
Abstract
The need to reduce restrictive practices in forensic mental health settings reflects a broader shift from traditional authoritarian and custodial approaches toward a more recovery-oriented ward environment. Safewards is an evidence-based model of care with ten interventions to reduce conflict and containment, focusing on social inclusion, communication skills, and patient support in stressful situations. This study aimed to describe the experiences of nursing staff with the implementation of Safewards in a Swedish forensic mental health clinic. Nine nurses participated in two focus group interviews. Using qualitative content analysis, three main themes were identified: Calling for leadership and resources, Striving for engagement, and Fostering awareness of nursing practice. Each main theme included two sub-themes. Participants described a general lack of leadership that left them feeling lost and uncertain during the implementation process. Descriptions related to preparation and training, hesitance to include patients in the implementation, and concerns about the fit of Safewards with existing clinical practices. Despite these challenges, the nurses were overall positive about Safewards, viewing the model as a step towards a recovery-oriented approach. The results support the implementation of Safewards Secure, a complement developed to the original Safewards model, tailored to the context of forensic mental health settings.
Introduction
In inpatient mental health settings, incidents of aggression, violence, and the use of coercive interventions, such as seclusion and restraint, often create a stressful and unsafe environment for both patients and staff (Weltens et al., 2021). For several years, there has been growing international awareness of the potential harm these practices can cause, including physical and psychological injury, trauma, and violations of human rights (Council of Europe, 2021; Funk & Bold, 2020; Herrman et al., 2022). Consequently, preventing and minimizing aggression, violence, and the use of restrictive practices through the development and evaluation of new and effective care models has become a global priority (Cratsley et al., 2021).
In forensic mental health settings, many patients’ backgrounds include severe mental illness, along with aggression, violence, or other offending behaviors, often related to the criminal activity that preceded their admission to forensic care (Tully et al., 2024). Unlike acute mental health settings, long-term forensic inpatient stays—which can span several years—often result in patients being relatively well-adjusted to the care environment and well known to staff. Consequently, more acute violent behavior that could lead to restrictive practices such as seclusion and restraint may be less common. Instead, the need to reduce aggression and restrictive practices in long-term forensic mental health settings can be seen as part of a broader shift away from traditional authoritarian and custodial approaches toward a more recovery-oriented ward environment (Maguire et al., 2018; Maguire et al., 2022).
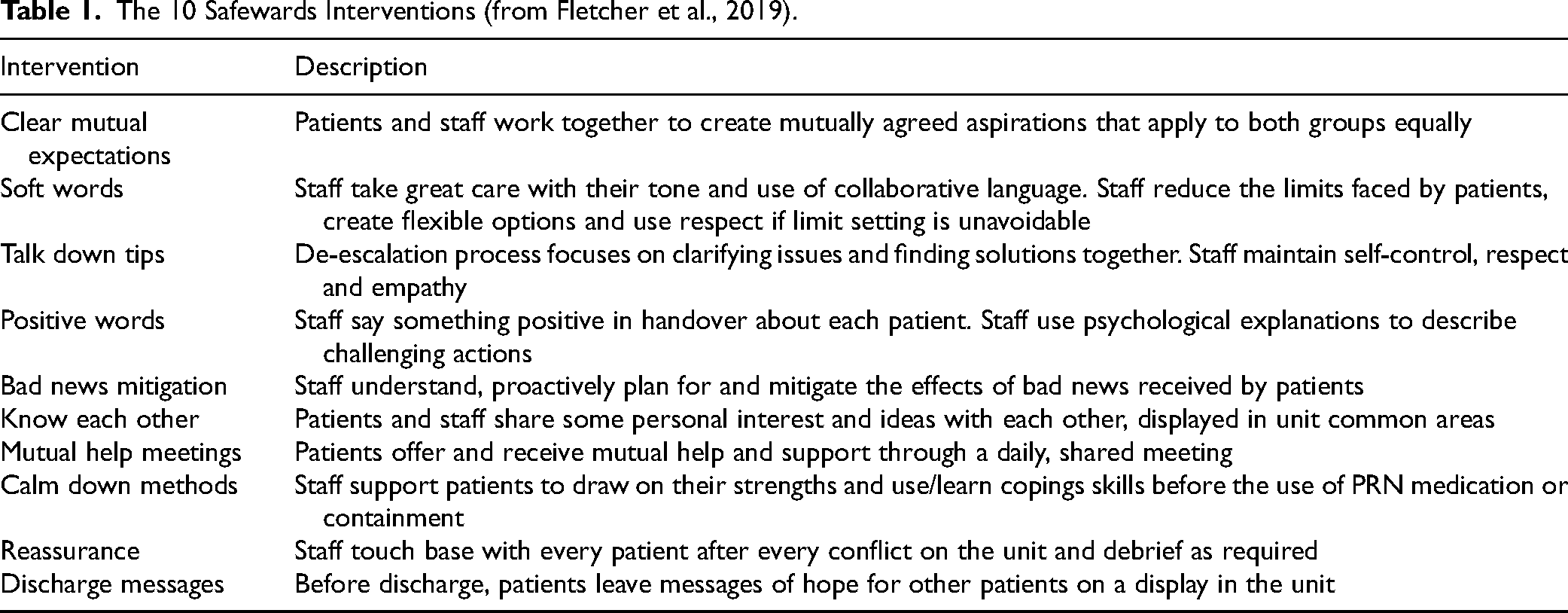
Safewards is a model of care developed in 2014, designed to reduce conflict (such as aggression directed at oneself or others, or absconding) and containment (such as seclusion, restraint, or involuntary medication). The model is based on six risk domains: staff team structure, physical environment, outside hospital, patient community, patient characteristics, and regulatory framework. Through ten interventions that emphasize fundamental relational aspects, staff work proactively to minimize risks related to these domains. The interventions involve the engagement of both staff and patients and focus on social inclusion, enhancing staff communication skills, and supporting patients in stressful situations (Bowers, 2014). Some of the interventions are more directed towards staff (e.g., Positive words, Soft words and Talk down), while others involve patients more actively, such as Know each other, Mutual help meetings, and Discharge messages. An overview of the ten interventions is presented in Table 1.
