
Abstract
The difficulties associated with transitioning from prison to the community are well-known, particularly for those with mental illness. Individuals released from prison are high users of public health services, and particularly emergency healthcare, perhaps reflecting poor access to stabilizing or preventative care. This study reports the outpatient, emergency and inpatient health contacts of a sample of men and women recruited from prison reception in New South Wales (NSW), in the 12 months postrelease. Differences in health service utilization by gender, Aboriginal and/or Torres Strait Islander status and the presence of serious mental illness were examined, along with the relationship between health service utilization and reoffending. A high rate of postrelease health service use and repeated contact with the criminal justice system was identified, with findings particularly pronounced for those identified at prison entry as having serious mental illness. An association was found between accessing emergency services and subsequently being charged with a reoffence, whereas accessing outpatient mental health services had no impact on subsequent reoffending risk. An increased focus on achieving continuity of mental healthcare between prison and the community is required to reduce the burden on public healthcare and correctional systems in NSW.
The postrelease period is one of heightened vulnerability for those exiting prison. The difficulties faced by those transitioning back to the community are reflected in poor health outcomes for this group, exemplified by excess mortality, particularly as a result of drug-related deaths, suicide, and homicide (Zlodre & Fazel, 2012). High levels of drug and violence-related morbidity (Keen et al., 2020; Willoughby et al., 2022) have also been reported. For many, the challenges of reintegration prove insurmountable. In NSW, Australia, nearly half of all people released from prison are reincarcerated within 2 years (Australian Productivity Commission, 2021), and Australia has the highest reincarceration rate internationally among countries for which these data are available (Yukhnenko et al., 2020).
One such challenge is navigating the health system. Difficulties experienced in the early postrelease period are likely to impact on health service utilization and, in particular, utilization that reflects the occurrence of health crises and the need for emergency care rather than regular maintenance and preventative care. Emergency health service utilization (e.g., ambulance callouts and emergency department attendance) is much greater for those transitioning from prison to the community than seen in the general population (de Andrade et al., 2019). International research from Canada and the United States of America has found that inpatient admissions for any reason are also common among those recently released from prison, particularly within the first week (Kouyoumdjian et al., 2018; Wang et al., 2013). One study found that one-fifth of adults released from prison in Western Australia over a two-year period had an inpatient admission in the year following release, almost twice the rate of the general adult population of the same age (Alan et al., 2011).
The conditions of crisis and instability that may lead a person to seek emergency healthcare or to require an inpatient admission are likely to be the same conditions that put them at risk of reincarceration. A US study found that early emergency department attendance among those released from prison was associated with subsequent reincarceration (Frank et al., 2013), and similarly, an Australian study found that this was particularly the case for those with four or more emergency contacts within 3 months of release (de Andrade et al., 2019). As such, the identification of those at risk of early and frequent health service contacts postrelease from prison may assist in identifying who will benefit most from targeted efforts to improve the continuity of healthcare during the transition from custody to the community.
Mental Illness and Postrelease Health Service Utilization
More than two-thirds of those interviewed on release from prison in Australia report a previous diagnosis of mental illness (Australian Institute of Health and Welfare, 2019), and research clearly shows that the presence of mental illness can be a significant barrier to community reintegration. Internationally, those exiting prison with mental illness tend to experience worse physical and mental health outcomes, are more likely to return to substance use, and often experience difficulties securing accommodation and employment (Cutcher et al., 2014; Mallik-Kane & Visher, 2008). They also have higher rates of reoffending and reincarceration (Baillargeon et al., 2009; Cloyes et al., 2010; Stewart & Wilton, 2014). Hospital admissions for mental health reasons among those released from prison are particularly high (Hobbs et al., 2006). Furthermore, individuals recently released from prison who present at emergency departments are more likely to do so for mental health reasons than those within the community (Frank et al., 2013). Emergency health service utilization for self-harm is also high. Studies of those released from prison in Queensland, Australia by Borschmann et al. (2017a, 2017b) found elevated rates of ambulance attendance for self-harm, as well as emergency department presentations for self-harm at a rate ten times that of the general population.
High rates of emergency or acute health service utilization in the early postrelease period have been argued to result from a lack of access to community-based ambulatory, or outpatient, mental health services for this group (Frank et al., 2013; Kouyoumdjian et al., 2018). The few Australian studies that have examined the continuity of mental healthcare following release from custody have found it to be lacking; including low rates of postrelease community mental health contacts among those who have mental health needs identified in prison (Browne et al., 2022; Chowdhury et al., 2022). This failure of healthcare continuity to support mental health stabilization, and the increased burden on emergency health services, may also impact on offending outcomes. Among those with mental illness, outpatient mental health service utilization is associated with a reduced risk of reoffending (Constantine et al., 2012; Hawthorne et al., 2012) while emergency health service utilization is associated with increased risk (Constantine et al., 2012).
Differences in Postrelease Health Service Utilization by Gender and Aboriginal/Torres Strait Islander Background
There is evidence that health service utilization postrelease from prison differs between demographically defined groups. Women have been found to have higher rates of emergency healthcare use and inpatient admissions after release than men (Alan et al., 2011; de Andrade et al., 2019). Whereas, in regards to mental healthcare, released women were no more likely than men to require emergency healthcare or inpatient admission (Alan et al., 2011; Frank et al., 2013). There is less evidence in regard to gender differences in outpatient mental health service use, although the results of one study in the United State (Lovell et al., 2002) suggest that women exiting prison are less likely to access community mental health services than men. These findings are paradoxical given that incarcerated women shoulder a substantially greater burden of mental ill health than incarcerated men (Browne et al., 2023; Tyler et al., 2019).
