
Abstract
Objectives
Home-based pulmonary rehabilitation (PR) is increasingly offered as an alternative to centre-based PR. This study explores differences in the characteristics of people with COPD enrolling in home-based versus centre-based PR in England and Wales and assesses whether availability of home-based PR is associated with increased enrolment.
Methods
This study used data from the UK 2023-24 National Respiratory Audit Programme PR audit. Eligible people had a primary condition of COPD, complete mental health and geographic data, and attended an initial assessment at a centre that completed the clinical and organisational audit. For the primary analysis only, people were further restricted to those enrolled on a purely home-based or centre-based programme at a centre that offered both options. Enrolment was defined as having attended an initial assessment and having at least one scheduled PR session with a defined start date. Differences in characteristics were assessed using Chi-square and Kruskal-Wallis tests. The association between availability of home-based PR and enrolment was assessed using a mixed-effects logistic regression model.
Results
13719/29981 (45.8%) people were eligible for inclusion in the primary analysis and 25039/29981 (83.5%) were eligible for the secondary analysis. Those who enrolled in a home-based programme were more likely to: be female (58.6% vs 48.2%; p<0.001); be more deprived (55.7% versus 46.6% in IMD quintiles 1 or 2, p<0.001); have a greater mental health burden (28.2% versus 22.2% with at least 1 cognitive impairment recorded, p<0.001); and classified their symptom burden as more severe at assessment (CAT score 23 versus 22, p <0.001). Home-based PR was unavailable for 9099/25039 (36.3%) people. Availability of home-based PR was not associated with reduced non-enrolment in PR when compared with centres that did not offer home-based PR (adj-OR for non-enrolment: 0.79; 95%CI:0.51-1.23)).
Conclusion
Healthcare providers and those developing home-based PR digital applications should consider tailoring their approach to those who are most likely to opt in, who tend to be younger, female, and have a higher burden of respiratory symptoms and mental health comorbidities.
Introduction
People with chronic obstructive pulmonary disease (COPD) are encouraged to take part in pulmonary rehabilitation (PR), as there is strong evidence that PR is effective and cost-effective at reducing the burden of COPD. 1 Undertaking a centre-based PR programme as part of a group can provide social support and motivation.2,3 However, not all people are able or willing to attend centre-based in-person PR sessions, and may be enrolled on a home-based programme instead. Home-based PR encompasses a broad range of delivery mechanisms, ranging from in-person one-to-one supervision at home 4 to group-based video conferencing 5 to unsupervised web-based PR programmes. 6 A Cochrane review of telerehabilitation for people with chronic respiratory disease (PR delivered through the use of communications technology) did not find differences in effectiveness between home-based telerehabilitation and centre-based PR, although the authors note that the telerehabilitation components of included studies were heterogenous and it was not possible isolate the effectiveness of particular components. 7
A mixed methods study on telerehabilitation for PR found that over half of people interviewed undertaking telerehabilitation mentioned that access to PR exercise equipment and professional support without needing to attend a centre saved time and costs and was more convenient. 8 In the UK, British Thoracic Society (BTS) guidelines recommend that those who could benefit from PR are directed towards centre-based PR. 3 The guidelines conclude that evidence into the effectiveness of home-based PR remains heterogenous, and that home-based PR should only be offered as a secondary option if centre-based PR is refused or the patient drops out. In the USA, both centre-based PR and telerehabilitation are offered together with no hierarchy of offer. 1
There is some evidence to suggest that home-based PR is as effective as centre-based PR1,9–13 with no reported differences in exercise capacity or health and quality-of-life outcomes, and a secondary analysis of two randomised controlled trials found that the risk of non-completion was nearly four times greater in centre-based compared with home-based PR. 12 The National Institute for Health and Care Excellence (NICE) has put out a recent call for evidence surrounding the effectiveness of home-based, digital PR programmes. 14 Whilst some studies have assessed the factors that contribute to non-attendance for PR, 15 so far there is little published data on the characteristics of people that attend home-based as opposed to centre-based PR. A greater understanding of these people is crucial in planning and commissioning services and in determining the overall effectiveness of new home-based delivery methods in the general population. Using data from the UK National Respiratory Audit Programme, this study assessed whether differences exist in the characteristics of people with COPD that undertake home-based PR rather than centre-based PR, and whether the availability of home-based PR is associated with an increase in overall PR enrolment rate at centres that offer both home-based and centre-based options compared to centres that offer centre-based PR only.