The 10 Safewards Interventions (from Fletcher et al., 2019).
Safewards was originally developed to address the reduction of conflict and containment in general acute mental health care. The model has been implemented and evaluated in various mental health settings, including wards for adults, adolescents, the elderly, patients with intellectual disabilities, and forensic care, in countries such as the United Kingdom, Australia, Poland, Germany, Denmark, Finland, Canada, and Sweden (Finch et al., 2022; Mullen et al., 2022; Pelto-Piri et al., 2024). A systematic review of Safewards’ effectiveness by Finch et al. (2022) concluded that Safewards could reduce conflict and containment in general mental health settings, but that more robust research is needed to evaluate the effectiveness in other types of settings. Similarly, Ward-Stockham et al. (2022) found in their mixed methods review that rates of conflict and containment could be reduced when Safewards was implemented, and that staff and consumers generally described positive changes in practice and ward atmosphere. Additionally, an integrative review by Mullen et al. (2022) found that while results varied across different studies, Safewards can be effective in reducing conflict and containment in both general and forensic mental health units. They also noted that successful implementation of Safewards often depended on reducing restrictive practices, maintaining high fidelity, and ensuring staff acceptability.
Several studies have explored staff experiences with implementing Safewards in clinical practice. Findings indicate that staff acceptability varies, with some showing high engagement and enthusiasm, while others view Safewards as too basic, questioning its potential effectiveness and appropriateness (Mullen et al., 2022). This variability is also evident in studies within forensic mental health settings, where some reports describe mainly positive staff attitudes (Cabral & Carthy, 2017; Maguire et al., 2018) while others reflect more mixed or negative experiences (Price et al., 2016; Whitmore, 2017). Concerns about implementing Safewards in forensic settings include challenges related to the complex dynamics of legislation, secure ward environments, extended lengths of stay, and the diverse needs of individuals with complex forensic histories (Maguire et al., 2018; Price et al., 2016; Whitmore, 2017). However, Safewards has been described as a model that could support a shift in forensic mental health nursing from traditional authoritarian approaches to practices based on recovery and person-centeredness (Maguire et al., 2018). In response to the need to adapt Safewards to forensic mental health environments, Safewards Secure was developed as a complement to the original model, addressing specific needs within forensic mental health. Developed in Australia using Delphi methodology and an international Nominal Group Technique, it involved forensic mental health and Safewards experts. In adapting Safewards, special attention was given to offending issues and behaviors as a key influence across all six risk domains (Maguire et al., 2022; Maguire et al., 2023a). However, at the time of this study, Safewards Secure appeared not well known in Swedish forensic mental health settings.
