
Abstract
The current legislative framework for the provision of health care in the Nigerian correctional system is the Nigerian Correctional Service Act (2019). The alignment of this framework with international best practice in prison mental health care has not been examined to date. This document review critically appraises the act regarding its capacity to deliver sustainable prison mental health care by comparing its provisions and operating protocol with illustrative standards for prison mental health services. We identified important gaps in assessment during reception, treatment planning, and referral processes; medication management; 24-h healthcare provision; patient safety; environmental adequacy; workforce and collaborative arrangements; and the overall governance mechanisms for the delivery of mental healthcare in the corrections system. Despite its fledgling implementation, the current statute, with its protocol, requires relevant amendments to establish clearer provisions for mental health care delivery to those in prison.
Introduction
Low and middle-income countries (LMICs) contribute close to 70% of the world's incarcerated population (Baranyi et al., 2019; Gureje & Abdulmalik, 2019). Nigeria is the most populous African nation and one of its largest economies (Nigerian Investment Promotion Commission, 2021; Whiting, 2019), with a prison population rate of 37 per 100,000 (Institute for Crime & Justice Policy Research, 2023b) (Figure 1 provides a brief country profile for Nigeria). There are 240 holding facilities within the Nigerian Correctional Service (NCoS) housing slightly over 80,000 inmates (Institute for Crime & Justice Policy Research, 2023b; Nigerian Correctional Service, 2023) in overcrowded conditions. The Nigerian prison population rate is considerably less than that of the US (531/100,000), South Africa (258/100,000), and the UK (England and Wales) (146/100,000) (Institute for Crime & Justice Policy Research, 2023a). However, a larger proportion of inmates are on remand awaiting trial (68% of the total population of inmates, compared to 23.3% in the US, 35.6% in South Africa, and 18.1% in England and Wales) (Institute for Crime & Justice Policy Research, 2023a). This combination of a relatively low imprisonment rate and a high proportion of inmates on remand could be due to law enforcement and judicial processes undermined by systemic underfunding, corruption, process inefficiency, and infrastructural inadequacies (Ajah et al., 2022; Igwe & Faga, 2024; Onah et al., 2022).
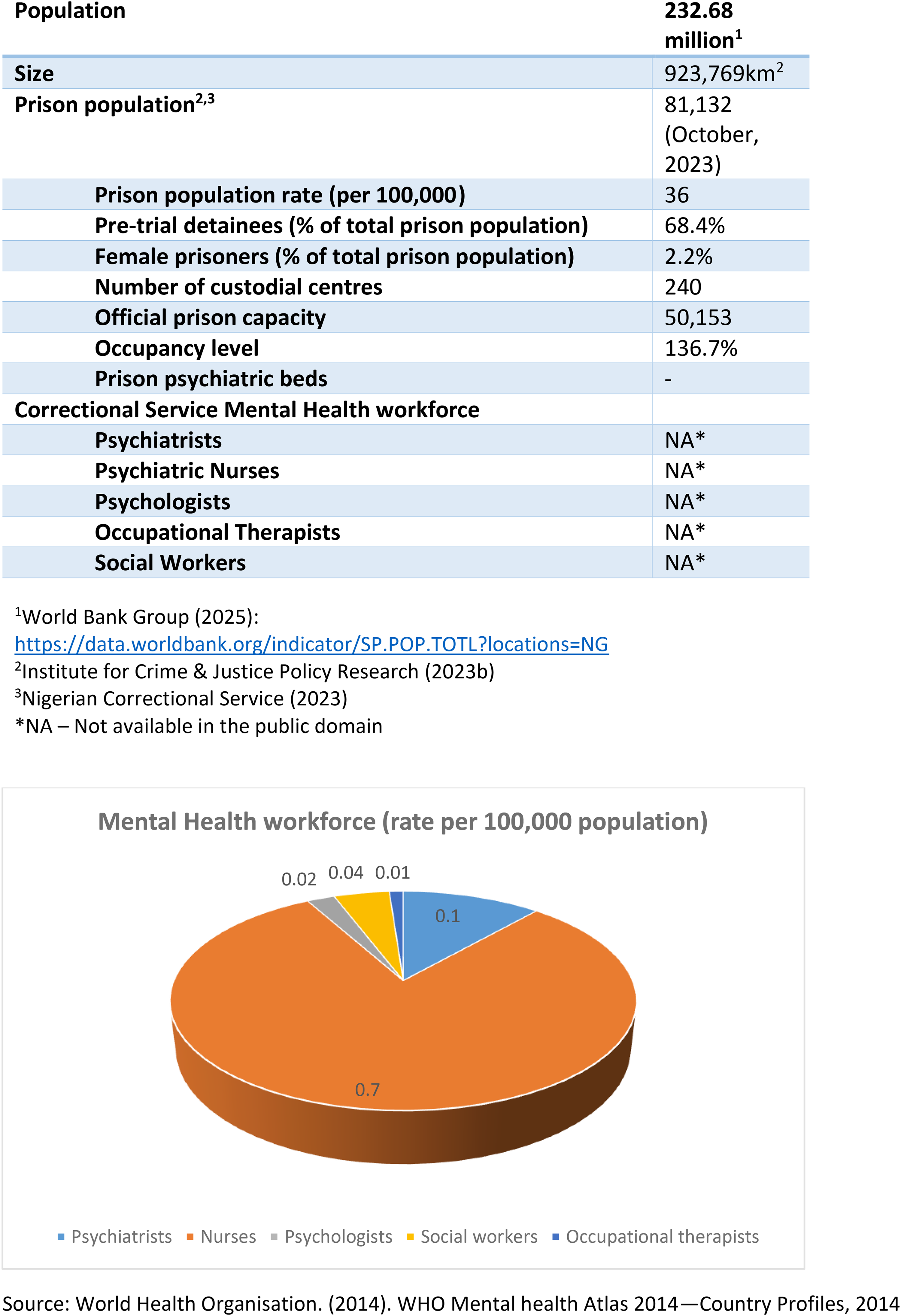
Country profile – Nigeria.
