
Abstract
Involuntary treatment orders can be used to compel individuals deemed incompetent to receive care that is considered necessary for their health condition. This article describes the varying perceptions of the legal procedures associated with involuntary treatment orders. Semi-structured interviews were conducted with 40 participants (service users, family members, healthcare professionals, and lawyers). The overarching theme “at the intersection of legal and clinical issues” captures the ways in which involuntary treatment orders are experienced and used at the crossroads of two distinct systems. Three interrelated themes were identified. The first theme, The Construction and Negotiation of Involuntary Treatment Orders, examines how involuntary treatment orders are shaped through formal legal criteria, informal clinical reasoning, institutional norms, and strategic negotiation, often revealing tensions and overlaps between legal and clinical logics. The second theme, Relational Dynamics in the Initiation of Involuntary Treatment Orders, focuses on how interpersonal interactions among different key actors influence perceptions of fairness, legitimacy, and coercion in the process surrounding involuntary treatment orders. The third theme, Barriers and Inequities in Access to Justice, highlights how structural, procedural, and psychosocial factors constrain service users’ ability to exercise their rights and shape unequal experiences within the legal process.
Introduction
For individuals living with mental health disorders who are deemed incompetent to consent to their care and categorically refuse their care, an involuntary treatment order may be a means to compel them to receive treatment considered necessary for their health. These court-ordered treatments may be initiated during a hospitalization or in the community. Although involuntary treatment orders fall under legislation that can be applied broadly across various settings, in practice, they are predominantly used in psychiatric contexts (Perrault & Bernheim 2023). Their use assumes that treating a person against their will can sometimes be essential to their recovery and is, therefore, in their best interest based on the principle of beneficence; though debates persist as to whose best interest is ultimately considered (Newton-Howes, 2019). Recent statistics from the Ministry of Justice (2021) show a steady increase in the use of involuntary treatment orders in Québec (Canada), with a rise of over 49% in requests submitted between 2015 and 2020, a trend also observed internationally.
Criteria for Involuntary Treatment Orders
The criteria for issuing an involuntary treatment order are defined in sections 10 and onward of the Civil Code of Quebec. In the case of F.D. v. McGill University Health Centre, the Quebec Court of Appeal developed a two-step analytical framework that clarifies the list of criteria to follow when assessing an involuntary treatment order. The first step is to determine whether the situation is under the judge's or the tribunal's jurisdiction. Then, two essential conditions must be met: incompetence to consent and categorical refusal of the treatment deemed necessary for the person's health. If either of these conditions is not met, the court must dismiss the application. Incompetency to consent is not defined by the law. In the context of an involuntary treatment order, it emerges as the conclusion of an evaluative process supported by case law and legal doctrine. The incompetence to consent will be considered if the overall responses to the following questions indicate a lack of understanding of their situation: (a) Do they understand the nature of the illness for which treatment is proposed? (b) Do they comprehend the nature and purpose of the treatment? (c) Do they grasp the risks and benefits of the treatment if they undergo it? (d) Do they understand the risks of not undergoing the treatment? (e) Is their ability to understand affected by the illness? These questions are commonly referred to as the “Nova Scotia criteria,” which, as a province, unlike Québec, has integrated them into its legislation. If the first two conditions are met (incompetence to consent, categorial refusal), the second step of the analytical framework invites a closer examination of the treatment plan necessary for the health of the individual. In this regard, the judge or tribunal must determine whether the treatment is necessary for the health of this person and is described with sufficient precision, whether it offers more advantages than disadvantages for the individual, and whether the duration of the requested involuntary treatment order is adequate to achieve the treatment plan's objectives. Unlike other jurisdictions, Québec law does not require dangerousness or a severe mental disorder to justify an involuntary treatment order.
Legislative Issues
Legislative discrepancies between Canadian provinces and other Western countries in terms of the criteria required for an involuntary treatment order or a community treatment order influence its definition and, consequently, its use and scope. Depending on legislative context, an involuntary treatment order may refer to an obligation of care both during and after hospitalization (e.g., Quebec) or exclusively within the community in jurisdictions where involuntary hospitalization automatically entails a treatment requirement. The goals of an involuntary treatment order are generally to improve treatment adherence, reduce the phenomenon of revolving-door admissions, increase clinicians’ ability to manage risks, and encourage recovery (Navaratnarajah et al., 2021).
A comparative study of 32 Commonwealth countries’ legislation on community treatment orders has also highlighted disparities in its application (Fistein et al., 2009). The authors of this review suggest that certain practices and legislation deviate from best practices and are therefore inadequate in terms of protecting the rights of people with mental health issues. In this regard, the United Nations Convention on the Rights of Persons with Disabilities (2007, Article 25) states that “State Parties shall require health professionals to provide the same quality of care to persons with disabilities as to others, including on the basis of free and informed consent by, inter alia, raising awareness of the human rights, dignity, autonomy and needs of persons with disabilities through training and the promulgation of ethical standards for public and private health care.” Concerning involuntary treatment orders, some authors propose prioritizing an approach focused on supporting individual rights and quality of care by questioning the objectives and desired effects of this coercive mechanism (Sashidharan et al., 2019). In Québec legislation, the predominant use of involuntary treatment orders in psychiatric contexts reflects the biomedical model of psychiatry that prevails in most countries and raises questions about its alignment with the principles of the Convention on the Rights of Persons with Disabilities, given the continued reliance on coercive interventions.
