
Abstract
Background
While telehealth has been used for specialist care during the COVID-19 pandemic, its benefits and barriers to use for delivering care in interstitial lung disease (ILD) remain unclear. We aimed to explore perspectives of patients and healthcare professionals (HCPs) towards telehealth use in ILD.
Method
This qualitative study using semi-structured interviews was undertaken in 18 patients with ILD from a single quaternary ILD centre and 18 HCPs of four different disciplines from various ILD centres around Australia. Interviews were transcribed verbatim and coded by two investigators independently using thematic analysis. Themes were developed by consensus.
Results
Patients and HCPs had experienced telehealth via video and telephone, predominantly for teleconsultation and/or telerehabilitation. For patients, benefits included provision of ongoing access to healthcare and significant reduction in travel. Healthcare professionals reported teleconsultations played an important role in patient follow-up rather than at initial contact. Concerns of suboptimal rapport and communication and a lack of physical examination were raised by both groups. Individual patient suitability, improvement in technological platform and support, and improved workflow for clinicians were important factors for utilisation of telehealth. Patients were open to the use of home monitoring devices, however, HCPs felt further research was required prior to clinical implementation.
Conclusion
This study highlights positive and negative experiences of telehealth for patients and HCPs in the management of ILD . It also identifies areas for improvement to create a tailored telehealth model for ILD care.
Keywords
Introduction
Interstitial lung diseases (ILDs) are a heterogeneous group of lung conditions with varying aetiologies and high morbidity and mortality. The management of ILD is frequently complex, requiring a multidisciplinary approach. ILD specialist care allows early accurate diagnosis, appropriate initiation of interventions, disease monitoring and timely lung transplantation referral, leading to improved outcomes and survival.1–3 However, barriers such as travel distance and geographical inequity, as well as assessment frequency, pose challenges to patients and their caregivers. 4
Telehealth is an emerging modality of healthcare provision, which has been rapidly adopted during the COVID-19 pandemic. Defined by the WHO as the provision of healthcare services at a distance using information and communication technologies, telehealth includes teleconsultation, telerehabilitation, remote monitoring, and tele-education.
5
Despite its growing use, evidence supporting telehealth in the management of
There is also growing interest in the use of remote monitoring technologies in the care of patients with respiratory conditions. Various devices are available for remote monitoring of disease manifestations and physiological parameters in ILD. Forced vital capacity, a well-established marker of ILD disease progression, 8 can be measured using a home spirometer although results are consistently lower with wider variability.9–12 Pulse oximeters, activity trackers and cough monitoring devices are available and easy to use. However, there is limited evidence on their utility and accuracy for remote monitoring in ILD.13–15 Given this field is rapidly growing with potential for improve patient care, the American Thoracic Society (ATS) has issued a framework to guide the evaluation and implementation of such devices, which includes domains for patient and clinician experiences. 16
While telehealth has been used for ILD specialist care during the COVID-19 pandemic and in small patient cohorts or research settings,17–19 little is known about its benefits and barriers for wider implementation. At our health service, teleconsultation via browser-based teleconferencing or telephone, as well as telerehabilitation have been the primary forms of telehealth integrated into ILD care since the pandemic, however stakeholder experiences remained unknown. This study aimed to explore patient and healthcare professional (HCP) perspectives on telehealth use for ILD specialist care to inform the development of future refined models of ILD care.
Method
Study design and participants
A qualitative study using semi-structured interviews was conducted between June 2022 and February 2023. This study was approved by the Alfred Health Human Research Ethics Committee (196/22).