While the evidence around health service utilization for Aboriginal and/or Torres Strait Islander people (hereafter, Aboriginal) following release from prison is limited, Australian studies have found higher rates of some forms of healthcare postrelease. For example, in Western Australia, rates of inpatient admission postrelease have been found to be higher among Aboriginal people (Alan et al., 2011; Hobbs et al., 2006). In Queensland, Aboriginal people have been found to have elevated rates of hospital attendance for injury (Young et al., 2019), and ambulance attendance for self-harm (Borschmann et al., 2017a). Evidence suggests that such elevated levels of healthcare need for Aboriginal people postrelease from prison are not adequately met. Calais-Ferreira et al. (2022) found Aboriginal people in Queensland were ∼50% less likely than non-Aboriginal people to receive continuity of primary healthcare after release from prison. The mental healthcare needs of Aboriginal people also remain unaddressed. Chowdhury et al. (2022) found that among individuals released following a first diagnosis of psychosis in prison, Aboriginal people were significantly less likely to have a mental health service contact postrelease than non-Aboriginal people.
Although it is clear that the health needs of those released from prison are not being met and that health service utilization is more often in response to the crisis, a full exploration of the relationship between mental illness, key demographics, and health and justice system contact indicators postrelease is required. Much of the research examining postrelease outcomes focus on samples recruited in the period just before release, which misses the group of individuals most likely to experience the revolving door of short-term periods in custody, including those on remand for minor offences (Browne et al., 2022). The current study aims to report outpatient, emergency and inpatient health contacts for a sample of men and women released from prisons in NSW, utilizing a sample recruited at prison entry to address this limitation. The impact of gender, Aboriginal background, and mental illness on health service utilization, as well as reoffending outcomes, within a 12-month follow-up period will be examined.
Methods
Setting and Sample
Baseline data collection for the study was conducted between June 2016 and May 2018 at the Metropolitan Remand and Reception Centre (MRRC) and Silverwater Women's Correctional Centre (SWCC), the main reception centers for men and women entering prison in NSW. During the data collection period, all those entering custody at these centers were identified via an electronic patient administration system and approached for participation, in random order, within 48 hr of their reception. During the recruitment period, 7,685 individuals (6,619 men and 1,066 women) were received into custody across the two centers. Women were oversampled for the purposes of planned stratified analyses; around 25% of women entrants were approached (n = 270) and just under 6% of men (n = 377). Of these, 60 (39 men and 21 women) declined to participate and 245 (108 men and 137 women) were unable to be interviewed due to absence (attending court or appointments) or inability (mentally/behaviorally unsettled or insufficient English). In total, 342 participants gave informed consent and completed the baseline data collection interview (229 men and 112 women). Excluded from the analysis was one participant with missing data and a further five who did not provide consent for data linkage. Of the remaining 336 participants, 319 people (209 men and 110 women) who were released and had reached the 12-month postrelease point at the time the linked dataset was obtained (January 2023), formed the final sample for analysis.
Baseline Interview
Baseline interviews of around one hour were conducted by a research officer who was also a registered mental health nurse (PC). A demographic questionnaire developed for the study was administered which included sociodemographic, clinical, and criminal justice information. This was followed by the Prison Mental Health Screening (PMHS) tool which was developed by the researchers as part of a larger study trialing the implementation of a new mental health reception screening instrument in NSW prisons (Browne et al., 2022). The PMHS tool elicited self-reported mental health history information including diagnoses, treatment, and key psychiatric symptoms experienced both historically and within the last month.
Data Linkage
Data were obtained from government-owned administrative data collections and probabilistically linked to our sample by an independent body, the NSW Centre for Health Record Linkage (CHeReL). The linkage was estimated by the CheReL to have a false positive linkage rate of 0.5%. Data on health service utilization for a period of twelve months postrelease from prison were obtained for each individual in the sample from NSW Ministry of Health data collections:
Admitted Patient Data Collection (APDC)
The APDC records inpatient episodes from all public hospitals, public psychiatric hospitals, multi-purpose services, and private hospitals and day procedure centers in NSW. Details of all inpatient admissions in the follow-up period were extracted including length of stay and nature of admission.
Emergency Department Data Collection (EDDC)
The EDDC includes information on presentations to most public emergency departments in NSW. Each emergency department presentation record has a diagnosis code based on International Classification of Diseases – 10 (ICD-10) diagnoses or Systemized Nomenclature of Medicine – Clinical Terms (SNOMED-CT) codes. New variables were created for “mental health,” “drug and alcohol,” and “self-harm” and coded manually from these diagnosis codes. These categories were not mutually exclusive, for example, all self-harm-related diagnoses were coded as both self-harm and mental health, and intentional drug overdose was coded as self-harm, mental health and drug and alcohol.
NSW Ambulance Datasets
Ambulance datasets include computer-aided dispatch (CAD), electronic medical records (eMRs) and paper-based patient healthcare records (PHCRs). The CAD dataset contains operational information from the time of ambulance dispatch to a scene and the eMR and PHCR contain data collected by clinicians attending the scene. The CAD variable indicating the reason for callout was manually recoded into four nonmutually exclusive variables “mental health,” “drug and alcohol,” “self-harm,” and “violence/behavioral disturbance.”
Mental Health-Ambulatory Collection (MH-AMB)
The MH-AMB collection contains data on episodes of outpatient mental healthcare, such as that provided by community mental health teams, including both contact and noncontact episodes of care (noncontact episodes may include care planning and case conference-type activities). For the purposes of this study, only episodes of care involving actual contact with the participant were examined.
Reoffending, reincarceration and custodial data were obtained from the NSW Bureau of Crime Statistics and Research's Reoffending Database (ROD). Participants were coded as having a reoffence if they had any finalized charges for offences that occurred in the twelve months following their initial release date. An episode of reincarceration was recorded if the individual had a prison reception date recorded in the ROD during the follow-up period.
