
Abstract
Inpatient forensic psychiatric rehabilitation is based on patient symptoms, life activities performance and perceived risks to self and others. Self-ratings provide insights into patients’ perspectives. We have found differences between self-ratings and staff-ratings using the World Health Organization Disability Assessment Schedule 2.0 (WHODAS). To understand rating differences, we performed a qualitative study exploring patients’ reasoning when self-rating WHODAS. Eighteen participants with a psychotic disorder and a history of aggression, cared for at a low to medium secure forensic psychiatric inpatient clinic in Sweden, were interviewed using verbal concurrent probing when self-rating the WHODAS. Participants’ responses during the concurrent probing interview were summarised under three central themes: difficulties understanding and expressing language associated with the questionnaire; cognitive difficulties; and contextual rating difficulties. The analysis of two additional questions, about meaningfulness and validity, resulted in one further theme: Value of doing the rating. The usability of the questionnaire and of the self-rating process was not uniform, given differences in participants’ language-related and cognitive abilities, as well as some questions not being readily applicable to an inpatient setting. Overall, the questions may prompt self-reflection, which could increase patient participation and self-awareness.
Introduction
In Sweden, individuals who have committed a crime under the influence of a severe mental disorder may be sentenced to forensic psychiatric care. Forensic psychiatric care is a specialised branch of psychiatry, governed by laws that differ across countries. In Sweden, the duration of care is not specified at the time of sentencing but rather determined by an individual's treatment needs and recidivism risk. The average duration of forensic psychiatric care is 89.7 months, although even longer for patients suffering from psychotic spectrum disorders (Sivak et al., 2023).
In forensic psychiatric care, the rehabilitation process is based on the patient's risk profile, psychosocial function and symptoms. Participation in daily routines, psychoeducational interventions, and assisted community-based social and occupational training form part of the rehabilitation process (Selvin et al., 2021). Assessment of a person's functional level should be reliable and valid. In addition to observational assessments by trained professionals, interview-based assessments are also used. The 36-item World Health Organization Disability Assessment Schedule 2.0 (WHODAS) is a well-established semi-structured instrument that measures perceived difficulties in performing daily activities over the 30 days prior to the assessment (Kostanjsek et al., 2010). WHODAS can be self-rated, staff-rated or used as an interview tool. Functional difficulties are measured in six domains: Understanding and communicating; Mobility; Self-care; Getting along; Life activities; and Participation. Each question is scored from 1 to 5 (1 = none, 2 = mild, 3 = moderate, 4 = severe and 5 = extreme/cannot). WHODAS 2.0 has good psychometric reliability, showing domain test-retest intraclass coefficients between 0.93 and 0.96, items in each domain reflecting the underlying domains with good to very good accuracy (Cronbach alphas of 0.47 to 0.94; WHO manual). It demonstrates sensitivity to change over time and has moderate to strong face validity compared with several other measures (Federici et al., 2017). The Swedish version of WHODAS 2.0 showed similar Cronbach alphas in a general population (Noren et al., 2023) and good reliability and convergent validity in a psychiatric outpatient setting (Midhage et al., 2021). Additionally, the Swedish 12-item WHODAS has been validated in outpatients with psychotic disorders with confirmatory factor analysis and demonstrated excellent internal consistency (α = 0.89) and strong construct validity (Holmberg et al., 2021).
Self-rating of daily-life functioning provides an insight into the patient's perspective and supports person-centred care. Previous research has shown differences between the self-ratings of patients with psychosis spectrum disorders and staff-ratings using WHODAS, and because of this, several studies have advised against the use of self-ratings (Akinsulore et al., 2015), while others have argued for the need to include both types of ratings, given the discrepancy in, for example, a forensic psychiatric sample (Kallman et al., 2024). Svensson et al. (2024) highlighted the importance for patients that staff consider their narratives, perspectives and aspirations in forming rehabilitation plans. The WHODAS is an instrument that can further this process, but to better understand potential sources of assessment differences and patient-perceived needs, it is important to understand its utility. As a step to potentially implementing this in clinical practice, it is imperative that we better understand sources of confusion for patients, whether they be within the instrument or are intrinsic to the person rating it. A method to achieve this is utilising the cognitive interview (Willis, 2005), which focuses on identifying potential errors in the design of the survey in different patient groups by identifying themes that describe the perceived difficulties (Husebo et al., 2018). This method can contribute to the understanding of how patients reason about their responses (Tourangeau, 1984). In this study, we use a cognitive interview strategy with concurrent patient self-rating of the 36-item WHODAS 2.0 to elucidate common themes that can affect the translation of the instrument into clinical practice.
