
Abstract
Few studies have reported the perspectives of inpatients under forensic mental health care with regards to their physical activity and the barriers they face. This mix-methods study reports perspectives on physical activity of 28 patients under forensic mental health care using a structured questionnaire and semi-structured interview. Descriptive statistics were used to summarise patient data. Physical activity knowledge, preferences, practices and barriers were qualitatively examined by thematic analysis. Five themes were identified: (1) while physical activity is viewed as important and beneficial by patients, knowledge remains lacking; (2) patients under forensic mental health care have individual physical activity preferences, goals and motivations; (3) environmental context and social influences impact engagement in physical activity; (4) confidence and skills play a role in physical activity planning and adherence; and (5) perceived barriers to physical activity include individual, service-related and environmental factors. This study highlights the overall preference expressed by forensic patients for lower intensity activity supervised by a known and supportive staff member. Forensic services need to be adaptive when considering how to offer physical activity opportunities while managing several service-related challenges.
Background
A significant proportion of people who are inpatients of forensic mental health services have physical health problems, including obesity and metabolic syndrome, and report low levels of physical activity (Moss et al., 2022). Poor cardiovascular and other health outcomes are associated with low levels of physical activity (Vancampfort et al., 2015). Prioritising the physical health of patients with mental illness has been a key priority for governments in recent years (Australian Government Department of Health, 2017; National Health Service, 2019; Welsh Government, 2020). This is particularly pertinent to people who are inpatients under forensic mental health care as their average length of stay is measured in years (Völlm et al., 2017). These patients are highly dependent on the availability of services within the hospital environment; equally, this presents a time and setting where an opportunity exists for health and physical activity to be prioritised, monitored and improved.
Many factors can impede the uptake of physical activity interventions in hospital settings including competing demands on staff, lack of knowledge, lack of skills, lack of resources and operational priorities (Geelen et al., 2021). While strategies for guiding implementation have been proposed, difficulties exist in identifying how to customise interventions for specific environments. One approach, arising from the field of Implementation Science, The Theoretical Domains Framework (TDF), was developed on the basis of a synthesis of 128 constructs related to behaviour change found in 33 different behaviour change theories (Cane et al., 2012). The TDF is not an explanation of a set of behaviours identifying causal processes, rather it identifies key determinants and constructs, and provides a guide to relevant explanations of current behaviours which can be assessed and subsequently identifies opportunities and methods for intervention. The TDF has been used successfully in other studies of physical activity (Taylor et al., 2013).
To date, there have been few studies that have sought the perspectives of inpatients of forensic mental health services, despite growing recognition of the importance of having patient voices and co-design processes incorporated into quality improvement of service delivery and clinical practice (Suomi et al., 2016). The limited available research has reported that forensic patients view their physical health issues as being ‘done to them’ and that the environment and associated institutional constraints contribute to their inability to live a healthy life (Every-Palmer et al., 2018). A recent study by Anthony et al. (2023) exploring adolescent and staff perspectives related to institutional barriers to physical activity, the rehabilitative benefits of physical activity, and the need for collaborative working within secure psychiatric care, noted widespread agreement as to the benefits of physical activity on mood, engagement and pro-social behaviours.
Positive outcomes have been reported for forensic patients engaged in physical activity including improved objective anthropometric and physical health measures as well as subjective self-reported well-being measures (Cormac et al., 2013; Wynaden et al., 2012). Similarly to non-forensic populations, physical health benefits include improved weight, waist size, diastolic blood pressure, hand strength, flexibility, lung function and aerobic capacity (Murphy et al., 2019; Vancampfort et al., 2015). Studies have also reported that forensic patients both enjoy physical activity and have, at least some, opportunities available to them (Bacon et al., 2012; Mateo-Urdiales et al., 2020). Improved well-being outcomes reported by patients have included feelings of relaxation, happiness, calmness and improved ability to cope with stress (Savage et al., 2009; Tetlie et al., 2008). Despite the benefits of physical activity, forensic patients have reported lower levels of activity in hospital when compared to the community or prison (Every-Palmer et al., 2018).
There is currently a lack of understanding of how forensic patients view the role and importance of physical activity and what their preferences are with respect to physical activity choices including type of activity, goals, social influences and preferred environment. To address this gap, the present study aimed to:
examine the knowledge, preferences and practices of patients under forensic mental health care with regard to physical activity and identify barriers to engaging in physical activity within a forensic hospital environment.
Methods
Context
The setting for this study was the High Secure Inpatient Service (HSIS) in Queensland, Australia. The state of Queensland in Australia has an estimated population of 5.2 million. The HSIS provides a secure hospital environment for approximately 70 patients with an approximate bed rate of 1.34 per 100,000. Admitted patients have complex mental health treatment needs and include patients who have been found not criminally responsible by a court for an offence, who are unfit for trial, or who have been referred from the prison system or other hospitals based on their risk profile. Patients who have been charged with a serious offence and who are found of unsound mind or unfit for trial are managed under Forensic Orders (FO). Patients who lack the capacity to consent to treatment for their mental illness and have a range of challenging behaviours may be admitted to the HSIS and treated involuntarily under a Treatment Authority (TA). Patients who are transferred to hospital from a watch house or prison are admitted as classified patients and may be admitted voluntarily or involuntarily (TA – Classified).
HSIS offers patients a range of physical activity options, although these can be limited by staffing numbers and availability. A daily campus walk is offered with smaller group activities provided on a less regular basis. Group activities occur at the gymnasium and less frequently at the outdoor swimming pool, tennis court, exercise equipment and on the ward. The HSIS grounds allow for small groups to play modified sports such as touch football, soccer and volleyball. Attendance at physical activities offered outside the ward environment is limited to those who have permission to leave the ward environment with the treating team's approval. Historically, physical activity has been prescribed by the physiotherapist, exercise physiologist and/or personal trainer. At the time of the present study, the recreational officer and personal trainer were overseeing most of the physical activity occurring at HSIS.
Study design
This research used a mixed methods design incorporating a short paper-based questionnaire and a semi-structured interview with inpatients admitted to HSIS, to understand their experiences and perspectives with regard to their physical health and activity. The conduct and reporting of the qualitative elements of the study adhere to the Standards for Reporting Qualitative Research (O’Brien et al., 2014).
