
Abstract
In New Zealand, service users who are Māori (Indigenous people of New Zealand) comprise roughly half of the population in forensic mental health services (FMHS). An actuarial risk assessment instrument, the Dynamic Appraisal of Situational Aggression (DASA) has been introduced to reduce the risk of imminent inpatient aggression, which is prevalent in such services. The current study is a qualitative descriptive design, enhanced by aspects of participatory action research, to evaluate the suitability of the DASA for Māori from a Māori perspective. Two hui (a Māori gathering) were held with seven Māori nurses and a Māori cultural advisor from a FMHS. The first hui (n = 7) explored Māori perspectives on the strengths, limitations and suitability of the DASA for Māori, and the second hui (n = 6) reflected on appropriate adaptations to the measure. The findings of this study confirmed support for using the DASA with Māori. However, five recommendations were made for adaptations for cultural enhancement. Such cultural enhancement would require further refining with Māori cultural advisors and psychometric testing to ensure the validity and reliability of the DASA for Māori.
Keywords
Introduction
Forensic mental health services (FMHS) are entrusted with assessing and treating individuals whose mental health needs intersect with criminal offending (Maguire et al., 2019). In these settings, inpatient aggression is prevalent and recognised as a serious health and safety issue (Verstegen et al., 2024). International research highlights high rates of inpatient aggression in FMHS and indicates the consequential negative impacts that can arise (Ireland et al., 2021; Ogonah et al., 2023). Such negative impacts include physical, psychological and emotional harm that can threaten the safety of staff, the therapeutic milieu and the quality of care received by service users (Verstegen et al., 2024).
In New Zealand, the frequency and prevalence of aggression tend to be higher in FMHS than in non-FMHS (McKenna, 2020; Te Pou o te Whakaaro Nui, 2015). As a result, there is increased pressure and demand for FMHS to support the needs of service users, who are at risk of engaging in aggression (McKenna & Sweetman, 2021; Wratten-Stone, 2016). The service users who are Māori (Indigenous people of New Zealand) are considerably over-represented in FMHS, accounting for approximately half of the population (McKenna, 2020). Consequently, Māori constitute a priority population within FMHS for support and treatment (Te Pou o te Whakaaro Nui, 2015; Wratten-Stone, 2016).
In forensic mental health settings, perceived safety is a key pillar of individuals’ successful recovery and serves as the foundation for all therapeutic interactions (Senneseth et al., 2021; Shepherd et al., 2016). Amidst the prevalence of inpatient aggression in these settings, literature on forensic recovery highlights the need for strategies to enhance service users’ sense of safety (Shepherd et al., 2016). In this instance, risk assessment plays a crucial role in ensuring individuals’ safety, health and well-being (Dickens et al., 2019). Risk assessment is a proactive procedure that involves a comprehensive determination of a person's degree of risk to others and the implementation of potential actions thoughtfully aimed at preventing or mitigating the risk of violence or aggression (Bratina, 2022). The existing literature recommends a number of risk assessment instruments, which FMHS can implement to gain a better understanding of aggression and work towards reducing it (Dickens et al., 2019; Ogonah et al., 2023). One such instrument that has been subject to considerable empirical investigation is the Dynamic Appraisal of Situational Aggression (DASA; Daffern & Ogloff, 2020).
The DASA is an actuarial risk assessment instrument developed to assist in assessing a service user's risk state for the next 24 h (Ogloff & Daffern, 2006). The DASA comprises seven items: irritability, impulsivity, unwillingness to follow instructions, sensitivity to a perceived provocation, easily angered when requests are denied, negative attitudes and verbal threats (Ogloff & Daffern, 2006). Each item is subsequently scored for its absence (0) or presence (1) in the previous 24 h (Daffern & Ogloff, 2020). The estimations are combined to give a total score from 0–7, indicating an individual's risk for aggression (Ogloff & Daffern, 2006). The total scores are divided into three classifications: 0, 1–3 and 4–7, indicating low risk, moderate risk and high or imminent risk, respectively (Daffern & Ogloff, 2020). Research has demonstrated that the DASA has been used by nurses internationally and found to be a valid and useful instrument in assessing an individual's likelihood of imminent aggression (Maguire et al., 2022).
The DASA has been introduced to FMHS in New Zealand to assist staff in appraising the risk of imminent aggression. However, the cross-cultural applicability of the instrument has not been considered with Māori, the Indigenous peoples of New Zealand (Coulter et al., 2023; Shepherd & Lewis-Fernandez, 2016). Before introducing any risk assessment instrument, there should be validation of the instruments’ psychometric properties to the unique social context of the environment in which it is being introduced, including its use with Indigenous peoples (Coulter et al., 2023). Without such validation, the assessment may result in skewed risk assessment (Shepherd & Spivak, 2021). While substantial psychometric testing of the DASA has occurred with non-Indigenous populations, no validation has occurred to date with Māori. This study aimed to undertake the initial steps toward such validation by determining the suitability of the DASA for Māori in FMHS in New Zealand.