Method
Design
An explorative qualitative design was used. Data for this study were collected as part of a larger mixed-methods study of how forensic psychiatric patients regard their possible disabilities and form part of the Stockholm Forensic Psychiatry Project.
Data Collection
The study was conducted at the North Section of the Stockholm Forensic Psychiatry inpatient service. A total of 18 patients with a psychotic disorder and a history of aggression were invited to participate by a staff member not involved with the patients’ care at the inpatient service. After written informed consent, the audio-recorded interviews were conducted from August to December 2019.
Inclusion criteria were adults (>20 years) with psychotic spectrum disorder (psychosis NOS and schizophrenia) according to DSM-5 (American Psychiatric Association, 2013), cared for >3 months and mentally stable with any substance use disorder in remission. Exclusion criteria were moderate or severe intellectual developmental disorder, pre-existing brain injury, central nervous system disorders, untreated endocrine diseases and inadequate Swedish language skills.
Verbal concurrent probing is a technique based on psychological theories of language comprehension, memory and judgement. It demonstrates a strong ability to capture problems associated with response validity in surveys (Schwarz, 2007; Tourangeau, 1984). This technique has the advantage of removing some of the cognitive burden from the respondent and minimising memory biases (Willis, 1999) and was therefore applied in this study.
We performed ‘item by item concurrent probing’ (Willis, 1999) of how participants interpreted and perceived the questions in the WHODAS questionnaire, excluding the ‘work/school activities’ section in domain 5, Life Activities, as per instructions to the WHODAS when somebody lacks participation in paid work/school (Kostanjsek et al., 2010). After each main question was answered, clarification questions were asked (see Supplemental File S1). In addition to the concurrent verbal probing procedure, participants were asked to answer two extra questions: (i) whether they view the WHODAS questions as meaningful; and (ii) whether they judge the WHODAS questions valid regarding their situation on the ward.
All interviews were conducted face-to-face by the first author; a psychiatric nurse specialist trained in interviewing forensic psychiatric patients using WHODAS and with no prior relationship with the participants. Due to clinic procedures, a staff member had to be present in the room. The participant had the opportunity to choose which staff member. After the first interview, the first and second authors listened to the audio recording to judge if adjustments to the semi-structured guide were required. A probing question regarding paraphrasing was added. All interviews were transcribed verbatim from complete audiotapes, and where syntax and meaning were difficult to ascertain, the first author listened to and checked the transcriptions multiple times. The second author listened to a subset of the recordings to verify the transcripts. Some field notes were made regarding answering WHODAS items on ‘sexual activities’ and ‘maintaining a friendship’, since some participants reacted to these questions with signs of distress and raised voices, which the interviewer interpreted as anger. These feelings were confirmed by the additional questions (i and ii).
The quotes were first translated into English verbatim by the last author, accounting only for different word sequences in English but maintaining incorrect syntax when present. A professional translator was then asked to back-translate this into Swedish. Translation and backtranslation were performed by different translators, enhancing methodological rigour (Yunus et al., 2022). Discrepancies were resolved in discussion between the first and last authors.
Qualitative Content Analysis
A qualitative content analysis (Graneheim & Lundman, 2004; Graneheim et al., 2017) was used to analyse the concurrent probing data. Themes were identified and analysed inductively and not driven by a predetermined theoretical framework.