Researcher characteristics
At the time of the study, KM was working as an advanced forensic psychiatry registrar (forensic psychiatrist in training) at the HSIS. She was not the treating psychiatrist for any of the patients included in the study. KM had a specific interest in the physical health and activity of the patients in the HSIS due to her previous employment as a physiotherapist. KM's dual role as both a clinician and researcher likely shaped the depth and focus of the inquiry. Her previous experience as a physiotherapist gave her a unique awareness of the physical health challenges faced by patients, which in turn influenced the formulation of research questions. This clinical perspective may have prompted KM to explore specific barriers and seek practical solutions that other researchers, without a similar clinical background, might not have considered. Additionally, KM's experience of working at HSIS and her commitment to patient well-being likely informed her interpretation of the findings, particularly in highlighting the intersection of mental and physical health in individuals with serious mental illness. Had another researcher, with a different focus or background, approached the study, they might have taken a different angle, potentially leading to other conclusions or a varied emphasis on the data. Further, KM, was offered a hybrid position with clinical and research focus at a time when the Queensland Centre for Mental Health Research was in the process of developing a strong research portfolio in the area of multimorbidity with a view to addressing the life expectancy gap of individuals with serious mental illness due to physical illness. Additionally, in the context of national and state level policy priorities, to address these issues, there was an opportunity for research to inform future physical health policy and service reform. Concerns regarding conflict of interest or power differential were managed by ensuring that the written material and consent process highlighted to patients that their participation was voluntary and that a decision to take part or decline participation would not affect their routine treatment, relationship with their treating team or their relationship with the broader environment (The Park, Centre for Mental Health and Research).
Sampling strategy
Participants were eligible for the study if they were a current inpatient at HSIS, aged over 18 years, had a diagnosis of a major mental illness, defined as schizophrenia spectrum and other psychotic disorders, mood and anxiety disorders and severe personality disorders, and could provide informed consent to participate. Treating psychiatrists at HSIS nominated eligible participants to the researcher KM who then invited participants to partake in the study and assessed their capacity to consent. A $10 gratuity was offered to participants.
The researchers note that the low number of high security beds per population in Queensland limited participant numbers. The researchers aimed to recruit as many participants as possible across the course of the 12-month study. Other limiting factors to participant numbers related to capacity to consent to the study and length of stay.
Instruments and measures
The quantitative component of this study involved a paper-based survey comprising the following measures:
Demographics including gender, age, length of stay, ethnicity, diagnosis and type of order. Questionnaire for patients regarding physical activity using the Theoretical Domains Framework (TDF). Physical activity preferences as reported at interview. Experiences of physical activity. Physical activity preferences and motivating factors. Barriers to physical activity.
The qualitative component of this study included a semi-structured interview that aimed to cover the following topics:
Both the structured questionnaire and the interview script were developed based on the current literature. The questions were developed from the physical activity questionnaire (Taylor et al., 2013). Changes were made to reflect the forensic hospital setting and were outlined in written correspondence to the original developers on the 31/05/2018. The questionnaire covered the domains outlined in the TDF (Cane et al., 2012) and included questions relating to knowledge, skills, intentions, goals, social influences and beliefs about capabilities. The interviews were focused on identifying personal beliefs, current practices and preferences as well as barriers and facilitators to physical activity for patients under forensic mental health care. The questionnaire and interview questions are available in Supplementary Material.
Data collection
Following the consent process, participants were offered a structured questionnaire to complete in their own time. The semi-structured interview occurred in a private interview room on the hospital ward, at a time suitable for the participant. Data collection was undertaken between February 2019 and February 2020.
Interviews were not audio-recorded due to concerns that this would further limit patient numbers, in the context of a small target population. The interviewer (KM) wrote comprehensive notes regarding what participants said during the interview.
Data processing and analysis
Questionnaire
Questionnaire responses were entered in Excel, cleaned and reviewed for missing data. Analysis involved descriptive statistics that were used to summarise discrete variables from the structured questionnaire.
Interviews
Interview notes were analysed using a thematic framework method, which has been well described (Gale et al., 2013). Data were coded and analysed in accordance with the five stages of this method by one researcher (KM). Stage one comprised of familiarisation with the data which involved the reading and re-reading of the data and noting down initial ideas. The second stage involved the generation of codes for the data by both inductive and deductive approaches. A number of codes were pre-defined, for example ‘improved mental health’ and ‘improved physical health’ as these areas of interest have previously been linked to benefits of physical activity. Other codes, for example ‘achievement’, ‘self-esteem’ and ‘sleep’ were generated inductively following close examination of the data. The initial coding was completed in Excel. The final stages involved collating the codes into potential themes which were written onto a thematic map for better visualisation. This allowed overarching initial themes and sub-themes to be developed. Further review ensured that themes were coherent and were identifiable as different from each other. Finalised themes and sub-themes were discussed and agreed upon by all authors involved in the study. Included excerpts were chosen representatively.
There were no missing data as the semi-structured interview provided opportunity for the researcher to identify and capture any missing data in the questionnaire.
Results
There were 68 patients who were inpatients at HSIS at the commencement of the study and over the study period there were 59 admissions. Of 31 eligible participants who were referred by their treating psychiatrists, a total of 28 completed a study. Three patients declined to participate. Participant characteristics are shown in Table 1.
Participant characteristics.
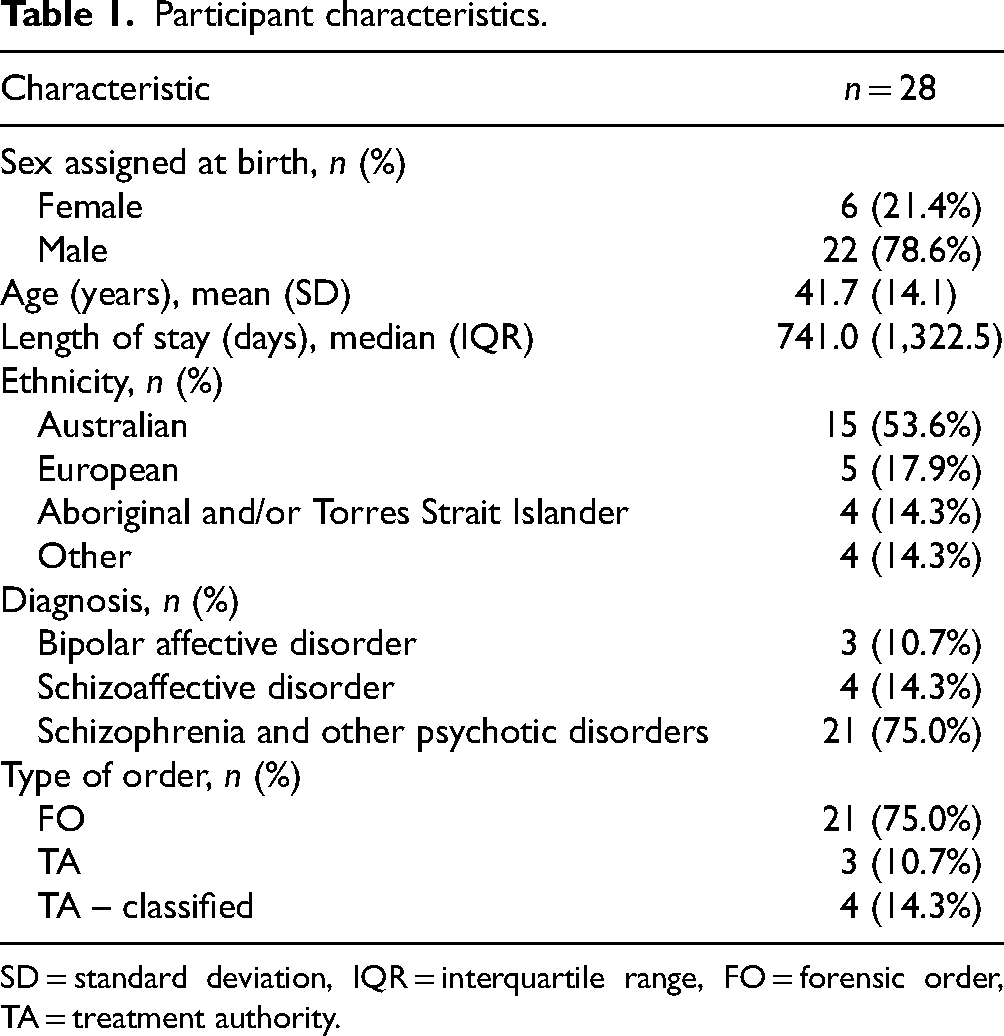
SD = standard deviation, IQR = interquartile range, FO = forensic order, TA = treatment authority.
