to find the best version of oneself, and when it becomes difficult, talk to a peer or professional without revealing one’s identity. (b) Competitor’s Arena: Participating in competitions helps a student hone the skills that are useful in getting desirable employment opportunities. This tab facilitates finding and starting many such competitions. (c) Placement Prospect: This tab helps one find an internship, find like-minded individuals to start one’s start-up company and post a job opportunity. (d) Podcast: This section has three parts: Life Hacks, Gyaan ki Batti
3
and Vote for Next Podcast. (e) Alternate Guide to College: Common concern among students include, for instance, how the instructors or the courses might be and how to do well on difficult parts of a course. This tab addresses these concerns. (f) Take a Challenge: One could offer or accept a challenge, such as a daily gratitude practice lasting a week, a one-minute mindfulness challenge and similar others. (g) Talk to Someone: This is the only tab that deals directly with mental health. The idea is that, while dealing with the challenges of college-life, one may sometimes want to talk to someone anonymously. There are three options here: Talk to a Wellbeing Expert; Talk to a Friend; or Join to Become a Wellbeing Activist.
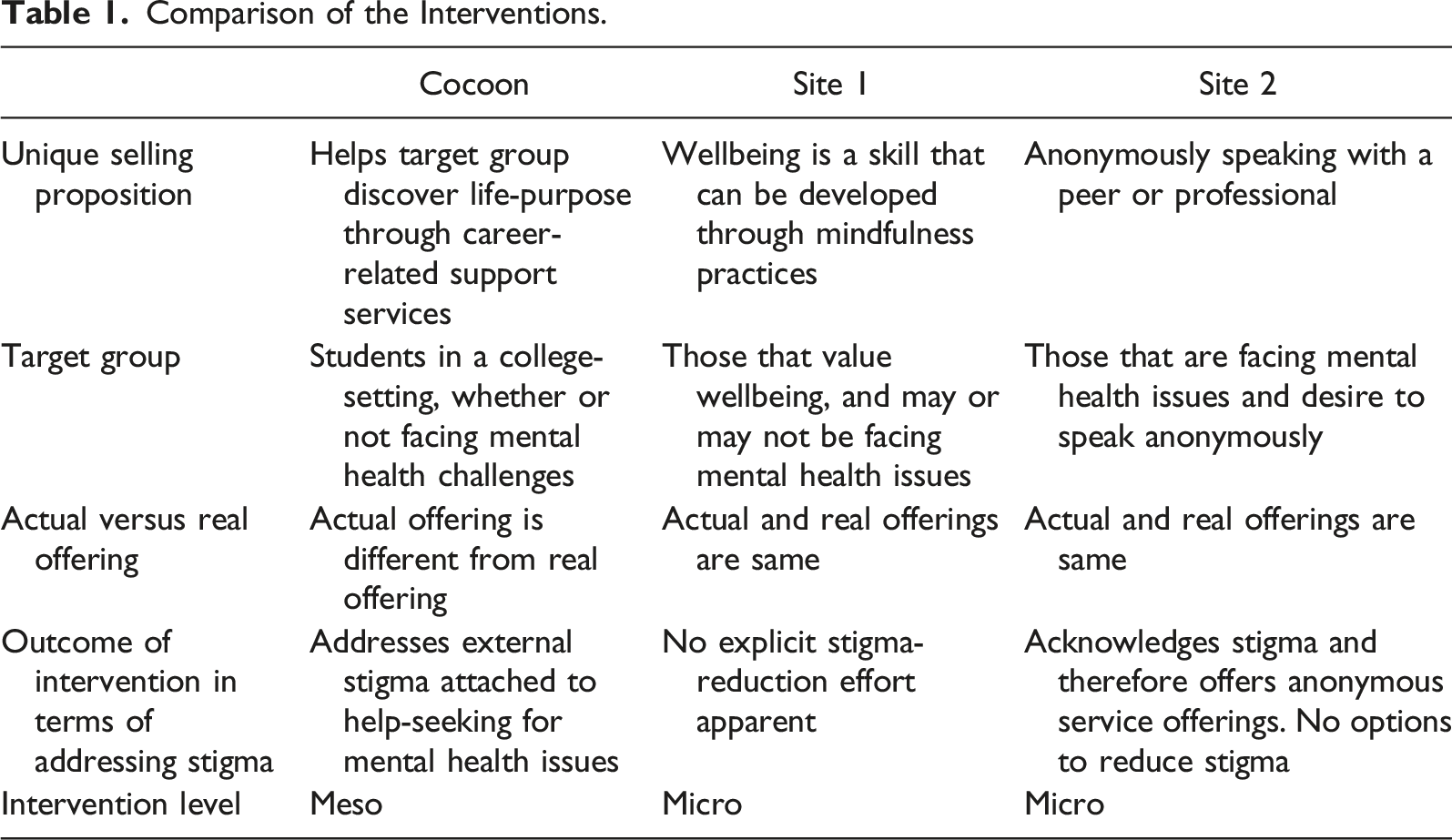
The SSM intervention provides an apparent offering as a substitute for a real one. In Cocoon, the apparent offering is career-related support and finding one’s purpose in a personally meaningful way (with the tag-line ‘paint your wings your colours’). The real offering is normalizing help-seeking behavior of those that are struggling with mental health challenges in fear of external stigma associated with help-seeking.