Methods
Consultation with Māori
Cultural consultation was undertaken with Māori cultural advisors at the service prior to a study proposal being devised. Author A.K. met with Māori cultural advisors on two occasions to discuss and establish the aim and methodology of the study. This consultation was undertaken to fulfil the Health Research Council of New Zealand's mandatory requirement to ensure that the scope of study involving Māori resonates with Māori interests and aspirations (HRC, 2010).
Research design
The current study is a qualitative descriptive study. The qualitative descriptive design is a methodological approach that seeks to describe and understand a phenomenon through an in-depth exploration of participants’ perspectives (Doyle et al., 2019). Using this approach, the role of the researcher is to remain close to the data and to the surface of the participant's words during data analysis (Sandelowski 2000). Doyle et al. (2019) suggest that the qualitative descriptive design is particularly useful in gaining foundational insights into a poorly understood phenomenon. Given the paucity of prior research on the current study topic, a qualitative descriptive design was employed to attain an in-depth understanding of DASA's suitability for Māori by exploring the meanings as described by participants who were Māori. Doyle et al. (2019)'s outline of qualitative descriptive design guided the selection of sampling, data collection and analysis methods. A detailed account of these methods will be presented in the sections that follow.
The nature of this study was also action-oriented, with a focus on involving participants in identifying issues and generating practical solutions. As such, the current qualitative descriptive study adopted aspects of participatory action research (PAR). PAR is a qualitative research approach that emphasises the active participation of people affected by the issue being studied, who generate practical actions to address issues that concern them (De Oliveira, 2023). PAR involves participants collaborating with the researcher to identify and clarify an issue, constructing a plan of action to effect change, reflecting on the results, and adjusting the plan as necessary (De Chesnay, 2015). In this study, the use of PAR was evident through two key processes. The focus of the study centred on identifying and addressing an issue that concerned the participants. Furthermore, collaborative recommendations were developed with participants to enhance the use of the DASA with Māori. This PAR-oriented approach resonates with the Māori notions of kotahitanga (unity), whereby action plans are established through participants’ collective efforts (Kiro, 2000).
Setting
The study was conducted in the Auckland Regional Forensic Psychiatry Services (ARFPS), also known as the Mason Clinic. The ARFPS is a secure 126-bed inpatient forensic mental health hospital in New Zealand. The hospital has eight forensic mental health inpatient units, from acute care to a low-secure hostel. In ARFPS, approximately half of the service users are Māori (Mason Clinic, 2011). The workforce in ARFPS comprises multidisciplinary staff, including forensic mental health nurses (McKenna, 2020). This workforce also includes taurawhiri (Māori cultural advisors), who offer cultural advisory and support services to all service users who are Māori within the ARFPS (Mason Clinic, 2018).
Procedure
This study was generated in response to the service-wide introduction of the DASA for use with all service users in 2023. The study was led by author A.K., who also facilitated the data collection and analysis processes. Consultation with a Māori cultural advisor informed the decision to use hui (a Māori gathering) as a data collection method. A hui equates to the use of focus groups. The consultation also led to the decision for a Māori cultural advisor to attend the hui to offer cultural supervision and lead Māori customary practices, such as karakia (prayer). These decisions were to ensure the cultural safety of participants who were Māori.
Two hui were held in 2023. Both hui were facilitated by author A.K., along with cultural support from the Māori cultural advisor. The purpose of the first hui was to gain Māori perspectives on the value of the DASA instrument, to consider its strengths, limitations and suitability for Māori. The purpose of the second hui was two-fold. Firstly, to reflect on the outcome of the first hui discussion and secondly, to make consensus recommendations for action. The recommended adaptations to the DASA were specific to service users who were Māori.
Recruitment and participants
Participants were recruited using a purposive sampling method in selecting participants with specific knowledge related to the phenomenon of interest (Doyle et al., 2019). In this study, Māori nurses were considered the most appropriate participants to navigate both the cultural and clinical aspects of the DASA. The criteria for inclusion were Māori nurses who self-identified as Māori and were currently working as registered nurses in ARFPS. A poster advertising the study was emailed to all Māori nurses in ARFPS by the service administrator, who had no personal contact with potential participants.
Seven people responded to the invitation and attended the first hui after signing the informed consent. All participants in the first hui (n = 7) were Māori and employed by the ARFPS; all from different departments within the ARFPS. Three participants were from the Kaupapa Māori (Māori-orientated) rehabilitation unit (one male and two females), two were from the male-only subacute unit (one male and one female), one was from the male and female mixed acute and rehabilitation unit (female), and one was the Māori cultural advisor from the service (male). While the cultural advisor initially attended the hui in a supervisory capacity, the cultural advisor wished to fully participate in the hui with other participants. As such, the cultural advisor undertook the role of cultural supervision and concurrently became a participant. This was considered appropriate by all other participants. All participants except the Māori cultural advisor were registered nurses. All participants except one had no prior experience using the DASA in their clinical practice.
