
Abstract
Obstructive sleep apnoea (OSA) is increasingly considered as a risk factor for metabolic disturbances, such as diabetes mellitus or dyslipidaemia. Continuous positive airway pressure (CPAP) therapy, the standard treatment for patients with OSA, may improve various metabolic variables, such as insulin sensitivity, glucose metabolism, lipids, fat distribution and adipokines. Several observational and uncontrolled clinical studies claim an improvement of these metabolic variables through the use of CPAP. However, there is only a limited number of clinical randomised controlled trials (RCTs) evaluating the effect of CPAP on metabolic variables. In this review, we summarise and discuss non-randomised studies and RCTs evaluating the effect of CPAP on metabolic variables in patients with OSA. In summary, the currently available body of evidence does not support a clinically important effect of CPAP treatment on any of the investigated metabolic variables. However, some investigators found small, but statistically significant changes in some metabolic variables, thus beneficial effects of CPAP treatment in selected patient cohorts cannot be excluded. To answer this question, more data from RCTs with well-defined study populations are warranted.
Keywords
Introduction
Obstructive sleep apnoea (OSA) is characterised by a repetitive collapse of the upper airways leading to apnoea and hypopnoea, which are associated with oxygen desaturations, intrathoracic pressure changes and arousals from sleep. It is thought that around 30% of the middle-aged male population in Western countries are affected by asymptomatic OSA. 1 Several epidemiological studies indicate that OSA is closely related to type 2 diabetes 2 and metabolic syndrome. 3 However, it is still a matter of debate, whether these conditions are linked causally, independent of obesity. 4
Application of nocturnal nasal continuous positive airway pressure (CPAP) is the gold standard of treatment for patients with OSA. The use of a CPAP device prevents apnoea, hypopnoea and snoring as well as other pathophysiological consequences of OSA by providing a positive pressure in the upper airways. It has been shown that CPAP improves quality of life and reduces daytime sleepiness as well as blood pressure in patients with moderate to severe OSA. 5 –7
Several observational and uncontrolled clinical studies claim an improvement of various metabolic variables through the use of CPAP. These variables include measures of insulin sensitivity, glucose metabolism, lipids, adipokines and fat distribution. However, there is only a limited number of clinical randomised controlled trials (RCTs) evaluating the effect of CPAP on metabolic variables. In this review, we summarise and discuss non-randomised studies and RCTs evaluating the effect of CPAP on metabolic variables in patients with OSA. We will focus on RCTs, as only these are able to clarify whether or not causal relationships have been established.
Methods
A literature search was performed using bibliographic databases (primarily Medline via PubMed) as well as hand-searching of eligible medical journals.
CPAP effects on insulin sensitivity and glucose metabolism
Non-randomised studies
Several non-randomised studies including diabetic and non-diabetic patients investigated the effect of CPAP treatment on insulin sensitivity, as measured by the insulin level, homeostasis model assessment-insulin resistance (HOMA-IR), short insulin tolerance test (SITT), insulin sensitivity index (ISI), quantitative insulin sensitive check index (QUICKI) or hyperinsulinaemic-euglycaemic clamp method.
Harsch et al. 8 reported a positive effect of CPAP treatment in 40 non-diabetic patients with OSA on ISI, as measured by the hyperinsulinaemic-euglycaemic clamp method, after 2 days and after 3 months of effective CPAP treatment. The same group investigated the effect of CPAP on insulin sensitivity in a sample of nine type 2 diabetics with OSA. 9 In the latter study, ISI as measured by the hyperinsulinaemic-euglycaemic clamp method was unchanged after 2 days of CPAP treatment, but significantly improved after 3 months of effective CPAP treatment. Dorkova et al. 10 found a reduced HOMA-IR in 16 patients with OSA using the CPAP device at least 4 h per night, but not in 15 patients with OSA using the CPAP device less than 4 h per night. In a study by Barcelo et al. 11 3 months of CPAP treatment reduced insulin and HOMA-IR in 20 OSA patients with excessive daytime sleepiness (EDS) but did not modify these variables in 15 OSA patients without EDS.