Statistical Analysis
Statistical analyses were carried out using SPSS Statistics 27. Descriptive statistics were obtained, with clinical and criminal justice characteristics for the entire sample (N = 319) reported and chi-square comparisons made by gender and Aboriginal background. Postrelease health service utilization and reoffending outcomes were examined as well as comparisons by gender, Aboriginal background and mental health diagnosis (i.e., the presence or absence of serious mental illness) using binary logistic regression. Weighting was applied for analyses not involving gender comparisons to account for the oversampling of women (weight factor 1.0 for men and 0.33 for women).
Cox proportional hazards regression analyses were conducted to assess the effect of gender, Aboriginal background, and the presence of serious mental illness diagnosis on survival time to first health service use and first reoffence. The period of observation for each participant spanned from their date of release from prison until censoring at the outcome (health contact or reoffence), or 12 months postrelease. A log-rank test was run to test differences in survival distributions for each group. The inspection of log-minus-log plots for each variable indicated that the assumption of proportional hazards was met in each case.
Finally, the relationship between healthcare and time to reoffence was examined with Cox regression, firstly for the entire sample, and then for the serious mental illness group only (n = 74). First ambulatory mental health contact, first emergency health contact, and first health contact (any) were examined as time-varying covariates at a univariate level, then adjusting for gender and Aboriginal background.
Ethics Approval
Ethical approval for this study was obtained from the NSW Population and Health Services Research Ethics Committee (2021/ETH01237), Justice Health and Forensic Mental Health Network Human Research Ethics Committee (G185/14), the NSW Aboriginal Health and Medical Research Council Ethics Committee (1137/15) and the Corrective Services NSW Ethics Committee (D16/139081).
Results
Sample Description
Sociodemographic, criminal justice and clinical characteristics of the sample at baseline are shown in Table 1. The median age at prison entry was 32 years (interquartile range 24–41 years). One-quarter (25.2%) of the overall sample were Aboriginal with a larger proportion of women (38.2%) than men (23.0%) identifying as Aboriginal, χ2 (1) = 8.24, p < .05. Over one-third of the sample (35.1%) reported being in a marital or de facto relationship and a similar proportion (38.4%) reported an educational level of below Year 10 (i.e., 15 years old). Just under three-quarters (71.1%) of the sample were unemployed at the time of the offense. Around two-thirds (64.2%) of the sample were on remand, nearly one-quarter (23.6%) were in custody for the first time, and 40.0% had been charged with a violent offense. Aboriginal participants were more likely to report an education level less than Year 10, χ2 (1) = 13.83, p < .001, and to have been in prison before, χ2 (1) = 3.88, p < .05. Women were more likely than men to be married or in a de facto relationship, χ2 (1) = 9.09, p < .05, to have been unemployed at the time of the offence, χ2 (1) = 17.30, p < .001, and to be in custody for the first time, χ2 (1) = 5.12, p < .05.
Sociodemographic, Criminal Justice, and Clinical Characteristics of the Sample, by Gender, and Aboriginal Status.
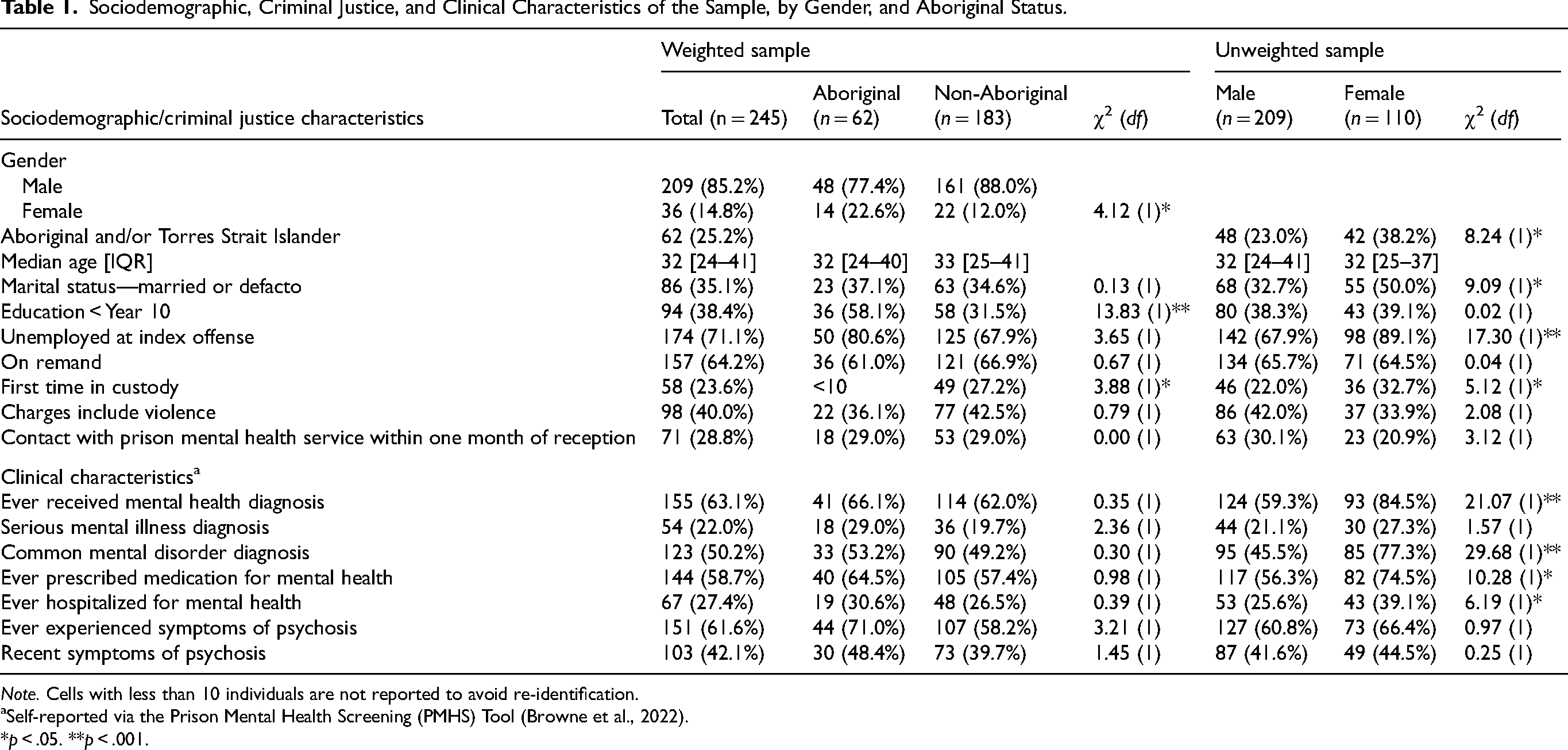
Note. Cells with less than 10 individuals are not reported to avoid re-identification.