The intervention uses stakeholder marketing approach (Hult et al., 2011). It brings together under the same umbrella general, non-depressed students (tabs (a) through (g)), depressed students (tabs (a) through (g)), faculty and administrators (tab (d)), and wellbeing professionals such as psychologists; psychiatrists; meditation and yoga experts (tabs (f) through (g)). The needs are common but not conflicting. Offering anonymity in tab (g) enables accessing a tabooed product without the Goffmanian “spoiling” of offline identity (Goffman, 1963; Veer & Golf-Papez, 2018). We therefore hypothesize: Individuals who perceive external stigma in an environment exhibit a greater likelihood to avail of services offered by an intervention that utilizes a meso-level SSM strategy rather than by ones that do not adopt such a strategy.
Methods
Data and Research Setting
Decriminalization of suicide in India in 2017 is a macro-level policy change. We collected data for our study two years after that, covering the window from April to September 2019. The study sample constituted UG students of UX, a fully residential university with its campus located in a semi-rural area of a northern Indian state. It had about 200 faculty members and a student population of approximately 2000 in UG, masters, and doctoral programs in the schools of engineering, natural sciences, social sciences, humanities, and management divided into more than 20 departments and five research centres. UX had a mental health support system in place, whose services were freely available to its students.
In order to test the efficacy of Cocoon to alleviate social inclusivity of stigmatized students, we tested the intention of respondents to subscribe to the services provided by three different web-based platforms. In addition to Cocoon, we selected two other platforms, both of which had already been in production when the responses were collected. We designated them as “Site 1” and “Site 2” (concealing their real identities). These two sites did not offer their services specifically to student communities. While Site 1 was a listening platform targeting individuals suffering from mental health issues, Site 2 was aimed at general users to improve wellbeing through meditative self-reflective practices dealing with mental health. Cocoon 4 , on the other hand, targeted students on career-related issues, with one section on taking a wellbeing challenge (thereby close to Site 2) and another section on talking to someone (similar to the functionality of Site 1). Respondents were shown videos giving the walk-through of the three different platforms (Sites 1, 2, and Cocoon) and then asked to mark their preference for the usage of the services offered by them for three consecutive months. In an environment where individuals suffering from mental health problems are in denial of their conditions and resist all efforts to seek external help and support because of stigma, we contended that Cocoon, founded on its meso-level SSM intervention strategy, would fare better than the other two sites.
Early in Cocoon’s design phase, we realized that a general mental wellness platform might unwittingly create an “us-versus-them” marginalization for students with mental health problems, causing them to feel disgruntled or alienated. To overcome this problem and to ensure better self-management and personal wellbeing for them, we sought to provide a nurturing social environment through Cocoon’s anonymous platform, in which students would feel integrated into the environment and get around the concerned stigma issues prevalent in the Indian society.
Cocoon’s uniqueness lies in the positioning of its image for the offerings created in the minds of the consumers of its services. Its design ensures normalization of the behavior of stigmatized individuals. This was rooted in the conviction that there was nothing inherently wrong or shameful in seeking help when one felt distressed. In this regard, Cocoon served as an inclusive platform, offering its services to all students and focusing primarily on their career growth and advancement, academic progress, and other creative activities. This established strong inclusiveness of the interactions among the users and helped alleviate the external stigma from which most depressed students suffered. In particular, there was no explicit association of mental health issues in Cocoon’s tagline “paint your wings your colors.”