However, in a limited number of studies 12 –14 there have been no improvements in measures of insulin sensitivity. Carneiro et al. 12 found no positive effect of 3 months of CPAP treatment on ISI in 7 patients with severe OSA (apnoea hypopnoea index (AHI) > 30 events h−1). Trenell et al. 13 included 29 patients with severe OSA (respiratory disturbance index (RDI) ≥ 30 events h−1) in their study. No improvement after 12 weeks of CPAP therapy on HOMA-IR was reported. Garcia et al. 15 reported an unexpected increase in HOMA-IR and QUICKI in 23 patients with OSA (AHI ≥ 15 h−1) after 6 months of CPAP treatment. However, according to the authors, this was explained by an increase in body weight (p = 0.04) during the study period.
A few non-randomised studies have analysed the effect of CPAP treatment on measures of glucose metabolism. 16,17 In a study by Dawson et al., 16 4–13 weeks of CPAP treatment reduced mean sleeping glucose, but not glycated haemoglobin (HbA1c) in 20 type 2 diabetic patients with OSA. Shpirer et al. 17 reported that CPAP treatment for 3–5 months decreased HbA1c levels (from 6.47 (0.67) to 6.28% (0.51), p = 0.038) in 12 patients with severe OSA (AHI ≥ 30 h−1). The authors stated that there was no significant change in the patients’ lipid profile or their body mass index (BMI) during the study period.
Other authors were not able to show positive effects of CPAP treatment on HbA1c 9,18 and fasting glucose. 14,18 In a study by Myhill et al., 18 3 months of CPAP treatment had no effect on fasting glucose and HbA1c in 44 type 2 diabetic patients with OSA. Harsch et al. 9 also reported no effect of 3 months of CPAP therapy on HbA1c in 9 patients with OSA and type 2 diabetes.
The interpretation of these trials might be problematic due to the lack of a control group. West et al. 19 argued that measures of glycaemic control and insulin resistance could be influenced in subjects taking part in a study, regardless of the intervention, because of behavioural changes of subjects, when being monitored. Considering this aspect, they concluded that in an uncontrolled trial it would be impossible to attribute any changes in insulin resistance or glucose metabolism merely to the CPAP intervention.
RCTs
Currently, nine RCTs on the effects of CPAP treatment on insulin sensitivity and glucose metabolism have been published (Table 1).
CPAP effects on insulin sensitivity and glucose metabolism.

CPAP: continuous positive airway pressure; HbA1c: glycated haemoglobin; HOMA: homoeostasis model assessment for estimating insulin resistance; ISI: insulin sensitivity index; ISx: insulin sensitivity as measured by the minimal model analysis; SITT: short insulin tolerance test; KITT: insulin sensitivity estimated by SITT; M/I: euglycaemic clamp: quantity of glucose metabolised per unit of plasma insulin concentration (a measure of insulin sensitivity); OGTT: oral glucose tolerance test; QUICKI: quantitative insulin sensitive check index; RCT: randomised controlled trial; AHI: apnoea hypopnoea index; BMI: body mass index.
A total of 34 non-diabetic patients with OSA (AHI > 15 h−1) naive to CPAP were randomised in a crossover trial by Coughlin et al. 21 Six weeks of CPAP (mean compliance therapeutic and subtherapeutic CPAP: 3.9 and 2.6 h per night, respectively) had no statistically significant effect on fasting glucose, fasting insulin and HOMA-IR. The authors argued that, irrespective of the presence of OSA and its severity, there could be a threshold level of obesity where excess body fat is the principle determinant of insulin sensitivity.
West et al. 19 evaluated the effect of 3 months of therapeutic CPAP treatment versus subtherapeutic CPAP on metabolic variables in 42 type 2 diabetic patients with newly diagnosed OSA (oxygen desaturation index (ODI) > 10 events h−1). Therapeutic CPAP had no positive effect on fasting glucose, fasting insulin, HbA1c, euglycaemic clamp and HOMA-IR. Again, the mean compliance with therapeutic and subtherapeutic CPAP was rather low (3.6 (2.8) and 3.3 (3.0) h per night, respectively). However, the authors mentioned that also as per protocol analysis including only good compliers did not change their results.