Self-reported via the Prison Mental Health Screening (PMHS) Tool (Browne et al., 2022).
*p < .05. **p < .001.
Nearly two-thirds (63.1%) of the sample reported ever having received a mental health diagnosis, 22.0% reported a serious mental illness diagnosis (schizophrenia, psychosis, or bipolar disorder) and 50.2% reported a diagnosis of depression or anxiety. A much higher proportion of women than men reported any psychiatric diagnosis (84.5% vs. 59.3% of men; χ2 (1) = 21.07, p < .001) or a common mental disorder diagnosis (77.3% vs. 45.5%; χ2 (1) = 29.68, p < .001). However, men and women reported similar rates of serious mental illness. Aboriginal participants reported higher rates of mental illness and other clinical factors than non-Aboriginal people, however, the differences were not statistically significant. Despite high rates of mental health diagnoses reported, only 28.8% of the overall sample had contact with prison mental health services within one month of reception.
Postrelease Health Service Utilization
The median number of days spent in custody following reception was 119 [IQR 46–273], or just under 4 months. Two-thirds of the sample (65.9%) were released from prison within 6 months of reception. Of the overall sample, 59.2% utilized at least one of the health services examined (emergency department, ambulance callout, and hospital admission) in the 12 months following release from prison, with 29.6% using health services for mental health reasons (Table 2). Half of the sample (49.9%) attended an emergency department for any reason, and over one-third had an ambulance callout (36.2%), or a hospital admission for any reason (35.3%). Around one in 10 had a psychiatric admission (10.2%) and one in five accessed ambulatory (outpatient) mental health services (21.0%).
Twelve-Month Postrelease Health Service Utilisation and Reoffending Outcomes, by Gender, Aboriginal Background and Serious Mental Illness (SMI) Diagnosis.
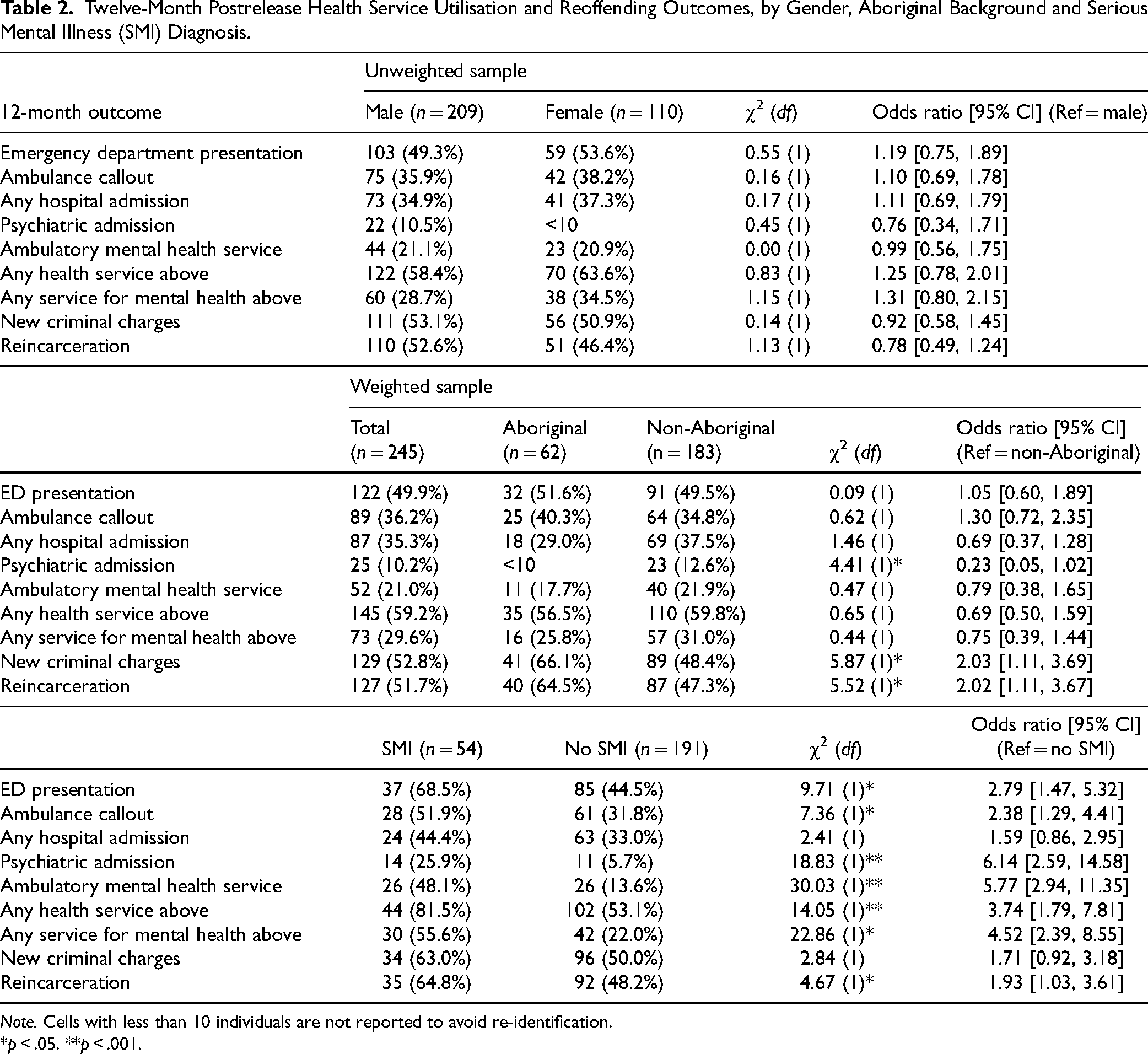
Note. Cells with less than 10 individuals are not reported to avoid re-identification.
