
Abstract
Objective:
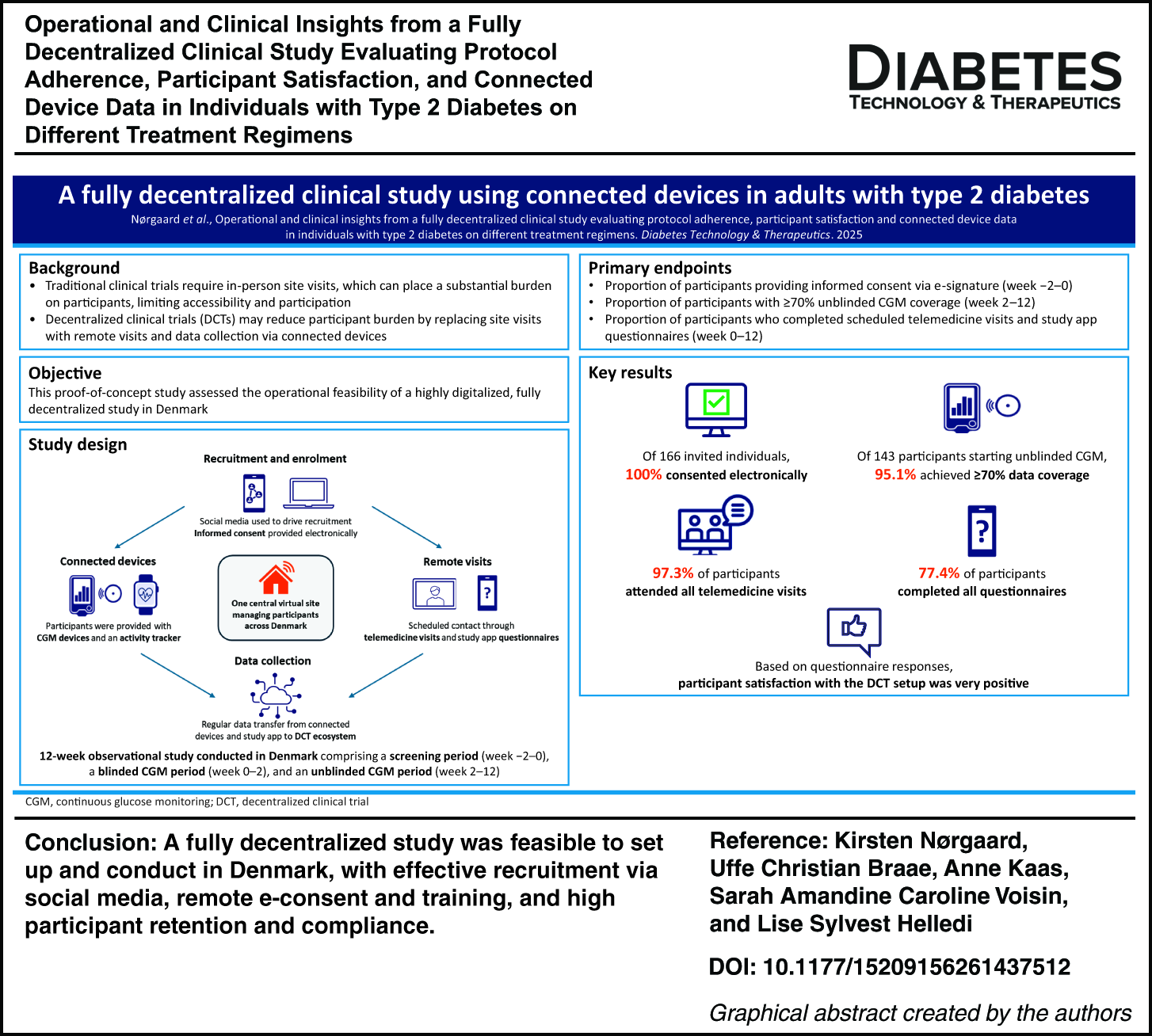
Traditional clinical trials place a substantial burden on participants owing to the need for frequent, tightly controlled site visits, which can limit access and participation. Advances in digital health allow for decentralized clinical trials (DCTs), with site visits replaced by virtual contact and data collection, potentially reducing burden and broadening access. This proof-of-concept study assessed the operational feasibility of a fully remote, digitalized DCT.
Methods:
This was a 12-week observational study conducted in Denmark; adults with type 2 diabetes were recruited via social media. Following e-consent, participants were provided with continuous glucose monitoring (CGM) devices and an activity tracker, with data collected via smartphone apps. All visits and support were conducted remotely. Primary endpoints were: proportion consenting via e-signature (weeks −2 to 0), proportion with ≥ 70% unblinded CGM coverage (weeks 2–12), and percentage of scheduled telemedicine visits and questionnaires completed (weeks 0–12). Safety was monitored remotely through adverse event (AE) reporting during telemedicine visits.
Results:
Most study places were filled within 2 days of advertisement. Of 166 invited individuals, 100% consented electronically; 156 were enrolled, and 87% completed the study. Among participants starting unblinded CGM, 95% achieved ≥70% data coverage, meeting international completeness standards. Adherence to remote interactions was high: 97% attended all telemedicine visits, and 77% completed all questionnaires; 72% completed all scheduled remote interactions. Satisfaction with the study and CGM devices was very high, although adherence to the activity tracker was low (12% with ≥70% coverage) owing to technical issues. Safety monitoring via remote AE reporting revealed no unexpected findings.
Conclusions:
A fully remote study was feasible to set up and conduct in Denmark, with rapid recruitment, high retention, and high compliance with CGM and telemedicine visits. DCTs have the potential to reduce participant burden, improve recruitment, and increase the representativeness of clinical trial populations.
Keywords
Get full access to this article
View all access options for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.