Higher rates of mental disorders among incarcerated individuals than in the general population have been documented across the globe (Emilian et al., 2025; Lovett et al., 2019), including Nigeria (Abdulmalik et al., 2014; Armiya’u et al., 2013). However, while there is a clear statutory duty of prisons in Nigeria to provide both physical and mental health care (Laws of the Federation of Nigeria, 2004), correctional mental health services are virtually non-existent. There are very few psychiatrists, psychiatric nurses, and other relevant mental health professionals within the country (see Figure 1) and specifically within correctional services (Ogunwale et al., 2020; United Nations Office on Drugs and Crime, 2022).
One of the critical pillars for improving prisoners’ health is the development of policy and legislative frameworks for prison health (World Health Organisation, 2020). The current legislative framework for the provision of services in the Nigerian prison system, the Nigerian Correctional Service Act (2019) (NCoSA), was largely driven by a paradigm shift from a punitive to a rehabilitative approach to imprisonment in an attempt by the government to conform with international best practice (Nigerian Correctional Service, 2023). It was intended to better address the welfare needs of incarcerated persons and to provide for non-custodial measures such as community sentencing, probation, parole, and restorative justice measures (Nigerian Correctional Service Act, 2019). The NCoSA is a clear improvement upon the earlier Prisons Act (Laws of the Federation of Nigeria, 2004) in terms of its more detailed provisions on the reception documentation of inmates, prison healthcare services, managing inmates’ mental health, and the involvement of a mental health review board in the evaluation of medical recommendations regarding inmates’ mental illness (see Figure 2).
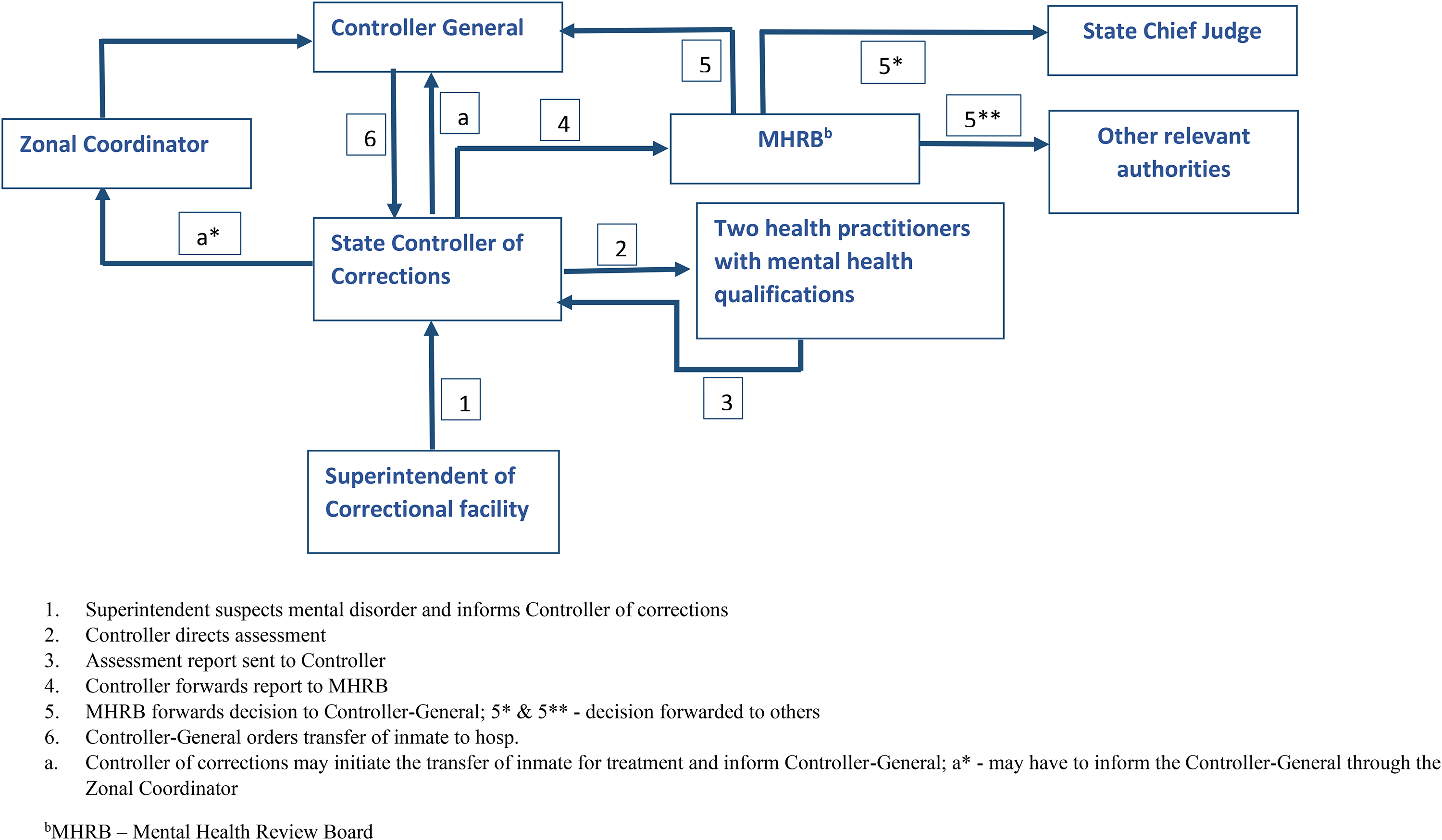
Mental health assessment, certification, and hospital transfer process under the Nigerian Correctional Service Act (2019).
A guidance document based on the NCoSA, the Operational Protocol and Guidelines for Managing Inmates with Mental Illness within the Criminal Justice System (OPGMICJS) was produced in 2022 by the NCoS (Nigerian Correctional Service, 2022). It has 10 broad sections divided into specific guidelines, covering mental health assessment and treatment, referral, transfer/diversion from the correctional service, substance abuse treatment, governance, non-custodial alternatives, and data management in the criminal justice system.