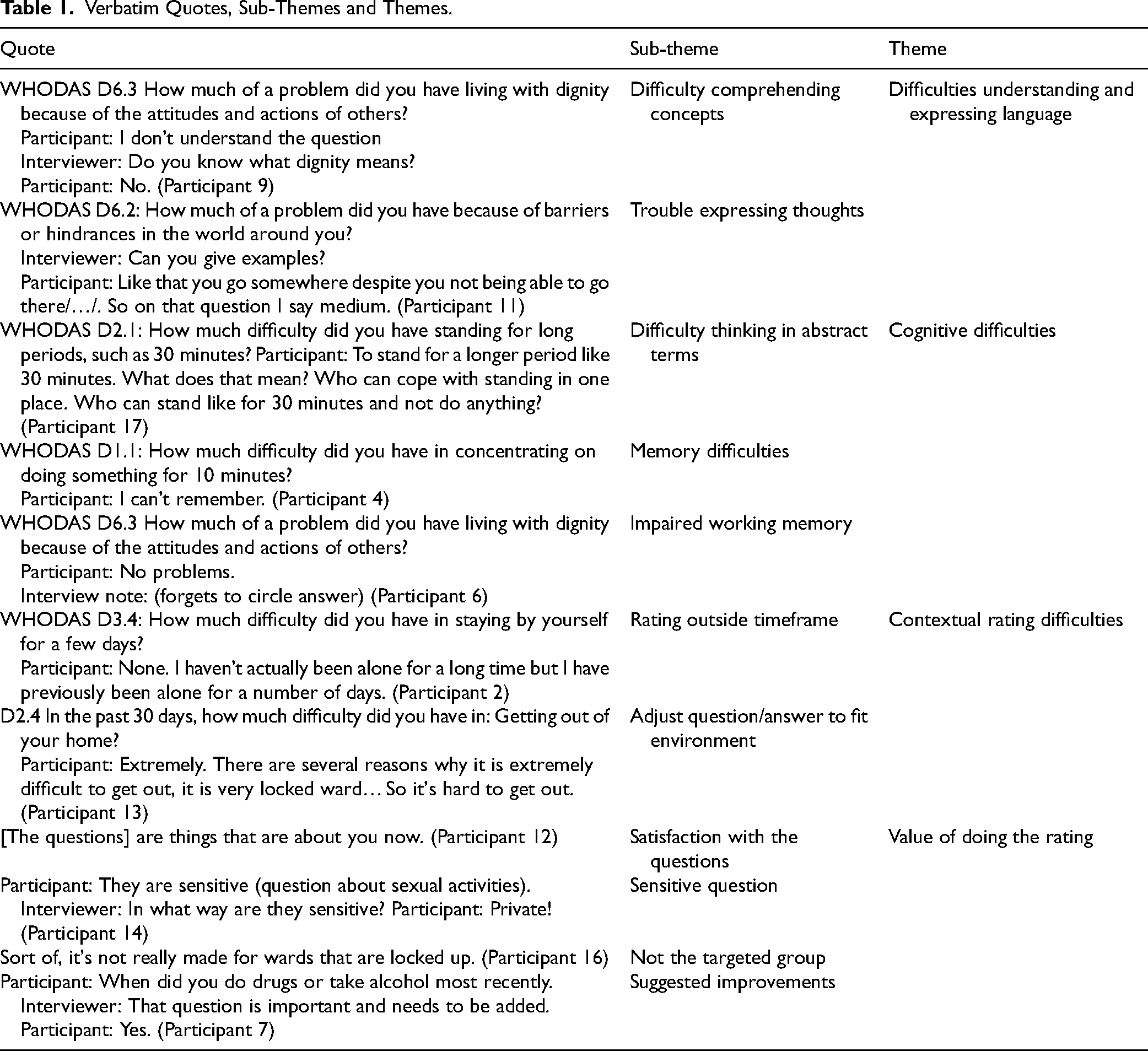
Verbatim transcripts were read through several times independently by the first and second authors for familiarisation with the data; thereafter, units of meaning were condensed and coded independently by the first and second authors with only minor discrepancies. The shared meaning of each code was discussed by the co-coders to reach agreement, a procedure to increase validity (Graneheim & Lundman, 2004). After coding 12 interviews, the data were considered redundant by both researchers (Hennink & Kaiser, 2022). Codes were sorted into sub-themes and unified into themes after joint discussion with all authors until consensus was reached (Graneheim et al., 2017). No contradiction of themes was found. Examples of responses and classifications are shown in Table 1.
Verbatim Quotes, Sub-Themes and Themes.
All four authors were female, two were psychiatric nurse specialists, two were psychiatrists, and three had PhDs. The authors had combined experience in qualitative research, forensic psychiatric research and practice. We acknowledge our understanding of theories of functional impairments in individuals with schizophrenia and consider this a strength in the analysis (Thibaudeau et al., 2021).
Results
Participants had been inpatients in forensic psychiatric care for 3 to 34 months (mean 11.94), the mean age was 33 years (25–57 years), 14 (78%) were men, and 11 (61%) had only completed primary school. The average interview time was 34.27 minutes (18.24–60.58 minutes), as shown in Table 2.