*p < .05. **p < .001.
There were no significant differences found between men and women in terms of health service utilization; likewise, Aboriginal participants were found to utilize health services at the same rate as their non-Aboriginal counterparts, however, they were significantly less likely to experience a psychiatric admission in the follow-up period (OR = 0.23, 95% CI = 0.05, 1.02). Those with a serious mental illness were significantly more likely to have utilized all health services examined, apart from a hospital admission for any reason, in the 12 months following release. For example, they were more than twice as likely as those without a serious mental illness to access emergency health services (OR = 2.79, 95% CI = 1.47, 5.32 for emergency department presentation; OR = 2.38, 95% CI = 1.29, 4.41 for ambulance callouts).
First Health Service Utilization
Of those who received any healthcare in the 12 months following prison (n = 145), the majority accessed an emergency service (ambulance and/or emergency department) first (71.6%). This was followed by ambulatory mental health service contact (17.4%) and hospital admission (11.0%) as the most common forms of first postrelease health service contact. Of those who accessed healthcare for mental health reasons in the 12 months following prison, a similar proportion accessed ambulatory mental healthcare services first (46.3%) as those who accessed an emergency service first (48.7%). The remaining 5.0% of those who received mental healthcare had a hospital admission as their first episode of care.
Reasons for Emergency Service Contact
Over half of the sample (53.5%) accessed emergency healthcare (ambulance and/or emergency department) in the 12 months after release from prison. Furthermore, around one in five (21.0%) of the total sample accessed emergency healthcare in the follow-up period for mental health reasons (39.0% of those with any emergency healthcare). Just over 13.0% of the total sample accessed emergency healthcare for self-harm reasons (25.2% of those with any emergency healthcare) and a similar proportion (14.2%) of the sample accessed emergency healthcare for reasons relating to drugs and alcohol (26.7% of those with any emergency healthcare).
Reoffending Outcomes of the Sample
Around half of the sample (52.8%) incurred new criminal charges within 12 months of release from prison and 51.7% were reincarcerated (Table 2). Aboriginal participants were twice as likely to have received new charges (OR = 2.03, 95% CI = 1.11, 3.69) and to be reincarcerated (OR = 2.02, 95% CI = 1.11, 3.67), than non-Aboriginal participants. Those with a serious mental illness were no more likely to have new charges within the follow-up period than those without serious mental illness, but they were significantly more likely to be reincarcerated (OR = 1.93, 95% CI = 1.03, 3.61). No differences were found in reoffending or re-incarceration rates between men and women.
Predictors of Time to Reoffence and First Healthcare Contact
Men and women did not differ in terms of time to first offense or time to first healthcare contact and there were no significant gender differences in the overall rates of reoffending or healthcare contact (Table 3). Aboriginal participants had a 65% higher rate of being charged with a reoffence in the 12 months postrelease from custody (HR = 1.61, 95% CI = 1.14, 2.28). The mean time to reoffence for Aboriginal participants was 6.77 months compared with 8.30 months for non-Aboriginal participants.
Predictors of Time to First Charge and First Health Contact.