Nguyen et al. 24 randomised 20 patients with newly diagnosed moderate to severe OSA (RDI ≥ 15 h−1) to therapeutic CPAP or subtherapeutic CPAP. None but one patient had previously been diagnosed with diabetes. No improvement in fasting glucose and 2 h fasting glucose of therapeutic CPAP versus subtherapeutic CPAP could be demonstrated. However, as the focus of this study was on cardiovascular imaging and markers of glucose metabolism were not declared as primary outcomes, no definite conclusions could be drawn.
Lam et al. 23 included 61 Chinese non-diabetic CPAP-naive patients with moderate to severe OSA (AHI ≥ 15 h−1) and a BMI of <35 kg m−2 in their study and investigated the effect of 1 week of CPAP treatment versus subtherapeutic CPAP on KITT, HOMA-IR, serum insulin and plasma glucose. After 1 week of CPAP treatment, insulin sensitivity increased as measured by KITT, but not when measured as HOMA-IR. Lam et al. 23 argued that this might be due to different metabolic aspects of insulin sensitivity covered by two different techniques (SITT and HOMA-IR, respectively).Those patients on therapeutic CPAP were evaluated again after 12 weeks. The positive effect on KITT only remained statistically significant in a subgroup of 20 overweight patients (BMI ≥ 25 kg m−2), but not in patients with a BMI <25 kg m−2.
In a randomised controlled crossover trial, Weinstock and et al. 27 investigated the impact of 8 weeks of CPAP treatment compared with subtherapeutic CPAP on various measures of glucose metabolism and insulin sensitivity in 50 subjects with moderate to severe OSA (AHI > 15 h−1) and impaired glucose tolerance. Across the entire sample, therapeutic CPAP did not lead to a significant improvement in fasting glucose, oral glucose tolerance test (OGTT) 2-h glucose, fasting insulin, OGTT 2-h insulin, ISI, HbA1c, HOMA-IR or HOMA-B (a measurement used to assess pancreatic β-cell function), when compared with subtherapeutic CPAP. Yet among the most severely affected subjects with an AHI ≥ 30 (n = 25), there were statistically significant improvements in ISI and 2-h insulin level after therapeutic CPAP compared with subtherapeutic CPAP.
In an RCT by Kohler et al., 7 41 obese patients with OSA (ODI > 10 h−1) and established CPAP therapy were included to investigate the effects of 14 days of CPAP treatment withdrawal on HOMA-IR, glucose and insulin. Although CPAP withdrawal was associated with a rapid recurrence of OSA leading to clear physiological effects on blood pressure and vascular function, no significant effects on glucose metabolism and insulin sensitivity were observed. Whether 2 weeks of CPAP withdrawal is long enough to evaluate effects on glucose metabolism, however, is questionable. Contrary to the aforementioned study, this trial did not specifically include patients with abnormal glucose metabolism and this could be a possible methodological explanation for the negative finding.
Hoyos et al. 22 randomised 65 non-diabetic CPAP-naive male patients with moderate to severe OSA (AHI ≥ 20 h−1, ODI > 15 h−1) to either 12 weeks of therapeutic CPAP or subtherapeutic CPAP to evaluate the effect on insulin sensitivity as measured by the minimal model analysis (ISx), HOMA-IR, QUICKI, fasting glucose and fasting insulin. No improvement after therapeutic CPAP on any of these measures compared with subtherapeutic CPAP could be demonstrated.
In a randomised controlled crossover trial by Sivam et al., 26 which included 27 mostly male OSA patients (AHI ≥ 25 h−1, ODI ≥ 20 h−1) with a BMI ≤ 35 kg m−2, 8 weeks of therapeutic CPAP had no effect on fasting glucose when compared with subtherapeutic CPAP.
In a small study by Comondore et al., 20 13 minimally symptomatic patients with suspected OSA (AHI > 15 h−1) were randomised to either CPAP treatment or no therapy for 4 weeks followed by a washout period of 4 weeks and then a crossover to the other intervention. Compared with no therapy, CPAP therapy had no statistically significant effect on fasting glucose, insulin, HbA1c and HOMA-IR.