Methods
Setting and data sources
This study used pulmonary rehabilitation data obtained from the National Respiratory Audit Programme (NRAP), which is a continuous national audit of asthma and COPD in primary, secondary and tertiary care across England and Wales commissioned by the Healthcare Quality Improvement Partnership and carried out by the Royal College of Physicians. This study used data from the 2023-24 pulmonary rehabilitation (PR) clinical and organisational audits. For the clinical audit, PR centres submit clinical, demographic and administrative data on people who have been assessed for PR at the centre using an online tool, with data anonymised and transferred to Imperial College London for data processing. 16 Centres also submit practice-level data annually with information about their policies and PR programme structure as part of the organisational audit. 17
Study design
This study followed a cross-sectional study design using data collected over the course of one year as part of the PR audit. The primary analysis assessed the differences in characteristics of people with COPD who enrolled onto home-based versus centre-based PR programmes. The secondary analysis assessed whether enrolment rate was associated with provision of home-based PR.
Participants
To be eligible for inclusion in the pulmonary rehabilitation audit, people must be aged 18 or over, have attended an initial assessment for pulmonary rehabilitation at a participating centre between 1st April 2023 and 31st March 2024, and have given their consent for inclusion in the audit. The data then undergoes a cleaning process to remove duplicates and records with logical inconsistencies. All scripts used in the cleaning process can be found at https://github.com/NationalAsthmaCOPDAudit. To be eligible for inclusion in this study, people in the audit must additionally: 1) have been assessed at a centre that provided complete organisational data to the organisational audit; 2) have a primary condition of COPD; 3) have complete Lower Super Output Area (LSOA) residential information; 4) have non-missing data for current mental illnesses or cognitive impairments. If a participant had more than one record in the audit, one record was chosen at random for inclusion in the analysis using the ‘sample’ function in R. For the primary analysis (but not the secondary analysis), people must have been enrolled onto a purely home-based or purely centre-based PR programme at a centre that offered both options. To be enrolled, the participant must have attended an initial assessment and have at least one scheduled PR session with a defined start date.
Variables
Clinical audit data was collected using an online web tool using patient and administrative data that had been recorded concurrently at time of assessment and discharge for PR.
Primary exposure
The primary exposure was whether a person was enrolled onto a home-based or centre-based PR programme. Home-based programmes could be classed as ‘in person’, ‘video-conferencing’, ‘phone calls’ (including manual programmes such as SPACE 18 ), or ‘other digital communication’ (including structured email contact and app-based programmes).
Variables of interest
Patient characteristics of interest were: gender (male, female, not recorded/prefer not to say, transgender), age (continuous variable), ethnicity (White, Black, Asian, Mixed ethnic background, not known/not stated), combined England and Wales Index of Multiple Deprivation (IMD), 19 a measure of relative deprivation based upon the lower super output area (LSOA) of the person’s address which was included as a categorical variable using quintiles from 1 (most deprived) to 5 (least deprived); rurality, obtained through linked ONS rurality data 20 (urban/rural); and any record of the follow mental illnesses or cognitive impairments: anxiety, depression, ‘severe mental illness’, ‘dementia/mild cognitive impairment’, and ‘other mental illness or cognitive impairment’. Also of interest were lung function and test results obtained or recorded at assessment: walking test (6-minute walk test 21 or incremental shuttle walk test 22 ) completed and practice test undertaken; endurance shuttle walk 23 completed and practice test undertaken; forced expiratory volume in 1 second (FEV1)/forced vital capacity (FVC) (FEV1/FVC); FEV1 %-predicted; Medical Research Council (MRC) dyspnoea score 24 (from Grade 1 ‘Not troubled by breathlessness except on strenuous exercise’ to Grade 5 ‘Too breathless to leave the house or breathless when dressing or undressing’); Chronic Respiratory Questionnaire (CRQ) 25 score for measuring the quality of life in people with chronic respiratory disease, (split into the four elements of dyspnoea, fatigue, emotion, and mastery, where each element can be receive a score from 1 (lowest quality of life) to 7 (highest quality of life) based upon the average score of questions within a particular element); and COPD assessment test (CAT) 26 to measure patient quality of life in people with COPD, with a score from 0 (least severe) to 40 (most severe). Finally, data was also collected on how the person had been referred for PR (primary care, secondary care post-acute exacerbation of COPD (AECOPD), secondary care stable COPD, and self-referral).