A total of six people from the first hui attended the second hui. The participants in the second hui (n = 6) included five Māori registered nurses (two males and three females) and the Māori cultural advisor from the service (male).
Ethical considerations
The Auckland Health Research Ethics Committee granted ethical approval, and locality authorisation was obtained from the service concerned. On the day of first hui, informed consent was obtained from each participant. All participants were informed that participation was voluntary, and they had the right to withdraw at any time. Participants were assured that all information shared in the hui was confidential, and anonymity would be preserved by removing any individuals’ identifying information.
Data collection
Data were collected during the hui. A semi-structured interview guide was used to guide participants’ discussion and included open-ended questions, such as “What is your perspective on the strength, limitation, and suitability of the DASA for Māori?” and “What aspects of the DASA, if any, do you consider that should be refined to be suitable for future use with Māori?” (Doyle et al., 2019). The discussions from the two hui were digitally recorded using two audio recorders, and field notes were taken.
Data analysis
The data was analysed using inductive thematic analysis in alignment with recommendations for qualitative descriptive research (Doyle et al., 2019). This method ensures that the emerging key findings are grounded in the participants’ words. The inductive thematic analysis followed the six-step framework proposed by Braun and Clarke (2021). The process of transcribing the data began with author A.K. listening to the audio recordings to become familiarised with the data. Sections of the transcript relevant and meaningful to the study were identified, colour-coded and compiled to create initial codes. These initial codes were then categorised to develop logical themes in a process that involved repeatedly returning to the raw data. Author A.K. discussed the potential themes with other authors through an iterative process, ensuring the participants’ words were identified as theme names. The process yielded the formation of the logical themes and subthemes. In keeping with the use of aspects of PAR, the summary of findings was presented to participants at the second hui to collaboratively reflect on the key findings and make consensus recommendations for action.
Trustworthiness
This study used criteria provided by Lincoln and Guba (1985) to ensure the study's trustworthiness. Member-checking was built into the study design and data collection process, whereby the preliminary findings from the first hui were presented to participants, and feedback was collected. This process sought to increase the credibility and authenticity of the findings, ensuring that they remained grounded in the participants’ words. The transferability of findings was assured by a detailed description of the participant demographics, recruitment process, and study setting. Coding and themes were established with other authors in a shared collaborative manner, ensuring the dependability of study findings. The confirmability and authenticity of the study findings were assured by the use of verbatim transcripts and the inclusion of quotes to support the study findings.
Results
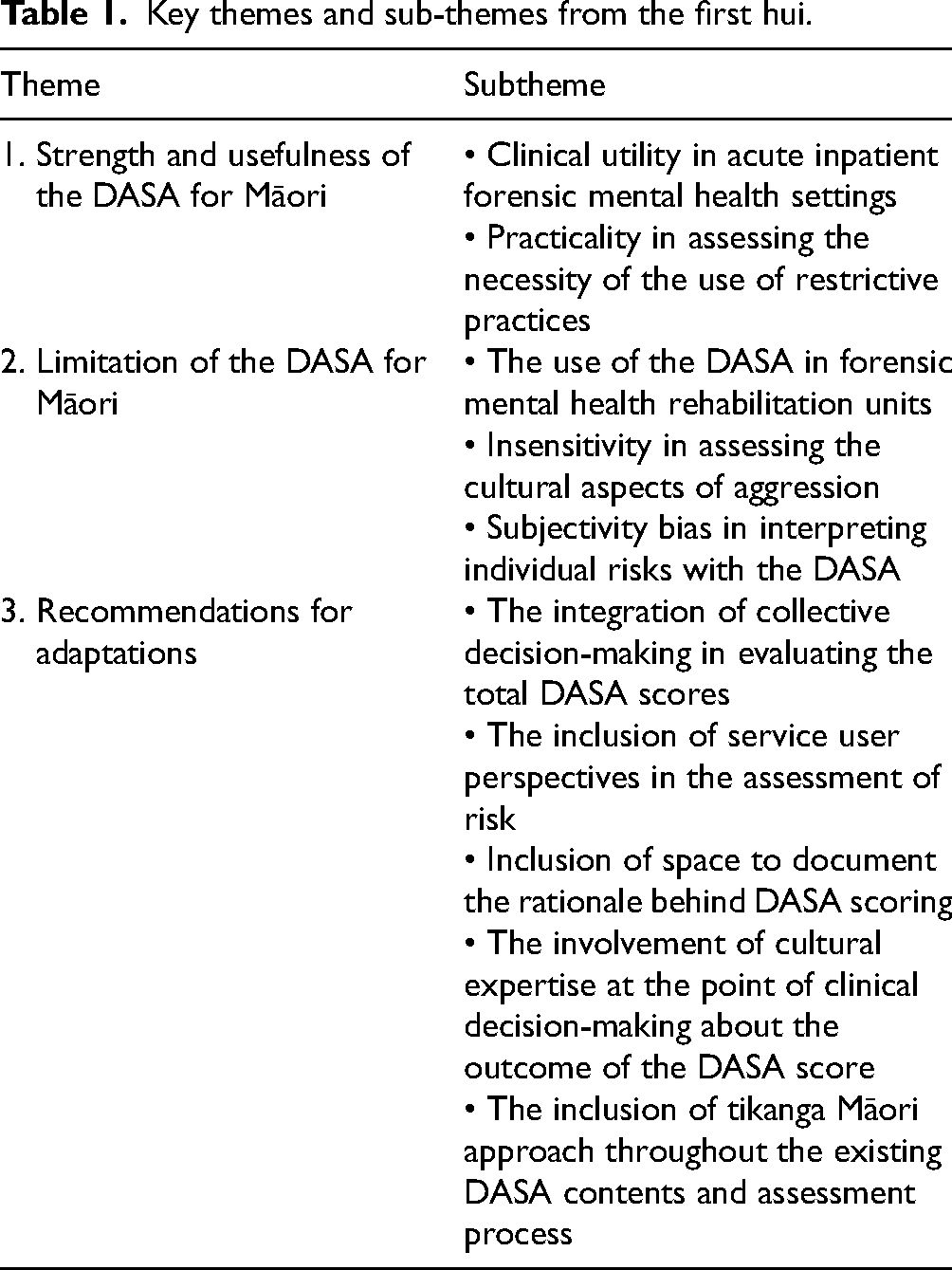
Three key themes emerged from analyses of the first hui transcripts. These themes were: (1) the strength and usefulness of the DASA for Māori, (2) the limitations of the DASA for Māori, and (3) the recommendations for the adaptation of the DASA to be suitable for use with Māori. The 10 sub-themes were identified within these three key themes, as shown in Table 1.