In Sweden, there are 25 forensic psychiatry clinics with a total of about 1,300 beds, with an occupancy rate that sometimes exceeds 100%. Approximately 85% of the patients are male, with a median age of 40 (Sveriges Kommuner och Regioner [Swedish Association of Local Authorities and Regions], 2023). The clinics are categorized into three security levels, ranging from level 1 (high) to level 3 (low) (Selvin, 2022). Safewards, in its original version, was first introduced in Sweden in a number of general acute mental health inpatient settings in 2017 and subsequently in forensic mental health settings. While initially, only a few forensic mental health settings implemented Safewards, there has been a growing interest in recent years. However, the implementation of Safewards in Swedish forensic mental health settings has not yet been evaluated, leaving it unclear whether nursing staff have faced similar implementation challenges as described in the literature. Given that Safewards is a complex intervention involving the simultaneous implementation of ten interventions, changes in staff behavior, local adaptations, and active patient participation, evaluations of the model in diverse cultures and contexts are essential for developing a sound evidence base. Therefore, the aim of this study was to describe the experiences of nursing staff with the implementation of Safewards in a Swedish forensic mental health clinic. Specifically, our research questions were:
How do nursing staff describe the facilitators and barriers to implementing Safewards?
How do nursing staff perceive and experience the impact of Safewards implementation?
Materials and Methods
Design
An exploratory qualitative design was used to collect data through two focus groups interviews (Krueger & Casey, 2001). In the data analysis, qualitative content analysis was used as described by (Graneheim & Lundman, 2004; Lindgren et al., 2020). The Consolidated Criteria for Reporting Qualitative Research (COREQ) was adhered to ensure transparency and comprehensiveness in the study (Tong et al., 2007).
Context
This study was conducted in 2023 at a 34-bed forensic mixed-gender mental health clinic in Sweden. The clinic consisted of four locked wards: one (Ward A, 7 beds) designated for medium security level 2, and Wards B (7 beds), C (11 beds), and D (9 beds), which operated at a low-security level 3. On Ward A, patients were assessed as being more prone to violent or absconding behavior and generally faced more restrictions, such as limited communication and restricted leaves. Wards B, C, and D were similar to general locked mental health inpatient wards in the country, where patients, for example, are allowed to use their own phones and computers and may have regularly planned leaves (Selvin, 2022). The average ward occupancy rate was about 95%. Each ward was staffed with four to five registered nurses and 15–19 nursing assistants. Affiliated to the wards were four psychiatrists, four psychologists, three social workers, and two occupational therapists. Acute coercive interventions, such as seclusion, involuntary medication, and mechanical restraint, were relatively uncommon on the wards, with a total incidence between 0.2 and <0.1 per 100 occupied bed days.
The Introduction of Safewards
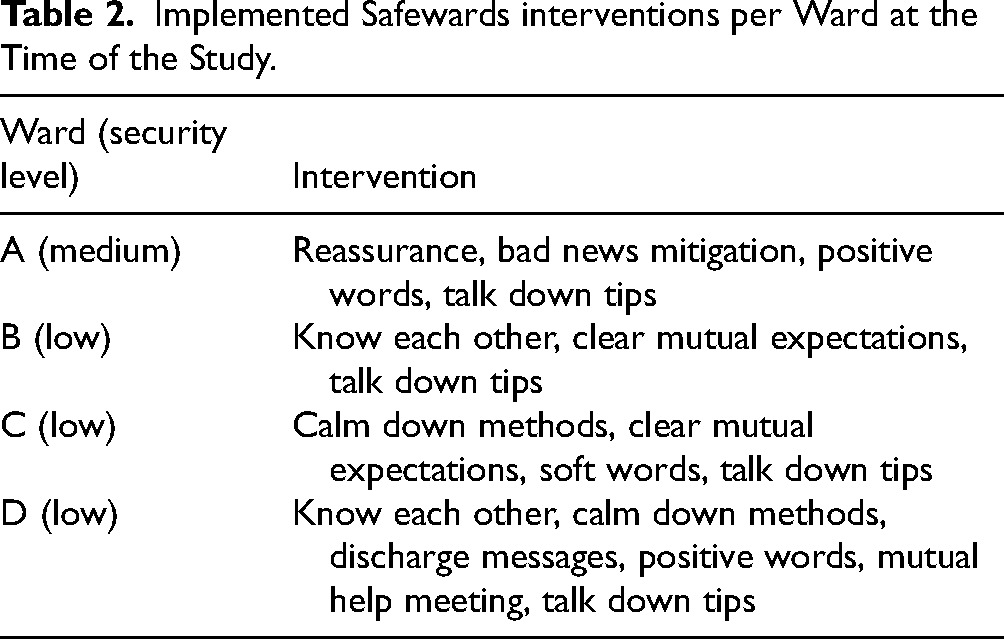
In 2020, encouraged by organizational directives, the management of the forensic mental health clinic decided to implement Safewards in all four wards. The original version of Safewards was the only one available at the time, and therefore it was the version used for the implementation. Staff training covered a one-hour theoretical introduction, and a three-hour group workshop on the ten interventions. Each ward was tasked with formulating implementation plans tailored to its specific needs and contexts. The managers of each ward assigned two to three staff members the role of Safewards champions. Staff were encouraged to participate in Safewards meetings, led by the champions, where decisions were made about the order in which to implement the interventions and where staff could volunteer to be more involved in the implementation process. After some time, a head champion was appointed part-time to support the implementation across all four wards, including facilitating recurring clinic-wide Safewards meetings. In 2023, three to six interventions were reported as implemented across the wards (Table 2).