Secondary exposure and outcome
The secondary exposure was whether a centre offered home-based PR, which was obtained from the PR organisational audit. The secondary outcome was whether the person was enrolled, which is collected as part of the clinical audit.
Statistical methods
For the primary analysis, differences in patient characteristics and tests between people enrolled on centre-based and home-based PR were assessed using chi-square tests for categorical variables or Kruskal-Wallis tests for continuous variables. To account for multiple testing, a Bonferroni correction 27 was applied when assessing statistical significance. For the secondary analysis, the association between the availability of home-based PR and enrolment was assessed using a mixed effects logistic regression model which included enrolment as the outcome and availability of home-based PR as the independent variable. The model additionally included the covariates age (quadratic), gender, ethnicity, deprivation, rurality, mental impairments, referral location, MRC grade, and CAT score in the model a priori as potential confounders. PR centre was included as a clustering variable to account for differences in centre-level characteristics. Missing data for MRC grade and CAT score was imputed using multiple imputation, with a complete-case analysis performed as a sensitivity analysis. The model was constructed to predict non-enrolment so that odds ratios approximate risk ratios. Statistical analysis was carried out using R version 4.4.1. 28
Ethical approval
The PR audit operates under Section 251 approval from the Confidentiality Advisory Group (CAG) of the Health Research Authority (HRA) (23/CAG/0167), meaning that individual patient consent is not required for this study. This work is covered under the HQIP overarching research CAG (24/CAG/0108) which includes research ethics approval (REC 24/YH/0175).
Results
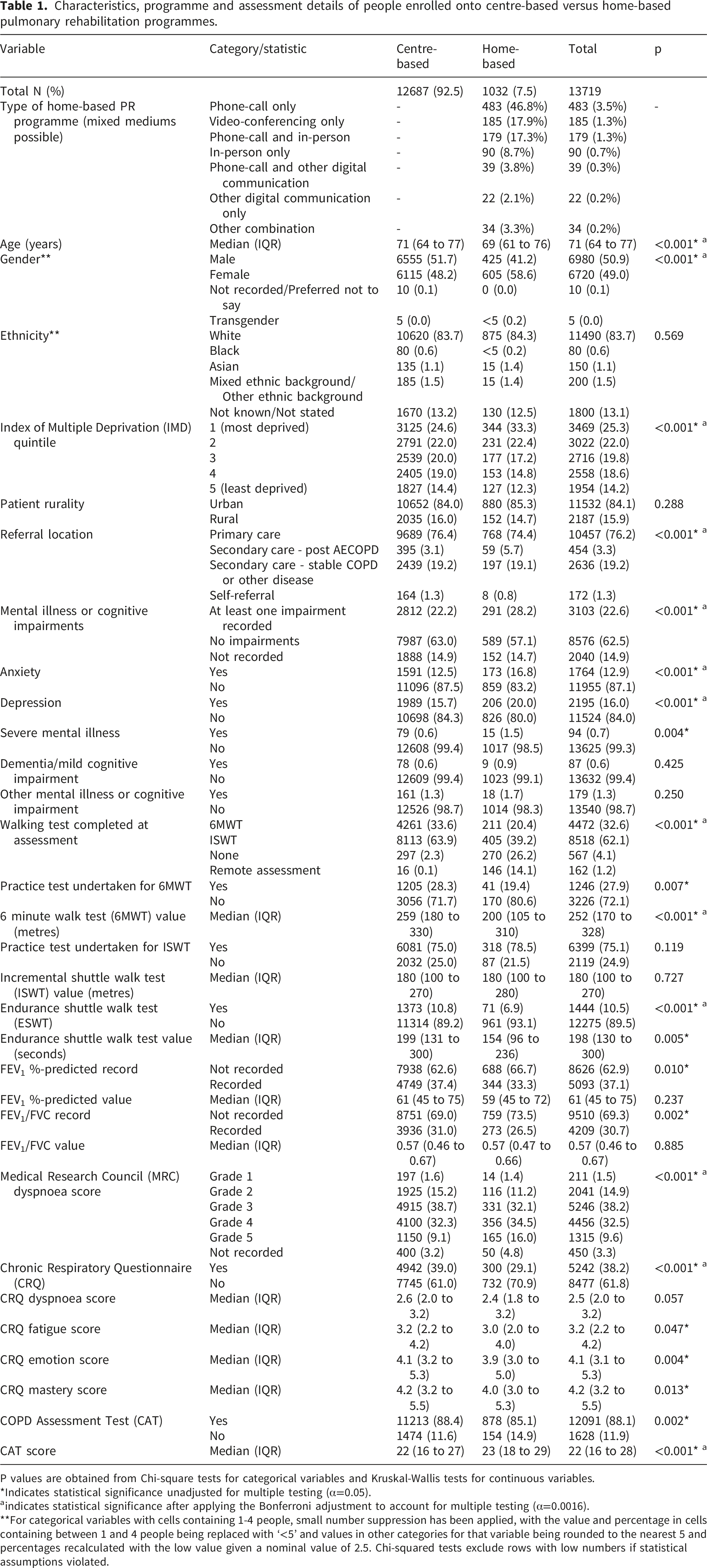
30,443 records from 29,981 individuals across 183 centres were submitted to the PR audit. After applying the eligibility criteria, 13719/29981 (45.8%) people across 93 centres were included in the primary analysis and 25039/29981 (83.5%) people across 160 centres were included in the secondary analysis (Figure 1). 