Key themes and sub-themes from the first hui.
Theme 1: Strength and usefulness of the DASA for Māori
Participants identified the strengths of the DASA in its clinical utility in acute inpatient forensic mental health settings, as well as its practicability in assessing the necessity of seclusion or high care.
Clinical utility in acute inpatient forensic mental health settings
Participants perceived the DASA as relevant to acute inpatient forensic mental health settings. While inpatient violence is common in this setting, the DASA could provide nurses with a clear indication of an individual's risk of imminent aggression: In forensic mental health services, inpatient violence is so prevalent, especially in acute forensic mental health settings. We need the DASA to look out for potential imminent aggression that will occur every day. (Participant 5)
The DASA was also seen as having clinical utility, as DASA scores could guide nurses in developing effective strategies to prevent individuals from engaging in aggressive behaviour: By using the DASA, nurses could assess the individual's early warning signs and track trends of preventative treatment to prevent individuals from displaying aggressive behaviour. (Participant 5)
Participant 2, the only participant with prior experience using the DASA, viewed the DASA as a useful instrument for acute inpatient forensic mental health settings. The participant expressed that the DASA was useful as a clinical instrument, and its use was easily incorporated into the workflow. Individuals’ DASA assessment results were discussed at the weekly multidisciplinary team meetings, and all staff collectively implemented collaborative care planning to prevent potential aggressive incidents. As Participant 2 stated: I can see that it is a good instrument for the acute inpatient unit. The DASA was useful for making appropriate nursing interventions or care plans as a team. Then, we would detail these in our clinical notes and discuss them in detail at the multidisciplinary team meetings.
Practicality in assessing the necessity of the use of restrictive practices
Participants considered that the DASA would be a practical instrument used to evaluate the severity of acute situations and determine the necessity of implementing restrictive practices, such as the use of high care, restraint, or seclusion: The DASA will be a good instrument for someone nursed in seclusion. In acute situations, nurses would want to rate someone with a rationale for commencing seclusion, restraint, or high care. (Participant 3)
Participant 3 added that the results of the DASA assessments and early warning signs of aggression could guide nurses to make informed and justified decisions when assessing the necessity of implementing restrictive practices for individuals with a high risk of aggression and stated: If there is any change in an individual's presentation or if nurses identify any early warning signs of aggression, we will need DASA and consider using it.
Theme 2: Limitations of the DASA for Māori
Despite the several benefits of DASA, participants collectively identified three key limitations in its current form. First, the DASA instrument was not considered suitable for use in rehabilitation units. Second, the instrument was perceived to be insensitive in assessing the cultural aspects of aggression. Third, participants expressed concerns about the potential subjectivity bias in using the DASA.