Our thematic analysis revealed five main themes regarding physical activity knowledge, preferences, practices and barriers for patients under forensic mental health care. These included (a) while physical activity is viewed as important and beneficial, knowledge remains lacking; (b) patients have individual physical activity preferences, goals and motivations; (c) environmental context and social influences impact engagement in physical activity; (d) confidence and skills play a role in physical activity planning and adherence; and (e) perceived barriers to physical activity include individual, service-related and environmental factors. These five themes will be used as headings under which the relevant findings from both the questionnaire and interviews will be presented.
Physical activity is viewed as important and beneficial by patients under forensic mental health care, however, knowledge remains lacking.
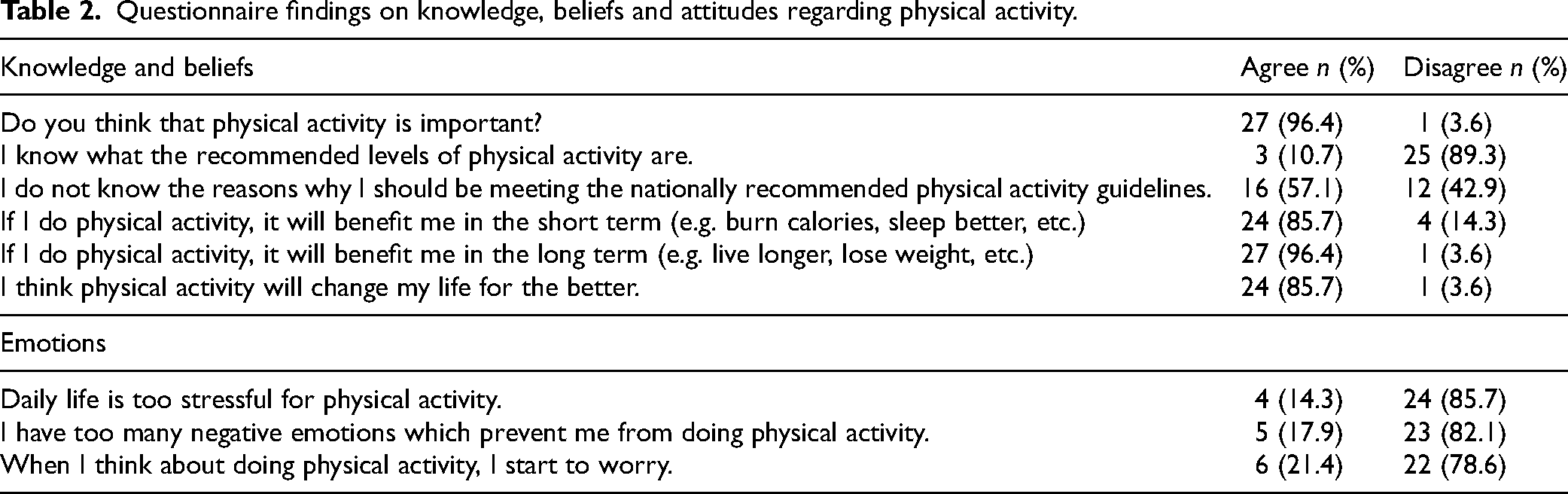
Questionnaire findings indicated that 96.4% considered physical activity to be important. However, more than half (57.1%) stated they had never read any information regarding physical activity guidelines. Although three participants indicated on the questionnaire that they were aware of the current World Health Organization's physical activity guidelines, no one was able to correctly state them. At interview, the majority (57.1%) were unable to describe why they should be doing physical activity, and only one participant recognised that there were various levels of intensity of physical activity.
The majority of participants (85.7%) wanted to engage in physical activity, with only 60.7% feeling any motivation to do so. Most participants felt confident with their skills, however some acknowledged that physical activity made them feel embarrassed (17.9%) and some felt inadequate when they compared themselves to their peers (21.4%). Problems with stress, negative emotions and worry were also noted as challenges in this cohort (Table 2).
Questionnaire findings on knowledge, beliefs and attitudes regarding physical activity.
While many participants had difficulty describing why they should be engaging in physical activity, they were able to reflect on experienced benefits. Table 3 outlines the range of benefits described by participants and includes both lower-level codes (e.g. medical illness, weight loss, muscle mass, etc.) being combined under higher-level codes (e.g. improved physical health and well-being).
Self-reported benefits of physical activity by forensic inpatients at interview.