93 out of 160 centres (58.1%) offered home-based PR. Differences between people who were enrolled onto home-based verses centre-based PR are displayed in Table 1. Those who enrolled in a home-based programme were two years younger on average (69 versus 71 years, p<0.001) and were more likely to: be female (58.6% versus 48.2%; p<0.001); be more deprived (55.7% versus 46.6% in IMD quintiles 1 or 2, p<0.001); have a greater mental health burden (28.2% versus 22.2% with at least one mental illness or cognitive impairment recorded, p<0.001); and were generally less likely to receive walking tests (59.6% versus 97.5% undertook one of 6MWT or ISWT, p<0.001). Those that completed a 6MWT were less likely to receive a practice test if enrolled onto home-based rather than centre-based PR (19.4% versus 28.3%, p=0.007), but this difference was not seen in the ISWT where practice rates were equivalent (78.5% versus 75.0%, p=0.119); likewise, those who enrolled onto home-based PR performed worse on the 6MWT (200m versus 259m, p<0.001) but not on the ISWT (180m versus 180m, p=0.727). Those enrolled onto a home-based programme were slightly less likely to have a recording of FEV1 %-predicted (33.3% versus 37.4% recorded, p = 0.010) and FEV1/FVC (26.5% versus 31.0%, p = 0.002), but no statistically significant differences in lung function were observed in those where a recording was present (p=0.237 and p=0.885). Those enrolled onto a home-based programme were also less likely to undertake CRQ (29.1% versus 39.0%, p<0.001) and CAT (85.1% versus 88.4%, p=0.004) health-related quality-of-life questionnaires and tended to experience a slightly decreased quality of life and have a higher MRC score (Table 1). People enrolled onto a home-based PR programme were more likely to have been referred post-AECOPD compared to those enrolled onto a centre-based programme (5.7% versus 3.1%, p<0.001). Rurality did not show a statistical difference between forms of delivery (p=0.288). Flow chart showing patient eligibility criteria for study analyses. Characteristics, programme and assessment details of people enrolled onto centre-based versus home-based pulmonary rehabilitation programmes. P values are obtained from Chi-square tests for categorical variables and Kruskal-Wallis tests for continuous variables. *Indicates statistical significance unadjusted for multiple testing (α=0.05). aindicates statistical significance after applying the Bonferroni adjustment to account for multiple testing (α=0.0016). **For categorical variables with cells containing 1-4 people, small number suppression has been applied, with the value and percentage in cells containing between 1 and 4 people being replaced with ‘<5’ and values in other categories for that variable being rounded to the nearest 5 and percentages recalculated with the low value given a nominal value of 2.5. Chi-squared tests exclude rows with low numbers if statistical assumptions violated.