Adults aged ≥18 years with a multidisciplinary diagnosis of ILD were recruited from the ILD specialist service at Alfred Health, a quaternary centre in Victoria, Australia. Patients were approached while attending clinic appointments or via telephone by an investigator (SD), who provided verbal and subsequent written study information via email or mail about the background and aim, procedure, and potential outputs of the study. The recruitment was purposive to capture participants with differing age, sex, ILD diagnosis, disease severity, and travel distance from the centre. Geographical proximity was classified as urban (major cities), regional (both inner and outer), and remote areas. 20 Healthcare professionals from various disciplines involved in ILD specialist care were recruited from different ILD centres across Australia through a nationwide electronic newsletter distributed by the Thoracic Society of Australia and New Zealand. Patients and HCPs were eligible irrespective of prior telehealth use. Participants who were unable to communicate in English or with cognitive impairment were excluded.
Semi-structured interviews
Interview guide.

aNo modification to the interview guide was required during the data collection/analysis process.
Data analysis
The transcripts were analysed independently by two investigators (SD and YHK) using reflexive thematic analysis. 21 Each investigator individually read the transcripts line by line to form descriptive codes to represent the data (open coding) and then grouped the codes to form themes. The investigators then came to a consensus on final themes through iterative discussion. Analysis occurred simultaneously with the interview process to inform future interviews and determine data saturation. Recruitment continued until no new themes emerged in each group. Patient demographic and clinical data was extracted from medical records.
Results
Patient characteristics.

Abbreviations: CPFE, combined pulmonary fibrosis and emphysema; CTD-ILD, connective tissue disease-associated interstitial lung disease; F, female; HP, hypersensitivity pneumonitis; IPF, idiopathic pulmonary fibrosis; IPAF, interstitial pneumonia with autoimmune features; M, male; NA, not available.
Healthcare professional characteristics.

Abbreviations: F, female; M, male; NSW, New South Wales; QLD, Queensland; SA, South Australia, VIC, Victoria; WA, Western Australia.
Major themes.
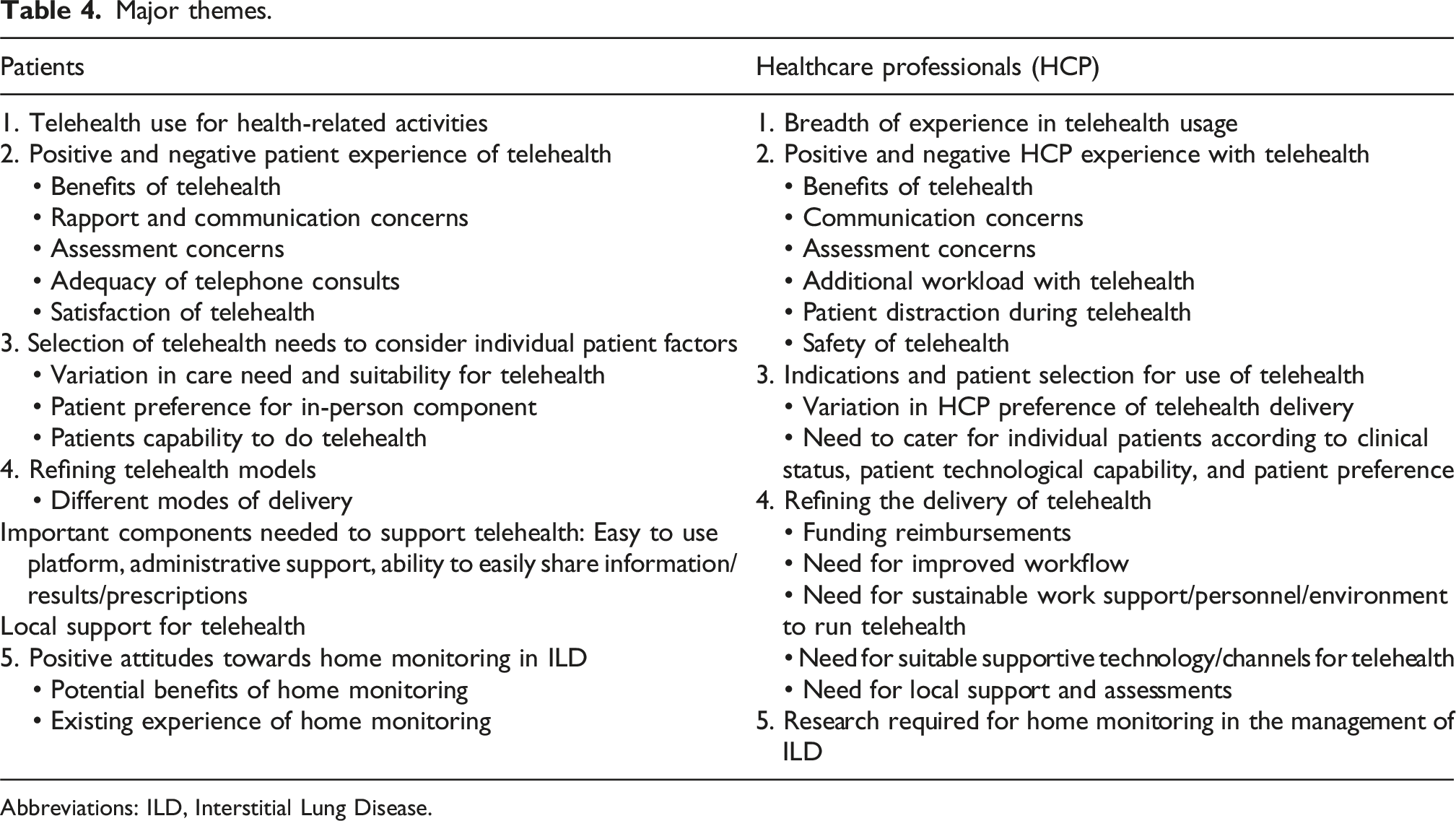
Abbreviations: ILD, Interstitial Lung Disease.
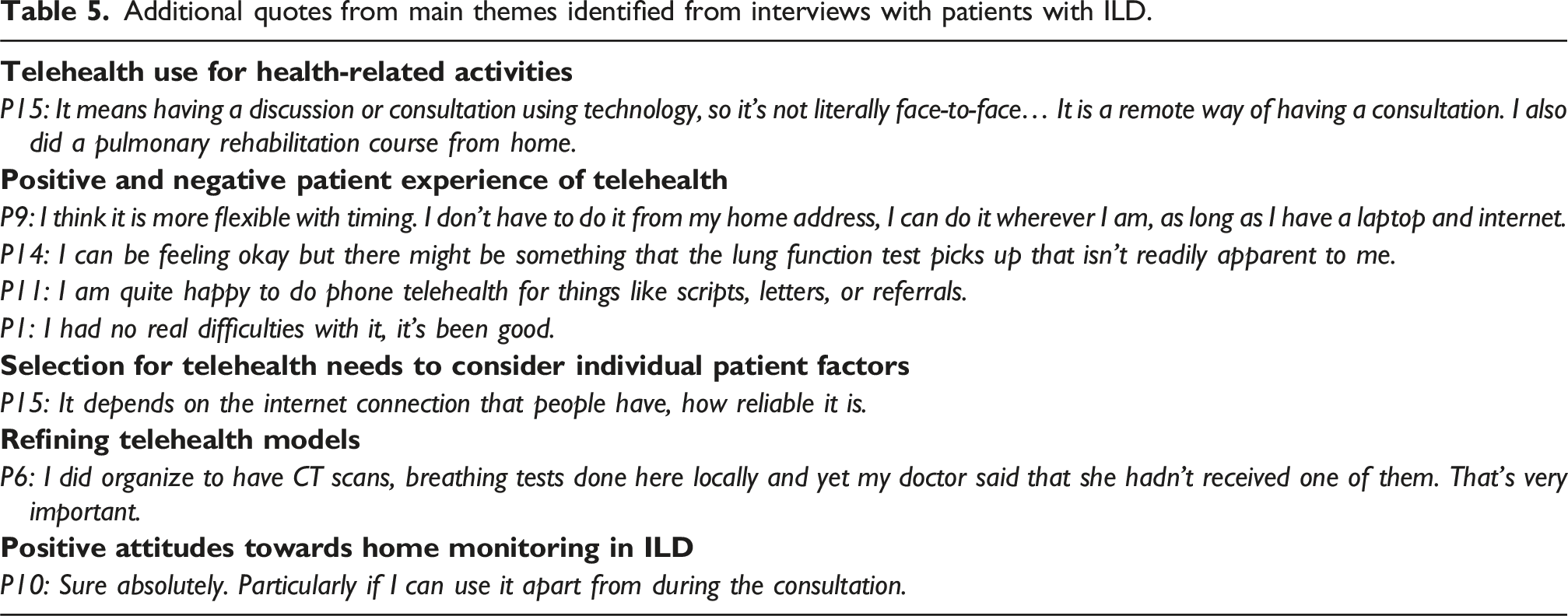
Additional quotes from main themes identified from interviews with patients with ILD.