Implemented Safewards interventions per Ward at the Time of the Study.
Participants
Purposive sampling was used for recruiting nursing staff participants with the inclusion criteria to currently be involved in the implementation of Safewards. As a first step, all champions—three per ward—were asked if they were interested in participating in the study. The clinic's head champion was not invited due to the presumed dependency relationship between the head and the regular champions. Seven of the champions expressed interest in participating. They were then asked to inquire if any other nursing staff members from their wards would like to join. Two nurses were recruited this way. Verbal and written information about the study was provided. Of the nine total participants, eight were women and one was a man. All participants were nursing assistants, with work experience ranging from 3 to 32 years (median 17 years). There were no participants from Ward A; however, three of the participating champions had recently worked at Ward A for over a year. Similarly, several of the participants had worked in more than one ward at the clinic since the introduction of Safewards.
Data Collection
Focus group one included four champions and focus group two three champions and two nursing assistants. Participants attended only one focus group in total. The focus groups, which lasted 44 and 80 min respectively, were conducted face to face at the clinic. A semi-structured interview focus group guide was used, based on the following questions: “Can you describe your experiences with the implementation of Safewards?” and “Can you describe any impact of the implementation of Safewards? In both interviews, author (JK) led the interviews and author (VP) had an observer role and provided follow-up questions. Participants were encouraged to interact with each other, i.e., asking each other questions, agreeing or disagreeing, commenting, and reflecting on what was being said in the group (Krueger & Casey, 2001). The interviews were audio recorded and transcribed verbatim, securely stored on a protected digital platform.
Analysis
Transcribed focus groups were analyzed using inductive qualitative content analysis (Graneheim & Lundman, 2004; Lindgren et al., 2020). Authors JK, SA, and LK separately read the focus group transcriptions several times to gain an overview and identified meaning units relevant to the aim. The authors then condensed their identified meaning units and grouped them into codes based on recurring patterns. Special attention was given to identifying relevant discussions and comments between participants that could further enhance understanding of the data. The codes were grouped based on similarities, after which authors JK, SA, LK, and VP interpreted and abstracted these codes into subthemes. Subthemes that resemble each other are grouped, and these groups are further abstracted and interpreted into main themes, which were discussed and reflected upon by all authors until consensus was reached.
Throughout the analysis, the authors engaged in reflexive practice, such as collaborative cross-checking, and critically considered their positionality. They regularly examined their own biases and perspectives to minimize influence on data interpretation (Berger, 2015). This was particularly important because VP was employed at the research and development department of the larger organization, which included the forensic mental health clinic, and was involved in the implementation of Safewards across the organization.
Ethical Considerations
Ethical approval was granted by the Swedish Ethical Review Board (Dnr 2020-03881). The participants were informed about the study and their right to withdraw at any time. Signed informed consent was obtained and documented from all participants. Participant integrity was protected by safeguarding all audio and text files.
Results
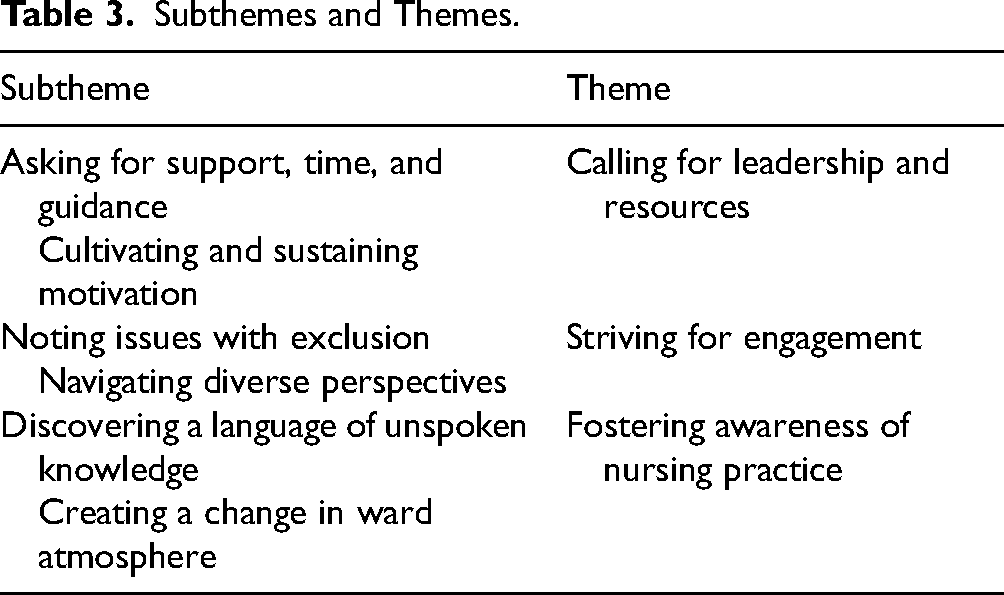
The analysis identified three main themes: Calling for Leadership and Resources, Striving for Engagement, and Fostering Awareness of Nursing Practice. Each theme included two subthemes and was linked to key aspects of both the organization, motivation for change, and nursing practice (Table 3). Quotes include both individual and interactive group discussion quotes, cited as F1 or F2 to indicate the corresponding focus group. Interactive quotes are marked with “R” for any of the respondents. Ellipses (‘…’) are used in quotes where content has been omitted for reasons of confidentiality, irrelevance, or repetition. Non-verbal sounds, such as hums of agreement, are indicated in brackets […] in the quotes.