Adjusted and unadjusted odds ratios from mixed effects logistic regression models for the association between home-based pulmonary rehabilitation availability and patient characteristics and enrolment. Odds ratios >1 indicate that a variable is associated with failure to enrol. Adjusted odds ratios are obtained from a mixed effects model that include all presented variables and includes PR centre as a random intercept. Unadjusted odds ratios are obtained from separate models for each variable, with PR centre included as a random intercept. The outcome for the regression models is failure to enrol.
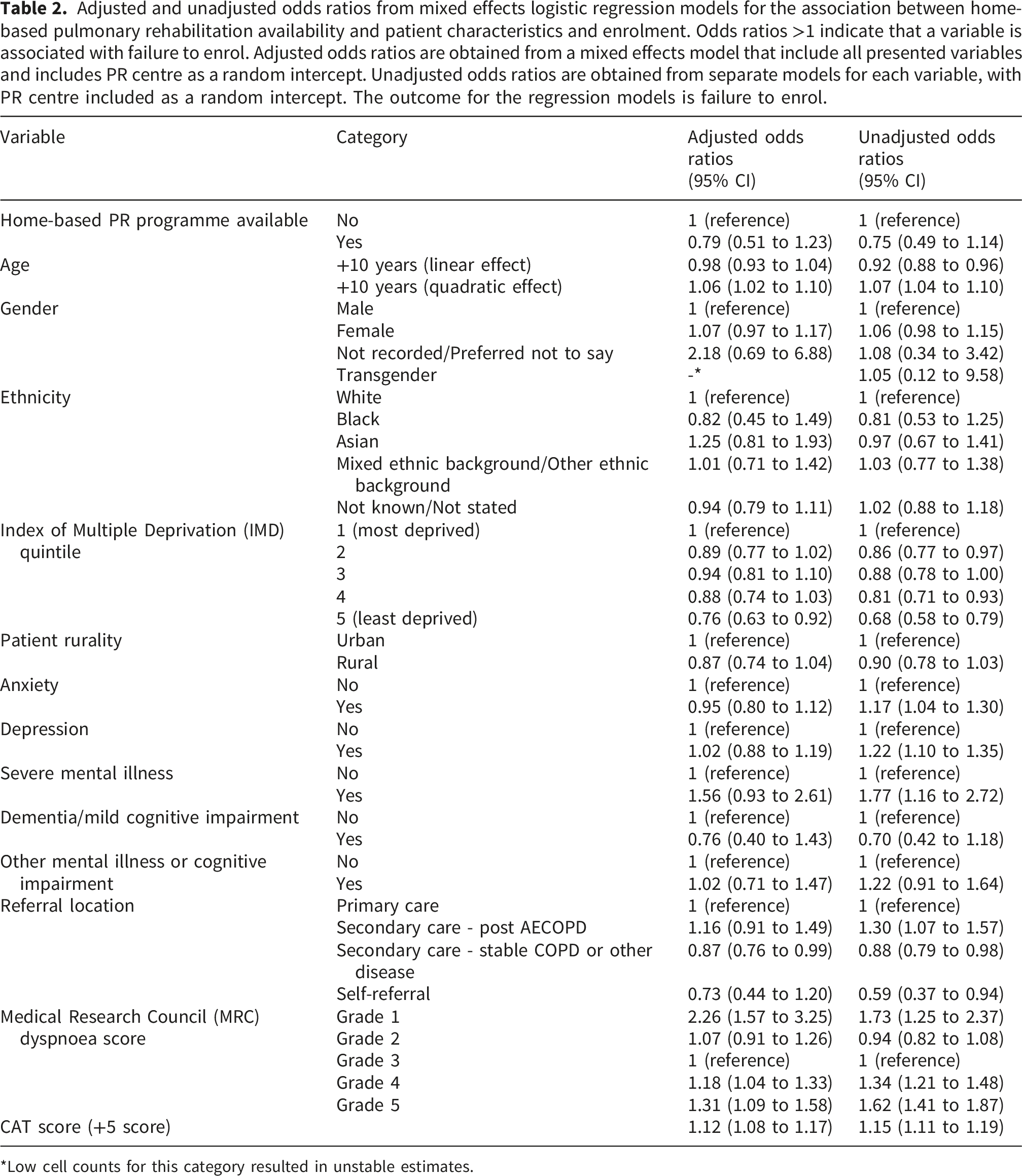
*Low cell counts for this category resulted in unstable estimates.
Discussion
Summary of main findings
We found that people with COPD that enrolled in home-based rather than centre-based PR were more likely to be younger, female, more deprived, and have a higher burden of mental health impairments and respiratory symptoms reflected in health-related quality-of-life questionnaires. We found that age, deprivation, and respiratory symptom burden were associated with non-enrolment. However, we did not find evidence that the availability of home-based PR services affected enrolment.
Research in context
There is evidence to suggest that home-based PR may be as effective as centre-based PR,9,12 although the evidence-base is sparse and heterogenous and remains inconclusive. 