This study aimed to examine the capacity of the NCoSA, with its companion OPGMICJS, to deliver sustainable prison mental health care in Nigeria by comparing its provisions with the representative UK Standards for Prison Mental Health Services (SPMHS-UK) (Royal College of Psychiatrists, 2023). The decision to compare the NCoSA with the SPMHS-UK is based on their shared history in terms of the development of correctional and mental health services (Ogunlesi & Ogunwale, 2018; Saifulahi-Idris et al., 2021). The Nigerian mental health and penal systems were established during the colonial era, thereby indicating a strong British influence on prison standards right from inception (Ogunlesi & Ogunwale, 2021; Otu, 1999). A recent bilateral agreement between Nigeria and the UK in 2014 on international prisoner transfer, with requirements for the Nigerian correctional system to meet UK standards, also suggests ongoing British influence on standard-setting within the Nigerian correctional environment (Adepegba, 2022; Mulgrew, 2011). This influence is subtly underpinned by the UK government's project-specific funding for prison reform in Nigeria (Nigerian Correctional Service, 2022). Additionally, the SPMHS-UK was produced by mental health professionals with experience in the prison healthcare system in a more developed country and could serve as a template for practice in an emerging economy like Nigeria, even though there may be contextual differences.
Methods
This study adopts a document review (also called document analysis) approach, which is commonly used in policy research (Dalglish et al., 2021; Dheensa & Feder, 2022). Document review is a systematic method of reviewing or evaluating documents and is useful for providing context, generating research questions, and supplementing other types of research (Bowen, 2009). The NCoSA and OPGMICJS were reviewed with the SPMHS-UK as a benchmark, and this analysis is presented in Table 1 (Supplementary Material). The SPMHS-UK has 11 categories, each with specific standards, as highlighted in the evaluation section of this paper. The standards are broadly consistent with the United Nations Standard Minimum Rules for the treatment of Prisoners (United Nations, 2015b). Only a summary of the representative standards under the SPMHS-UK is provided as the analytical framework.
An interpretive approach to all the documents was favoured over rigid textual analysis given potential contextual variations between the correctional systems in Nigeria and the UK. This document analysis assumes a ‘black letter’ position whereby the focus is on the content rather than the demonstrable impact of the legislation with its operating protocol (Kelly, 2011).