Subthemes and Themes.
Calling for Leadership and Resources
Throughout the interviews in both focus groups, leadership, and the availability of various resources to support the implementation of Safewards emerged as recurring topics. Two subthemes were identified: Asking for Support, Time, and Guidance, which reflects uncertainty about the implementation strategy, and Cultivating and Sustaining Motivation, capturing the challenges of keeping staff inspired.
Asking for Support, Time, and Guidance
Participants emphasized the critical role Safewards champions played in advancing the implementation process. Champions assumed responsibility by providing information, conducting training sessions, facilitating joint reflections, and offering guidance throughout. Without their leadership and support, the implementation became more challenging. Participants also noted that if champions left their positions, or their roles on the ward changed, this had a negative impact, leading to a sense of insufficient guidance. Identifying a suitable replacement for the champion role could be difficult. I'm passionate about my job, and it was just obvious that we should work on this. We had a registered nurse, and a nursing assistant who became Safewards champions, and they went all in, and this joy of starting Safewards really spread to all of us. Then both left and they had been holding onto this and getting the ship ready to sail, and then it became like, we got lost at sea, who is navigating this ship? (F2) R – There are too few discussions about Safewards. What we see is this Safewards group running off to meetings /…/ and then they come back with a bunch of stuff /…/ they could sit down and explain it to us instead of throwing us in front of a computer and letting us read through everything. There should be more discussion so that we get more involved /…/ [hums of agreement from several in the group] R – No, there hasn’t been much of that there either. R – I completely agree with you, it's been pretty much nothing, I can say. (F2)
Cultivating and Sustaining Motivation
Participants generally described motivation levels as varied; some nursing staff were excited at the beginning but lost interest over time, some found motivation as the implementation progressed, while some remained uninterested throughout the whole process. The role of champions and actively engaged nursing staff in fostering and sustaining team motivation was described as crucial, however, there was a concern about whether they would be able to maintain their enthusiasm over time. If there are some who are driven and constantly have this mindset, then I think it will be contagious, but they also need to have the energy. And you can’t constantly…go around reminding people about…things. So I hope, but that's what it takes, so you hope that those who are passionate about it have the energy to keep going so it rubs of on new staff (F1). The Safewards seminars we have digitally with the entire country - they provide a lot; you feel a bit extra motivated after them (F1)
Striving for Engagement
The importance of engagement from all, rather than just some, individuals involved in the implementation of Safewards was repeatedly emphasized by many participants in both groups. Engagement was described as including both interest and enthusiasm for Safewards, as well as recognizing its relevance to the ward community. Two subthemes emerged under this theme: Noting issues with exclusion and Navigating Diverse Perspectives.
Noting Issues With Exclusion
Several participants in both groups felt excluded at times during the implementation process, particularly when it seemed orchestrated by a small group of staff members. This led to feelings of being left out, unprepared, and confused when later involved in Safewards interventions, impacting their engagement levels. Participants emphasized the need to include all professions and students in the implementation process. They observed that a lack of interdisciplinary collaboration negatively affected the process and called for greater involvement of everyone. Registered nurses were not as involved as nursing assistants because they were often working across several units, which limited their time and training in Safewards. Additionally, participants felt that doctors’ lack of awareness and involvement in Safewards was problematic given their impact on patient care.
R - And there we are facing an uphill battle with the doctors. Unfortunately. …
R - That's difficult.
R - It's not easy.