Additional quotes from main themes identified from interviews with healthcare professionals.

Major themes for patients with ILD on the use of telehealth
Telehealth use for health-related activities
All patients reported telehealth use predominantly for teleconsultation with their specialists or general practitioners, with only a few having participated in telerehabilitation. Patients’ experience of telehealth was predominantly via telephone and/or video. Whilst patients had a good understanding of what teleconsultation entailed, their knowledge of other applications of telehealth was limited. P4: It involves a consultation with a medical practitioner the same as I would if I was going to see a doctor for the purpose of diagnosis, for the purpose of attending to my health… I think for me it’s any medical thing that I need, the only difference is that it is through the phone or video link.
Positive and negative patient experience of telehealth
Patients acknowledged the advantages of telehealth for continuity of care through the COVID-19 pandemic. Beyond the pandemic, telehealth was reported as being convenient and reduced travel time and cost, particularly for those living further away from an ILD centre. P1: Through COVID we were able to continue our appointments without the stress of having to get in and out of hospital, so it was a great help there. P2: We live in the country, getting to the appointments is a 4-hour drive. So, it is a lot more convenient with telehealth. Without having to travel, it saves you a lot more stress and expense.
However, suboptimal rapport and communication with telehealth was a concern, with patients perceiving a more personal connection and better communication with their specialist when seen in-person. Additionally, performing lung function and having a physician listen to their lungs provided more confidence in the assessment of their condition. P5: I don’t think you can get an accurate assessment just by talking to someone over the phone... If your doctor doesn’t see you, I can’t see how they can tell if you are getting better or not. Apart from what you tell them. P12: 100% they are compromised. You develop rapport when you have a one-on-one consultation, you haven’t got that when you talk to someone on the phone or look at them on a computer screen.
Patients expressed that the preferred delivery mode of teleconsultations would depend on the consulting purpose. Telephone was felt to be adequate for simple consultations e.g. when requiring a medication prescription, but the video component was helpful with visual cues for assessment and discussion. P7: I think contact with people really does help to gauge communication between two people, so I certainly say that the video has been good. The phone telehealth, I don’t have anything bad to say about it, I just don’t think it is as good. P9: I think video telehealth is almost as good as sitting there talking to someone.
Patients generally found telehealth via phone or video conference was easy to use, with very few expressing technological difficulties. Previous use of telecommunication technology for keeping in touch with family aided their use of similar technologies for telehealth. P16: I was apprehensive at first about it (video telehealth) because I thought gosh I might go in and muck this up but no, it is very helpful and very simple to follow.
Selection for telehealth needs to consider individual patient factors
All patients felt that the use of telehealth needed to take various individual factors into consideration, including disease stage and stability, patient preference, and patient capability to participate in telehealth such as technological knowledge and availability. While most patients were comfortable with using telehealth, all expressed a preference for in-person review to allow for comprehensive assessment including examination, and better interaction with their HCPs, particularly during deterioration of health status. P1: If it deteriorates over time, I wouldn’t be comfortable not having been assessed in-person… But telehealth can be a supportive role. P4: At the moment I think that I am still reviewing medication. Once I am stable, I am happy to do a mix of telehealth and face-to-face appointments. P9: I am probably fortunate that I have used computers with work. I am not advocating that I am the most proficient user of technology, but I am not afraid of it and I sort of know how to get around it. I can imagine there are a lot of people out there in my position that don’t have the ability.