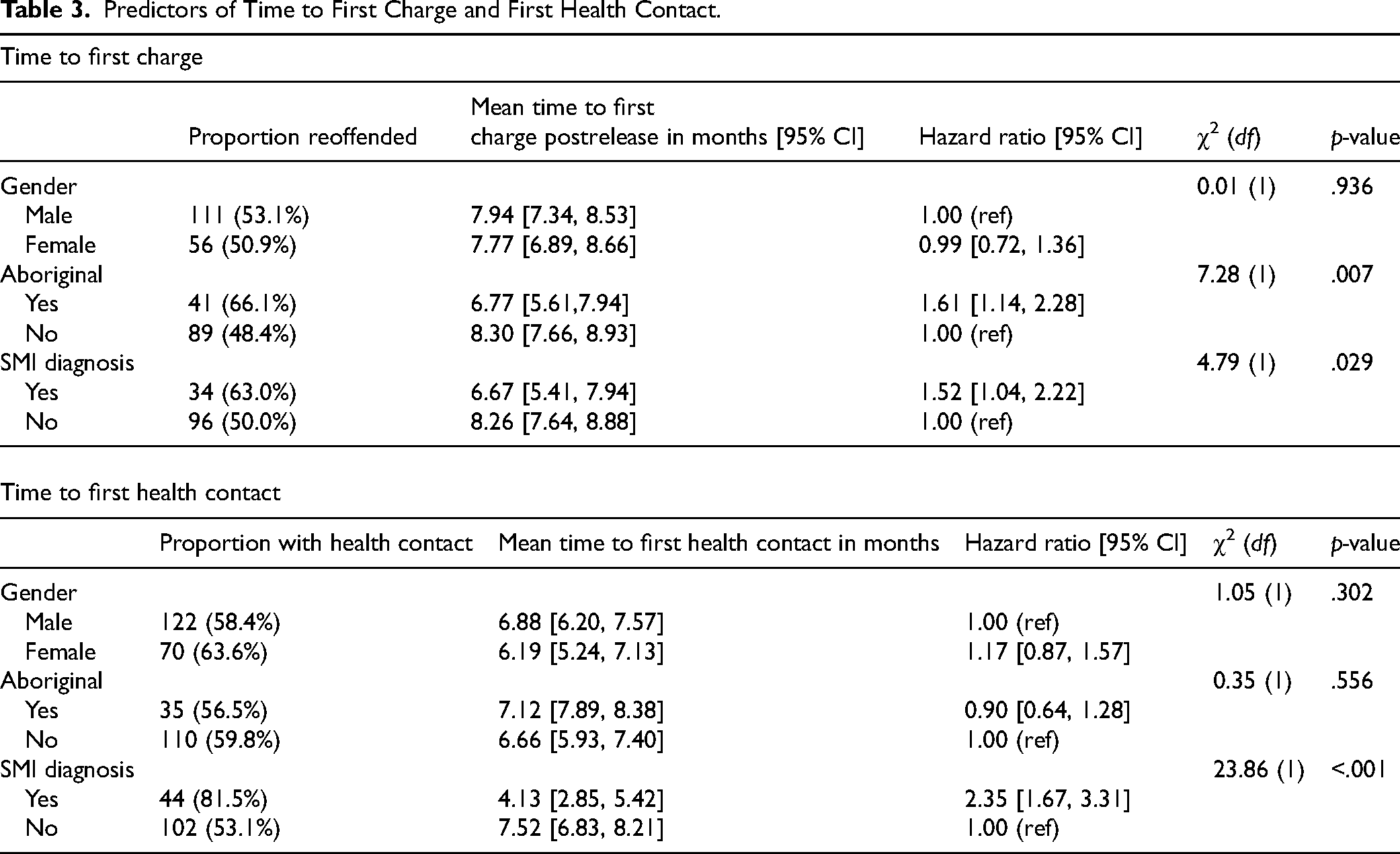
No difference was found between Aboriginal and non-Aboriginal participants in healthcare access in the 12-months postrelease (HR = 0.90, 95% CI = 0.64, 1.28), but their first healthcare contact was later compared with non-Aboriginal participants (M = 7.12 months vs. 6.66 months). Those with serious mental illness had a higher rate of reoffending (HR = 1.52, 95% CI = 1.04, 2.22), and were more likely to have healthcare contact than those without a serious mental illness (HR = 2.21, 95% CI = 1.53, 3.18). On average, they accessed health services much sooner after release (M = 4.13 months) than those without a serious mental illness (M = 7.52 months).
Relationship Between Health Service Utilization and Time to First Offence in the Postrelease Period
Accessing ambulatory healthcare postrelease from prison was not associated with reoffence for the overall sample or the serious mental illness subgroup (Table 4). Accessing any kind of healthcare was associated with an increased rate of reoffence for the overall sample (aHR = 1.69, 95% CI = 1.16, 2.45) but not the serious mental illness group. Accessing emergency care was associated with an increased rate of reoffence by 80% for the overall sample (aHR = 1.80, 95% CI = 1.21, 2.68) and 100% for those with a serious mental illness (aHR = 2.08, 95% CI = 0.99, 4.39).
Adjusted Cox Proportional Hazards Regression Analysis of Health Service Utilisation and Rate of First Offence for the Total Sample and the Serious Mental Illness (SMI) Group.
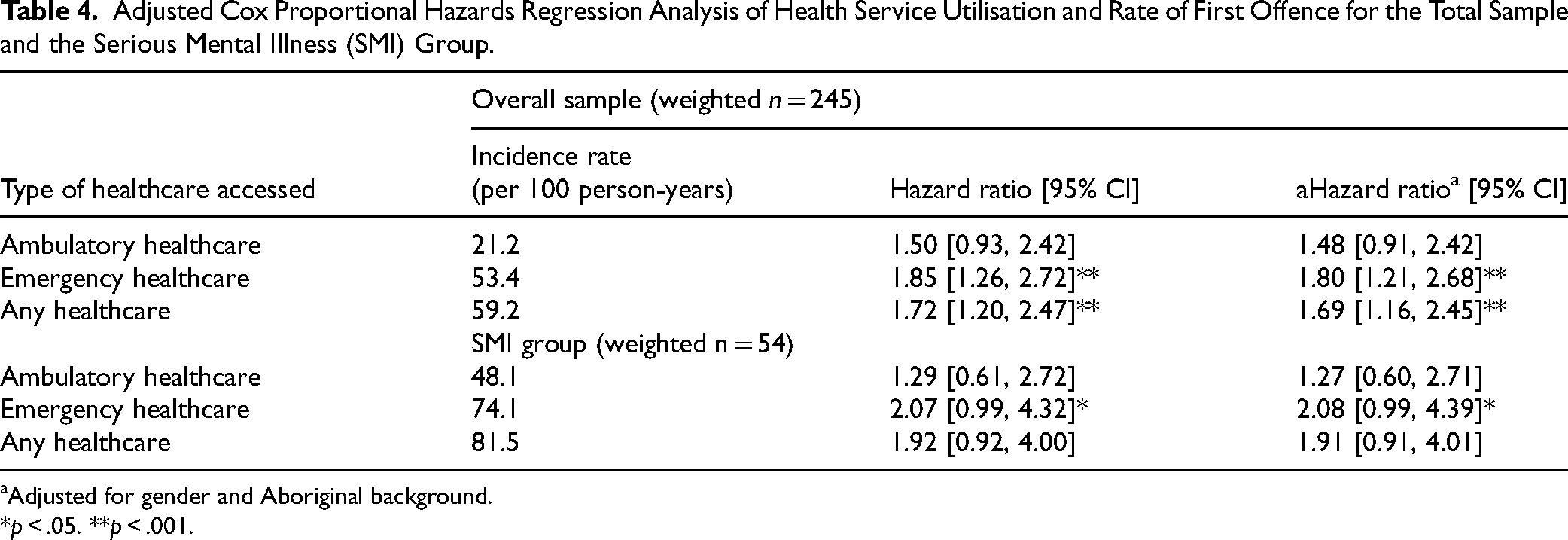
Adjusted for gender and Aboriginal background.