3 Whilst the number of people enrolling in home-based PR over centre-based PR is small (7.5% in our study population), this number may be expected to rise with the increase in the home-based offerings available and a population that experienced a shift to remotely-provided healthcare during the coronavirus-19 pandemic, along with the recently released NHS 10 year plan promoting a shift from analogue to digital care. 29 A qualitative study that interviewed people that took part in a randomised controlled trial of a home-based versus centre-based PR programme 30 found that people often liked the flexibility of the home-based trial, with people who were self-conscious about exercising with others able to exercise alone in a comfortable environment. This may correspond with the results from our study which found a greater prevalence of anxiety and depression in people who enrolled in home-based PR. Given that the overall uptake of centre-based PR after referral is low, 31 any increases in the accessibility of PR should be welcomed. A non-randomised preference-based non-inferiority trial of home-based versus centre-based PR 32 found that 36% of people opted for home-based PR, a far greater percentage than in our study, however this was based on a much smaller total sample size of 105 people and the eligibility criteria included all chronic respiratory diseases. Much like in our study, people opting for home-based PR were younger, although unlike our study there was no difference in preference by gender. A mixed-methods systematic review of adherence to home-based PR identified severity of respiratory symptoms as a barrier to completion of PR, 33 highlighting that whilst those with more severe respiratory symptoms are more likely to enrol on home-based PR, they remain less likely to complete it.