The use of the DASA in forensic mental health rehabilitation units
The discussion among participants indicated a concern about DASA's suitability in rehabilitation units. Participants stated that the existing risk assessment and management processes within rehabilitation units were already encapsulated in safety plans (or care plans) to adequately address individuals’ risk factors. The employment of the DASA was seen as duplicating the efforts of existing risk assessment and management processes in rehabilitation units: When I compare the DASA to what we already do in the rehabilitation unit, the risk assessments we have in the rehabilitation unit are enough to address everything. I think it is doubling up more paperwork. (Participant 1)
Participants questioned the suitability of the DASA for rehabilitation settings. While the risk of aggression may still be present, service users within the rehabilitation unit are likely to present less frequent changes in their mental state and risk, compared to those in the acute unit. As such, DASA was considered to be a more suitable instrument for acute settings than rehabilitation units. In the rehabilitation unit, people tend to stay for a long time, and those people do not have many changes in their presentations. You may want to get the DASA done for acutely unwell people. (Participant 2)
Insensitivity in assessing the cultural aspects of aggression
Participants expressed that one of the major limitations of the DASA was its inability to fully capture the essence of cultural expressions of emotions unique to Māori. Participants offered specific illustrations, such as the haka (Māori cultural practice), to exemplify their collective concerns about the DASA's insensitivity in assessing cultural aspects of aggression. If someone with no cultural awareness observes haka, then this person could mark the DASA scores as high. (Participant 3)
Participants added that individuals from non-Māori cultures might not be able to interpret the cultural context of the haka thoroughly. As a result, those non-Māori individuals could misinterpret this form of Māori cultural expression of emotion as aggressive behaviour: Haka might be interpreted as an expression of aggression for non-Māori individuals, but it is just a way of showing our passion in a way that we express our Māori culture. (Participant 2)
Subjectivity bias in interpreting individual risks with the DASA
During the discussion, participants raised concerns about the potential impact of subjectivity bias in assessing individual risks using the DASA. Subjectivity, driven by personal perceptions, could considerably impact the DASA scoring process outcomes and lead to variations in risk evaluation when different assessors are involved. Participant 3 stated: The DASA is indicative of all those different interpretations of aggression. There is a lot of subjectivity bias in this instrument.
Participant 2 had a similar view and expressed concerns about potential subjectivity bias in the assessment process using the DASA. Participant 2 added that different nurses might have varying interpretations of an individual's risk, which could result in discrepancies when assigning individual scores: Different nurses get different interpretations. Different nurses might give different DASA scores. Without seeing the person, one nurse could say, “Yeah, put that person in high care because you have rated that person as seven”, or “I do not even need to see that person because this person's DASA score is seven”.
Theme 3: Recommendations for adaptation
Participants collectively identified five options for adaptations that could be made to the current version of the DASA to overcome the limitations that participants had described. The suggested adaptations are organised into five sub-themes, each focusing on a specific area where improvements could make the DASA more clinically useful and culturally responsive to Māori.
The integration of collective decision-making in evaluating the total DASA scores
Participants emphasised the importance of integrating collective decision-making when evaluating individuals’ total DASA scores. They recommended adopting a collaborative approach to evaluating total DASA scores to mitigate concerns regarding subjectivity bias. In light of this recommendation for adaptation, participants viewed the DASA as a team responsibility, suggesting that the evaluation of total DASA scores should be integrated into the collective efforts of all nurses on the shift as a team: You should do DASA as a team. Staff should discuss those total DASA scores together, and the early intervention, and plan what to do next. (Participant 2)
Participants’ views on the collaborative approach entailed the participation of all nurses as a group to collectively evaluate an individual's total DASA scores and develop a mutually agreed care plan to optimise safety and recovery for the individual: So, rated a DASA score of seven…Because the score of seven is high, that score would even be at a level for team discussion. At the team meeting, all staff would collectively agree on the total scores and see what the best intervention for this person is. (Participant 3)
The inclusion of service user perspectives in the assessment of risk
Including service user perspectives in risk assessment emerged as a central sub-theme among participants. Participants provided an example where individuals’ aggression was triggered by the mispronunciation of their name. By illustrating this example, the participant highlighted the possibility of misinterpretations that may occur when service user perspectives are not considered in the assessment of risks: You may have a service user who is Māori, easily annoyed or angered. As a nurse, you should surely ask why they are angry. Maybe they are angry just because their names have been pronounced wrong? (Participant 4)
By advocating for the inclusion of service user perspectives in risk assessment, participants added that service users should be well-informed about the purpose of the DASA and its application to risk assessment: Tāngata whai i te ora (a person seeking health) needs to be involved in the risk assessment processes. When nurses use DASA, we should tell those individuals that we will use this instrument and explain why. (Participant 3)
Inclusion of space to document the rationale behind DASA scoring
Participants expressed that DASA should have space for nurses to document the rationale of their scoring decisions: There is no space to write the rationale behind DASA scoring…It is just like ticking yes or no. (Participant 5)