Comparison of the Interventions.
Our sample size consisted of 105 UG students. A trained student research assistant went to two large-sized classrooms that had mixed proportion of students from different disciplines and showed them an explanatory video of the three sites. With the permission of the concerned course instructors, the research assistant introduced the study and explained its purpose to the students. Subsequently, she showed videos explaining the three offerings to the students. After signing an informed consent form to participate voluntarily in the study, students from each of the two classes completed the survey individually, during which discussions with their peers were not permitted. The three site videos were shown on a mobile device, subsequent to which the participants responded on a google form 5 .
Measures
Unless otherwise noted, scales ranging from 1 = “strongly disagree” to 7 = “strongly agree” were used in the present study. For each of the construct variables that were measured using well-defined measurement scales, we tested construct validity by carrying out factor analysis on the items in the scales to revalidate their legitimacy. In this way, we ensured that the items loaded effectively on the corresponding constructs. For each construct, we obtained single-factor solutions, which substantiated construct validity and provided sufficient justifications for including the constructs as the study variables in our model. We also verified scale reliability by computing the values of Cronbach’s alpha for each construct. All alpha values were found to lie in the range of
Dependent Variable
We employed a proxy variable to gauge the purchase intention of the respondents to avail of the services provided by each of the three platforms. The use of such a variable to control for an underlying unobserved variable is common in marketing and econometric studies (Montgomery et al., 2000; Peña-García et al., 2020). The specific investment scheme we employed for this purpose ran as follows: all prospective users of the platforms were told to imagine that they were given a certain sum of money (e.g., □900 or 900 Indian Rupees) for three months for the purpose of investment, with the local currency appropriate for the financial and economic standards of the population of users in the region or country where the services would be offered (thus, for Cocoon, Site 1 and Site 2, it was □900). They were then instructed to invest portions of that money in one or more of the platforms depending on their choice. The variable
Stigma
Prior studies have confirmed that there is a sociocultural stigma attached to mental depression (Henderson et al., 2013). A previous depressive episode in the life of an individual does not stop the affected person from entertaining negative opinions about depression that reflect the views of the community and the particular social and cultural milieu. Because of stigma and shame attached to depression, personal weakness often becomes an ingrained self-prejudice that leads an affected individual to avoid problem acknowledgment and to decline offers of help, support, or potentially beneficial assistance (Kanter et al., 2008). We measured stigma by the 5-point Likert-type scale of Komiya et al. (2000). This scale assesses perceptions of individuals concerning how stigmatizing it turns out to receive psychological treatment. This is one of the standard stigma scales used in the field, and an example item reads: “It is a sign of personal weakness or inadequacy to see a psychologist for emotional or interpersonal problems.”
Controls
We included several control variables in order to explore alternative explanations for the relationships predicted in our model. These include a number of individual characteristics of students that could potentially influence the nature of the concerned relationships. To account for basic student demographics, we controlled for age (
We introduced wellbeing as an additional control. This construct is commonly understood in terms of subjective happiness as a positive emotional condition or affect of an individual and their satisfaction with life (Rose et al., 2017). It is as much as matter of individual personality as it is an element of the socio-cultural environment in which individuals function (Diener et al., 1999). We measured wellbeing on a 5-item scale 6 adapted from Lyubomirsky & Lepper (1999) and Diener et al. (1985). An example reads: “The general conditions of my life at the present stage are excellent.”
Statistical Analysis
The dependent variable (DV) in our study is the total amount (
A Tobit regression model makes the basic assumption that the underlying latent continuous variable follows a normal distribution, but the corresponding observed variable is censored due to limits imposed by its detection (He et al., 2020). Our continuous, censored DV is, therefore, a good candidate for Tobit. In this regard, our sample of 105 observations was not large; however, it was adequate for six covariates, including controls, for performing the statistical analysis in our study. To safeguard against bias, in addition to executing the standard Tobit regressions, we conducted bootstrap Monte Carlo simulations in the regressions. Between the two procedures, we did not see any significant differences in the values of the estimated coefficients.
Additionally, there was no panel structure in the data. There was, therefore, no need to compute a cluster-corrected covariance matrix for adjusting standard errors for intragroup correlations among the subscribers. However, we employed heteroskedasticity-robust standard errors to minimize the effect of heteroskedasticity and heteroskedasticity-robust
Findings
Primary Analysis
Basic Statistics of Model Constructs.