There are two ongoing trials in this area that are directly relevant to this study. The HomeBase2 trial 34 is an ongoing cluster-randomised controlled trial based in Australia which looks to identify whether giving people the option of home-based or centre-based PR improves completion rates and health outcomes over the sole provision of centre-based PR alone. Unlike our study, which focused on enrolment as a secondary objective, the HomeBase2 trial only includes people who have been assessed and enrolled. The results of our (non-randomised) study suggest that this is unlikely to be an issue, with enrolment not being associated with availability of home-based PR. Along with providing strong evidence on how the availability of PR options affects outcomes, this trial will provide useful information on the patient characteristics of a study population from outside of the UK. The REPORT trial is another ongoing randomised controlled trial, based in Denmark. 17 People who decline centre-based pulmonary rehabilitation are eligible to take part in this study, which compares usual care (no PR) to one-on-one face-to-face home-based PR and group tele-health (home-based) PR. The premise for this study is that people who decline centre-based PR are a distinct population who may still benefit from home-based PR. Although no direct comparison with people taking part in centre-based PR will be possible in this trial, the study will provide important evidence into the effectiveness of home-based PR in the important sub-population of patients that decline centre-based PR but not home-based PR.
Implications for further research
The quality of the assessment test for those that were enrolled onto a home-based versus centre-based course appeared to be lower, with participants less likely to receive walking tests, practice tests, and measurement of health-related quality of life, and were more likely to undergo a remote assessment despite BTS guidelines recommending in-person assessment regardless of the mode of PR delivery. 3 Recommendations for in-person assessment are partly due to lack of evidence of the reliability of remote exercise tests35–37 and further research in this area is important if there is a shift towards remote assessment for home-based PR. Remote assessment should not hinder the provision of a health-related quality of life questionnaire, and understanding why these questionnaires are less likely to be used in those enrolling into home-based PR is especially important from both a patient perspective and a research perspective given the uncertainties in the effectiveness of home-based PR. Moreover, our research suggests that practice tests are more commonly carried out for the ISWT compared to the 6MWT; practice tests are required to ensure that the measured baseline is accurate and that improvements in tests are not simply due to a learning effect. 38 Given that 70% of patients did not receive a 6MWT practice test, compared to 25% of patients not receiving an ISWT practice test, we suggest that the ISWT may be the preferred test for objectively measuring clinical improvement after PR and that the importance of practice tests must be emphasised across PR services.
The lack of a statistically significant association between home-based PR and enrolment in the secondary analysis was contrary to our expectations and warrants further research, although the wide confidence intervals for this effect estimate suggest the analysis may be inadequately powered to identify a true effect. The lack of an observed effect could be because centres may have limited capacity to provide a home-based service and so do not encourage patients to enrol despite it being available. This result may also indicate that the opportunity to access home-based PR was not made obvious at the time of referral or was not supported by a shared decision-making process, resulting in low overall uptake of this option in centres where it was available. Ensuring that people considering PR know that flexible models exist at the initial discussion is vital to improve uptake by the most vulnerable members of the COPD community, which are identified in the analysis as the most likely to take up alternative delivery methods. This is important because our results showed that individuals with more severe respiratory symptoms are less likely to enrol in PR, despite being the individuals who stand to benefit the most. 3 Many people decline referral to PR 31 but the NRAP dataset only contains data on those who are referred and attend their initial assessment; this may mean that availability of home-based PR has a greater impact at the referral stage rather than the assessment stage but that this study was not able to be assess that.
Strengths and limitations
We consider the main strength of this study to be its large sample size, with the study cohort being obtained from a national audit of PR services in the UK. This led to a sample size of nearly 14,000 people for the primary analysis and over 25,000 people for the secondary analysis, which resulted in a study that was well-powered to identify true differences despite multiple testing. Being based upon a nationwide cohort that could theoretically include all people assessed for PR in England and Wales means that our results will certainly be applicable to England and Wales, and may also be applicable in other demographically and geographically similar nations. Another strength of our study is the availability of granular data on walking tests and respiratory symptom burden that is unlikely to be available in comparatively-sized population-based studies carried out using routinely collected electronic healthcare records.
One of the limitations of our study was the low numbers in some relevant categories, such as severe mental health impairments, that mean that our study was likely underpowered to capture true differences in these categories. When assessing the relationship between availability of home-based PR and enrolment, walking test results were not incorporated into the model. This was because over half of people who were not enrolled did not complete a walking test, compared with only 5.5% of people who were enrolled not completing one. This data was not imputed because of the risk of it being missing not at random. The inclusion of the CAT score and MRC dyspnoea score, both of which have been shown to be correlated with walk test results,39,40 will mitigate the exclusion of walking test data from the model somewhat. Given that we did not find an association between availability of home-based PR and enrolment and the adjusted and unadjusted estimates are almost identical, we consider it unlikely that the a priori covariates we included in the model are confounding the association between availability of home-based PR and enrolment, and that the addition of walking test data in the model would not alter the overall conclusions.