Drawing from prior experience utilising the DASA in the acute unit, one participant highlighted a limitation in the current structure of the DASA, stating that there was no dedicated space for nurses to provide rationale behind DASA scoring decisions. I remember we had to put DASA scoring from zero to high numbers, but there was no space to put the rationale. There is a need for space for the rationale behind DASA scoring decisions. What are you putting DASA scores for? (Participant 2)
The involvement of cultural expertise at the point of clinical decision-making about the outcome of the DASA score
Participants stated that Māori cultural advisors should be involved at the point of clinical decision-making about the score: If you have no Māori down there, how can we assess and put scoring for Māori service users that come in? We just need taurawhiri (Māori cultural advisors) to come in with their cultural expertise. (Participant 2)
Participants added that the involvement of Māori cultural advisors would ensure that the interpretation of DASA assessment outcome is undertaken with cultural sensitivity. The cultural expertise of a Māori cultural advisor could offer valuable insight into the holistic needs specific to Māori: If this person did not have that plan, you must involve the Māori cultural advisors to bring in that cultural aspect specific to Māori. This might not be okay for the service users who are Māori, but at least it is a start because it is the culture and where and what Māori see fit. (Participant 3)
The inclusion of the Tikanga Māori approach throughout the existing DASA contents and assessment process
Participants suggested integrating tikanga Māori approaches (Māori customary practices) throughout the existing DASA content and assessment processes. Participants viewed this approach as promoting cultural responsiveness to risk assessment. In light of these recommendations, the cultural advisor called for translating the DASA into te reo Māori (the Māori language), suggesting that DASA items should be named in te reo Māori alongside English: When we are talking about the cultural aspects of this instrument [DASA], it is about using the language that may interpret the essence of Māori culture to make that instrument more appropriate for Māori. If we include te reo Māori language, I recommend it to be alongside English. (Māori cultural advisor)
One participant had a similar viewpoint, suggesting the cultural translation of the DASA item names into the Māori language. For example, using the word “pukuriri” (a Māori term meaning irritability) to describe irritability can enhance the cultural relevance of the risk assessment for service users who are Māori: If we are going to make the DASA specific to Māori, I would be inclined to at least include Māori words in there, in line with Te Ao Māori (the Māori worldview). For example, the term “irritability” could be translated to “pukuriri”. (Participant 1)
In addition to making linguistic adjustments, participants recommended integrating culturally specific practices into the risk assessment process. One such practice recommended was the mihi whakatau (a Māori welcome ceremony), a ceremonial greeting used to welcome new service users encountering the service. Participants emphasised that initial contact through this cultural practice is crucial for establishing a culturally safe and supportive environment for service users who are Māori. Therefore, such culturally specific practices should occur before conducting the risk assessment: If we have a new admission entering the service from prison, staff will be all in there to meet this person and facilitate tikanga Māori (Māori customary practices) process, such as mihi whakatau. Then, the staff would do a risk assessment with that person. This sounds like a flowing process that provides a culturally safe environment for those individuals. (Participant 3)
Action
At the end of the first hui, all participants agreed that further discussion was required to reach a consensus on the adaptations that could be made to the DASA. Participants agreed that the summary of the first hui discussion was required to inform the second hui discussion, with the view of returning it to the group of participants for further consultation. Participants suggested that the facilitator not rush this process, and a collective decision was made to reschedule the second hui one month later.
The second hui
All participants in the second hui reaffirmed their endorsement of the outcomes from the first hui, which they felt had collectively established a solid foundation to develop the DASA to be more culturally responsive for service users who are Māori. The data analysis from the first hui was presented to participants at the second hui, which informed the discussion that followed: Lots of good points were addressed at the last hui. We need to make a huge change on it [DASA] to ensure its relevance for Māori. (Participant 5)
Participants collectively affirmed their commitment to the cultural enhancement of the DASA and reached a point of consensus about this enhancement. All participants agreed that integrating all five recommendations for adaptations would be the optimal way to enhance the instrument for Māori: It is just time to start looking back at what was addressed at the last hui. The solution is all there on how DASA could be refined to be culturally relevant for use with Māori. (Participant 2)
In light of this consensus, participants reiterated that it must be Māori guiding and defining this integration, as only Māori hold mātauranga Māori (Māori knowledge): We cannot have non-Māori making these decisions if they are not Māori. Our genetic makeup is different. So, you need those Māori people to make decisions that hold mātauranga Māori. (Participant 3)
The Māori cultural advisor emphasized that integrating the DASA would require the involvement of cultural expertise at the point of decision-making: If the DASA needs to be used with Māori, we need senior cultural expertise within the service at that level to guide the decision-making of this instrument we use.
Action
The facilitator was responsible for ensuring that the momentum of the research project continued. The second hui discussion was facilitated until all participants collaboratively established a consensus decision about the options for adaptations. At the end of the second hui, all participants expressed satisfaction with the outcome of the hui; therefore, no further consultation was required.