Demographic Data.
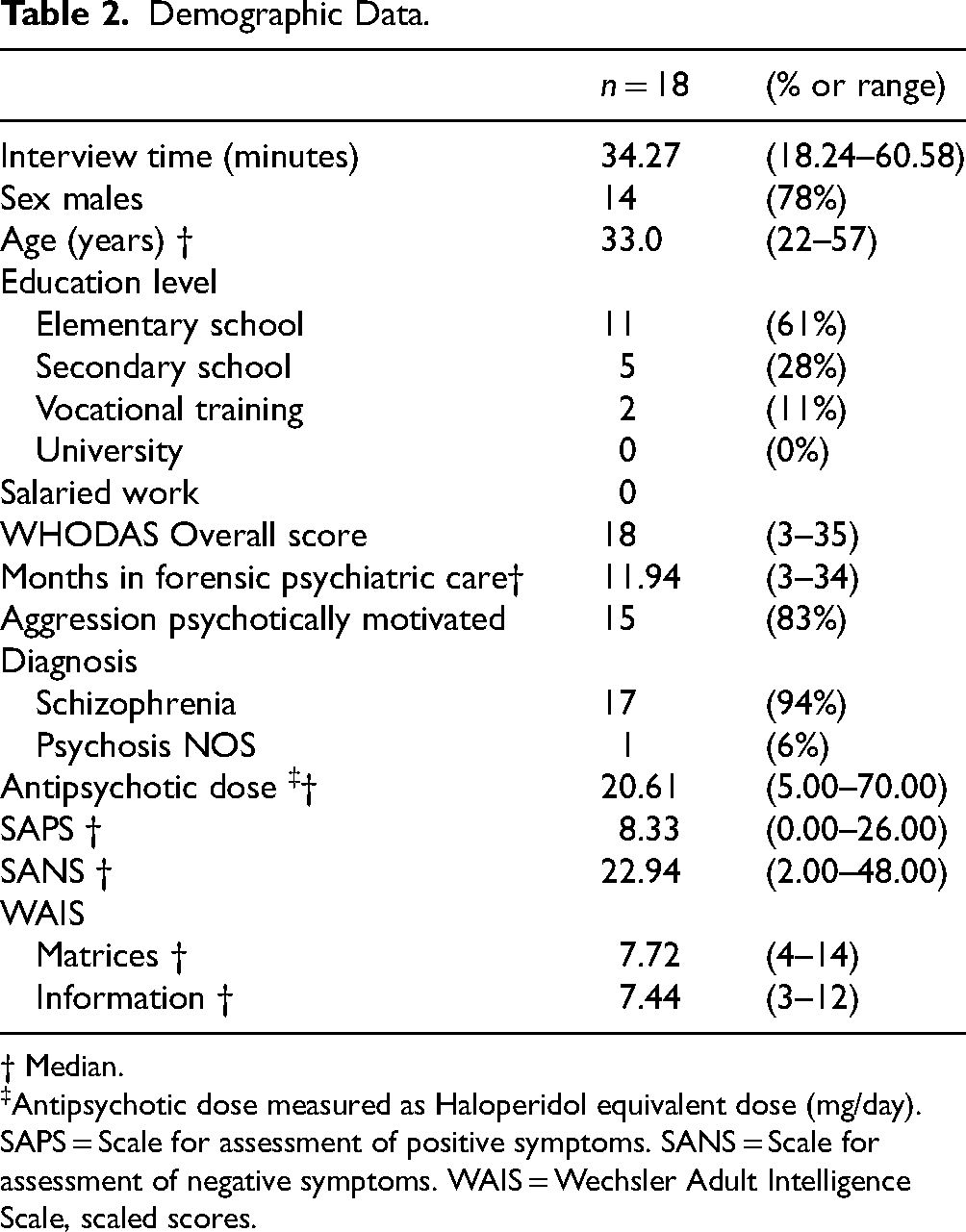
† Median.
Antipsychotic dose measured as Haloperidol equivalent dose (mg/day).
SAPS = Scale for assessment of positive symptoms. SANS = Scale for assessment of negative symptoms. WAIS = Wechsler Adult Intelligence Scale, scaled scores.