Refining telehealth models
Many patients were open to a mix of telehealth and in-person care, but felt these needed to be supported by local access to investigations such as lung function tests and imaging. P17: If it was possible to alternate the appointments, one face-to-face and one video perhaps with the added lung function test being done (locally), so that then we do know how I am going, how I am progressing, yes, I think that could work.
Other important components needed to support telehealth included an easy-to-use platform, administrative support for addressing difficulties, and the capacity for real-time information sharing between patients and HCPs as well as between members of the treating team in between telehealth sessions. P1: In my case the easier telehealth is to use the better. P15: If you wanted to show me some results of a test, say lung function tests, you do a screen share… you can actually show people x-ray images; well images of anything for that matter.
Positive attitudes towards home monitoring in ILD
Most patients were very open to using home monitoring devices if that would help with disease monitoring. A few patients owned oximeters, while others used mobile applications to monitor step count. Most patients were unaware of the possibility of home spirometry. P1: I think it’d be helpful to get a better understanding of where your health condition is at. P13: I purchased an oximeter from my chemist so I am able to check myself and when I am feeling that I am a little bit low on energy.
Major themes for healthcare professionals on the use of telehealth in ILD care
Breadth of experience in telehealth usage
Healthcare professionals were familiar with the various applications of telehealth, including teleconsultation, telerehabilitation, multidisciplinary meetings (MDMs), telemonitoring and tele-education. However, the majority had experience only in teleconsultations, telerehabilitation or MDMs. HCP1: It means that any part of patient care that you deliver monitoring at a distance. So could be related to consultation of patients, monitoring of patient, discussion with other healthcare professionals that are involved in management of the patient. HCP18: Telehealth is care provided predominantly through video link or also via telephone, and then also use of digital technology to allow remote access to services such as the multidisciplinary meeting.
Positive and negative HCP experience with telehealth
Major benefits of telehealth identified by HCPs were convenience to patients and increased access to ILD specialist care. This was felt to be particularly important for patients living in regional or rural areas, allowing specialist involvement without the burden of travel. HCP16: It does increase that access and means that patients who are unable to travel in, can still access medical support.
Healthcare professionals, especially physicians, raised concerns with the use of telehealth in regard to effective communication and patient assessment. Use of telephone was challenging for building rapport with the patient and made physical assessment difficult. Video telehealth helped with personal connection and some visual assessment, however, did not permit physical examination which was felt to be important, especially for initial assessments. HCP2: It’s a lack of that visual connection and not being able to share screens and show the patient what you usually show, you know delivering often bad news to a patient in a telephone call can make rapport and empathy very hard to establish. HCP13: Relationship, rapport, still some cues are difficult to pick up on video especially if the reception is poor that can interfere quite a bit. The examination, lung function, meeting family members helps with difficult consultations, lots of factors there which require face-to-face or are better with face-to-face.
Healthcare professionals perceived increased workload with telehealth, which required extra time to complete tasks such as arranging tests locally or posting medication prescriptions and patient information. HCP3: As a nurse, it does create a lot more work having to send out things after the discussion with the doctor, and I don’t know how much a lot of smaller services who don’t have that support have managed. HCP7: It creates a lot of chasing up of investigations from elsewhere where previously people would just be having their investigations here and you would be able to access it easily.
Some physicians also found patients could be distracted during teleconsultations, which compromised the quality of the interaction. However, telehealth was felt to be safe from a privacy perspective. HCP2: There are problems with patients not setting themselves up in a manner to get the most out of the consultation. They may be driving or dealing with children, it is something that is squeezed in in their lives.