Discussion
Risk assessment plays a significant part in forensic mental health nurses’ daily practice (Gerace et al., 2012). Identifying service users who require support and interventions to prevent acts of aggression is established by nurses’ routine uptake of risk assessment (Woods, 2013). Concerning the value and responsibility of conducting the risk assessment, the literature suggests that risk assessment is a core aspect of forensic mental health nurses’ roles and critical to aggression prevention efforts (Maguire et al., 2022). This finding resonates with the views of participants in this study, who considered the uptake of risk assessment as part of nurses’ responsibilities while indicating strong support for risk assessment in daily clinical practice.
In this study, a discussion among participants indicated a concern about the prevalence of inpatient aggression in FMHS. Participants suggested that there is a need for effective strategies to prevent individuals from engaging in high-risk behaviours. In this regard, there was a collective expression by participants that the DASA could be a useful instrument for guiding decisions on the use of restrictive practices. Nevertheless, this perspective warrants scrutiny. It is important to note that using the DASA to guide decisions on restrictive practices fundamentally deviates from its original purpose of assessing the individual's risk of imminent aggression (Ogloff & Daffern, 2006). This deviation raises questions about potential participant misinterpretations regarding how the DASA should be used. Such misinterpretations may stem from the absence of formal education on the DASA within the service. Therefore, training within the service is necessary to ensure an accurate understanding and application of the DASA's intended purpose.
The findings of this study indicate support for the use of DASA with service users who are Māori. Nevertheless, there was a prerequisite for this support. For the DASA to be safely used with Māori, there was a recognition of the need for the current content and process of the DASA to be refined locally within a cultural context and validated with Māori accordingly. In determining the suitability of the DASA for Māori from a Māori perspective, the recurrent themes of concern centred on cultural meanings related to the expression of emotions. An illustrated example of this expression was the haka, which is a Māori cultural practice that involves rigorous rhythmic movements, such as stomping on the feet and slapping of the chest and thighs (Clément, 2017). Concern was expressed that non-Māori may misinterpret haka as aggressive, if non-Māori individuals were unfamiliar with the cultural significance behind this expression. In this regard, there was a collective view that the present version of the DASA would require cultural enhancement and validation to establish an understanding of risk relevant to Māori.
Participants’ conditional support of using the DASA with Māori resonates with the findings of other research, which highlight the importance of cross-cultural validation of risk assessment instruments (Coulter et al., 2023). The need for such validation has become a subject of investigation in the international literature, given the prevailing concerns about the suitability of such instruments for Indigenous populations (Shepherd & Lewis-Fernandez, 2016). Internationally, risk assessment instruments in forensic mental health settings are often developed and validated primarily with non-Indigenous populations (Coulter et al., 2023). However, these instruments are then used to assess Indigenous individuals’ risk without explicit cross-cultural validation (Shepherd & Spivak, 2021). The court proceedings in Canada ( Ewert v. Canada, 2015 ) highlight that this practice is inappropriate and underline the potential negative consequences that could occur from such practice. In Ewert v. Canada (2018), expert testimony discovered that some structured risk assessment instruments were culturally biased and unreliable for use with Indigenous peoples in Canada. The Supreme Court concluded that the Correctional Service of Canada violated its legal obligations by employing risk assessments that were not validated for use with Indigenous populations (Ewert v. Canada, 2015). This court ruling suggests that the cross-cultural validation of risk assessment instruments with Māori is an important issue that requires attention.
For risk assessment instruments to be valid for use with service users who are Māori, it is important to adopt an academic approach in developing and introducing such instruments. This academic approach requires the commencement of cross-cultural psychometric testing to assess the instrument's validity with Māori. Furthermore, this approach entails making any required modifications from the outset rather than introducing the instrument into clinical settings without cultural validation by the populations concerned. According to Shepherd and Lewis-Fernandez (2016), cross-cultural psychometric testing can provide an understanding of how culturally specific expressions of emotions impact the risk of Indigenous individuals being assessed. In the case of the DASA, adopting this overall academic approach becomes critical to ensure that the risk items and content within the DASA framework align with the cultural expression of Māori. Unfortunately, such strategic approaches were not adequately taken when DASA was initially introduced to the ARFPS in New Zealand. Hence, participants’ concerns about the suitability of DASA with Māori were valid, bringing attention to shortcomings in how the instrument was introduced.