Evaluation of the NCoSA and OPGMICJS Using the SPMHS-UK Framework
Reception and Assessment
The SPMHS-UK focuses on multi-stage screening by professionals competent in assessing common mental health problems, a standardised assessment format, adequate medical history-taking with access to medical records, risk assessment, clear communication, and referral to specialist teams where necessary. Section 13 of the NCoSA addresses the documentation of the inmate at reception, under which the correctional superintendent ‘may’ rely on ‘relevant professionals’ in determining the inmate's mental state or physical health. Guideline 2(1–9) of the OPGMICJS specifically addresses mental health assessment of inmates, mandating mental health screening as part of reception procedures. The focus is on the use of screening instruments such as the General Health Questionnaire version 12 (GHQ-12) (Goldberg, 1972) and Patient Health Questionnaire (PHQ-9) (Kroenke et al., 2001), and greater emphasis is placed on psychological assessment, substance use disorders, and suicidal behaviour.
Like the SPMHS-UK, the NCoSA, with its OPGMICJS, makes provision for mental health screening in a standardized format. It also provides for referrals to mental health professionals. However, in contrast to the SPMHS-UK, which requires a two-stage screening process by professionals competent in recognising common mental health problems, the NCoSA and OPGMICJS make no mention of the professionals’ competence. Furthermore, the NCoSA and OPGMICJS do not provide specific guidance on the availability of inmates’ medical records during reception assessment, effective communication with inmates about their health needs or rights, or the substantial attention to risk assessment and discussion during reception screening. Comprehensive risk assessment appears to be deferred to the stage of further assessment by a mental health professional and treatment planning, even though assessment for suicidal behaviour is mentioned by the OPGMICJS at reception.
Treatment and Recovery
Key standards in the SPMHS-UK under the treatment and recovery include stepped care, providing information to patients, co-production of written care plans with patients, regular team meetings, liaison between mental and physical healthcare providers, and inter-agency working. Others refer to collaborative management of suicidal behaviour, evidence-based pharmacological and psychological care, perinatal care provision, and adequate patient follow-up. Stepped care involves the organisation and integration of multiple mental health services along a continuum of support to provide appropriate intervention intensity based on individual need (Mughal et al., 2023; National Institute for Health and Care Excellence, 2011). Section 23 of the NCoSA directs the NCoS to develop services for mental and physical health. Specific provisions indicate that doctors from the state or federal civil service should provide healthcare when no medical doctors are available in a particular prison. The prison superintendent is required to report cases of mental illness in inmates to the State Controller of Corrections following a clear procedure (see Figure 2).
The OPGMICJS directs further assessment of a mentally ill prisoner by a ‘mental health professional’ post-screening. The level of training or expertise of the mental health professional is not stipulated in the guidelines. This assessment is to be conducted within 2–4 weeks of admission to prison, and the need for individualised, multidisciplinary care that respects the patient's autonomy is duly emphasised. Risk assessment and provisions for transfer to specialised services, as well as transition out of prison and aftercare, are highlighted. Guidelines 10 (4–6) focus on the mental health of pregnant women and their readiness for delivery and childcare.
Consistent with the SPMHS-UK, the NCoSA, with the OPGMICJS, envisions a multidisciplinary team approach to care. Federal or state government authorities’ involvement in providing medical support for mental healthcare in prisons may be regarded as consistent with the UK standard of inter-agency working. Collaborative management of suicidal behaviour is addressed, but under a different standard of the SPMHS-UK (‘safety’) considered below. The OPGMICJS specifically covers perinatal mental health.
In contrast to the SPMHS-UK approach, the duration of further assessment for the inmate is substantially longer (2–4 weeks versus 24–48 h). The NCoSA and OPGMICJS do not follow the recommended stepped-care model of mental healthcare. While there is provision for ‘regular mental health assessment’ in the OPGMICJS, there is no clear plan for sustainable multidisciplinary team engagement or co-production of treatment plans with inmate-patients. There is also no clear emphasis on the liaison between physical and mental healthcare providers. There are no detailed guidelines for evidence-based pharmacological and psychological care or for follow-up plans, although the importance of ‘individualised care’ is stressed in the OPGMICJS.
Discharge and Transfers
The SPMHS-UK standards under this category cover referral policy, comprehensive handover, inter-service collaboration, guidelines for community referral, and post-referral contact within 14 days. In the NCoSA, Section 24 permits the state controller to order the transfer of the patient to another custodial centre or hospital for treatment under its terms and those of the National Mental Health Act (2021) until recovery has been certified by the Mental Health Review Board (MHRB). It also covers the return of the inmate to prison to complete his term or the detention of the inmate in a non-secure psychiatric hospital under mental health legislation pending the determination of the sentence of imprisonment.
As shown in Table 1, the OPGMICJS outlines the need to transfer the inmate's assessment records to other correctional centres as necessary. The OPGMICJS also stipulates post-hospitalisation arrangements to connect patients with mental health services, thereby ensuring access to treatment outside the correctional system. While monitoring their care is the responsibility of the MHRB, the procedure for this is unclear, as there is no requirement for the treating physician to issue any periodic reports to the MHRB. Rather, reports are to be issued to the prison authorities. However, it appears that under section 24(5)(b) of the NCoSA, the MHRB is also expected to have such reports and certify return to custody once the inmate recovers.