R - Still, still, I think the doctors should get information about Safewards as well. Maybe they have?
/…/
R - There, you mustn’t come and interfere, so they have their opinions and that's that! … And yet we are the ones who see the patients all the time. It's actually us who work with them, who are closest to them. We are the ones who take the hit. If something goes wrong. (F2). What we did instead was to remake the rules that already existed and wrote them in a better way and more clearly – and the patients were not involved in the intervention as they should have been. We were not loyal to the method, that I can say, but we remade the rules so that instead of writing ´You areńt allowed tó we changed it to ´You are allowed tó and we made it so that the expectations applied to both the staff and the patients and not only the patients. (F2) We've dared to try a bit more. For example, relaxing the coffee break times—a small detail, but at first, people were saying it would be a disaster. Someone even said, ‘They won't do anything but drink coffee.’ But it hasn't been a problem at all. (F1)
Navigating Diverse Perspectives
Participants noted that introducing Safewards revealed divergent views among the staff, leading to a division into two distinct groups: pro-Safewards and anti-Safewards. The pro-Safewards staff adopted a more flexible and caring approach, while the anti-Safewards group maintained an authoritarian stance, expecting patients to adhere to rules without question. The environment on some wards was described as stricter than on others, with most staff assuming authoritative roles. There are those who believe that we need coercive measures, you know. This Safewards thing will never work; you have to be tough and firm, like, right from the start. It's a bit peculiar with those who have been working in psychiatry for, let's say, 30 years; they don't like Safewards. Personally, I think that maybe it doesn't always work, but you have to try. (F2) Many believed that Safewards meant simply saying yes to everything - that it was just “yes” all the time and not setting any limits … It was lack of knowledge, they didn't know what it was about, but even today I can still experience that there is a bit of resistance from some. (F1)
Fostering Awareness of Nursing Practice
The impact of Safewards on nursing practice in the wards was a common topic in both group interviews. Two subthemes were identified: Discovering a language for unspoken knowledge, which highlights the connection between Safewards-based communication and nursing care, and Creating change in ward atmosphere, which reflects how new practices in nursing care influenced the overall environment on the wards.
Discovering a Language for Unspoken Knowledge
Participants described that even though many of them could recognize much of Safewards, it was meaningful to receive a new language and structure that could be used to communicate nursing practice. I believe it becomes easier and more accepted when a name is introduced, like Safewards, and you realize you’ve been working based on it without knowing it was Safewards. (F2) [At handover]… when it comes to this person [a patient with often challenging behavior], you know exactly what you're about to hear. But since we started using Positive Words, you immediately hit the brakes when you come to that person and start talking in a different way. It's changed how you speak about that person. (F2)
Creating a Change in Ward Atmosphere
Many participants felt that Safewards influenced nursing care in a way that improved the overall ward environment. Some noted that Positive Words transformed handover practices, shifting the focus from negative aspects of patients’ behaviors to more positive narratives and a better understanding of factors influencing those behaviors. I think that when it comes to interacting with patients, it's become more open in some way, and you really listen to the patient. And that's something where there's been some resistance, but we keep pushing for it, because I think it's important to keep the patient in focus. (F1) We were told that it was even risky to participate because it posed a threat to security. However, after some motivation and persuasion, everyone agreed to it, but it took some time. We also explained that there was no need to provide personal details like addresses or children's names, but rather share interests such as favorite foods and hobbies, so they could get an idea of what kind of person you are. (F1) That it's no longer about this power dynamic among us who work, but it has evolved into a different kind of relationship. (F2)
Discussion
This study aimed to describe nursing staff´s experiences with implementing Safewards in four wards of a Swedish forensic mental health clinic. Participants emphasized the critical roles of leadership, resources, engagement, and awareness of different approaches to forensic mental health nursing, findings that align with and reinforce previous research on Safewards implementation in forensic settings. Although the participants generally felt that Safewards was suitable for implementation in forensic mental health settings, they identified aspects of the model that would benefit from adaptation. None of the participants specifically mentioned Safewards Secure, suggesting a lack of awareness of the adapted model.
In a qualitative systematic review (Björkdahl et al., 2024) using the i-PARIHS implementation framework (Harvey & Kitson, 2015) to identify barriers and enablers for implementing Safewards in mental health inpatient settings, three key determinants emerged: i) leadership support, ii) the perceived alignment, or “degree of fit,” of Safewards with existing practices and values, and iii) nurses’ personal values and beliefs. The review included ten articles, three of which focused on forensic mental health services. In our study, we found all three of these determinants reflected in the thematic findings. One of them was the insufficient leadership support perceived by the participants. They specifically described managers’ limited understanding of the model, lack of involvement, inadequate training, and follow-up resources. These challenges often left staff feeling lost and on their own in their struggle to advance the implementation process and became especially clear in those cases where managers had expressed opposition against Safewards. Ward managers in forensic mental health play a crucial role in shaping the ward's atmosphere and implementing new mental health reform guidelines, which sometimes necessitate cultural change (Maguire et al., 2023b). However, the role has also been described as one of the most overburdened in healthcare (Baker et al., 2012) often lacking role clarity and involving multitasking responsibilities (Maguire et al., 2023b).