Two meta-syntheses of qualitative literature conclude that involuntary/community treatment orders use is driven not only by therapeutic adherence but also by the need to manage violence risk towards oneself or others, reflecting practices in Québec (Goulet et al., 2020; Lepping & Malik, 2013). Although dangerousness is not, by itself, a relevant factor for issuing an involuntary treatment order in Québec, it can become relevant when the judge or tribunal considers whether the necessary treatment provides more benefits than risks and as a means of preventing violence. The service users’ understanding of the involuntary treatment order is also closely linked to the issue of violence risk (Goulet et al., 2023).
Ethical and Clinical Issues
The increasing use of this legal mechanism prompts questioning regarding the reasons for this shift, especially as studies struggle to clearly demonstrate its clinical effectiveness. For instance, an umbrella review of systematic reviews and meta-analyses reported inconclusive benefits with the use of community treatment orders regarding subsequent health service use, follow-ups, inpatient admissions, and other clinical and forensic outcomes such as treatment adherence and criminal justice contacts (Kisely et al., 2024). Significant ethical concerns remain regarding the legitimacy of involuntary/community treatment orders, as they constitute a coercive response in balancing individual freedom and societal protection. Its application and whether these practices remain consistent with their intended purposes and aligned with human rights standards merit further examination.
A meta-synthesis of 44 qualitative studies identified different key themes related to involuntary treatment orders through key actors’ perspectives, including coercion as leverage, blurred lines between protection and abuse, coping through compliance, tension between advocacy and control, and the challenges of therapeutic relationships in coercive contexts, and family members feeling responsible yet sidelined (Goulet et al., 2020). Patients also expressed a lack of understanding of the legislation and procedures associated with community treatment orders, and family members reported dissatisfaction with certain aspects of the process (Corring et al., 2019). Similarly, an integrative review from de Waardt et al. (2022) reported mixed perspectives on the use of community treatment orders from patients, significant others, and mental health workers, though a common theme was the coercive and stigmatizing nature of this measure. Despite these knowledge syntheses on the subject, very little is known about the experiences of the different actors involved in the legal processes surrounding involuntary treatment orders and community treatment orders.
Given this gap in knowledge and Québec's unique and complex legislative context, it is essential to explore the perspectives of key actors involved with involuntary treatment orders in order to improve the processes and legislation. While previous papers have addressed the main clinical issues (Goulet et al., 2023; Lessard-Deschênes & Goulet, 2022), this study specifically aims to describe the various perceptions of the legal procedures associated with involuntary treatment orders. By doing so, it contributes to a more comprehensive understanding of how these procedures are experienced and interpreted by those involved—knowledge that is critical for informing future reforms, promoting procedural justice, and supporting more equitable and context-sensitive practices in the use of involuntary treatment orders.
Method
Design
A descriptive qualitative design with an organizational participatory research approach (Bush et al., 2018) was used. Stemming from a constructivist standpoint, multiple realities are acknowledged, based on the assumption that only human experience can be known (Avenier, 2011). Since the legal processes surrounding involuntary treatment orders are experienced by individuals occupying various roles, exploring these multiple realities can deepen our understanding of the phenomenon and support the construction of a more nuanced interpretation of this experience, one that allows for the coexistence of diverse perspectives. A patient partner was also involved in the development of the protocol, in data collection, and in the analysis.
Setting and Sample
The study was conducted in three mental health and forensic psychiatry institutes in the province of Quebec. The general and forensic psychiatry departments of each institute were solicited, including the follow-up of individuals under involuntary treatment orders in hospital and community settings.
Individuals who had been subject to an involuntary treatment order (n = 6), family members (n = 5), healthcare providers (psychiatrists, nurses, social workers, criminologists, occupational therapists) (n = 24), and lawyers (n = 5) were recruited, for a total of 40 participants. A convenience sampling strategy was used to maximize variation in characteristics likely to influence perspectives on the involuntary treatment order experience (geographic location, diagnoses, settings, professional disciplines). Recruitment was planned to continue until data saturation was reached, which usually occurs between 5 and 12 participants per group (Creswell & Poth, 2017), but the COVID-19 pandemic forced recruitment to be terminated before reaching this target. Recruitment strategies, along with inclusion and exclusion criteria, have been previously presented in a specific article on clinical issues (Goulet et al., 2023).
Data Collection
All interviews and data collection were centered on the use of involuntary treatment orders for individuals diagnosed with mental health conditions. Semi-structured interview guides were developed for the various participant categories based on themes derived from a meta-synthesis on involuntary treatment orders (Goulet et al., 2020). While the formulation of questions was adapted slightly for each group, the core topics covered were consistent across: understanding of the legal criteria for an involuntary treatment order; experience of the legal process; communication and information-sharing; involvement in decision-making; perceived or lived impacts of the involuntary treatment order; and recommendations. Interviews lasting between 30 and 90 min were conducted in person with each participant by the lead author, the patient partner, or a graduate student (CLD).
Analysis
Interview recordings were fully transcribed and imported into QDAMiner software (version 6.0.2). A thematic content analysis was conducted iteratively for each participant group, following Miles et al. (2019). This iterative process involved a cyclical analysis between coding and theme development: each interview was coded using a codebook informed by the literature, while remaining open to the emergence of new codes. Coding and themes were continuously refined through regular team discussions. Summary sheets were produced for each stakeholder group to highlight commonalities and differences across interviews.