Responses to Concurrent Probing Questions
Problems were reported or observed for 26 of the 32 questionnaire items. In all, participants reported 178 problems. Only six items had no reported problems regarding understanding, D2.2 (Standing up from sitting down?), D2.5, D3.1 (Washing your whole body?), D3.3 (Eating?), D4.3 (Getting along with people who are close to you?) and D6.8 (How much of a problem did you have in doing things by yourself for relaxation or pleasure?).
General Themes and Problems Related to Forensic Psychiatric Patients' Understanding of the Questions in the WHODAS Questionnaire
All the participants’ responses during the concurrent probing interview fit into three central themes: difficulties understanding the questions and expressing language; cognitive difficulties; and contextual rating difficulties. The analysis of the two additional questions resulted in one further theme: value of doing the rating.
Difficulties Understanding and Expressing Language
Participants described problems related to comprehension of concepts, revealing that keywords and concepts were not fully understood. Comprehension difficulties were present across all WHODAS domains. Participants expressed uncertainty about the meaning of words, and some asked the interviewer what a word meant. Several participants stated during probing that they had problems understanding whole sentences, and some just guessed: ‘At first I found it pretty difficult to understand the question, so I sort of guessed a bit’ (Participant 10). Specific concepts that caused problems included, for example, ‘household tasks’, ‘maintaining’, ‘world around you’ and ‘dignity’. Regardless of not knowing or only guessing what sentences or words meant, some participants rated a disability score on the item in the form. D5.2. In the past 30 days, how much difficulty did you have in: Doing most important household tasks well? Household tasks, what do you think is included in that? /…/ To shower or?
(Participant 9) D6.2 /…/ Because of barriers or hindrances in the world around you? I don’t understand what they mean by the world around you?
(Participant 2) D6.1 /…/ Joining in community activities (for example, festivities, religious or other activities) in the same way as anyone else can? (Rates) No problems. Can you give an example of activities that you would do to participate in society? Working. /… / Any special job? Criminality.
(Participant 14) D1.3 /…/ Analysing and finding solutions to problems in day-to-day life? Can you tell me how you approached analysing a situation? Just so, when every time I take medicine, I have to sit outside for half an hour.
(Participant 12) D2.3 /…/ Moving around inside your home? So you chose a “little” rating because you mainly sit. No because everyone has their own opinion, own problems at home. That's why I chose “little” …. Yes, if I’m not allowed to play then there is a problem if my little brother sits and plays. I can’t just remove my brother from there when he has the controls and is playing.
(Participant 17)
Cognitive Difficulties
Participants reported cognitive difficulties when completing the questionnaire, which the interviewer observed. Regarding thinking in abstract terms, participants seemed to interpret the WHODAS questions concretely rather than in general or abstract terms, without processing theoretical concepts. This type of difficulty was evident when participants’ reasoning was tied to the exact wording of a question. D2.1 /…/ Standing for long periods, such as 30 minutes? One can’t cope with standing for 30 minutes in one spot, so one changes positions.
(Participant 14) D2.1 /…/ Standing for long periods, such as 30 minutes? I can’t remember the last time I did that.
(Participant 2) D6.2 /…/ Because of barriers or hindrances in the world around you? No, nothing (forgets to rate the question).
(Participant 6) D6.6 /…/ Has your health been a drain on the financial resources of you or your family? So, what would you like to circle? Big I would say. I think you just circled on the wrong row.
(Participant 15) D1.3 /…/ Analysing and finding solutions to problems in day-to-day life? Analyse and find solutions to day to day problems? This is big also. Big problems? Is it problems we talk about here?
(Participant 17) H1 Overall, in the past 30 days, how many days were these difficulties present? Which difficulties?
(Participant 18)
Contextual Rating Difficulties
Participants expressed that they had problems answering with a 30-day timeframe due to a lack of experience since residing in a forensic psychiatric ward. Rating ‘without experiencing any difficulties’ was quite common, while some participants rated their difficulties outside the timeframe. For instance, some participants chose to disregard the timeframe and rated how they envisioned future difficulties, while others based their ratings on their past. D3.4 /…/ Staying by yourself for a few days? No difficulties. How did you arrive at this answer? When I was at home like and when my parents went to work, then I was alone.
(Participant 11) D3.4 /…/ Staying by yourself for a few days? None (rating). I haven’t been alone here at the hospital… But if you, for example, count being in your own room then there is no difficulty.
(Participant 8)
Value of Doing the Rating
Despite difficulties experienced in connection with answering the WHODAS questionnaire, several different opinions were put forward by the participants regarding the overall usability and acceptability, as displayed regarding satisfaction with the questions.