*p < .05. **p < .001.
Discussion
This study examined a sample of men and women recruited upon reception into prison in NSW and reported on their postrelease health service utilization and reoffending outcomes. As expected, a high prevalence of mental illness was reported by the sample, and high rates of postrelease health service use and repeated contact with the criminal justice system was identified. These postrelease findings were pronounced for those identified at prison entry as having serious mental illness. The type of postrelease health service contact was important, with a positive association found between accessing emergency services and subsequently being charged with a reoffence, but no evidence of a protective effect of accessing outpatient/ambulatory mental health services. Efforts to improve the continuity of healthcare between prison and the community are likely to be required to reduce the burden on the emergency health system as well as to reduce the risk of vulnerable people cycling in and out of custody.
Main Findings
In the cohort of men and women recently received into custody, nearly two-thirds reported ever being diagnosed with a mental illness, and one-fifth reported a serious mental illness diagnosis (schizophrenia, psychosis, or bipolar disorder). These high rates are consistent with local and international research (Browne et al., 2023; Fazel et al., 2016). Women reported a greater burden of mental illness than men, as has also been reported previously (Browne et al., 2023; Tyler et al., 2019). Rates of mental illness were, however, similar between Aboriginal and non-Aboriginal people; a finding that has previously been reported in studies of Aboriginal men in prison (Butler et al., 2007), while studies of Aboriginal women have higher rates of mental ill health than non-Aboriginal women (Butler et al., 2007; Stewart et al., 2021).
Over half the sample (59.2%) utilized public health services at least once in the year postrelease from prison, half (49.9%) attended an emergency department and one-third (36.2%) accessed ambulance services, reinforcing the high level of urgent or crisis-based healthcare need for this group. The level of emergency service contact among people released from prison was higher (53.5% in the first 12 months) than that reported for the general population in NSW, among whom around one-third have emergency service contact annually (Centre for Epidemiology and Evidence, 2023). Almost 40% of those who accessed emergency services did so for mental health reasons; a quarter for reasons related to self-harm; which speaks to the inadequate availability of community-based health services to address these issues.
The rate of hospital admissions for any reason (35.3%) in the prison-release cohort was, however, similar to that reported for the general population at around a third, but for the prison-release sample, there was a strikingly higher rate of psychiatric admission compared to the general population (10.2% vs. 1.8%). Over one-third (36.2%) of the study cohort utilized ambulance services in contrast with 11.5% in the general population (Australian Productivity Commission, 2022). Finally, 21% accessed ambulatory mental health services in comparison with 1.8% of those in the NSW population as reported within the National Community Mental Health Care Database 2020–2021 (AIHW, 2023).
We found no difference in health service utilization between men and women, which was consistent with a recent study of acute health service contact in Queensland, Australia (Janca et al., 2023); but in contrast with previous studies suggesting that women are more frequent users of postrelease healthcare (Alan et al., 2011; de Andrade et al., 2019). It is likely that these findings reflect a higher level of unmet need in women released from custody, given that they reported much higher rates of mental illness at prison entry than men. Additionally, despite evidence to suggest that Aboriginal people are more likely to utilize health services postrelease from prison (Alan et al., 2011; Hobbs et al., 2006; Young et al., 2019), there were few significant differences between these subgroups in our sample, and in fact Aboriginal people were significantly less likely to experience a hospital admission in the 12 months postrelease; a finding perhaps more likely to reflect a lack of access as opposed to a lack of need.
Considering that those exiting prison with mental illness have been found to experience worse physical and mental health outcomes than those without (Cutcher et al., 2014), it is unsurprising that those with a serious mental illness in the study cohort had much more contact with health services postrelease from prison, and sooner after release, than did those without a serious mental illness. While we might expect those with serious mental illness to have higher rates of psychiatric admission and ambulatory mental health contacts, the finding that they also have more than twice the rate of emergency health contacts reflects the particular level of vulnerability experienced by this group in the early postrelease period and calls into question the effectiveness of efforts aimed at mental healthcare continuity between prison and the community. Furthermore, nearly half of those who accessed mental healthcare in the 12 months postrelease from prison first accessed these services within an emergency context (i.e., ambulance and/or emergency department), and around one in five accessed an emergency service for mental health reasons. These findings may reflect the lack of available/accessible community mental health services or a lack of awareness as to how to access these services among those with mental illness who are released from prison. Many individuals are released into temporary accommodation or homelessness, which may prevent long-term engagement with a community team. Community mental health teams are also often not equipped to support the complex needs of those with both serious mental illness and offending behavior or histories of incarceration, which include multiple comorbidities, high rates of trauma, substance abuse issues, and mistrust of services, all of which can impede engagement. In recent years, the NSW Government has funded a Community Transitions Team operated by Justice Health and Forensic Mental Health Network to better support the transition between prison and the community for those with serious mental illness with an evaluation underway to examine its effectiveness.