Indications and patient selection for use of telehealth
Most HCPs felt the initial contact with a patient should be in-person to allow a comprehensive assessment including a physical examination to be undertaken. This was critical in achieving a more accurate diagnosis and in making treatment decisions. Telehealth was thought to be more appropriate for subsequent appointments and monitoring once a patient’s baseline and the clinician-patient relationship had been established. HCP6: You can build a better rapport with the video. You can look at the patient, you can look at their hands. But I do think there should be an option to call the patient, it should be clinician discretion to call the patient. HCP12: I find that telehealth worked very well when I was seeing follow up patients that I had already met and been through the process to work out the cause of their disease.
It was widely felt that patient selection for telehealth was important, considering clinical factors (including disease complexity and trajectory, age, comorbidities, frailty, and treatment aims), patient preference and patient’s technological skills. Face-to-face contacts were perceived to be important for patients with complex disease process and treatment regimens, and declining health status. HCP8: I think the complexity of their illness, where they live, how tech savvy they are, I guess what is to lose as well is if someone is in their very end stage and palliative, I am more likely to do a telephone consult because also there is less risk involved if we miss something. HCP11: Many patients don’t have the capacity to do that and particularly in the older patient population struggle with those sorts of interactions. I had a patient who lived quite remotely who didn’t have great internet signal and we couldn’t use the video function.
Refining the delivery of telehealth
Suggestions to improve the delivery of ILD care by telehealth included having dedicated telehealth clinics, increased administrative staff, real-time technological support to assist patients and clinicians, sustainable technological infrastructure, and availability of government funding and local services for patient investigations such as lung function. HCP1: It would be ideal to have a secretary or IT administrator that can be there to help the older patients who can do it. HCP7: The [government funding] rules around how we can conduct telehealth also can be quite limiting particularly where they can’t use technology and they are expected to just get a phone call from us because that was what we were able to do a few years ago but now can’t. HCP11: I think very reliable technology and easy to use and to implement, able to integrate with the hospital technological interface. There has to be some local point of contact, be it a really good GP or a physician who can provide a more immediate and physical evaluation in the setting of a deterioration.
Research required for home monitoring in the management of ILD
Most HCPs were open to using home monitoring devices. However, many acknowledged uncertainties in the reliability and validity of results that require further evaluation. HCP6: My understanding from the literature is that they can be very variable and so whether it is right for prime time now, I am not sure. HCP8: I think it is an exciting new phase. I am doing research myself in the area but a lot of my patients have a pulse oximeter… Sometimes we don’t know what it means.
Discussion
This qualitative study found that the perspectives of telehealth amongst patients with ILD and HCPs were largely similar. Telehealth was felt to be convenient, and in particular, improved access to specialist care for patients restricted by disease severity and/or geographic locality. The major concern from both groups was the suboptimal assessment of patients’ clinical status, due to the lack of a physical examination and lung function testing which are pivotal components of disease monitoring. Both groups reported that preference for telehealth should be based on individual factors such as indications from previous clinical encounters, disease factors, and both HCP and patient preference. While the use of telehealth was acceptable to both groups, there is certainly scope for improvement, such as increased administrative support for HCPs, reliable technology and greater support from local services. Patients and HCPs were open to the use of home monitoring devices, however, HCPs had some reservations regarding their current clinical application.