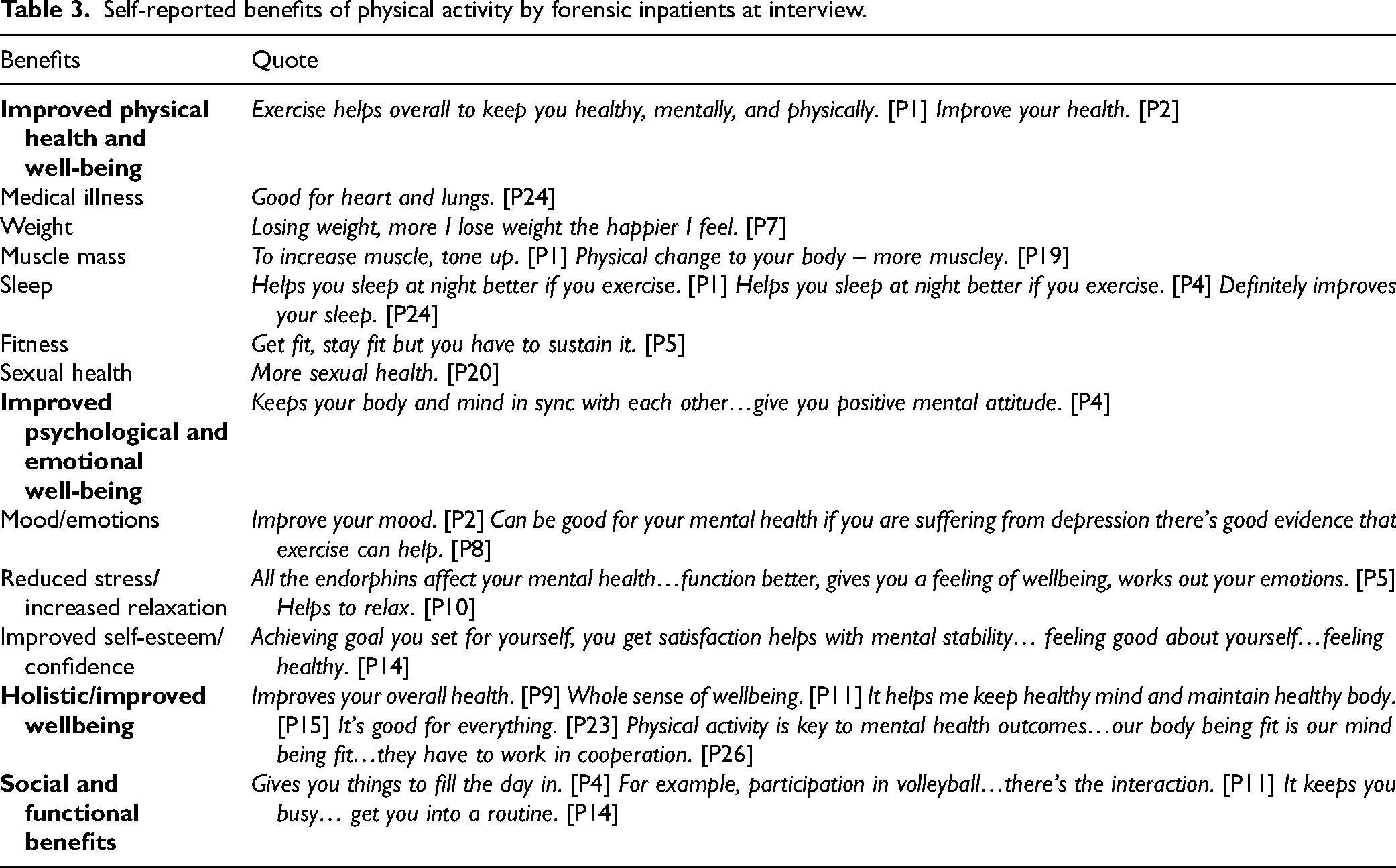
Short and long-term benefits for physical health and well-being were also noted. Short-term benefits that participants identified included weight loss, increased muscle tone, improved cardiovascular health, improved breathing and reduction in cravings. Weight loss was the most identified short-term benefit (35.7%), followed by cardiovascular related benefits (32.1%). Long-term benefits included prevention of health concerns, reduction in pain, longer life expectancy and improved overall physical health and fitness. Physical activity was also linked to better sleep quality.
A number of short- and long-term benefits were highlighted under the sub-theme of improved psychological and emotional well-being. The most reported short-term benefit of physical activity related to a positive impact on mood and thinking (50.0%). Participants identified a positive mental attitude, feeling good about oneself, improved confidence and relaxation as other short-term benefits of physical activity on their psychological and emotional well-being. Longer-term benefits included improved mental stability and satisfaction and achievement of goals.
Participants were able to identify that physical activity had a benefit beyond improvements in specific aspects of their physical and mental health and noted that physical activity provided opportunities for engaging in social activities and maintaining function.
2. Patients under forensic mental health care have individual physical activity goals, motivations and preferences.
Participants described their individual preferences and practices of physical activity in interviews (Table 4). The majority of participants (85.7%) reported that they would attend an organised physical activity program and over two thirds (67.9%) would give up their leisure time to attend. When a voucher was proposed to incentivise attendance, two participants who had concerns about their health stated that the voucher would influence their decision to attend.
Physical activity preferences and practices of inpatients under forensic mental health care.
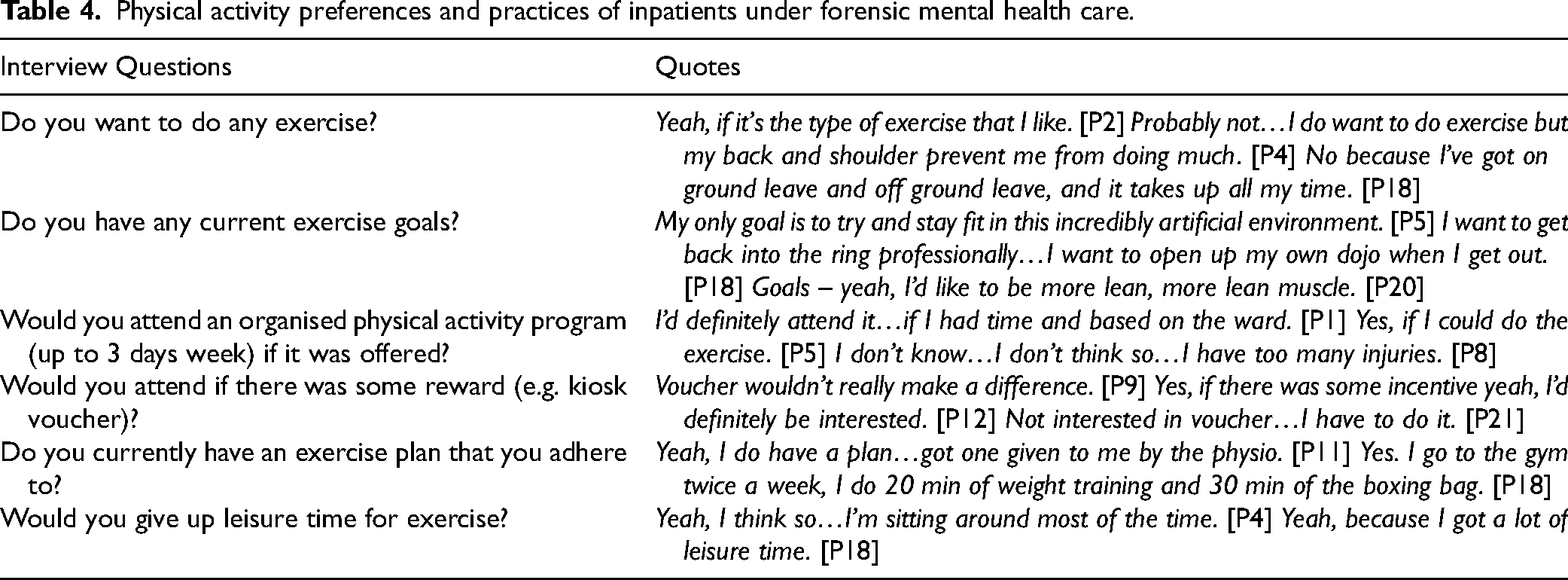
The most frequently reported preferred physical activity was walking (39.3%). Patients also endorsed going to the gym (32.1%), doing weights (28.6%), cardio/aerobic workouts (25.0%), jogging/running (21.4%) and swimming (14.3%). There was support for using equipment such as a treadmill (14.3%), exercise bike (14.3%) and rowing machine (3.6%). A number of patients were interested in groups sports including volleyball (10.7%) and indoor bowls (3.6%) and three patients preferred yoga/Pilates (10.7%).