“Power and authority” is a key implementation determinant (Harvey & Kitson, 2015) that refers to the ability to influence or control decision-making processes. It involves the trust and confidence management places in champions and nursing staff to make on-the-spot decisions, drive improvements, and introduce new approaches during implementation. In our study, participants’ calls for stronger leadership may reflect uncertainty about their own power and authority in the implementation process, increasing the risk of passivity. For leaders, clarifying this aspect to boost staff confidence could enhance engagement and intervention sustainability. At the same time, participants in both groups described insufficient Safewards training opportunities, knowledge, and skills, aspects that have been highlighted as a barrier to implementation in several Safewards studies in forensic mental health settings (Cabral & Carthy, 2017; Price et al., 2016; Whitmore, 2017) and which could be related to hesitance to assume power and authority in the implementation process.
“Opinion leaders,” another implementation determinant of the i-PARIHS refers to key players in the implementation process, with a supportive or obstructive influence depending on their attitudes and behaviors towards change (Harvey & Kitson, 2015). Although the term may include formal leadership, it mainly refers to peer-based influence among staff members and groups. The importance of assigning champion roles to senior staff members who have been recognized as supportive opinion leaders with expertise and credibility among peers, have been highlighted in previous Safewards studies (Fletcher et al., 2021; Higgins et al., 2018). In our study, the importance of champions was highly recognized, and it is therefore not surprising that participants described feeling lost when influential champions left their jobs and replacements were difficult to find. It also remains unclear whether having registered nurses in the role of champions would have resulted in greater buy-in from some staff.
Additionally, participants described challenges with resisting staff, including some managers. According to Rogers (2003), among these resistant individuals may be opinion leaders who question the relevance of change and argue that there are valid reasons to maintain the status quo. They are often seen as problematic and are avoided during change initiatives. However, both perspectives are valuable to an organization. Resistant staff challenge leaders to convincingly and thoughtfully articulate the need for change. Those resisting may raise important concerns, such as negative experiences from past change efforts, doubts about the innovation's compatibility with current practices, or inadequate resources, and rightly identifying situations where the chances of success are low (Khaw et al., 2023).
In our study, the implementation of Safewards exposed a divide among pro- and anti-Safewards staff, with the resistance from the opposing group appearing rooted in a traditional, authoritarian, and risk-focused approach. We believe that the coexistence of traditional and recovery-oriented cultures could have further contributed to the uncertainty described by staff regarding the foundational bearings of the clinic. More specifically, Safewards related “splits in the team” in forensic settings has been described by for example Price et al. (2016) and Cabral & Carthy (2017). At the same time, risk and security are defining, undeniable, and critical parts of forensic mental health care, and the pro- and anti-Safewards groups may reflect differing values and beliefs about what ensures security in these settings (Marshall et al., 2019). Our study found that the traditional methods of ensuring security seemed challenged by Safewards’ emphasis on safety through positive relationships and caring communication.
It has been suggested that the closer the degree of fit of a new innovation to previous ways of working, the easier the uptake by staff into practice. When perceived as inadequate by staff, the innovation is simply not adopted, or efforts to adapt it to the local context through practice-based knowledge may be initiated (Harvey & Kitson, 2015) In our study, nursing staff adjusted or did not implement some interventions they perceived as unsuitable for forensic mental health care, such as Discharge Messages, due to long periods of stay, and Know Each Other, related to safety issues. In Safewards Secure (Maguire et al., 2022; Maguire et al., 2023a), forensic mental health-related adaptations or recommendations have been made for all the original Safewards interventions, based on recovery-oriented principles as well as security concerns. Safewards Secure, therefore, appears to represent a function with the potential to increase the degree of fit of Safewards in forensic mental health, thereby enhancing recipient acceptability and adoption willingness among a wider group of staff. In addition, we believe that the name “Safewards Secure” is well thought out, signaling to those otherwise hesitant that the adaptation has considered specific security aspects of forensic mental health care.