Ethical Considerations
Scientific and ethical approvals were obtained from the three mental health institutes participating in the study.
Results
Three main themes emerged from the analysis and are grouped under the overarching theme, At the Intersection of Legal and Clinical Issues: (1) construction and negotiation in practice; (2) relational dynamics between the various actors and their influence on the perceptions of fairness and coercion; and (3) barriers and inequities in access to justice (see Figure 1). The results represent the varied perspectives of different groups of actors. When a particular group is not mentioned in relation to a theme, or when instances of agreement or disagreement between groups are not specified, it indicates that it did not emerge clearly from the data.
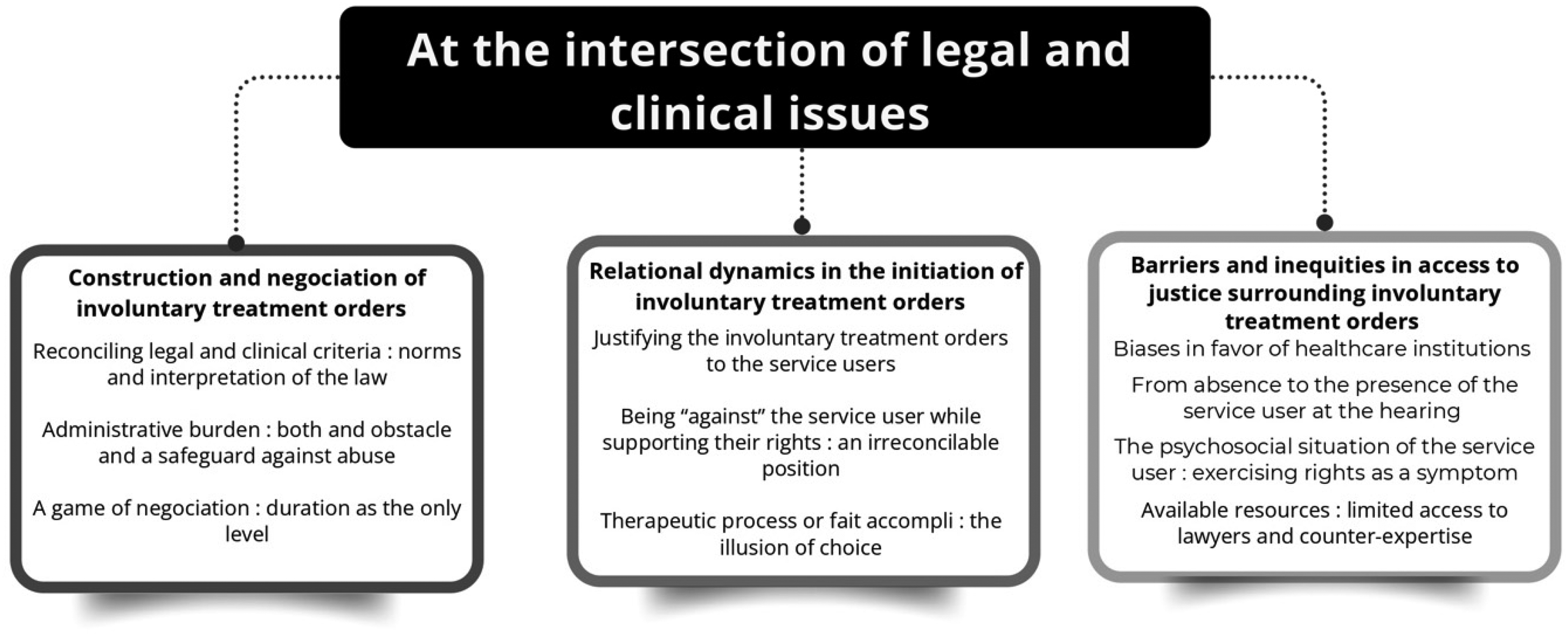
Overarching Themes, Themes, and Subthemes.
The Construction and Negotiation of Involuntary Treatment Orders
This theme explores how involuntary treatment orders are shaped through professional judgments, institutional norms, informal knowledge, and strategic interactions.