Participants described a range of physical activity goals and motivations. In total, 82.1% of the study participants wanted to engage in physical activity. Thirteen participants (46.4%) reported a current goal. Goals included weight loss, improving muscle tone and strength, improving fitness, rehabilitation from injuries and getting back to previous sports and activities (e.g. golf, running, boxing, swimming).
3. The environmental context and social influences impact engagement in physical activity.
Results from both the questionnaire and interview confirm that the environmental context and social influences play a role in providing opportunity and motivation for patients to engage in physical activity (Table 5). While the majority of participants (78.6%) indicated on the questionnaire that there were facilities available for them to help them engage in physical activity, 25.0% identified that HSIS was not very attractive, and this put them off doing physical activity. Participants noted that there was availability of equipment (e.g. treadmill, exercise bike) on some wards. At interview, 12 participants reported that they did not mind where they engaged in physical activity while the gym was identified as a preferred environment for attending a group physical activity program by eight participants. Three participants preferred to exercise outside and one individual nominated the outside equipment and another the ward environment.
Environmental context and social influences.
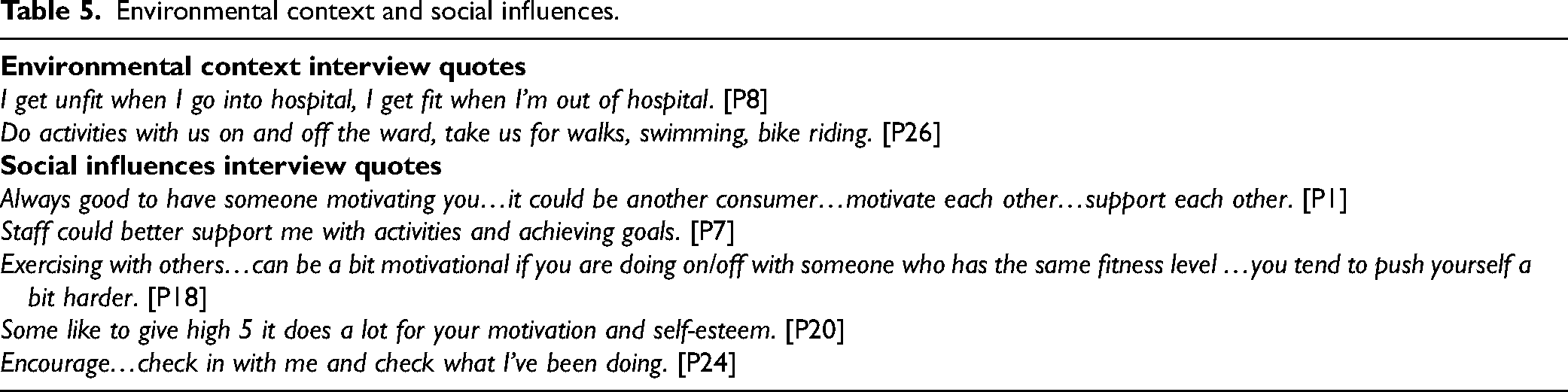
In terms of social influences, participants identified who they would like to exercise with and who they would like to oversee their physical activity. Results from the questionnaire indicated that 42.9% did not have friends/co-patients who participated in physical activity and 28.6% reported that they did not have anyone to undertake physical activity with. From analysis of interview notes, there was a noted desire to exercise with others, with only two participants reporting that they preferred to exercise alone. Participants noted that they felt increased motivation and support when exercising with peers.
A variety of answers were given when participants were asked who they would like to oversee their physical activity. No preference (28.6%) was the most common response, followed by the recreational officer (21.4%). Participants were also asked about their preferred environment for physical activity. The majority either did not indicate a preference (36%) or did not answer (10.7%). Of those that reported a preference, 28.6% stated the gym, 14.3% indicated outside and 3.6% proposed the ward environment.
The majority of participants (89.3%) reported that staff supported and encouraged their participation in physical activity. Participants offered a number of suggestions on how staff could further support them with their physical activity (Table 5).
4. Confidence and skills play a role in physical activity planning and adherence.
Participants expressed varying levels of confidence in their ability to engage in physical activity (Table 6). While 96.4% indicated that they felt confident about their capabilities on the questionnaire, at interview participants mentioned limitations due to physical conditions and injuries affecting their confidence to undertake physical activity. The majority (78.6%) believed that they could exercise to a good enough standard. The rest proposed a range of concerns they had including poor skills, effects of medications and lack of time and equipment.
Capabilities and skills as reported by patients under forensic mental health care.