Care delivery for ILD requires a multidisciplinary approach involving regular specialist review, investigations, MDM and supportive care such as pulmonary rehabilitation and palliative care. Our findings show that HCPs and patients would be open to the use of a hybrid model of care including both in-person and telehealth with flexible delivery modes, supported by access to local services. Integrated telehealth models of care have been shown to be successful in other chronic diseases such as heart failure, to allow more frequent monitoring of patients and improve access to management, with reduced hospitalisations and mortality.22–24 Nevertheless, equity of access to telehealth can be of concern, which can be influenced by access to or familiarity with telecommunication platforms, technological infrastructure and geographical location. 25 Those who use telehealth have been found to be more affluent and more likely to be white and female, while patients of lower socioeconomic status are less likely to engage. 26 Solutions proposed to improve access include financial assistance for devices and internet access, outreach programs and funding for healthcare infrastructure. 27 Monetary incentives or higher remuneration for providing telehealth to disadvantaged populations may encourage health services. 28
Key limitations of telehealth are difficulty with patient assessment and communication. Disparities exist between patient self-assessment and physician evaluation coupled with objective tests of the ILD disease state. 29 Telephone reviews when supported by lung function tests have been found to be adequate. 29 Similarly, in our study, physicians felt physical examination was important for making a diagnosis, but telehealth could be used for monitoring when supported by objective testing. This requires access to local services and reliable communication of results. Shared electronic medical records between health systems may ease the access to results from different providers. Furthermore, diagnosis and treatment discussions in ILD can involve challenging conversations, and therefore require good rapport and a robust physician-patient relationship. 30 Communication and information exchange is crucial for patients to understand their disease and participate in self-management. Poor communication can lead to patient anxiety and concerns about management. 31
Telehealth is unlikely to be suitable for all patients. This study identified various factors that may influence the use of telehealth in ILD, including patient preference, digital literacy, availability and quality of technology, disease complexity and distance from health services. These are compatible with previous non-ILD studies and highlight the need for individualised care. 32 In addition, older patients may be more likely to face technological difficulties and those with lower levels of education have been found to be less likely to have their medical needs addressed through telehealth. 26 Furthermore, choosing an appropriate clinical encounter for telehealth is important. An Australian study of tele-rheumatology during the COVID-19 pandemic found that while attendance improved, it was associated with delayed diagnosis, reduced likelihood of treatment change, and requirements for earlier subsequent face-to-face reviews in selected patients, such as those with no diagnosis. 33 In our study, both cohorts felt telehealth worked well after initial in-person contact to establish a therapeutic relationship and patient baseline, which has been reported for other conditions. 34 Telemonitoring has the potential to improve patient assessment during telehealth, identify clinical deterioration and aid treatment decisions. In this study, while both patients and clinicians responded positively to the potential use of telemonitoring, clinicians remain cautious of their clinical application in the absence of standardised methods. Given the potential of telemonitoring for improved patient assessment, further validation of these devices is warranted prior to wider implementation in ILD telehealth models of care.
Limitations of this study include being a single-centre study and therefore may not be reflective of all the perspectives of patients with ILD from other centres. However, patients from the Alfred ILD service are referred from private clinics and other hospitals in Victoria and therefore capture patients from various regions with varied socioeconomic status. Included patients also had a wide range of diagnoses and disease severity. While the perspectives of HCPs from different backgrounds were included, they remained limited to the Australian experience. Additionally, patients and caregivers of non-English speaking backgrounds were not interviewed, such that their perspectives remain unknown. There is also the potential for selection bias as a small proportion of patients (4/18) and HCPs (7/18) had a pre-existing relationship with the recruiting investigator. Of note, patients’ caregivers were not included in this study due to timing and logistic constraints, who may offer different perspectives.
Conclusions
This study highlights positive and negative experiences of telehealth for patients with ILD. While telehealth for improving healthcare delivery is promising, areas for improvement have been identified which need to be addressed in order to create a successful and tailored telehealth model for ILD care. Further research is required to evaluate the clinical outcomes and cost-effectiveness of hybrid telehealth models in ILD care, assess long-term acceptability of home monitoring devices and to develop strategies for supporting patients with lower digital literacy.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Ivan Cash Grant from the Lung Foundation Australia. HB reports honoraria and travel support from Boehringer Ingelheim and Janssen, outside the submitted work. IG reports honoraria from Boehringer Ingelheim and advisory board fees from TianLi Biopharma. YHK reports grants from the National Health and Medical Research Council Investigator Grant, Medical Research Future Fund, Austin Medical Research Foundation Research Grant, Lung Foundation Australia / Thoracic Society of Australia and New Zealand and the Royal Australasian College of Physicians.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.