Reconciling Legal and Clinical Criteria: Norms and Interpretations of the Law
Defense lawyers and hospital staff clearly outlined the criteria for incompetence and categorical refusal. These formal criteria structure hearings, although a certain gray area persists in their interpretation and operationalization. “The criteria for the involuntary treatment order have become more restrictive. (…) They are really focused on categorical refusal. But, there's always a way … There are always gray areas in psychiatry. For instance, someone who takes medication only in the hospital but will likely stop upon release, well, we have to demonstrate that this has frequently happened in the past, or that the person's statements suggest a utilitarian approach.” (Criminologist 13)
In addition to these formal criteria, other factors, while not explicitly recognized by legislation, influence decision-making. These include the person's potential danger to themselves or others, a concern heavily discussed among all participants. The adversarial process (service user versus the treatment team), which emphasizes the obligation to convince the judge, sometimes encourages an exaggeration of the service user's situation by the hospital staff. This perception is noted by service users, psychiatrists, and lawyers alike. According to lawyers and psychiatrists, the focus on dangerousness in assessing the benefits and risks of the treatment plan, rather than the individual benefits to the service user or on incompetence or categorical refusal, not only influences the treatment team's decision to pursue an involuntary treatment order but also the judge's ruling. Dangerousness can thus be seen as an informal criterion to argue for an involuntary treatment order. “The client has a very high potential for danger, so we decided we should try. If the judge says no, they say no, but I feel like I need to try. So I think judges understand that too.” (Psychiatrist 12) “An involuntary treatment order is not issued because the person is dangerous. This is a possible criticism I would direct at professionals. They present the case this way, even though the focus should be on incompetence. When presenting the case, they will discuss this angle. It surely provides an image for the judge: ‘Oh, look at what happens when she's untreated.’ But I think the focus should be more on incompetence, categorical refusal, and necessity.” (Lawyer 2)
Concerning legal professionals, questions arise about their training on the specific mental health issues, as well as on the norms applied in practice. “They [the judges] want to diagnose themselves. They have to assess mental illness on their own. They are in no way able to make a diagnosis, nor do they have the competence or experience to truly understand … But they have to evaluate it. And even if violence is not a criterion in the treatment order, if there is violence, it triggers certain ‘red flags,’ and we’re going to include it because of that.” (Psychiatrist 3)
Some psychiatrists also see the necessity of hospitalization as an implicit criterion. Indeed, all examples cited by participants refer to situations in which the person was hospitalized. One psychiatrist questions this implicit norm: “I don’t understand why the patient has to be hospitalized to get an order; that has always puzzled me. (…) Sometimes patients are in accommodation resources, clearly struggling with their illness and needing treatment, but not necessarily in the hospital.” (Psychiatrist 6)
Among the participants who have or had an involuntary treatment order, one participant demonstrated a fairly good understanding of the criteria related to the involuntary treatment order; the others all reported a lack of knowledge or believed that their presumed dangerousness was the reason for the involuntary treatment order. “My lawyer didn’t explain that to me. If I had understood the criteria, I wouldn’t be under a treatment order.” (Patient 3)
The complexity of the clinical criteria, combined with the legal ones, creates confusion among health and legal professionals, contributing to occasional misinterpretations or informal assessments of the individual's situation and the process surrounding the involuntary treatment order. Generally, unlike psychiatrists and lawyers, service users, family members, and other healthcare providers develop informal understandings of legal mechanisms, their knowledge derived from experiential and clinical knowledge rather than from formal legal training, thereby creating a gap between their “legal culture” and the formal legal mechanisms.
Administrative Burden: Both an Obstacle and a Safeguard Against Abuse
The procedures surrounding the involuntary treatment order are administratively complex, time-consuming, and require collaboration among multiple actors within the healthcare network, as well as the drafting of expert reports. This administrative burden has two significant consequences. First, it favors service users who refuse the proposed treatment. Professionals may be discouraged by the administrative processes—a participant noted that “some psychiatrists might just choose not to do it.” It's not a process the treatment team “tries out”; they only undertake it when they are confident the legal criteria are clearly met. In this regard, although the burden of proof required is the balance of probabilities, healthcare institutions apply a stricter threshold when deciding to initiate an involuntary treatment order. The second consequence is that the administrative complexity has the opposite effect of increasing the requested involuntary treatment order duration by some treatment teams. Furthermore, from the service user perspective, they either felt that the assessment in follow-ups was not up-to-date or that it was not reviewed at all. “Justice sets a high bar because it's about defending individual freedoms, which is very important and necessary, but we also need to consider reality. So we have to find a balance. That's why people end up requesting two, three, or four years. The complexity of the process, at a minimum … It takes a full day of work to get a treatment order.” (Psychiatrist 2)
A Game of Negotiation: Duration as the Only Lever
Participants unanimously agreed that it is nearly impossible for the person subject to the involuntary treatment order to prevail. A well-prepared defense or a counter-expertise in favor of the service user tends to influence the involuntary treatment order's conditions, like the duration, rather than the tribunal's decision itself. According to several participants, this negotiation over the conditions gives the impression that the service user's requests are being heard. “I don’t have the figures, but it's pretty rare that it's denied. Otherwise, what happens is that there's a negotiation around the duration. To go to court, the whole process, lawyers are used to it, doctors are used to it. So the process is already well established so that, once in court, it isn’t pointless.” (Criminologist 13)
Some psychiatrists said they request a longer duration because this aspect is usually negotiated in court. Generally, psychiatrists tend to propose involuntary treatment orders with a duration of one to three years. One psychiatrist described the expected annual progression as follows: “The first year, we stabilize the person. The second year, we start social reintegration, and the third year, we work on self-awareness.” Repeated involuntary treatment order renewals for the same person can also lengthen the requested duration, sometimes going up to five years. One service user recommended an annual renewal to ensure closer monitoring and to respect the individual's interests in the involuntary treatment order. “What's important is treating the client: if the judge says no, three years is too long, I’d rather have one year than none.” (Psychiatrist 12) “I wouldn’t set it that long, I’d go year by year … It will be costly, but the interests of the patient and justice should come before costs. Every year.” (Service user 2)
While families generally prefer longer involuntary treatment order durations, some are reassured by the judge-imposed limits. “I found the judge fair; he said, ‘I’m giving you two years for that medication. If you change the medication, you have to come back to court. You won’t do what you want with this young man.’ I found that great.” (Family 3)
Relational Dynamics in the Initiation of Involuntary Treatment Orders
This theme explores how the dual roles of clinicians, the framing and justifications of the procedure, and courtroom dynamics influence perceptions of fairness, support, and coercion.