Sharma et al. 25 conducted a randomised controlled crossover trial. However, the trial was retracted from The New England Journal of Medicine (Table 1).
Conclusion
Among the described RCTs, there are considerable differences regarding methodological aspects. Some studies included only non-diabetic patients, others only diabetics. One trial specifically included patients with impaired glucose tolerance, but not patients with overt diabetes. 27 Based on the existing data, it could be hypothesized that treatment effects of CPAP are too small to positively influence insulin sensitivity in patients with established diabetes and that a CPAP effect on insulin sensitivity is more likely in non-diabetic patients with severe OSA, if at all.
To what extent obesity drives changes in insulin sensitivity in patients with OSA is still a matter of debate. Harsch et al. 8 argued that CPAP treatment effects on insulin sensitivity would be more pronounced in less obese patients. Coughlin et al. 21 postulated that there could be a threshold level of obesity where excess body fat is the principal determinant of insulin sensitivity irrespective of the presence of OSA or its severity. This issue was conversely discussed by Lam et al. 23 who found that in an Asian OSA population improvements in insulin sensitivity after 12 weeks of CPAP treatment only remained significant in an overweight subgroup (BMI between 25 and 30.3 kg m−2), but not in a subgroup with BMI’s lower than 25 kg m−2. Hoyos et al. 22 mentioned that visceral adiposity, rather than overall adiposity, should be taken into account when measuring treatment effects of CPAP on metabolic variables. Concerning glucose metabolism, a reduction of HbA1c should not be expected after a few weeks of CPAP therapy, considering the lifespan of erythrocytes. Another reason for the differing results could have been due to ethnic differences among the study populations. It is further conceivable that the different methods used to assess insulin sensitivity and glucose metabolism play a major role in interpreting the results. No study, however, found an improvement of CPAP treatment compared with subtherapeutic CPAP on HOMA-IR or the euglycaemic clamp, which is considered the gold standard for assessing insulin resistance. 28,29
So far, there is no compelling evidence that CPAP treatment, independently from weight reduction, is able to improve insulin sensitivity and markers of glucose metabolism to a clinically significant extent.
CPAP effects on lipids
Non-randomised studies
In a number of non-randomised studies, the effect of CPAP treatment on serum lipids (total cholesterol, low-density lipoprotein cholesterol (LDL), very low-density lipoprotein cholesterol (VLDL), high-density lipoprotein cholesterol (HDL), triglycerides, apolipoprotein A (ApoA) and apolipoprotein B (ApoB)) has been investigated.
In a study by Barcelo et al., 11 total cholesterol was significantly reduced after 3 months of CPAP treatment in a subgroup of 20 OSA patients with EDS (Epworth sleepiness scale (ESS) > 10 and multiple sleep latency test (MSLT) < 5 min.), but not in 15 OSA patients without EDS (ESS < 10 and MSLT > 10 min.). Triglycerides and HDL were unaffected after 3 months of CPAP therapy.
Cuhadaroğlu et al. 30 found a significant reduction of total cholesterol and LDL in 31 patients with moderate to severe OSA (AHI > 15 h−1), who had been compliant users of CPAP therapy (> 4 h per night) for 8 weeks. Total cholesterol and ApoB were significantly reduced (HDL, LDL and Apo A were not reduced) in a trial by Dorkova et al. 10 after 8 weeks of CPAP treatment in 16 patients with severe OSA (AHI ≥ 30 h−1) and metabolic syndrome, who had been compliant users of a CPAP device for 8 weeks. No changes were reported in 16 patients, who used CPAP less than 4 h per night. 10
In line with the aforementioned studies, Steiropoulos et al. 31 detected a fall in total cholesterol, as well as in total cholesterol/HDL-ratio and ApoB/ApoA-ratio, again only in the more compliant patients (CPAP use > 4 h per night) with OSA, after 6 months of CPAP treatment. Triglycerides, HDL, LDL, ApoA and ApoB were unchanged in good compliers as well as in patients with poor compliance.
Kawano et al. 32 investigated the effect of 6 months of CPAP therapy on the LDL/HDL-ratio of 30 patients with OSA. In these patients, LDL/HDL-ratio was reduced whereas it was unchanged in 11 age- and sex-matched control patients with OSA, in whom CPAP therapy could not be established. Both groups showed no changes in LDL, HDL or triglycerides.