Coefficient Estimates for Cocoon, Site 1, and Site 2.
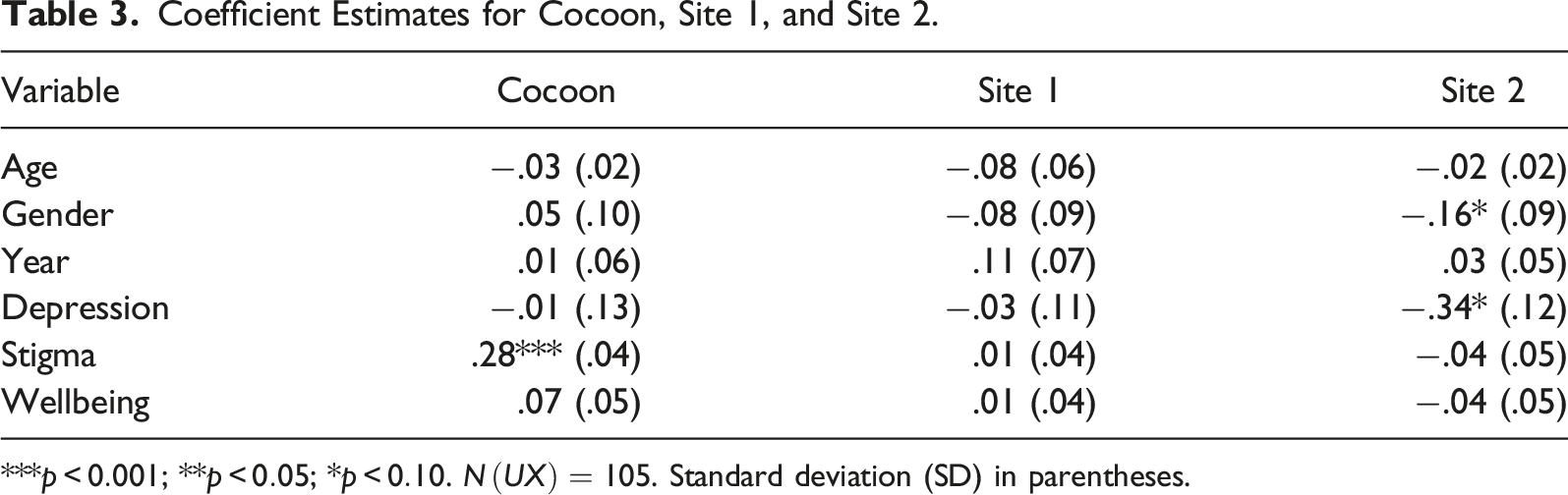
***
Our hypothesis asserts that stigmatized individuals will show a greater likelihood to avail of wellbeing-related services offered by an intervention platform that utilizes a meso-level SSM strategy rather than by one that does not adopt such a strategy. The results show that our hypothesis is supported with high significance (
Supplementary Analysis
In order to consider an alternative estimation model, we ran a number of supplementary tests for the final results. The details of these post-hoc analyses are not included here for considerations of space. Briefly, we considered three viable alternatives to Tobit: (i) We first transformed the DV to a percentage score of investment amount for each student and then ran a fractional logit on the transformed DV; (ii) We divided the entire range of the DV into four categories and then ran a generalized ordinal logistic model using the gologit29 command in Stata; (iii) We estimated a probit model by creating a binary classification variable for the investment amount
Discussion, Limitations, and Conclusion
Theoretical Contributions
The design and development of Cocoon began in earnest when the criticality of an inclusive intervention was felt to provide support and assistance during times of immediate need of students affected by mental health issues. In the multitude of common activities where students focus on skill development and career advancement, as well as talk anonymously with one another, stigma is alleviated and help-seeking emerges spontaneously and somewhat unconsciously. Cocoon provides this inclusive platform by shadowing direct addressing of mental health issues, thereby obviating perceptions of stigma and generating a more beneficial outcome than micro-level explicit interventions. Data were collected to probe students’ intention to use the Cocoon platform more effectively and spontaneously compared to other interventions that deal with mental issues directly.