The questionnaire was highly valued by many participants because it focused on their everyday lives, how they handled them, and how they viewed them. They [the questions] how one feels, thinks and how one views things. /…/ Ehh, I think it is quite interesting as it makes you think about yourself in a way one usually doesn't.
(Participant 1) They are meaningful. Why do they feel meaningful? Yes, one can evaluate on one's own how things have been.
(Participant 11) D4.5 /…/ Sexual activities? These are sensitive (question about sexual activities). Sensitive in what way? Private.
(Participant 14)
Furthermore, the questions were perceived as a health check and a reminder of progress, thus providing bearings in the rehabilitation process. Have time to scrutinize oneself in a way one otherwise doesn’t. So pretty good and important questions to reflect over.
(Participant 8) No that was a lot around the state of health. I have big psychological problems, but the only reason I would not be able to manage these questions is if I had some type of physical handicap.
(Participant 2) Not because it is the last 30 days because I have been here for 30 days… No so they are not so current… for here it is not the same thing as being outside. It's a very sheltered environment here.
(Participant 18) Also, this how much time you should, which difficulties because of your health the last 30 days, with how much time you have spent on your health? It becomes like 2 questions with different answers.
(Participant 16) (Missing question) When did you last use drugs? Ah for those who haven’t used they can, what's it called, fill in, so proud, that I haven’t done it.
(Participant 7) Some of the questions were very like each other.
(Participant 15)
Discussion
This study is the first qualitative study of individuals with psychotic disorders residing within a forensic psychiatric service that examines thought processes employed when self-rating the WHODAS questionnaire. The analysis resulted in the identification of three central themes: difficulties understanding and expressing language; cognitive difficulties; and contextual rating difficulties. The value to the individual of doing the rating was also explored, resulting in one further theme: value of doing the rating, where some expressed positive views that WHODAS focuses on everyday life and that answering the questions served as an eye opener regarding personal disabilities/support needs. Others felt that the context and the tool itself hampered usability.
Schwarz (2007) identified the underpinnings of constructed questionnaires as language comprehension, memory and judgement. In this study, we found problems in just these aspects when using the WHODAS in individuals with psychosis, a disorder marked by varying degrees of cognitive dysfunction and impaired social functioning (Świtaj et al., 2012). Whilst thought disorder manifesting through abnormal speech patterns is common in schizophrenia (Comparelli et al., 2020), this should not directly impact the understanding of questions and ratings per se; they will, however, influence the verbal description of the reasoning behind answers as seen here. Yet thought disorder is also associated with difficulties in problem-solving and social cognition, leading to significant disability in terms of daily-life functioning (Oeztuerk et al., 2022) as well as negative effects on social interaction and therapeutic alliances in a care setting (de de Sousa et al., 2019).
Less well researched is that language comprehension differs significantly in some individuals with schizophrenia compared with healthy individuals (Ziv et al., 2022). Our findings highlight that participants had difficulties understanding relatively simple concepts, such as ‘household chores’, as well as complex and theoretical ones. Misunderstanding even simple questions, such as ‘difficulties in standing for 30 minutes’, was evident in several participants’ answers. Of concern to the care process is that some patients guessed the meaning of a word rather than asking for help understanding it. These difficulties affect conversations about the domains in WHODAS and indicate that such discussions, even about simple everyday tasks, need to be particularly precise and include more follow-up questions to support the conversation.
Another possible source of language-concept errors in the self-ratings, especially when many patients misunderstood particular questions, is a problem with the wording of the questions. An example of this is answering that they had no problems with being alone, rather than saying they had no issues living independently to manage self-care. On closer inspection, this may be because specific questions in the Swedish version target concepts that differ from those in the English version. For example, the question D3.4 Difficulties in ‘Staying by yourself for a few days’ in the context of feeding and dressing is translated as ‘Being alone for a few days’, conjuring more issues of loneliness and neediness, which many of our respondents appeared to be addressing. Likewise, the question D4.5 How much difficulty did you have in ‘Sexual activities’ in the past 30 days? is translated in Swedish to difficulties in being ‘sexually close to someone’, which differs in that it not only encompasses sexual function but it also creates an expectation of intimacy and relationship within that function. We are unsure whether this relates to the anger respondents expressed in their responses to this question.