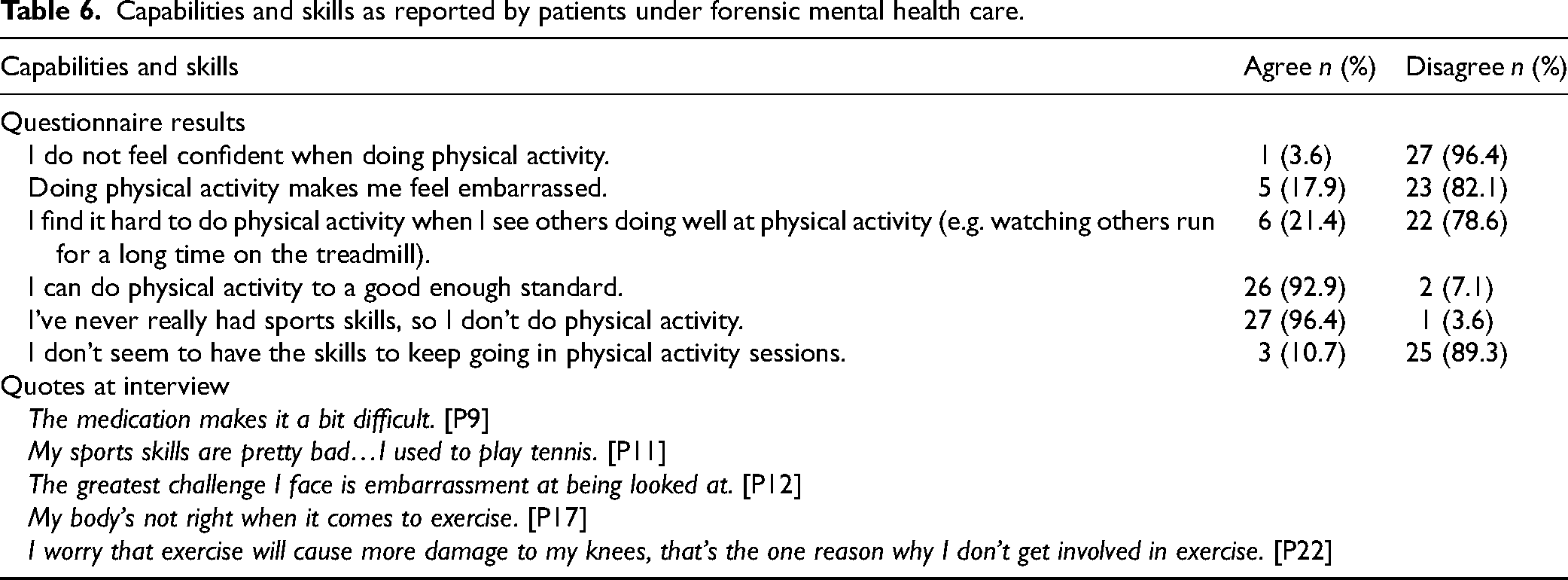
Approximately two thirds (67.9%) of participants indicated on the questionnaire that they planned where to undertake physical activity, with the majority of participants (78.6%) reporting that they also planned when they would undertake physical activity. Four participants (14.3%) advised that they did not plan what physical activity they would undertake. At interview, participants shared their exercise plans and routines. While it was clear that some participants adhered to regular exercise routines, others had difficulty adhering to their plans due to a number of factors including a lack of confidence and skills.
5. Barriers to physical activity include individual, service-related and environmental factors.
Participants reported various barriers to engaging in physical activity (Table 7). The majority of patients (75.0%) identified their physical health as a significant barrier to physical activity. This related to co-morbid medical illness (64.3%), weight issues (14.3%) and poor fitness (3.6%). It was also noted that body weight and weight-gain impacted physical activity choices. The most commonly identified health concern impacting on a decision to engage in physical activity related to knee pain (25.0%), followed by back pain (21.4%) and shoulder pain (17.9%).
Identified barriers to physical activity at interview.
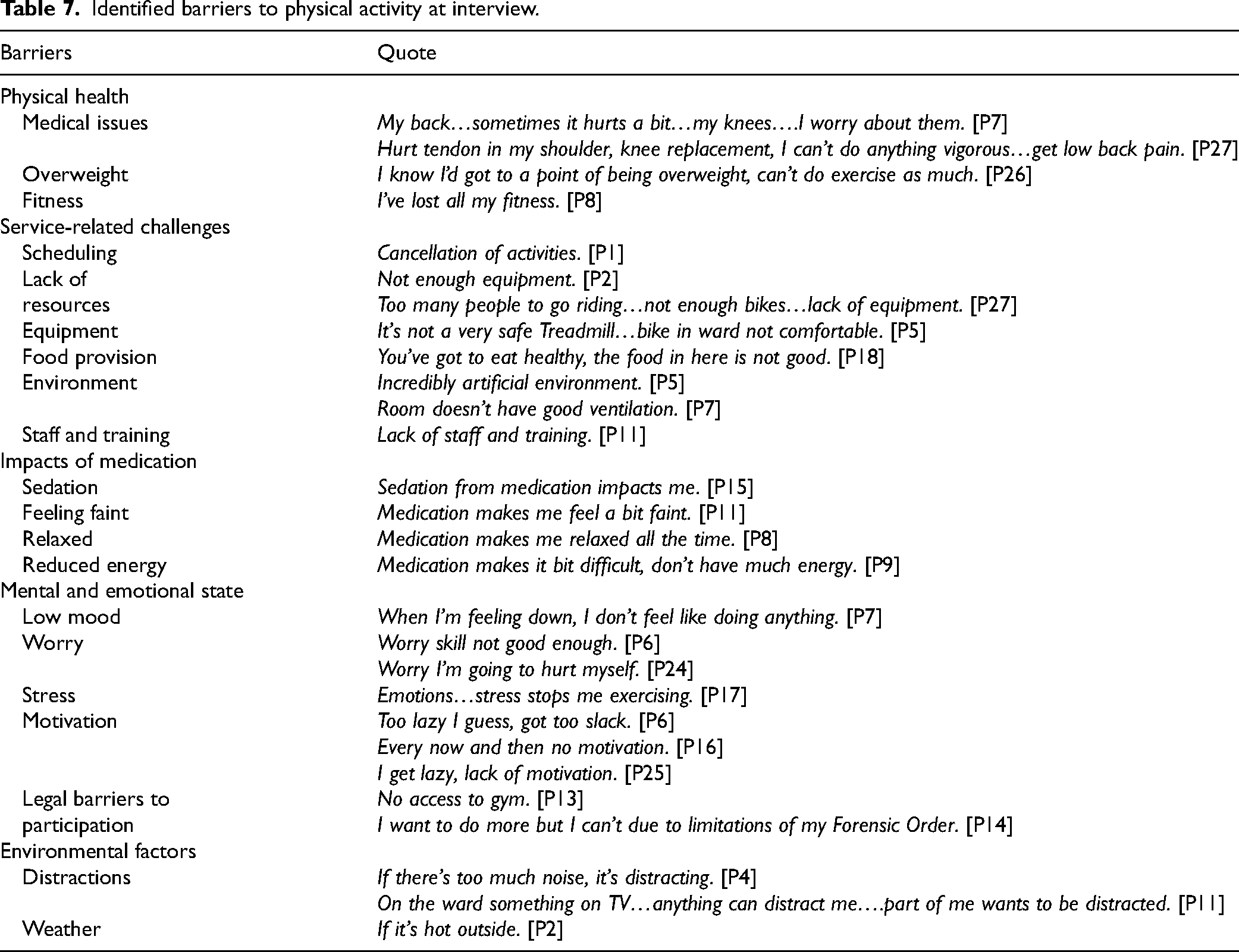
There were a number of service-related challenges identified. Participants noted a lack of resourcing (e.g. insufficient equipment availability, lack of variety in exercise options, need for better equipment), staffing issues (e.g. insufficient staff presence and support, need for better training and supervision), problems with equipment (e.g. safety and comfort issues), problems in the environment (e.g. rooms not having good ventilation) and lack of scheduling of regular physical activity. Two participants identified issues with the food that was provided on the ward as impacting on their weight and therefore their ability to engage in activity.