Under the OPGMICJS, discharge planning from the hospital is required to be led by the ‘correctional service psychiatrist’ in collaboration with the treating psychiatrist who is not employed by the correctional service. In agreement with the SPMHS-UK, the NCoSA, with the OPGMICJS, provides analogous details on referral policy, comprehensive handover to and collaboration with the receiving service, and some degree of post-referral contact. However, while in the SPMHS-UK, it is expected that the post-referral contact should be made within 14 days, there is no stipulated timeframe under the NCoSA or the OPGMICJS. One omission in the Nigerian framework is the lack of clear guidelines for community referral.
Safety
The key considerations under safety in the SPMHS-UK have to do with the prevention of self-harm or suicide and the physical healthcare of the mentally ill inmate. Under sections 13 and 23 of the NCoSA, the facility superintendent is expected to consider the severity of illness before admitting a person to prison and to ensure safe and sanitary conditions during imprisonment. Guideline 3(9) of the OPGMICJS recommends appropriate supervision of inmates with mental illness, as well as considerations of their safety based on risk assessment for violent victimisation and self-harm when cells are allocated to them.
In contrast to the UK standards, there is insufficient mental health team involvement in safety planning for inmate-patients under the NCoSA or the OPGMICJS. There is no clear information on staff safety considerations or on interagency communication regarding safety-related issues. The NCoSA and OPGMICJS are silent on the processes to follow in safeguarding, even though there are general safety considerations. Safeguarding has been defined as ‘protecting people's health, well-being and human rights, and enabling them to live free from harm, abuse and neglect’ (Care Quality Commission, 2022). Other aspects related to safety in which the NCoSA and OPGMICJS seem to be inadequate include clear provisions on food refusal and associated capacity assessment, as well as information sharing about serious offenders.
Patient Experience
This includes patient involvement in care and treatment, providing opportunities for feedback, and treating patients with compassion, dignity, and respect. Consistent with the SPMHS-UK standards, feedback under the NCoSA and the OPGMICJS is covered. Inmates may file complaints with official visitors to their custodial facilities, who are appointed under the NCoSA. These visitors are senior state and federal judicial officers, and members of the National Human Rights Commission, among others. Under the OPGMICJS, such complaints may be made to the medical officer or mental health professional in charge of the custodial centre and, if not satisfactorily addressed, escalated to the MHRB, the Controller of Corrections, or the Controller-General of Corrections.
Collaborative Partnerships
Collaborative partnerships in the SPMHS-UK include inter-agency working, regular multi-pathway meetings, policy on reporting intelligence through the security reporting system, support for mental health awareness training for prison staff, and a joint working protocol between in-prison specialists and the mental health team.
The NCoSA and the OPGMICJS mention collaborative partnerships with state governments, community mental health care providers, and Non-governmental Organisations (NGOs) in providing mental health services to inmates. Section 33(2) of the NCoSA provides for specialised civil society groups interested in human rights and justice reforms to serve in an advisory capacity to the Controller General. Mental health training is partially covered under Guideline 5(8) of the OPGMICJS. Even so, the NCoSA and OPGMICJS do not sufficiently address areas such as regular multi-pathway meetings and policies on reporting intelligence according to security reporting systems as specified in the UK standards.
Medication Management
Within the SPMHS-UK, critical considerations include specific treatment goals for patients, audits of the safe use of high-risk medications, monitoring of psychotropic prescribing rates, annual medication reviews, medication adherence monitoring/records, and protocols guiding prescribing roles. The NCoSA and its OPGMICJS have no clear provisions on medication management in prison.
Environment
The conceptualisation of the environment under the SPMHS-UK addresses issues such as safe, welcoming interview rooms; consultation spaces that ensure confidentiality; the availability of therapy rooms; and the provision of IT resources to support both clinical and administrative information sharing. Neither the NCoSA nor the OPGMICJS addresses environmental provisions for mental healthcare directly.
Work Force
The SPMHS-UK contains workforce-related standards such as multidisciplinary team arrangements, safe staffing mechanisms, specialists’ input (mental health and pharmacy), and appropriate clinical leadership. Others include staff support (well-being), role-relevant training (induction programmes), trauma-informed care, safe working conditions, and reflective practice.
Guideline 5(8) of the OPGMICJS provides for the training of correctional staff in substance abuse with a focus on assessment, psychological intervention, substance use counselling, and peer counselling. This represents some forms of role-relevant training. However, compared with the SPMHS-UK, the NCoSA and its OPGMICJS do not clearly address safe staffing mechanisms, staff support and well-being, trauma-informed care, clinical supervision, safe working conditions, and reflective practice.