Impairments in abstract thinking are a known cognitive deficit in many individuals with schizophrenia (Gebreegziabhere et al., 2022). In the current study, disturbance in participants’ cognitive processes manifested principally as an inflexible, detailed and concrete understanding of the WHODAS items and problematic conceptual interpretations. Furthermore, cognitive impairments are strongly associated with impaired long-term memory (Guo et al., 2019) and working memory (Sheffield et al., 2018). Cognitive impairment related to working memory affects individuals’ ability to remember and process information during quite a short time frame (Wu & Jiang, 2020), and this became evident when participants repeatedly forgot the instructions on the WHODAS questionnaire and had to ask the interviewer for guidance. Moreover, in the H-section, participants had obvious difficulties remembering their scoring of the effect of difficulties and providing an answer regarding how many days the difficulties had affected their lives. It has been suggested that individuals with schizophrenia, especially those suffering from severe psychopathological conditions and adverse symptoms, may experience a reduced ability to estimate time (Mavrogiorgou et al., 2022). Specific questions targeting participants’ feelings of time and time estimates when performing the WHODAS items were not included in the present study. Still, they could provide valuable information in future psychometric evaluations of the questionnaire. The pronounced findings in this study may reflect the lower intellectual abilities of many of our participants and cannot be viewed as generalisable to all individuals with schizophrenia.
Under the theme ‘Contextual rating difficulties’, participants reported that the care context affected their assessments. They did this by directly stating that the limitations of the environment caused impairments. This is in line with previous studies that point out that forensic psychiatric care is a restrictive care environment which inhibits patient autonomy (Magnusson et al., 2020). The WHODAS manual makes clear that there is an environmental impact which WHODAS does not consider (Kostanjsek et al., 2010). To cope with this contextual difficulty, some participants adapted the timeframes to answer the questions, a factor to bear in mind if using the WHODAS in clinical care. In fact, it would be recommended to adapt the timelines so that pre-forensic care periods and current time frames are rated separately. Even after adjusting their answers to prior experience, some participants solved the contextual problem by anticipating future functions, not necessarily understanding that some of these questions could be answered based on current tasks and experiences. This can be seen in the context of their limited scope for action, as care decisions have been made by the administrative court, making it difficult for the nurses to fully support patient participation (Magnusson et al., 2020). Being heard in the forensic psychiatric setting is important for the rehabilitative content to have meaning for the patient (Gildberg et al., 2010); this can occur through self-assessments. Even though participants experienced several difficulties in responding, thereby reducing the questionnaire's usability, answering the items was perceived as valuable because it enabled them to engage with their life narrative, as seen in previous research (Svensson et al., 2024). At the same time, some patients believe that WHODAS is better suited to others with more serious illnesses and physical conditions than they themselves. But for most patients, it seems that answering the questions helped participants reflect on their psychosocial disabilities. Providing forensic psychiatric patients with time and space to reflect on their individual performance in daily-life activities could increase their motivation to participate in daily routines as practice for reintegration into society, along with enhancing patients’ participation in their care (Selvin et al., 2021).
Strengths and Weaknesses
In this study, the sample size was relatively small; however, qualitative research is often based on small samples and on information richness. Even though data was considered redundant when no new codes were identified after 12 interviews, we improved the reliability of the data by including all 18 individuals in this study.
Concurrent probing techniques, whilst avoiding memory bias, have been criticised for potentially introducing bias, since questions may lead respondents to a specific answer (Willis, 2015). To minimise such bias, we strove to select non-leading probes.
Providing verbatim transcriptions to the participants for validation would not have yielded any quality improvements, given the extended time period between the interviews and the subsequent transcription and analysis stages. Furthermore, having staff present during the interviews and ratings may have affected participants’ ratings, especially if they had not already discussed similar questions with their treatment team or felt it would negatively impact their care process.
The inclusion of individuals who had a history of substance use disorders and or intellectual challenges means we are not able to generalise the findings to schizophrenia per se. The sample does, however, reflect individuals who in Sweden are cared for in a forensic psychiatric setting, enabling some generalisability to that population. A limitation is that we cannot, with our design, rule out the effect of delusions, particularly of a persecutory nature, on a reluctance to admit to issues in the self-ratings. However, the vast majority did not exhibit such delusions at the time of the ratings, and in a subsequent review of the data, we found no indication that these symptoms influenced ratings or reasoning. Furthermore, we did not include women in the sample, meaning we cannot extrapolate the findings of this study to women. The participants were patients at a forensic psychiatric clinic, and thus, the results regarding the usability of WHODAS may not be transferable to patients with psychosis in general.