No treatment effect of a 3-months CPAP study on total cholesterol, LDL, HDL or triglycerides was reported by Myhill et al. 18 in 44 type 2 diabetic patients with OSA (AHI > 15 h−1).
Trenell et al. 13 also did not find a treatment effect of 12 weeks of effective CPAP in 29 patients with severe OSA (RDI ≥ 30 h−1) on total cholesterol, trigylcerides or HDL. There were no differences regarding measures of serum lipids between good compliers to CPAP treatment (≥ 4 h per night; n = 19) and poor compliers (≤ 4 h per night; n = 10).
Conclusion
Several authors 10,11,30,31 reported a statistically significant fall in total cholesterol following the use of CPAP in patients with OSA. This effect seemed to be more pronounced in the more severely affected OSA patients and in patients using their CPAP device more than 4 h per night. Possibly, the greater effect seen in more severe OSA is due to a higher level of sympathetic activation and arousals from sleep before normalisation of nocturnal breathing by CPAP. However, other authors 13,18 did not show a positive effect of CPAP treatment on total cholesterol. Concerning other measures of serum lipids, the described studies showed fairly inconsistent results.
RCTs
Six RCTs on CPAP treatment effects on lipids have been published to date (Table 2).
CPAP effects on lipids.

CPAP: continuous positive airway pressure; FFA: free fatty acids; HDL: high-density lipoprotein; LDL: low-density lipoprotein; RCT: randomised controlled trial; BMI: body mass index.
In a randomised crossover trial by Comondore et al., 20 13 patients with minimal daytime sleepiness with OSA and an AHI > 15 events h−1 were randomised to either CPAP or no therapy for 4 weeks followed by a washout of 4 weeks, and then crossed over to the other group. Cholesterol, HDL and LDL were unchanged, whereas triglycerides tended to fall by 0.52 mmol L−1 (not statistically significant). The authors did not offer information on lipid lowering drugs or changes of diet and weight.
Coughlin et al. 21 included 34 drug-free OSA patients in a sham-placebo-controlled crossover trial on the effect of CPAP treatment on various cardiovascular markers. CPAP led to a non-significant fall in cholesterol by 0.2 mmol L−1. HDL, LDL and triglycerides were unchanged, irrespective of the patient’s compliance to treatment. There were also no statistically significant differences of weight, BMI, body fat and fat distribution at follow-up between the treatment limbs.
Robinson et al. 34 analysed data of two RCTs, including 213 patients with OSA (ODI > 10 h−1; ESS > 9). There is no information given on lipid-lowering medication. Cholesterol and triglycerides were measured before and after 1 month of therapeutic versus subtherapeutic CPAP therapy. Receiving therapeutic CPAP was associated with a significant reduction in cholesterol of 0.28 mmol L−1. When compared with subtherapeutic CPAP though, the reduction did not quite remain statistically significant (p = 0.06). There was no statistically significant difference of weight change between the two groups. Due to the study’s exploratory analysis approach, the findings are hypothesis generating and not definitive proof of a causal relationship between OSA and dyslipidemia.
Kohler et al. 7 used an alternative approach to investigate the effect of CPAP treatment on cardiovascular markers, by withdrawing an established CPAP therapy for 2 weeks in 21 highly compliant patients with OSA, while the control group (n = 20) remained on therapeutic CPAP. No significant difference in change of total cholesterol was observed between the two groups. Interestingly, there was a small but statistically significant fall in triglycerides (0.2 mmol L−1) in the group receiving subtherapeutic CPAP (no information about changes in diet and weight). The rate of subjects on cholesterol-lowering medication did not differ statistically significant between the two groups (35 and 33.3%, respectively). Whether 2 weeks of CPAP withdrawal is long enough to evaluate effects on lipids however is questionable.
Nguyen et al. 24 randomised 20 patients with newly diagnosed moderate to severe OSA (RDI ≥ 15 h−1) to therapeutic CPAP or subtherapeutic CPAP. Cholesterol/HDL, HDL, LDL and triglycerides were unchanged after 3 months of therapeutic CPAP treatment compared with subtherapeutic CPAP (no information on lipid-lowering medication or changes of diet and weight).