Conclusions
Our results provide a substantial evidence-base for researchers and healthcare staff looking to understand the characteristics of people who enrol in home-based PR rather than centre-based PR. This will allow healthcare providers and those developing home-based PR programmes to tailor their approach to those who are most likely to opt in who tend to be younger, female, and have a higher burden of respiratory symptoms and mental health comorbidities. Increasing referral rates from primary and secondary care may be a more effective measure to increase enrolment than simply diversifying the PR services offered.
Supplemental material
Supplemental Material - The characteristics of people with COPD who enrol in home-based pulmonary rehabilitation versus centre-based pulmonary rehabilitation: A nationwide cross-sectional study
Supplemental Material for The characteristics of people with COPD who enrol in home-based pulmonary rehabilitation versus centre-based pulmonary rehabilitation: A nationwide cross-sectional study by Alexander Adamson, Harley Kwok, Sally J. Singh, Tom M. A. Wilkinson, Holly Drover, Jennifer K. Quint in Chronic Respiratory Disease.
Footnotes
Acknowledgements
This work has been presented previously at the American Thoracic Society Conference 2025. 41 We thank the Healthcare Quality Improvement Partnership for commissioning the National Respiratory Audit Programme, National Respiratory Audit Programme team, and all of the staff in the centres and hospitals in England and Wales who tirelessly inputted the audit data.
Ethical considerations
The PR audit operates under Section 251 approval from the Confidentiality Advisory Group (CAG) of the Health Research Authority (HRA) (23/CAG/0167), meaning that individual patient consent is not required for this study. This work is covered under the HQIP overarching research CAG (24/CAG/0108) which includes research ethics approval (REC 24/YH/0175).
Consent to participate
Patient consent was not required for this study.
Author contributions
AA cleaned the data and ran the analyses for the study (including visualisations) and produced the first draft of the manuscript. AA, HK, SJS, TW, HD and JKQ made substantial contributions to the conception, investigation, and methodology, and took part in writing, reviewing, and editing of the manuscript. JKQ also led in the supervision of the project. All authors gave final approval of the version to be published and agreed to be accountable for all aspects of the work. The corresponding author attests that all listed authors meet the authorship criteria and that no others meeting the criteria have been omitted. AA is the guarantor. AA accepts full responsibility for the work and/or the conduct of the study, had access to the data, and controlled the decision to publish. Transparency: The lead author (the guarantor) affirms that the manuscript is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned (and, if relevant, registered) have been explained.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: AA and HK perform data analysis for NRAP. SS is the PR clinical lead for NRAP. TW is the senior clinical lead for NRAP and has received grants and consultancy fees from AZ, GSK, Janssen, Chiesi, Enanta, Ockham Biotech, Sanofi, Synairgen, Tidalsense and is a Founder and Director of my mhealth. HD is the Honorary PR Clinical Fellow for NRAP. JQ is the analysis lead for NRAP and has been supported by institutional research grants from UKRI, NIHR, Health Data Research UK, BI, AZ, Insmed, and received personal fees for advisory board participation, consultancy or speaking fees from GlaxoSmithKline, BI.
Data Availability Statement
Data may be obtained from a third party and are not publicly available. Data collected on behalf of Healthcare Quality Improvement Partnership (HQIP) by all National Clinical Audit and Patient Outcomes Programme (NCAPOP) projects are routinely reported at an aggregate level and these reports are available in the resources section of the HQIP website (https://www.hqip.org.uk/resources/). The reported data are also placed on the data.gov.uk website. The R scripts used to perform the analysis can be found at ![]() .
.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.