Practice and Policy Impact
Based on our results, there is a risk of misunderstanding in patient-nurse communication, particularly when using WHODAS self-ratings or when shared understanding of concepts is assumed. This could lead to the wrong support or to no support being given. Our results illustrate the significant demands placed on staff to adapt information and questions in a person-centred way, using good pedagogical and communicative competence, and to check with the individual what they understand about words and concepts. Based on this, interview ratings with the opportunity for follow-up questions are preferable in this patient group, as they tend to prompt self-reflection. But further studies of this kind are of great importance initially in a comparable diagnostic group, but also in general psychiatric outpatient care, and beyond in other psychiatric diagnostic groups.
Conclusion
The usefulness of the WHODAS questionnaire was not uniform, as several participants had difficulty understanding the questions and raised contextual issues, which argue against self-ratings being appropriate in this patient group. On this basis, our findings are in line with the results of quantitative studies on difficulties with self-ratings for people with schizophrenia. The lack of congruence with staff-ratings has been attributed to a lack of insight; yet in this study, we find that the problems are more fundamental in nature. For some individuals, there are significant impairments in understanding language and in judging what the questions are about. Furthermore, we found working memory difficulties in retaining instructions for WHODAS ratings in a subset of participants. Using the WHODAS as a tool in exploring personal views on disabilities within a forensic psychiatric setting may start a process of self-reflection, which could increase patient participation and self-awareness. Based on the findings, it would appear beneficial to consider the purpose of the assessment within the rehabilitation process, including timelines and where patient rehabilitation is carried out. Initial assessment difficulties before admission could be evaluated, while later assessments could focus on difficulties experienced in the ward environment and, later still, when they have leave provisions.
Supplemental Material
sj-pdf-1-fmh-10.1177_14999013251395299 - Supplemental material for The Usability of WHODAS Self-Rating for Forensic Psychiatric Inpatients with Schizophrenia
Supplemental material, sj-pdf-1-fmh-10.1177_14999013251395299 for The Usability of WHODAS Self-Rating for Forensic Psychiatric Inpatients with Schizophrenia by Malin V Källman, Mathilde Hedlund Lindberg, Marianne Kristiansson and Anette GM Johansson in International Journal of Forensic Mental Health
Supplemental Material
sj-docx-2-fmh-10.1177_14999013251395299 - Supplemental material for The Usability of WHODAS Self-Rating for Forensic Psychiatric Inpatients with Schizophrenia
Supplemental material, sj-docx-2-fmh-10.1177_14999013251395299 for The Usability of WHODAS Self-Rating for Forensic Psychiatric Inpatients with Schizophrenia by Malin V Källman, Mathilde Hedlund Lindberg, Marianne Kristiansson and Anette GM Johansson in International Journal of Forensic Mental Health
Footnotes
Acknowledgements
The authors would like to extend a warm thank you to the patients who, through their participation and openness, have chosen to make this study possible.
Ethical Considerations
Approval from the Stockholm Ethics board 2014/827-31/4, addendums approved 2017/219-32, 2018/307-32/4 and Swedish Ethical Review Authority 2019-01422.
Consent to Participate
Patients gave oral and written informed consent whilst clinically stable and after the conclusion of all appeal processes. Information was given verbally as well as in written form.
Consent for Publication
Written informed consent for publication was provided by the participants.
Authorship Contribution
Malin V Källman contributed to the conception, data collection, analysis and drafting the manuscript. Mathilde Hedlund Lindberg contributed to the conception, analysis and reviewing the work critically for important intellectual content. Marianne Kristiansson contributed to the conception, analysis and reviewing the work critically for important intellectual content. Anette GM Johansson contributed to the conception, analysis, reviewing the work critically for important intellectual content, supervision and responsible for obtaining funding for the study. All authors approved of the final version and agreed to be accountable.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: the Swedish Research Council [grant number 2021-06362]; Region Stockholm [grant numbers ALF-952824, 951046]; Svenska Läkaresällskapet [grant numbers 779731, 589661]; Fredrik and Ingrid Thuring's fund [grant numbers 00127, 00264].
Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Data Availability Statement
Data can be obtained upon special request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.