Notably, the inclusion of patients in the implementation process was described as low, reflecting the influence of traditional restrictive risk-focused cultures that view patients as passive recipients of care, unsuitable for or incapable of actively participating in improvement efforts on the ward (Tomlin et al., 2018). A study by Selvin et al. (2016) found that patients in forensic mental health care valued participation through influence, good communication, confidence, trust, initiative, and engagement in activities. This aligns with the principles of Safewards and supports patient inclusion in forensic mental health. In fact, Pelto-Piri et al. (2024) argued that patient inclusion is crucial to Safewards’ effectiveness, highlighting that the most of the ten interventions rely on patient participation to adhere to the model.
Patient inclusion requires mutual engagement from both patients and staff and needs to be facilitated by staff through invitation, encouragement, and support (Sahlsten et al., 2008). At the same time, patient participation can be complex. For example, patients in forensic mental health care settings have described participating in activities primarily to strategically present themselves as healthy to staff, thereby increasing their chances for discharge (Selvin 2022). In our study, many challenges described by participants seemed to stem from a general sense of uncertainty. This was linked to the coexistence of a stricter traditional culture with the more recovery-oriented Safewards model, organizational resistance from some managers despite its implementation, staff reliance on champions who were often absent, and the lack of patient inclusion in a model where this was fundamental. Interestingly, in a literature review of interventions in forensic mental health, Barnao and Ward (2015) observed a practice of blending divergent therapeutic and correctional models to address patients’ complex needs. They argued that this mixture of paradigms could potentially create more issues than it resolves, leading to confusion—particularly in the staff-patient relationship—which would hinder practitioners in navigating their way forward.
According to Tully et al. (2024), forensic mental health services are important components of mental health systems but suffer from an insufficient evidence base for common practices, including restrictive measures and the inclusion of patient perspectives. For Safewards and Safewards Secure to truly support a shift toward a more recovery-oriented nursing approach in forensic mental health, efforts must be made to openly address both the challenges and benefits of their implementation.
Relevance for Clinical Practice
In line with previous research on the implementation of Safewards in forensic mental health settings, the results of our study further emphasize the importance of establishing leadership support at both the ward management and champion levels. This includes clearly defining “who is navigating the ship,” providing relevant training and support, and ensuring staff are confident in the extent of their authority to make implementation decisions. We also suggest that when preparing for the start of implementation, discussing with all staff the characteristics of the ward's current clinical practice—whether it is traditionally focused on risk, safety, and control or more recovery-oriented. This includes identifying subgroups within the staff and openly weighing the advantages and challenges of different approaches. Finally, we believe it is important to discuss with staff the alignment of Safewards with existing nursing practices, carefully considering any important concerns raised by resistant staff, and select the adapted and context-sensitive Safewards Secure.
Strengths and Limitations
A strength of the study is that several aspects of trustworthiness were addressed (Ahmed, 2024), including the acknowledgment of the researchers’ personal biases and preconceptions (credibility), the provision of detailed contextual information and sampling strategies (transferability), and the involvement of different members of the research group at various stages of data analysis (confirmability). Additional components of trustworthiness could have been incorporated, such as maintaining a detailed record of all decisions made throughout the study to enhance transparency and traceability.
The use of focus groups generated data through participants’ sharing and discussions of their implementation experiences, which likely contributed to data richness (Krueger & Casey, 2001). The two focus groups included four and five participants, respectively, and it is possible that slightly larger groups of about 5–8 participants per group could have provided more data. However, larger groups may also increase the risk of some participants not feeling confident enough to actively contribute.
The focus groups included seven nursing assistants who also served as champions during the implementation, which is a strength. However, the limited representation—only two additional nursing assistants, no registered nurses, and no participants from medium secure ward A—is a limitation that likely affected data diversity. The reason for the absence of participants from ward A is unknown, though the recent work experience from ward A of three participants may have compensated this limitation to some extent.
The participants generally had a positive attitude towards Safewards, which may have skewed our findings. It is a well-known challenge to recruit less positive staff members for qualitative research evaluations, which can result in findings that are less representative of the clinical “real life” and, consequently, less useful for understanding complex implementation components.
Conclusion
This study describes the experiences of nursing staff with the implementation of Safewards in a Swedish forensic mental health clinic. The results highlight three critical areas influencing the implementation: leadership and resources, engagement, and alignment with nursing practice. The study underscores the importance of structured planning before and during the implementation process, along with continuous follow-up to avoid fragmentation and feelings of being lost. The results support Safewards as a useful model to structure and clarify nursing practice in forensic mental health.
Footnotes
Acknowledgments
We would like to thank the participants who generously took their time and shared their experiences. OpenAI's ChatGPT was used to provide language and grammar suggestions. All final edits and decisions were made by the authors.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the AFA Försäkring.
Conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The data that support the findings of this study are available from the corresponding author (JK) upon reasonable request.