The inclusivity of all individuals on Cocoon, with its explicit shadowing of direct mental health issues, facilitates an integration of the stigmatized individuals with others to share thoughts, ideas, career goals, and personal problems within an exclusively anonymous setting. Motivated by Goffman’s (1963) view that stigma leads to an individual’s spoiled identity, we argue that the identity of stigmatized individuals, even when spoiled or denigrated, could be resuscitated into its rightful state by establishing the inclusivity of these individuals with others without stigmatizing experiences. This is particularly encouraging, but the process must be carried out under careful and protective observances of anonymity. A study by Neale et al. (2011) applied a similar principle in the context of recovery from drug use as a transformation from spoiled to unspoiled identity.
As regards the breadth of inclusivity, Cocoon works better than the two direct micro-level interventions in handling stigma in a social environment with exposures to conversations, interventions, or efforts. Nevertheless, as mentioned before, Cocoon, during the course of data collection for the present study, was not in production but only available to potential users for testing. The respondents, therefore, did not have the opportunity to practically avail of its services.
Nevertheless, the use of a perception variable for the usefulness of a product or service to a potential user is one of the critical indicators of their intention to use the product or service (Peña-García et al., 2020). It is conceivable that when a product or service becomes popular, for any number of reasons, among similar groups of individuals, more potential users in allied situations and environments will be drawn to it or attracted by it. Some fractions of them, therefore, will actually end up using it in the fullness of time.
It is also important to recognize that Cocoon was primarily designed to alleviate the adverse effects of stigma among depressed college students who declined all offers of help, support, or assistance provided by mental health professionals. The intention of potential users of the platform to benefit from the services offered by Cocoon, whether motivated by popularity, word-of-mouth references, or any other means, is still a strong indicator of actual use of the services in the future. It is for this reason our DV served as a “proxy” for actual use. Such examples are common in the marketing and econometrics literature.
The institutional norm under consideration is personal responsibilization of a depressed individual to seek help in a stigmatized social environment that deems mental health issues to be a spoiler of identity (Goffman, 1963). We argue that it is impossible to target the norm with a purely macro-level policy change (e.g., the decriminalization of suicide in 2017 in India). Suicide attempts often emerge as an outcome of depression. We conducted our study two years after the policy change but found that Site 1 and Site 2 interventions that target both general and depressed individuals trigger stigma more than the Cocoon intervention. Currently, there is a singular dearth of policies in Indian educational institutions to be inclusive toward students suffering from mental health problems. Consequently, we intended to deinstitutionalize the prevailing influence of stigma and replace it with normalization, inclusion, and dignity of all affected subjects. Rettie et al. (2012: 421) have referred to such normalization as the “social process where products and practices outside the range of normality, gradually become accepted as standard and normal.” Indeed, there is a visible gap in the literature of normalization processes of tabooed consumption (Maguire et al., 2015). In this context, normalization is the category shift (Gollnhofer, 2017) that enables social inclusion of the excluded stigmatized groups of mentally depressed individuals and makes it easier for them to eventually seek external help.
Our study introducing the meso-level intervention also responds to the call to “embrace new tools and thinking, such as a meso-marketing approach, to synthesise micro- and macro-processes to effect change” (Brennan et al., 2016, p. 231). As a bridge “between the individual and the environment” (Brennan et al., 2016, p. 226), it involves more than one layer of the social change market (House et al., 1995) and goes beyond targeting individuals that shun help-seeking. We involve other stakeholders, such as non-depressed students and teachers, in order to address the external societal stigma that leads to avoidance of help-seeking by depressed students. In doing so, we move away from the micro-macro dyad (Brennan et al., 2016) with the use of a meso-level intervention to address a complex, wicked problem that does not have a direct solution at either the micro or the macro level. Its primary benefit is to establish a connection between the meso and the macro levels.
We admit, however, that it might not suffice to have a single meso intervention to address the problem of societal stigma. Nevertheless, it could greatly help to create a community-level awareness that might incrementally work to modify negative or deterring institutional norms that macro-level interventions typically target. This view is supported by Kemper and Kennedy (2021: 36): “culmination of multiple social marketing interventions, over the long term, can see a change in institutionalized norms that perpetuate wicked problems (i.e., mental health stigma)” and “cultural-moral institutional norms that support the inherent dignity of all humans (no matter their mental health status) could be incorporated into social marketing interventions.” In this regard, Cocoon upholds inclusivity, normalization, and dignity to those that were struggling with mental health issues. Further, motivated by earlier work of Trenchard-Mabere (2016) and Hovell et al. (2002), we argue that a meso-level intervention is an essential prerequisite for macro-level changes to address stigma, a particularly wicked problem today. We hope that changes of social norms at the community level can eventually lead to societal macro-level changes with modification and enhancement of institutional norms.