Justifying the Involuntary Treatment Orders to the Service User
Psychiatrists communicated a similar rationale among themselves when justifying the involuntary treatment orders. This discourse emphasized the need to involve a neutral third party to resolve a lack of agreement with the service user and to uphold their rights. “It's a way to respect your rights. I know you feel your rights are being violated, that you don’t really want what we’re proposing, but I believe it's the best way to respect your rights while making sure I’ve done everything as a doctor to help you.” (Psychiatrist 11)
From the service user's perspective, they did not feel they received sufficient information before legal action was taken. One participant stated they were informed a few days before the process for the involuntary treatment order began, while another did not recall it being discussed with them. “They didn’t inform me about the pros and cons, he just wanted to shut me up … They didn’t say, ‘If you don’t take it, we’ll take you to court and get the right to treat you,’ they didn’t explain that part to me.” (Service user 2)
Being “Against” the Service User While Supporting Their Rights: An Irreconcilable Position
All participants discussed the importance of informing the service user of their rights and recourse, but ambiguities remained in its use and intent. Most care providers expressed discomfort with being “against” the service user, especially given the duality of their roles. For example, the psychiatrist must ensure that the service user's rights are respected while also serving as an expert for the healthcare institution. Faced with this difficulty, social workers, criminologists, and nurses often align with the institution (their employer), preferring instead to refer the service user to their lawyer or to the service user committee for questions regarding support for their rights. “If the hospital is seen as the enemy, then I’m part of it too, so it's like I have a dual role in this. The role is inherently conflicting because if I’m part of the ‘enemy,’ obviously, it's hard for the person to trust me in that.” (Social Worker 10)
Therapeutic Process or Fait Accompli: The Illusion of Choice?
As mentioned earlier, involuntary treatment order requests are very rarely rejected. This aspect either gives the impression, from the perspective of professionals, that the process is unproblematic, or, from the perspective of certain service users and families, that the outcome is predetermined. Generally, participants felt that the legal process runs smoothly most of the time, with some psychiatrists even describing it as “calm” or “reasonable.” Only a few healthcare providers raised the possibility that a court hearing could be challenging for the service user; instead, the therapeutic aspect of the process was emphasized, except when the judge did not listen to the individual. However, some participants described the process as highly anxiety-inducing for everyone involved. For some psychiatrists, the court's decorum, including the judge's neutrality, is crucial to the therapeutic value of the involuntary treatment order. It would reinforce a sense of justice and impartiality in the process.
Psychiatrists and lawyers discussed the importance of judges’ relational skills, and there was a notable variability in their approaches. Some psychiatrists stressed the importance of not focusing solely on the legal aspects of the case and ensuring that the service user was not only heard but felt heard and respected in their wishes. Yet, several nurses noted that some service users justify their decision not to attend court due to an expectation that only the psychiatrist will truly be heard. Not feeling heard in the legal process is also identified as a potential cause of trauma. “Patients have told me, on the units: ‘Anyway, there's no point in me showing up for the judge; the judge only listens to the psychiatrist.’” (Nurse 1) “A judge who is solely sensitive to legal aspects doesn’t understand that it's the person's life at stake, that it may be a turning point in their life, it's someone's voice that needs to be heard. Some judges intuitively understand and adopt this stance, but for those who don’t, it can be very difficult.” (Psychiatrist 7)
From the family's perspective, opinions were mixed. Some reported negative experiences due to the service user's lawyer appearing to support the psychiatrist's position, while others were satisfied with the respectful approach of the lawyers involved.
Barriers and Inequities in Access to Justice Surrounding Involuntary Treatment Orders
This theme explores how structural, procedural, and interpersonal factors constrain service users’ ability to exercise their rights within the involuntary treatment order process.