Other barriers related to the impacts of medication on an individual. There were significant concerns raised regarding medication side-effects, particularly around sedation (43%), and other impacts such as feeling faint, too relaxed and having reduced energy. While weight-gain and metabolic risk is a common consideration for prescribers of antipsychotic medications, interestingly, patients in this study did not report concerns of weight-gain linked to medication usage.
Another concern raised by participants related to their mental and emotional state. Mental state was frequently raised as being a barrier, with concerns around low mood/poor mental state, stress and worry. Physical activity was seen as a positive coping mechanism for stress and working out emotions. A deteriorated mental state was noted to affect both motivation and participation.
Lack of motivation was another common sub-theme raised as a barrier to physical activity by 60.7% of the group. There were significant challenges with finding motivation to exercise, variability in motivation levels and struggles with perceived laziness. Some participants noted that their motivation levels varied, and they had difficulties in staying motivated consistently.
A sub-theme relevant to a forensic hospital was legal barriers to participation. In particular, restrictions on movement (related to conditions of participants’ orders under Mental Health Act legislation) prevented some participants from attending the gym on the hospital grounds, a community gym off hospital grounds, and being able to undertake longer walks unescorted.
Environmental factors comprising the weather and environmental distractions was another identified sub-theme. Three participants (10.7%) noted that the weather played a role in their accessibility to exercise, as they preferred to exercise outside. There were also a range of distractions that participants reported impacted their intent to engage in physical activity including a busy and noisy ward, outside noises, the television, phone calls and going to the canteen.
Discussion
Our study aimed to capture the individual perspectives of inpatients under forensic mental health care on physical activity knowledge, preferences, practices and the benefits and challenges faced in a forensic hospital environment, and the support needed for patients to be engaged in physical activity. Participants’ responses highlight the multi-dimensional nature of physical activity engagement and the complex interplay of physical, mental, service-related and environmental factors that influence patients’ physical activity choices and experiences. Five themes were identified including (1) while physical activity is viewed as important and beneficial by patients, knowledge remains lacking; (2) patients have individual physical activity preferences, goals and motivations; (3) environmental context and social influences impact engagement in physical activity; (4) confidence and skills play a role in physical activity planning and adherence; and (5) perceived barriers to physical activity include individual, service-related and environmental factors.
We found that physical activity was viewed as important and beneficial. When discussing the importance of physical activity, participants described a strong link between their physical and mental health. Physical activity was described as a way to keep both the body and brain working, contributing to a sense of well-being and having a healthy mind. This is similar to other studies that have reported that patients regard physical and mental health as being inseparable (Blanner Kristiansen et al., 2015). There were gaps in patient knowledge regarding why physical activity was important and the recommended guidelines for physical activity despite patients identifying that engaging in physical activity was important for their physical and mental health and well-being. This lack of awareness is not specific to mental health patients (Chen et al., 2022). This suggests that while patients have a lived experience of the benefits of physical activity, many have knowledge gaps regarding why and how physical activity contributes to improved health and well-being (e.g. prevention of specific medical conditions, impact on cardiovascular risk factors).
These findings have implications for forensic services and highlight the need for further education. While there has been some conjecture regarding the benefit of education as a behavioural change intervention (Albarracin et al., 2024), the TDF has identified knowledge as an important influence on some health behaviours (Cane et al., 2012). A lack of knowledge about how physical activity improves health (e.g. reduces risk of chronic diseases) can be a barrier to engaging in it. The long-stay nature of hospitalisations for patients under inpatient forensic mental health care allows time for both physical activity guideline education and opportunity. Enhancing knowledge can assist patients in making more informed decisions, and therefore targeted education for this population should be considered. In turn, this contributes to a more comprehensive and effective approach to holistic treatment and recovery (Public Health England, 2021).
An important finding of this paper was that patients under forensic mental health care have individual physical activity preferences, goals and motivations and engagement is impacted by the environmental context and social influences. This is in keeping with the TDF which highlights that capability, opportunity and motivation interact to produce behaviour (Cane et al., 2012). Motivation comprises attitudes, norms and intention (Albarracin et al., 2024) and interventions can target both intrinsic motivation (enjoying physical activity for its own sake) and extrinsic motivation (e.g. for weight loss, health benefits). Importantly, understanding what the preferences and achievable goals are for individuals under forensic mental health care is crucial for sustaining physical activity, promote progress and to enhance motivation. Our study found that walking was the preferred form of physical activity with a preference for a known staff member (e.g. recreational officer) or other health professional to be providing oversight. This is in line with other research findings (Chapman et al., 2016). It was noted that individual preferences varied widely, based on personal experiences, physical limitations and personal interests. Forensic services need to consider individual needs and offer a range of opportunities in addition to walking in order to enhance engagement of patients in physical activity (e.g. group sport, gym, cardiovascular workouts, swimming, bike riding, strength training, yoga and Pilates).
Social influences can have a powerful impact on an individual's motivation and commitment to physical activity (Biddle & Mutrie, 2008). In this sense, staff and patient perspectives are both important. Our study noted a desire by patients under forensic mental health care to undertake physical activity with others. This was in line with findings of research examining factors influencing prisoners’ engagement in exercise (Hammond et al., 2024). This research highlighted the social aspects of exercise to increase self-motivation and to make exercise more enjoyable. Physical activity within a supportive environment can therefore enhance internalising motivation and minimise barriers to engagement. Having co-patients who encourage and participate in physical activity can be a strong motivator. In particular, group activities provide opportunities for social interaction and create accountability, increasing the likelihood of regular participation.