Contrary to the aforementioned studies, a more recently published trial 33 reported on reduced markers of serum lipids after therapeutic CPAP treatment when compared with subtherapeutic CPAP. Phillips et al. 33 randomised 29 patients (7/29 on statin medication) with moderate to severe OSA (AHI ≥ 25 h−1) to either 2 months of therapeutic CPAP treatment or 2 months of subtherapeutic CPAP. Postprandial lipidemia was determined by taking seven blood samples during wake and sleep periods. By doing so, the area under the 24-h triglyceride concentration curve could be calculated. In both groups, triglycerides peaked at 02:00 p.m. and 03:00 a.m; both peaks were significantly lower in the group receiving therapeutic CPAP as compared to the subtherapeutic CPAP group. Furthermore, total cholesterol (−0.19 mmol/L), HDL (−0.03 mmol/L) and non-HDL cholesterol (−0.16 mmol/L) fell statistically significant after therapeutic CPAP compared with subtherapeutic CPAP, again calculated as means of 7 blood samples during 24 h. No information on changes of diet and weight has been offered by the authors.
Sharma et al. 25 conducted a randomised controlled crossover trial. However, the trial was retracted from The New England Journal of Medicine (Table 2).
Conclusion
If effective CPAP treatment led to a significant reduction of total cholesterol, this would be an important finding. However, of the six currently published RCTs on the effect of CPAP treatment on lipids, only one 33 found significant reductions in total cholesterol and triglycerides, when compared to patients randomised to subtherapeutic CPAP treatment. Concerning laboratory tests, the published trials differed considerably. Phillips et al. 33 calculated means of 7 blood samples during 24 h, whereas the other authors used standard fasting lipid tests. Concerning the use of lipid-lowering medication, the described patient samples were heterogeneous. This might play an important role when comparing results as the effect of CPAP treatment on total cholesterol seems to be fairly small and would be easily attained by the use of statin medication. Since the currently available RCT data show inconsistent findings regarding the effect of CPAP on lipid metabolism, no definite conclusion can be drawn. To clarify the actual impact of CPAP on total cholesterol and other lipids, large RCTs with carefully selected patients are warranted.
CPAP effects on adipokines
Adiponectin, an adipocyte-derived bioactive substance (adipocytokine) has anti-diabetic, anti-atherosclerotic and anti-inflammatory properties. 35 Reduced plasma levels have been related to insulin resistance and coronary heart disease. 36
A deficiency of leptin, a protein hormone secreted by adipose tissue, has been linked to morbid obesity and diabetes whereas its replacement seems to lead to decreased food intake, normalised glucose homeostasis and increased energy expenditure. 37
Non-randomised studies
Some authors 12,38 reported on reduced levels of plasma adiponectin in obese patients with OSA compared with obese persons without OSA. Moreover, they observed that CPAP treatment was able to reverse the reduction of adiponectin, independent from the degree of obesity or from changes in insulin resistance.
Several authors 13 –15,39 did not find significant changes in plasma levels of adiponectin after effective use of CPAP in patients with OSA. It has been argued that the lack of a sustained effect of CPAP treatment on adiponectin levels might be explained by the overwhelming effect of obesity on adiponectin secretion. 39
In a couple of non-randomised studies, 10,15,40 plasma levels of leptin remained unchanged after CPAP treatment compared with no CPAP treatment in patients with OSA. Other investigators 13,30 reported significant falls in plasma leptin levels in OSA patients using their CPAP devices for at least 4 h per night. In another study by Harsch et al., 41 leptin levels were significantly decreased after 8 weeks of CPAP treatment in patient with OSA, whereas BMI remained unchanged. Furthermore, this effect seemed to be more pronounced in patients with a BMI <30 kg m−2.
RCTs
Up to date, three RCTs on the effect of CPAP treatment on levels of adiponectin in patients with OSA have been published (Table 3).
CPAP effects on adipokines.

CPAP: continuous positive airway pressure; RCT: randomised controlled trial; BMI: body mass index.