Biases in Favor of Healthcare Institutions
Except for service users, participants indicated that current involuntary treatment order practices are fair, well-regulated, and respectful of service user rights. “Even though it's about forcing the client to receive treatment, there's still an entire system in place that protects clients. It's not improvisation; it's a legal procedure.” (Nurse 8)
A perceived cognitive bias favoring the healthcare system and influencing some judges’ decisions was discussed by several participants. A lawyer suggested a potential cognitive bias against individuals with psychiatric diagnoses. Additionally, while some judges were identified as reluctant to issue involuntary treatment orders, others seemed to show a favorable bias toward them. A psychiatrist gave an example where a judge's personal experience made them more accepting of a stigmatized treatment: “The last time I sought electroconvulsive therapy, the judge commented: ‘You know, many of my colleagues are really resistant to this kind of treatment. Personally, I consider it an excellent treatment. From experience …’ She hinted that she knew someone who benefited from the same treatment” (Psychiatrist 1) “We have to consider the structural inequality between the patient on one side and the system on the other.” (Lawyer 4)
From the Absence to the Presence of the Service User at the Hearing
Various options for service user representation were discussed. In many cases, service users do not appear in court or arrange for legal representation. The absence of the service user in court is sometimes perceived as facilitating the issuance of an involuntary treatment order, while in other cases it complicates the process: “The judge told us, ‘One might think it could be faster and easier because the patient isn’t present, but in fact, it's the opposite. It must be more difficult and complex because the patient isn’t here, so we need more information.” (Psychiatrist 1) “Generally, when they don’t show up, it's much more favorable for us because the patient hasn’t even given an opinion; they didn’t appear before the judge, so the judge just takes what the psychiatrist says.” (Nurse 14) “Was I at my hearing? Not sure, I think I wasn’t there. The following month, I met with the review board and told them I hadn’t been to court.” (Service user 2)
When service users are present at the hearing, a lack of support was noted. The individual subject to the involuntary treatment order is typically accompanied by an orderly or a security agent, rarely someone with whom they had developed a trusting relationship. This dichotomy is also apparent in the physical organization of the courtroom, where the psychiatrist and the service user sit on opposite sides, even though the objective of mental health care is to support the individual's recovery by building a therapeutic relationship. “Someone facing an involuntary treatment order goes to court, their lawyer doesn’t explain things. They’re unprepared. (…) The judge favors, right from the start, the psychiatrist.” (Service user 3)
Several psychiatrists were mindful of the service user being well represented and aware of their rights. However, service users reported that they were not systematically aware that they were entitled to a lawyer. When service users are less aware of their rights, they are less able to exercise them. A psychiatrist shared an example where a service user's lack of awareness of their right to categorical refusal limited their ability to voice it. Providing the necessary explanations so that the service user understands their rights can be a strategy to maintain the therapeutic aspect of the procedure. Lastly, one service user recommended the systematic integration of peer support workers to assist individuals under an involuntary treatment order in navigating their treatment journey. “Every hospital should have a peer support worker or someone acting in that role to establish a connection, so that the person can understand the situation fully and make an informed decision about cooperating with the authority.” (Service user 1)
The Psychosocial Situation of the Service User: Exercising Rights as a Symptom
Mental state deterioration, financial instability, and weak social support networks can be barriers for service users to access legal resources. Due to mistrust or delusional beliefs often present in service users’ clinical profiles, defense lawyers face a complex task. According to some participants, the criteria for involuntary treatment orders are inherently related to the signs and symptoms of severe psychiatric disorders. This presents challenges to build the client-lawyer relationship, and service users’ disorganized presentation in court may inadvertently validate the psychiatric evaluation, even if the courtroom decorum can be a stressor. “We see that patients are generally so unwell that it's apparent to the judge. So there's no need to apply extra pressure. When patients testify, it's generally the most convincing part of the afternoon in helping the judge understand the need for such an order.” (Psychiatrist 11)
From the treatment team's perspective, the decision to contest an involuntary treatment order is often seen more as a symptom of the service user's condition rather than an expression of their rights and freedoms. Some lawyers and care providers expressed a certain resistance to service users’ right to appeal, viewing it as a barrier to meeting their clinical needs. When service users request a defense that challenges the treatment, call for postponement to prepare their case, or request counter-expertise, some professionals perceive these requests as counter-therapeutic. The competence of defense lawyers can even be questioned: “There are experienced lawyers who won’t ask for the impossible, won’t use misleading means to buy time and support the service user's unjustified refusal, which ultimately harms them. I think there should be training on what a psychotic patient is, what it means for someone to refuse treatment when they need it, so we don’t deal with people requesting a counter-expertise, a delay, a postponement. (…) Because of legal principles, the judge has no other choice than to allow these delays.” (Psychiatrist 4)
Available Resources: Limited Access to Lawyers and Counter-Expertise
Most service users subject to an involuntary treatment order are eligible for legal aid, while those who do not qualify must cover these expenses themselves, which can be substantial. Given the high number of involuntary treatment order requests and the limited number of defense lawyers handling them, there is an observed imbalance of resources in favor of the healthcare system. The healthcare system's resources, perceived as unlimited by many, enable thorough case preparation, extensive service user interactions, and expert testimony without financial constraints. Furthermore, legal aid fees do not cover expert witness fees, meaning counter-expertise is only available in exceptional cases, whereas the hospital lawyer's access to a psychiatric expert is ensured through the treating psychiatrist's report. “The firm covers the difference between the expert's fee and the amount granted by legal aid.” (Lawyer 1)
A perceived conflict of interest is noted by some service users and family members. Service users are often provided with a list of potential lawyers in the hospital, which results in the same defense lawyers being called upon repeatedly. When service users observe familiar interactions between the institution's lawyers and the defense lawyer, it may compromise the perceived neutrality of the judicial system: “You want a lawyer, and you get a nice list of lawyers who have worked with the hospital for 40 years. When they see each other, they leave the room to ‘have a quick chat’ in the office. You want to talk to your lawyer … the lawyer and doctor are laughing in the office together. There's no impartiality.” (Service user 2)
Delays in access to requests and information were also mentioned as obstacles. Orders are often sent to the law office with only a few days’ notice, while the hospital's legal team has typically been preparing for at least a week. Delays tied to counter-expertise are described by requesting psychiatrists as counter-therapeutic: “the slower we treat, the more harm is done.”
The healthcare team's legal support is identified by psychiatrists as a central factor facilitating the legal process. The approach taken by hospital lawyers involves pre-evaluating cases to select those that clearly meet the criteria for an involuntary treatment order, providing a preliminary legal assessment to ensure the cases are legally valid. Hospital legal services also help find court dates, support psychiatrists in their preparation with templates already established, and review their expert reports.