Leadership and Governance
Within SPMHS-UK, leadership and governance standards address the involvement of mental health teams in prison clinical governance, patient involvement in governance, and the adequate dissemination of policies, procedures, and guidelines. Other standards in this category include data governance, quality improvement, incident reporting, and complaints processes.
The analogous structure meeting this standard under the current NCoSA is a Mental Health Review Board (MHRB), which is established for each state and the Federal Capital Territory (FCT). The board comprises a psychiatrist (chair), a psychologist, a social worker, a representative of psychiatric hospitals in the state, and prison medical personnel. Guideline 6 of the OPGMICJS expands on the provision establishing the MHRB by clearly spelling out its functions to include policy making, mental health assessment review, certification of cases, mental health promotion and illness prevention initiatives, stigma reduction, relevant oversight of correctional mental health facilities, and coordination of activities involving local neuropsychiatric hospitals. Figure 2 illustrates the critical role of the MHRB in the review and certification of suspected cases of serious mental disorder among prison inmates.
Section 33 of the NCoSA permits the controller-general to make regulations and standing orders. The procedures for incident reporting and the process for raising concerns about standards of care may be partially covered in the NCoSA by its provisions on inmates’ complaints to official visitors. Aligning with the SPMHS-UK standards, guideline 7 of OPGMICJS covers data collection and management, including diagnoses and medication data. Quality improvement processes and support for research relevant to correctional mental health are not directly addressed in the NCoSA or OPGMICJS. Patient involvement in the governance framework is not provided for in the NCoSA and OPGMICJS.
24-h Mental Healthcare
Here, the SPMHS-UK highlights the agreed operational policy on admission, the availability of medical staff at all times (including out of hours), and safe staffing levels across shifts, with at least one qualified nurse on all shifts. 24-h mental healthcare is not directly addressed under the NCoSA or the OPGMICJS.
Discussion
To the authors’ knowledge, this is the first attempt to critically evaluate the relatively new Nigerian correctional service legislation against a set of standards that are arguably consistent with international best practice in prison mental healthcare. Addressing deficiencies in the current care framework has implications for Nigeria's achievement of the sustainable development goals related to promoting global mental health (Jenkins, 2019; Ogunwale & Liebrenz, 2021; United Nations, 2015a), with particular emphasis on mental health in prisons.
From the outset, it is important to note that some cultural factors may affect the applicability of UK standards to the Nigerian correctional system. The current slant of the Nigerian correctional service toward rehabilitation and reformation (Nigerian Correctional Service, 2023) is likely to advance Nigeria's alignment with international best practices in prison mental health care. The emergent parole and probation culture in the Nigerian criminal justice system (Okeke et al., 2024; Onuigbo & Nkolo, 2024) may also support standards that embrace timely assessment and prison diversion schemes. However, a predominant spiritual rather than biomedical model of mental illness in the country, occurring alongside considerable stigmatisation of those with mental disorders (Ogunwale et al., 2023), could prevent inmates with mental health problems from accessing available treatment under the current framework.
Assessment and Treatment of Mental Disorder, Hospital Transfers, and Post-Hospitalisation Issues
The reception assessment process instituted within the NCoSA and OPGMICJS lacks specific emphasis on comprehensive risk assessment and early identification of emergency situations (such as opiate withdrawal or drug toxicity), which should result in appropriate treatment and referral (Okoro et al., 2018; Royal College of Psychiatrists, 2023). Previous research has shown that reception assessment for mental disorders is not common in Nigerian prisons (Olagunju et al., 2018), with significant implications for the mental health treatment gap in prison (Olagunju et al., 2024). Such gaps contribute to reductions in quality of life (Fakorede et al., 2021) and other adverse outcomes such as interpersonal violence, violent victimisation, and suicidal behaviour (Caravaca Sánchez & Wolff, 2016; Facer-Irwin et al., 2019; Favril et al., 2020).
The use of screening instruments, though recommended, is fraught with the risk of false positives and poor case identification (Robinson et al., 2012; Senior et al., 2013). Limitations in the validity of screening instruments must be borne in mind when focusing on collecting a minimum amount of relevant information, identifying priority conditions, and highlighting disease risk factors (Grubin, 2010; Patel et al., 2018). Screening should be followed by triage based on risk assessment, thereby establishing a sequence of screening, triage, assessment, intervention, and reintegration (Forrester et al., 2018). Appropriately trained specialist or non-specialist staff are also required (Jack et al., 2025) for ensuring validity of assessments.