West et al. 19 included 42 type 2 diabetic patients with newly diagnosed OSA (ODI > 10 h−1) in their RCT. Three months of therapeutic CPAP had no effect on adiponectin levels, when compared with 3 months of subtherapeutic CPAP.
In a large RCT by Kohler et al., 42 100 men with moderate to severe OSA (ESS ≥ 10 h−1; ODI > 10 h−1) were randomly assigned to either receiving therapeutic CPAP (n = 51) or subtherapeutic CPAP (n = 49). Four weeks of therapeutic CPAP had no effect on plasma levels of adiponectin when compared with subtherapeutic CPAP.
In line with these two trials, Hoyos et al. 22 found no effect of 12 weeks of therapeutic CPAP treatment on plasma levels of adiponectin or leptin in 34 non-diabetic, CPAP-naive male patients with moderate to severe OSA (AHI ≥ 20 h−1, ODI > 15 h−1), when compared with 31 patients receiving subtherapeutic CPAP treatment. The study by Hoyos et al. has so far been the only RCT investigating the effect of CPAP on plasma levels of leptin.
Conclusion
The existing data from RCTs do not support an effect of CPAP treatment on plasma levels of adiponectin or leptin. Some investigators 39,42 argued that levels of adiponectin might be overwhelmingly driven by the BMI and that especially in very obese patients with OSA one could not expect a significant change in adiponectin through the short-term use of CPAP.
CPAP effects on fat distribution
Currently, there is fairly heterogeneous data on a proposed effect of CPAP therapy on abdominal fat distribution and on changes in liver fat deposits in patients with OSA, as assessed either by computed tomography (CT) or by magnetic resonance imaging (MRI).
Non-randomised studies
In the studies by Chin et al. 43 and by Trenell et al., 13 CPAP treatment (6 months and 12 weeks, respectively) led to a significant reduction of visceral adipose fat (VAF), while subcutaneous abdominal fat (SAF) remained unchanged in both trials.
In contrast, Vgontzas et al. 14 and Lam et al. 23 reported that 3 months of CPAP therapy did not affect the amount of either VAF or SAF.
RCTs
Currently, three RCTs have been published investigating the effect of therapeutic CPAP versus subtherapeutic CPAP on abdominal fat distribution in patients with OSA (Table 4).
CPAP effects on fat distribution.
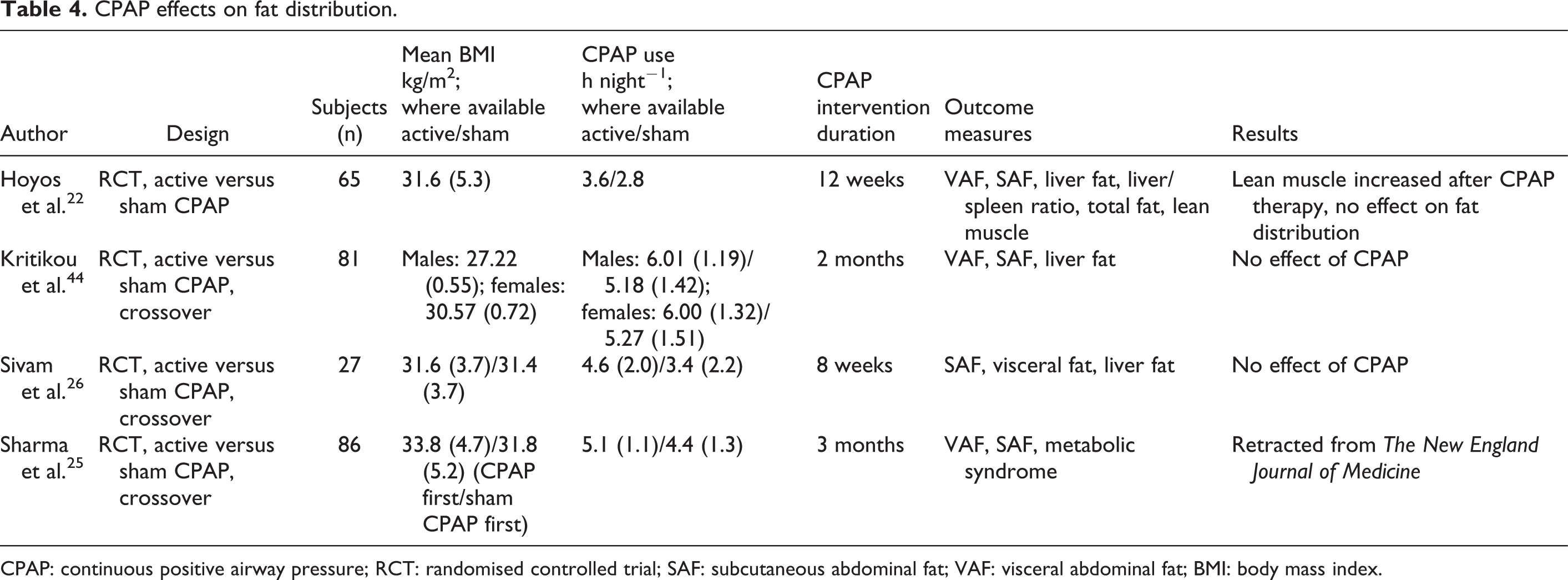
CPAP: continuous positive airway pressure; RCT: randomised controlled trial; SAF: subcutaneous abdominal fat; VAF: visceral abdominal fat; BMI: body mass index.
Hoyos et al. 22 randomised 65 CPAP-naive male patients with moderate to severe OSA (AHI ≥ 20 h−1, ODI > 15 h−1) to receive either therapeutic (n = 34) or subtherapeutic (n = 31) CPAP for 12 weeks. No changes in VAF and SAF were detected as assessed by CT scans. Amounts of liver fat, total fat and total lean muscle mass also remained unchanged after 12 weeks of therapeutic CPAP compared with subtherapeutic CPAP.