Discussion
This study aimed to describe the perceptions of key actors involved in involuntary treatment orders regarding their associated legal procedures. Similar to previous studies on involuntary/community treatment orders (Corring et al., 2019; de Waardt et al., 2022; Goulet et al., 2023), we found that, generally, professionals and relatives were more accepting, whereas patients were more critical. However, our study offers some insight into the legal implications of the use of involuntary treatment orders, which have been limited in previous studies.
Paradox of Clinical Roles Within the Adversarial Debate
The findings indicate that healthcare professionals’ involvement in supporting and defending service users’ rights is largely confined to a referral role. Information provided can be limited due to the healthcare team's limited understanding of involuntary treatment orders. According to the Standards of Practice for Nurses in Mental Health in Quebec (OIIQ, 2016), nurses should not only inform service users of their rights but also advocate for them. Some researchers have questioned the concept of “allyship” in mental healthcare. For professionals, it entails recognizing and leveraging their privileged position to benefit service users, an oppressed group, for equity and reduced power dynamics (Scholz et al., 2019). In a Quebec study analyzing 547 involuntary treatment order requests, only 4.4% included a testimony from an ally (Dumais Michaud, 2022). This lack of rights advocacy cannot be isolated from the clinical and legal structures that shape it. Our study underscores that providers face a role conflict in adversarial settings, where they are perceived as “opponents” to the service user, a conflict documented in studies on broader coercion (Pariseau-Legault et al., 2020). The suggestion of peer support for rights advocacy by a service user highlights this artificial divide shaped by legal needs that impacts clinical practices. Moreover, professionals involved in involuntary treatment order processes face structural tension that generates ethical conflicts when they are simultaneously responsible for delivering care and initiating or reinforcing legal procedures that restrict service users’ rights. In these cases, professionals’ obligations to institutional mandates contradict their role as advocates or allies, so this tension may limit their ability to meaningfully support service user autonomy during legal processes. In jurisdictions like the United Kingdom, the introduction of Independent Mental Health Advocates (IMHAs) offers a structural response to these challenges. IMHAs are trained advocates, independent of the treatment team, mandated to support individuals and can offer support to persons under the Mental Health Act (Mind, 2024). Considering such models may help address the structural barriers to allyship identified in this study and support a more equitable procedural environment.
Moreover, all healthcare providers in this study expressed general support for involuntary treatment orders, reinforcing the belief they are “doing the right thing,” which limits the development of a role supporting service user rights. Our findings show little ethical questioning regarding the decision to pursue an involuntary treatment order, placing beneficence at the center of the argument. Although healthcare providers are not obligated to seek an involuntary treatment order and can respect a service user's categorical refusal, the social responsibility borne particularly by psychiatrists sometimes positions the involuntary treatment order as the ultimate social safety net. This raises the question of whether individual rights take precedence over societal rights. In 2015, the Canadian Psychiatric Association declared that, “for public safety reasons, interventions that the patient may refuse or choose will be limited. The right of others to not suffer harm or be endangered may supersede the patient's right to refuse psychiatric treatment” (4). While some argue that the involuntary treatment order is a less coercive alternative to involuntary hospitalization, others suggest it represents an extension of social control by healthcare providers through de-institutionalized coercion (Velpry, 2010). Few healthcare professionals appear to consider the impact of involuntary treatment orders, systematically placing service users in a position where they feel their rights are under threat. In contrast, some family members advocate for greater coercion within involuntary treatment orders, as current legislation may not always allow sufficient intervention to change their relative's condition.
Legal Reality vs. Clinical Reality
Arguments for or against involuntary treatment orders create a dichotomy between complex health and legal situations that are challenging to reconcile. One important ethical concern is the confusion between “dangerousness” and “risk.” As discussed by Simon (2006), imminent danger is strongly ingrained in psychiatric and legal discourse, without infallible methods to predict imminence with temporal reliability. This ambiguity can disproportionately affect marginalized individuals, raising concerns about the subjectivity of psychiatric expertise and the fairness of coercive decisions grounded in risk assessments. This is exemplified by reliance on informal criteria like dangerousness, the service user's hospitalization, or the involuntary treatment order duration. While participants noted that involuntary treatment orders generally last 2–3 years, this raises questions about the objective of this timeframe. Is it “full recovery”? Is it competency restoration? Although it is legally possible to discharge a service user from an involuntary treatment order before the end of its duration, none of the study participants mentioned this option, even when service users no longer met the involuntary treatment order criteria.
Additionally, the administrative burden frequently mentioned by participants is often viewed as a protective measure against potential abuse of individuals’ rights. Yet, a mental health rights advocacy report criticized the high acceptance rate of involuntary treatment orders in Montreal courts (Québec), with less than 1% of requests being fully denied in 2018 (Action Autonomie, 2021). Our qualitative findings add context to these statistics. First, hospitals’ preliminary legal assessment in choosing cases that will likely succeed may create a high likelihood that counter-expertise would confirm the original report. Secondly, the findings should also be interpreted in light of Québec's legal framework. The legal process, typically initiated by the treating institution and involving court authorization, positions the hospital as both the petitioner and expert witness. According to a report on involuntary treatment orders, “the means at the disposal of institutions are unparalleled with those available to people attempting to defend themselves” (Action Autonomie, 2021). In a setting where inequities in access to legal resources exist, this approach may strengthen the impression among participants that judges have a favorable bias toward institutions and a negative bias toward service users.