Mental health screening at the early stage of imprisonment could potentially promote prison diversion schemes following a sequential intercept model (Adjorlolo, 2016; Munetz & Griffin, 2006; United Nations, 2015b). This may help in curtailing the over-representation of mentally ill offenders in Nigerian prisons. This should not be limited by risks to self or others as currently envisaged by the OPGMICJS (Nigerian Correctional Service, 2022; guideline 9(1–6)) as such risks are recognised and manageable in in-patient psychiatric settings. The duration of further assessment is set at 2–4 weeks, which risks being indeterminate and increases the likelihood of morbidity and mortality due to missed opportunities for structured intervention (Fazel et al., 2016; Forrester et al., 2018).
In treatment, a stepped care model is efficient and effective (National Institute for Health and Care Excellence, 2011) and should be embraced by the NCoSA with the OPGMICJS. Communication with patients and patient involvement in their care, with their rights respected, are important with implications for the coproduction of care packages (Cunningham & Wakeling, 2022).
The main ethical challenge with physicians in the correctional system making discharge decisions after offenders’ hospitalisation is the allocation of clinical responsibility. The treating psychiatrist should assume responsibility for discharge (Medical and Dental Council of Nigeria, 2008). Furthermore, the involvement of doctors under the state or federal ministry of health to care for mentally ill prisoners where correctional service physicians are lacking may be infeasible since they are not employees of the correctional service. Some form of devolution of prison healthcare to state and federal ministries of health may be warranted, as seen in prison in-reach services elsewhere (Steel et al., 2007).
Regarding inmates’ security during hospital transfers, although the NCoSA imposes no specific statutory liability on medical officers or other hospital staff for an incarcerated individual's escape from hospital, such incidents are likely to lead to unwarranted scrutiny of hospitals by the correctional system and other agencies. As there are currently no secure psychiatric hospitals in Nigeria (Ogunlesi & Ogunwale, 2018), this may lead to a refusal to accept such patients without specific, personalised security arrangements by the correctional service, as implied in section 25 of the NCoSA. Psychiatric hospitals in Nigeria exercise discretion in deciding which offenders to accept for hospital care, as there is no law mandating that they accept all patients, except in an emergency (National Health Act, 2014). This tension between security concerns and healthcare delivery can be resolved through effective collaboration among the ministries of the interior, justice, and health at all levels.
Community referral post-incarceration should be addressed clearly in amendments to the NCoSA or updates to the OPGMICJS, as it has implications for continuity of care post-imprisonment or during parole (Hu et al., 2020; Jarrett et al., 2012). The American APIC model for planning community transitions from incarceration, encompassing
Involuntary Treatment in Prison
Despite the vulnerability of incarcerated individuals, the NCoS and OPGMICJS are silent with regard to involuntary treatment in prison, although current opinion is divided on this (Carroll et al., 2021; Davies & Dimond, 2012; Simpson, 2003; Spencer & Dean, 2019; Wilson, 2012). Similarly, the Nigerian Mental Health legislation (Mental Health Act, 2021) does not provide a clear framework for the compulsory treatment of mentally disordered offenders within prison settings. Part IV of the Mental Health Act provides for the compulsory treatment of mentally disordered offenders (without location specified and prison not excluded) or involuntary treatment in a mental health institution. It may be suggested that the standards of necessity and proportionality 1 could apply in such situations. Human rights cases adopting a common law approach (Qurashi, 2003) from other jurisdictions provide guidance in this respect. 2 This approach, with appropriate safeguards and service enhancements (Spencer & Dean, 2019), could be carefully considered in amending the NCoSA with its OPGMICJS, given the country's limited mental health resources.
Patient Safety and Medication Management
There is insufficient involvement of the mental health team in safety planning for inmate-patients (McFadzean et al., 2023), and gaps exist in safeguarding processes (Foster, 2024), food refusal policies (Cumming, 2024), and information sharing about serious offenders and staff safety. Additionally, establishing an appropriate liaison between physical and mental healthcare would strengthen the equivalence of care (Edge et al., 2020). Equivalence of care is the principle whereby persons detained must receive healthcare equivalent to that dispensed to the general public in the same country (Niveau, 2007). The NCoSA and OPGMICJS need to be amended to sufficiently address these issues.
Medication is supervised by correctional healthcare workers during the working day, with little staff support for self-administration outside clinic hours. A more sustainable approach may be to place some consenting psychotic patient-inmates on long-acting injections, which demonstrate substantial effectiveness in relapse prevention (Kim et al., 2020; Kishimoto et al., 2014).
Processes (e.g. close monitoring during initiation of medication) to ensure early identification of side effects, poor compliance with medication, and drug-drug interactions (Royal College of Psychiatrists, 2023) should be established. Prescribing patterns in prison mental health care need to be monitored to improve practice and achieve rational prescribing (Royal College of General Practitioners, 2019; Royal College of Psychiatrists, 2023). The use of medications that may be highly toxic in overdose should be adopted with caution when patients self-administer them (Royal College of General Practitioners, 2019).