Half of the cohort returned to prison within one year of release. In NSW, just under half of all people released from prison in 2020–2021 returned within 2 years (Australian Productivity Commission, 2023). A possible contributor to the high rates of reincarceration within our sample may be the short periods of time that our participants spent in prison. While we did not have detailed release information for participants, the fact that two-thirds were released within 6 months likely reflects a high rate of release from remand (e.g., to bail, community-based sentence, or withdrawn charges). Those with brief periods in custody have less opportunity to plan for release in terms of securing stable accommodation and arranging continuing healthcare and this is likely to impact on postrelease outcomes (Browne et al., 2022). Our findings regarding group differences in reoffending—that men and women reoffended at similar rates and that Aboriginal participants were more likely to reoffend than non-Aboriginal participants—are consistent with NSW reoffending statistics as reported by BOCSAR (2023). The “incarceration gap”—the disproportionate representation of Aboriginal people in Australian prisons—is well documented and is likely to reflect the well-known intergenerational impacts of ongoing systemic disadvantage, trauma and discrimination, which the authors argue must be addressed urgently, along with better provision of postrelease healthcare.
Our finding of an increased risk of reoffending among those who accessed emergency healthcare following release from prison, and particularly for those with serious mental illness, is broadly consistent with previous findings (Constantine et al., 2012; Frank et al., 2013). We did not, however, find the protective effect of ambulatory mental healthcare use on the risk of reoffending that has been found previously (Constantine et al., 2012; Hawthorne et al., 2012), indicating that these services may not be having a sufficient stabilizing effect, or are not being accessed adequately, perhaps, particularly for a predominantly remanded population. Further research might explore the impact of ambulatory mental health treatment “dosage” on subsequent outcomes, including within key subgroups.
Strengths and Limitations
This study is novel in its approach to examining postrelease healthcare and reoffending in a sample recruited on reception into prison as opposed to those identified upon, or shortly prior to release, as occurs in most postrelease studies. The advantage of this approach is the ability to examine outcomes for remandees, a group with higher morbidity but who are often overlooked in studies; they may stay in prison for brief periods of time but nonetheless account for a large proportion of overall service use (Jones et al., 2021).
Our findings regarding health service utilization are limited to the available data. For example, the Emergency Department Data Collection includes data from most, but not all, public emergency departments and some regional hospitals and private hospital emergency departments were also excluded from this collection. Additionally, we did not have access to data on the use of private outpatient mental health services or appointments with general practitioners. As such it is likely that our estimates of the rates of health and mental health service utilization in the cohort following release from prison, while high, under-represent the actual rates.
Recruitment of the sample commenced in 2016 with postrelease-data being captured between 2016 and 2022 dependent on release date; therefore some data are around 8 years old. Further research in this area may re-examine health and reoffending outcomes in the context of an increasing prison population, stricter bail laws via amendments to the NSW Bail Act in 2022 and 2024, and recent targeted efforts to improve continuity of care for those with serious mental illness such as the Community Transition Team mentioned earlier in the discussion.
Finally, the sample size restricted further subgroup analyses and prevented us from examining the intersection between gender and Aboriginal background in more detail, along with the presence of serious mental illness. Ogilvie et al. (2024), for example, found that among offenders, Indigenous women have the highest rates of mental illness and mental health contacts in comparison with other demographic groups, and that offending trajectories differ across both gender and Indigenous status. Our nonsignificant findings regarding health service utilization among Aboriginal people may reflect the small number of Aboriginal women in our sample. Similarly, some of the negative findings from the current study may have resulted from underpowered analyses and thus require repetition in a larger sample.
Conclusions
The findings of the current study provide further evidence of the links between poor mental health among people in prison and the high rates of postrelease healthcare utilization, particularly emergency contacts, as well as repeated contact with the criminal justice system. While established in other prison samples and contexts, the current findings indicate that these complex relationships are of even greater importance for those identified on entry to prison, a group dominated by remandees and those on short sentences who are often excluded from prison-release studies. The impact of even short periods of time in custody, particularly for those with mental health and other vulnerabilities, can be catastrophic with regard to the maintenance of community-based support. This highlights the crucial need for the early identification of people with mental illness in order to divert them from the justice system and into community mental healthcare where possible, and the need to commence postrelease care planning as early as possible. Healthcare, in prison just as in the community, does not occur in isolation, and should be considered alongside other forms of social care such as housing, disability and cultural support. A coordinated approach to care in the community may go some way to reducing the burden on already stretched public healthcare and correctional systems, as well as improving outcomes for some of the most vulnerable groups in our community.
Footnotes
Acknowledgments
This research was supported by an Australian Government Research Training Program (RTP) Scholarship, a National Health and Medical Research Council (NHMRC) Grant: The Australian Centre for Research Excellence in Offender Health (GNT1057492), and NHMRC Investigator Grant: Improving the Mental Health of People in Contact, or at Risk of Contact, with the Criminal Justice System (APP1175408). Justice Health and Forensic Mental Health Network (JHFMHN) provided in-kind support to JHFMHN clinicians and researchers involved in the project. Approval to access linked data was granted by Data Custodians at the NSW Ministry of Health and the NSW Bureau of Crime Statistics and Research (BOCSAR). Linkage was conducted by the NSW Centre for Health Record Linkage (CHeReL).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Australian Government Research Training Program (RTP) Scholarship, National Health and Medical Research Council (grant number GNT1057492; APP1175408).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.