The Involuntary Treatment Order as a Therapeutic Process in Itself?
The process of judicial proceedings for involuntary treatment orders is sometimes perceived as having therapeutic potential. Recent studies suggest that procedural justice influences perceived coercion among individuals with mental health issues (Lessard-Deschênes et al., 2024; Nakhost et al., 2018). Procedural justice theory focuses on the fairness of the decision-making process, positing that individuals who perceive that they are treated justly and respectfully are more likely to accept the outcome. The theory's principles (voice, respect, trust, and neutrality) highlight the importance of allowing individuals to voice their opinions and experience respect and dignity within a benevolent, unbiased process.
Our findings indicate that the hearing process does not always align with these principles. Many healthcare providers believe that for service users, the opportunity to be heard is as therapeutic as the proposed treatment itself. Yet, disorganized presentations in court can reinforce the medical expert's case, leading some defense lawyers to avoid having the service user testify. Lack of opportunity to voice their perspective deprives service users of potential benefits, such as viewing the process more positively or feeling valued alongside other involved parties. Even when service users testify, the lack of hearing preparation raises essential questions. Although many family members and psychiatrists report that hearings generally run smoothly and that service users are heard, Domingue et al. (2022) found that service users’ statements were rarely considered despite the opportunity to speak, giving an illusion of having a “voice”. In judge-heard cases, the current sequence prioritizes the party initiating the request. The treatment team's evidence is presented first, meaning the service user may wait up to an hour to respond after hearing testimony that portrays them as incompetent and in need of care. Dumais Michaud (2022) highlights not only inequalities in access to justice but also a “more intimate dimension in the ability to express oneself and refute the team's often closed testimony. Allowing the service user to speak first may align better with the principles of procedural justice, but would require legal reforms.
The subjective perception of the process, coupled with the imbalance in resource access, suggests that the principle of neutrality is difficult to uphold. Applying procedural justice principles could potentially support service users under involuntary treatment orders more effectively without altering their application. However, implementing these principles will be fruitless unless service users are adequately informed and empowered to believe they can influence the decision.
Limitations of the Study
This study has limitations that should be acknowledged. First, the sample size was limited due to the COVID-19 pandemic, and, although sufficient to reach thematic saturation for most groups, the inclusion of additional service users may have allowed for a broader range of perspectives. Social desirability bias may have shaped the narratives of participants. To mitigate this, service user interviews were conducted by a trained patient partner to reduce power imbalances and encourage honest disclosure. Another limitation is the absence of a variety of judicial actors, like the judges’ perspectives, which would have enriched the analysis of legal procedures. Lastly, changes in legal norms and clinical practices since data collection may influence the applicability of certain findings. Nonetheless, the consistency of themes across stakeholder groups and the triangulation of perspectives lend credibility to the study's conclusions.
Conclusions and Recommendations
This study highlights how involuntary treatment orders in Quebec operate at the intersection of clinical, legal, and experiential realities, often revealing tensions between the therapeutic intentions of healthcare providers and the procedural fairness perceived by service users. The perspectives gathered underscore the paradox of clinical roles, where providers are expected to support patients while also initiating coercive legal procedures. Furthermore, the perspective of legal actors sheds light on the confusion surrounding the legal criteria of involuntary treatment orders and the many informal knowledges derived from it.
Based on these findings, several recommendations emerge. Complex societal issues have necessitated the establishment of specialized courts, as is the case for sexual and domestic violence. Our findings suggest creating a specialized mental health tribunal in the province of Quebec that could tailor its approaches to better meet the needs of service users under involuntary treatment orders, with judges and staff specializing in law as well as the unique issues of the individuals appearing before them.
Considering the coercive nature of involuntary treatment orders, we should promote alternatives that support autonomy and self-determination. In this regard, psychiatric advance directives allow a competent individual to express future treatment preferences (Braun et al., 2023). Although Quebec's legislative context does not yet support this practice, interest is growing, as demonstrated by intersectoral reflection days on this topic. Additionally, it is desirable to draw inspiration from alternative dispute resolution methods (e.g., mediation), which focus on the needs of the parties involved.
Involuntary treatment orders exemplify the complex interplay between public safety, individual rights, and professional responsibility. Rethinking their use through the lens of procedural justice and structural reform can help restore trust and balance among all parties involved. Future research should include judicial perspectives and evaluate the impact of rights-based interventions that seek to empower service users and transform coercive practices in mental health care.
Footnotes
Ethical Approval and Informed Consent Statements
Scientific and ethical approvals were obtained from the three mental health institutes participating in the study.
Consent Statement
Written or verbal informed consent for inclusion in this research was obtained from the participants before starting interviews.
Author Contributions
M.H.G. and A.C. conceived the study. M.H.G. and C.L.D. analyzed the data. M.H.G. took the lead in writing the manuscript. All authors contributed to the interpretation of the results and provided critical feedback.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Fonds de recherche du Québec - Santé, the Canadian Institutes of Health Research, and the Fondation de l'Institut universitaire en santé mentale de Montréal.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.