Environment
There are architectural, therapeutic, and utility considerations in designing mental health treatment settings in prison (López & Maiello-Reidy, 2017). These factors include simple spatial orientation, adequate lighting, outdoor spaces, appropriate acoustics, fit-for-purpose furnishing (López & Maiello-Reidy, 2017), and connection to nature (Söderlund & Newman, 2017). The SPMHS-UK recommendations on safe and welcoming therapy spaces, confidentiality considerations, and the provision of IT utilities for clinical and administrative information sharing are apt and should serve as a practical guide for updating the OPGMICJS to meet environmental standards.
Governance and Human Resource Management
The MHRB is currently expected to issue its report independently to the Controller-General, the state Chief Judge, and ‘other relevant authorities’. This multilateral approach to issuing reports may lead to contradictory directives from different authorities. Additionally, its relationship to the newly established parole boards (British Council, 2022), which also consider mental health issues during parole, needs to be well defined to avoid undue role overlaps.
Given the shortage in mental health human resources in the country and within correctional services in particular, there is a need for the NCoSA and OPGMICJS to embrace a task-shifting and integrative approach to mental health service provision (Adebowale et al., 2014; Adebowale et al., 2018; Gureje et al., 2015; Jack et al., 2025; Ogunlesi & Ogunwale, 2018). Supporting the prison estate in establishing mental health awareness training for its staff will also be helpful in this regard (Darani et al., 2023; Parker, 2009). Additionally, establishing mental health wings within correctional facilities should be considered in legislative amendments to ensure 24-h mental health service coverage, with a note of caution to avoid unlawful involuntary treatment (Carroll et al., 2021). Currently, the medical wings in Nigerian prisons are skewed towards the provision of physical healthcare without dedicated psychiatric beds (Laws of Nigeria, 1948).
Funding for healthcare, including mental health in correctional settings, is only tangentially addressed in the NCoSA and the OPGMICJS. This is disadvantageous to health care planning, including hospital transfers. Mentally ill incarcerated persons could potentially benefit from the mental health fund established under the Nigerian Mental Health Act, as well as the ‘vulnerable group fund’ under the new National Health Insurance Authority Act (2022). In terms of patient experience, more proactive feedback (rather than complaints) from inmate-patients will be desirable to better plan services (Lovett et al., 2019) and facilitate quality improvement.
Limitations
Our study has limitations that should be considered when interpreting its findings. This review was based on psychiatrists’ perspectives on the adequacy of mental health-related legislation and guidelines in a correctional system. Thus, the authors might not have been entirely value-free in their critiques. Despite the relevance of the SPMHS-UK to the Nigerian context, it is not necessarily the gold standard internationally, and its comparison with the NCoSA and OPGMICJS might have nuanced utility in certain aspects, which may have variable salience across settings, e.g. inmate involvement in mental health governance and IT access in the prison healthcare environment. The authors were ‘outsiders’ to the correctional system, which could have strengthened their analytical objectivity. However, some of our critiques might have been driven by a fractional understanding of what is currently realistic within the Nigerian correctional system.
Conclusion
The current legislative framework for the provision of mental health care in the Nigerian correctional system is a useful first step to improving inmates’ access to improved correctional mental healthcare. However, using the SPMHS-UK as our evaluative template, we have identified important gaps in the areas of assessment during reception, treatment planning and referral processes, medication management, 24-h healthcare provision, patient safety, environmental adequacy, workforce and collaborative arrangements, and the overall governance mechanism for the delivery of mental healthcare in the corrections system, which require addressing. These clearly provide an impetus for legislative and executive action in terms of practical implementation as well as future amendments to offer inmates sustainable mental healthcare during the frequently difficult conditions of incarceration. Imprisonment continues to provide a treatment opportunity for the mentally ill who might not have been otherwise treated in the community and confers significant public health benefits in terms of reductions in both health inequality and recidivism.
Supplemental Material
sj-docx-1-fmh-10.1177_14999013261426018 - Supplemental material for Mental Health Care in Nigerian Prisons: A Practice-Based Critique of the Current Legal Framework
Supplemental material, sj-docx-1-fmh-10.1177_14999013261426018 for Mental Health Care in Nigerian Prisons: A Practice-Based Critique of the Current Legal Framework by Adegboyega Ogunwale, Deirdre MacManus and Nigel Blackwood in International Journal of Forensic Mental Health
Footnotes
Ethical Considerations
Not applicable.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Author Contribution(s)
Funding
Adegboyega Ogunwale is supported by the PGR International Studentship (2022–2026) of the Doctoral College, King's College London.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
All the data relevant to this publication are available in the public domain.
Supplemental Material
Supplemental material for this article is available online.
Cases
Herczegfalvy v Austria (1992). 15 EHRR 437.
Huang v Secretary of State for the Home Department (2007). UKHL 11.
Keenan v United Kingdom (27229/95) (2001). 33 EHRR 38.
Munjaz v United Kingdom (2913/06) (2012). M.H.L.R 351 ECHR.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.