Kritikou et al. 44 studied 42 patients with OSA (females AHI > 10 h−1; males AHI > 15 h−1) and reported that there was no effect after 2 months of therapeutic CPAP on VAF, SAF and liver fat when compared with 2 months of subtherapeutic CPAP treatment, as assessed by CT.
In a randomised controlled crossover trial by Sivam et al., 26 VAF, SAF and liver fat were quantified using MRI and magnetic resonance spectroscopy in 27 OSA patients (AHI ≥ 25 h−1, ODI ≥ 20 h−1) receiving both therapeutic and subtherapeutic CPAP treatment for 2 months with an intervening washout period of 1 month. No significant differences in changes of VAF, SAF or liver fat were detected.
Sharma et al. 25 published a randomised controlled crossover trial. However, the trial was retracted from The New England Journal of Medicine (Table 4).
Conclusion
The implementation of a control group is crucial when interpreting effects of CPAP treatment on metabolic variables. It is conceivable that in patients with OSA changes in body weight and various measures of fat distribution may be the result of lifestyle changes linked to taking part in a clinical trial. Thus, in such RCTs, subjects should be instructed to not change diet or physical activity. However, in a RCT looking at the effects of 3 months of CPAP treatment there was no change in daily physical activity in patients with OSA and diabetes mellitus treated with CPAP. 45 Of the three RCTs on the effect of therapeutic CPAP versus subtherapeutic CPAP on abdominal fat distribution, none detected statistically significant changes. 22,26,44 It seems that CPAP therapy will not reduce visceral adiposity to a clinically important extent, without additional weight-loss interventions. 22
Summary and clinical implications
Numerous clinical trials investigated the effect of CPAP therapy on various metabolic variables. However, only a limited number of RCTs are available, and these studies often included heterogeneous patient populations making direct comparisons between the studies difficult. In conclusion, the currently available body of evidence does not support a clinically important effect of CPAP treatment in patients with OSA on any of the metabolic variables discussed in this review. However, some investigators found small, but statistically significant changes in some metabolic variables, thus beneficial effects of CPAP treatment in selected patient cohorts cannot be excluded. To answer this question, more data from RCTs with well-defined study populations are warranted.
Footnotes
Conflict of interest
The authors declared no conflicts of interest.
Funding
The present work was financially supported by Swiss National Science Foundation (32003B_143365/1).