Implications for the Practitioner and Study Limitations
Self-harm and suicidality are often consequences of depressive mental conditions. Such actions were condemned and castigated as criminal offense in India until 2016 (Bekedam, 2016). On March 27, 2017, the Mental Healthcare Act, 2017, decriminalized suicide. Not surprisingly, until 2014, there were no government programs available for the promotion of mental health or suicide prevention (Sneha et al., 2018; World Health Organization, 2014). Although the legal state has now changed somewhat, the stigma attached to mental health issues has remained as one of the last vestiges of the earlier sociocultural tradition, and it is unlikely to disappear anytime soon. Fear of stigma works as a major deterrent to seeking help, even when it is offered free of cost.
As it happens, the issue of stigma attached to mental health has not been addressed as a rigorous public-policy measure. Its sensitiveness arises from the need to maintain sufficient confidentiality and anonymity in this process. In this regard, our study has practical implications for many higher education institutions where stress and personal distress result in spoiled identity and depressive conditions of individuals. The Cocoon platform, our meso-level SSM intervention, with its delicate concealment of mental-health explicitness, helps to underscore the unstigmatized and elevated self-recognition of the affected individuals. It also works better than direct interventions when handling stigma in a free, socially mixing environment.
A number of earlier scholars have contended that micro-level social marketing interventions, directed at individual consumers to seek help, would hardly be meaningful in an environment that had external stigma attached to wicked problems (Wymer, 2011, 2015). We show that meso-level interventions can address these problems by involving multiple-stakeholders with conflicting interests and gradually change the condition of the sociocultural environment 9 . They thus effectively delegitimize sociocultural stigma attached to mental health problems and pave the way for micro-level changes.
Available tools 10 like Nod (to address loneliness in college campuses using positive psychology, cognitive behavioral therapy and mindfulness), 7 Cups (anxiety and stress chat for emotional support) or Your DOST in the Indian context (“dost” means friend; counselling to overcome emotions) are interventions dealing with emotional distress among young people. Others like Healthy Minds (free meditation/mindfulness tool to develop the skill of well-being), InsightTimer (guided meditations for sleep, anxiety and stress), Smiling Mind (meditation/mindfulness app) and UCLA Mindful App (free mindful app by University of California Los Angeles Mindful Awareness Research Centre) focus on wellbeing, targeting audience that are not necessarily suffering from stress, loneliness, anxiety, or depression. These interventions are specifically meant for mental health, whether on the wellness or illness sides of the continuum. The problem that our study attempts to investigate concerns the effectiveness of an intervention in situations where students are in a state of denial of their mental illness, primarily because there is a strong perception of societal stigma attached to mental health problems. To the best of our knowledge, such interventions are not widely available, if at all, in India or elsewhere at the moment.
Finally, it is important to note that the Cocoon platform was designed and developed over a period of time lasting many months, and it went through several rounds of pretesting that involved showing the prospective users a version of the intervention, taking their feedback through a series of in-depth qualitative interviews and two focus-group discussions, and incorporating the collected feedback in the final design. This further included assessing the appeal of the Cocoon idea, its imagery, its name, and its various taglines that accompanied the offered services. However, the pretesting part was not conducted on the respondents that subsequently provided quantitative data for the present study. We did not, therefore, ask follow-up questions about Cocoon to this particular sample of respondents during the comparative testing with Site 1 and Site 2. We have refrained from including these results in the present paper, but they are available upon request.
Future Directions
The present paper provides a glimpse of our ongoing study on the integration and inclusion of individuals who feel severely stigmatized as a result of their depressive mental conditions. The work, its encouraging results notwithstanding, does leave room for further investigation in the future. It is important to remember that a single intervention of this nature is usually insufficient to bring about systemic changes that are required to deal with wicked problems of high complexity (Kemper & Ballantine, 2017). In fact, multilevel inventions are recommended at macro (society), meso (community), and micro (individual) levels. Our SSM intervention lays the basic groundwork for building such multilevel interventions.
Footnotes
Acknowledgements
The authors wish to acknowledge and thank two anonymous reviewers of Social Marketing Quarterly for many insightful comments as well as for suggesting a number of improvements in the paper. Thanks are also due to our students Kritika Prakash and Aashi Mittal for collecting data and building the web platform.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.