Participants in this study recommended specific adaptations for DASA's cultural enhancement to ensure its suitability for Māori. The study presents two important concepts for the cultural enhancement of the DASA. The first concept is collective decision-making. The term collective decision-making refers to a process whereby the group members decide on a course of action based on consensus (Montes de Oca et al., 2011). To date, no published literature has explicitly described the concept of collective decision-making in the FMHS context in New Zealand. Despite this, one evidence-based practical example of collective decision-making in mental health nursing is the “safety huddle.” The safety huddle is a short, focused team gathering where teams collectively identify safety risks within the unit that require immediate action (Gray, 2020). Currently, no research specifically examines the value of the safety huddle in the FMHS context in New Zealand. However, international evidence suggests that introducing daily safety huddles in secure forensic mental health units helps reduce the incidents of inpatient violence and promotes a positive work environment (O'Sullivan et al., 2020). In keeping with the notions of collective decision-making, participants in this study proposed integrating DASA assessment procedures into the safety huddle format. Participants considered that this integration could allow nurses to use a similar team-based method to collaboratively evaluate individuals’ total DASA scores. There was also a view among participants that such integration could ensure a shared understanding of the rationale behind DASA scores, helping to address the perceived limitations regarding the absence of space on the current DASA form to document the scoring decisions.
The shared decision-making was another concept considered essential for the cultural adaptation of the DASA. The concept of shared decision-making recognises the importance of service users being empowered to actively participate in their care and reach a decision about their treatment with assigned healthcare professionals (Laight, 2022). In this study, the participants’ notion of shared decision-making implied the active engagement of service users in the assessment of risk while acknowledging the expertise of both nurses and service users to produce better decisions and potentially better health outcomes. Participants’ emphasis on shared decision-making resonates with findings from other studies, which emphasise that risk assessment should be more inclusive, transparent and collaborative between service users and staff (Markham, 2020; Shepherd & Lewis-Fernandez, 2016). As suggested by study participants, integrating the shared decision-making concept into the current DASA framework could promote a holistic and culturally informed approach to understanding and addressing risks specific to service users who are Māori.
In light of the emphasis on shared decision-making, another key suggestion was the involvement of Māori cultural advisors at the point of determining the total DASA scores. Although being clinically useful in many contexts, the predefined item descriptions within the existing DASA do not capture the cultural nuances that inform the understanding of risks in a Māori context. The complexity of these cultural dimensions requires a holistic approach that integrates Māori expertise into the risk assessment process. Therefore, it was recognised that involving Māori cultural advisors to clarify these cultural complexities is crucial when the total DASA scores are evaluated to inform shared decision-making.
With the proposed adaptations of collective decision-making and shared decision-making, consultation with Māori cultural advisors would be required to establish the cultural enhancement of the DASA. In this study, it was emphasised that only Māori who are competent in mātauranga Māori (Māori knowledge) should define and guide this cultural enhancement. Royal (1998) defined mātauranga Māori as “the explanation of human behaviour that is based upon traditional concepts handed down through the generations” (p. 2). Two influential authors in New Zealand (Durie, 1998; Mead, 2003) concur with Royal (1998) in viewing mātauranga Māori as a Māori way of being and engaging in the world. This Indigenous worldview represents a unique knowledge system that only Māori can interpret, which is distinct from Western worldviews (Kiro, 2000). The emphasis on mātauranga Māori highlights the importance of involving Māori cultural expertise in the process of refining the existing DASA. There was a view among participants that Māori cultural advisors are the appropriate individuals for this process. The Māori cultural advisors’ expertise in mātauranga Māori could ensure that the cultural enhancement occurs within a Māori cultural context. Once this enhancement is established, the outcome would then need to be psychometrically tested for reliability and validity with service users who are Māori.
Limitations and recommendations for future study
The qualitative nature of the study may limit the generalisability of the findings, as the study specifically explores a Māori perspective. The study findings are grounded in one particular cultural context, and therefore, the findings may not be applicable to other ethnic groups or broader populations (Denzin & Lincoln, 2011). Furthermore, this study was limited by data collection from Māori nurses in one regional forensic mental health setting. As such, the restricted scope of the data collection site may impact the transferability of the research findings to other settings. A replication of the study in a different setting would provide greater empirical support for the findings in this study. Another recommendation for future study relates to the recent development of an Aggression Prevention Protocol (APP; Maguire et al., 2019). The APP has been developed as a risk management framework, which targets preventative interventions aligned with the level of risk assessed using the DASA (Maguire et al., 2019). Given that this study did not include Māori perspectives on the use of APP interventions, this remains an area for future study.
Conclusion
This study presents the first effort to evaluate the suitability of the DASA for Māori from a Māori perspective. This study's findings confirm support for using this instrument with service users who are Māori and substantially over-represented in FMHS in New Zealand (McKenna, 2020). However, the present version of the DASA was considered limited in its ability to consider or reflect Māori cultural elements. To address this limitation, options for adaptations were suggested for the cultural enhancement of this instrument. Such enhancement would warrant a collaborative process with Māori expertise to guide the development and validation of any changes to the DASA.
Footnotes
Ethical considerations
The Auckland Health Research Ethics Committee granted ethical approval, and locality authorisation was obtained from the service concerned.
Consent to participate
All participants signed informed consent on the day of first hui.
Author contributions
All authors contributed to the design and/or conduct of the study. All authors approved the current version of the review.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The datasets generated and analysed during the current study are not publicly available in accordance with the conditions of the ethics approval and participant consent.