Staff have an awareness of the secure environment and have expertise in providing health care for inpatients. Staff as positive role models has been shown to improve health outcomes in various studies (Bacon et al., 2012; Day & Johnson, 2017). However, studies from other secure inpatient services have highlighted that staff can find it challenging to provide an engaging environment for patients and studies of patient perspectives identify the additional challenges of engagement in secure settings that can be monotonous, with limited purposeful activities and opportunities for social engagement (Davies et al., 2023; Walker et al., 2022). In our study, participants reported that staff were supportive and encouraging. Forensic services need to recognise and harness these influences to create a supportive environment that promotes regular physical activity. If being active is valued and encouraged by forensic services (staff, environment), patients are more likely to engage in it. Previous studies have reported the benefits of using exercise specialists in the provision of exercise interventions for patients with severe mental illness and this should be incorporated by forensic services (Korman et al., 2018).
The environmental context and available resources play a significant role in influencing patients’ engagement in physical activity (Glowacki et al., 2018). The built environment, access to facilities, outdoor spaces and the overall surroundings can either promote or hinder opportunities for physical activity. While the majority of participants in our study (78.6%) reported that there were facilities available to help them engage in physical activity, 25% indicated that the hospital environment was not aesthetically pleasing and that this influenced their decision to not engage in physical activity. Forensic services need to consider the built environment and provide regular access to gyms and other facilities to engage patients in a range of structured physical activities.
Physical activity has been shown to improve confidence in patients under forensic mental health care (Wynaden et al., 2012). In turn, confidence is associated with a sense of satisfaction, accomplishment, stress relief and overall well-being and plays a significant role in physical activity planning and adherence. Positively, our study demonstrated that the majority of participants felt confident about their capabilities and planned both where and when they would undertake physical activity. However, there remained challenges around goal setting and physical activity opportunities. Concerningly, there were a number of patients who conceptualised themselves as ‘lazy’. Forensic services need to support patients to create and achieve realistic physical activity goals in order to enhance intrinsic motivation and challenge schemas of laziness. Effective planning (specific goals, allocated time and plans for potential obstacles) will enhance and support physical activity adherence, motivation and persistence.
Our findings support previous research that physical activity is beneficial for patients under forensic mental health (Anthony et al., 2023). In particular, participants reported improvements in both their physical and mental health and overall well-being in both the short and longer term. Five participants noted that engaging in physical activity would increase their life expectancy. This is significant given the finding that patients with severe mental illness continue to have a mortality rate of 2.2 times that of people without, and an average of 10 years of potential lost life (Walker et al., 2015). The reported social and functional benefits may counteract the concerns voiced by previous forensic populations that they are bored in hospital and that weight-gain was something out of their control (Every-Palmer et al., 2018; Farnworth et al., 2004).
The concerning response that ‘I get unfit when I go into hospital, I get fit when I’m out of hospital’ has been reflected in previous research that reported 78% of study participants believed that they were more active in the community than as forensic inpatients (Every-Palmer et al., 2018). Our study found that 29% of participants identified their current health status as the most significant challenge to physical activity. The concern study participants had regarding their current physical health status contributing to physical activity engagement has been documented as a barrier to healthy lifestyle changes in prior studies (Blanner Kristiansen et al., 2015). Other commonly identified barriers related to sub-themes of physical health problems (co-morbid medical illness, obesity and poor fitness), service-related challenges (lack of resourcing, staffing, problems with equipment and the environment), the impacts of medication (particularly sedation) and motivation. These barriers are similar to previously identified barriers in forensic settings (Anthony et al., 2023).
Strengths and limitations
One strength of this study was that qualitative analysis encompassed a broad range of information relating to patient knowledge, preferences, practices and patient identified benefits and barriers in regard to physical activity. Inclusion of quantitative data supported the findings of the qualitative data.
Another strength is that the sample for this study is broadly representative of other forensic population in Australia in that there was a high proportion of male participants and an over-representation of Aboriginal and Torres Strait Islander peoples. We think the most significant factor to engagement related to the secure environment setting in respect to which this offered a novel and enjoyable interaction. If an Aboriginal or Torres Strait Islander researcher had been available, this may have encouraged greater engagement. There may have been differences in views due to different gender and cultural background but the sample was not large enough to draw these out.
Another limitation was that the interviews were not audio-recorded. This was a considered decision to increase participant numbers due to concerns that recording patients with persecutory thoughts could impact their mental state and reduce voluntary participation. The interviewer was deliberate in her attempts to document verbatim what was reported by participants. Future research considering this issue could offer participants the choice of being audio-recorded. This would provide autonomy for individuals while recognising that some individuals with symptoms (such as paranoia) have a lower level of comfort with audio-recording (Briggie et al., 2016).
Conclusion
Our study explored the perspectives of mental health inpatients on physical activity knowledge, preferences and practices, highlighting both the benefits and challenges experienced within a forensic hospital environment. Through the exploration of five distinct themes, our analysis has highlighted the complex interplay of physical, mental, environmental and service-related factors that shape patients’ engagement in physical activity. This research emphasises the role of education in enhancing patients’ knowledge about the significance of physical activity, coupled with a need for tailored support to address individual preferences, goals and motivations. Social influences in promoting group activities, the impact of environmental context on physical activity opportunities, the pivotal role of confidence in adherence, and the array of multi-faceted benefits associated with physical activity were all notable findings. Furthermore, the study endorses the finding that hospitalisation can impact physical activity engagement and highlights the importance of addressing barriers related to physical health status, service challenges, medication side-effects and motivation. To assist recovery and improve outcomes, forensic services must proactively integrate physical activity into the comprehensive treatment framework for patients under forensic mental health care, thereby contributing to holistic well-being and improved outcomes.
Supplemental Material
sj-docx-1-fmh-10.1177_14999013251315479 - Supplemental material for Physical activity of inpatients under forensic mental health care: A mixed methods study of patient knowledge, preferences, practices and identified barriers
Supplemental material, sj-docx-1-fmh-10.1177_14999013251315479 for Physical activity of inpatients under forensic mental health care: A mixed methods study of patient knowledge, preferences, practices and identified barriers by Katherine Moss, Carla Meurk, Megan L. Steele and Ed Heffernan in International Journal of Forensic Mental Health
Footnotes
Ethical approval
Ethical approval was granted by the West Moreton Health Human Research Ethics Committee (HREC/18/QWMS/67) and the University of Queensland (clearance number 2018002132).
Consent to participate
The researchers ensured that participants had capacity to consent to participating in the study to ensure that their human rights were upheld. In addition, eligible participants were assured that their participation was voluntary and that a decision not to participate would not affect their routine treatment or their relationship with the treating team. Participants were also advised that they were free to withdraw from the study at any time.
Author contributions
KM analysed and interpreted the patient data and was a major contributor in writing the manuscript. All authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the Royal Australian and New Zealand College of Psychiatrists,
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.