
Abstract
Emphysema on high-resolution computed tomography of the chest is the recent focus in the general practice in idiopathic pulmonary fibrosis (IPF). However, adequate attention has not been paid to obstructive disorder. Therefore, we retrospectively evaluated the association between the degree of airway obstruction and longevity in IPF subjects, with a hypothesis that lower forced expiratory volume in 1 second (FEV1)/forced vital capacity (FVC) has an impact on prognosis. One hundred and fourteen consecutive IPF subjects who had been diagnosed with IPF and had undergone evaluation including pulmonary function test from January 2008 to May 2013 were included in the study. The relationship between baseline data and survival was examined. FEV1/FVC was widely distributed, ranging from 48.6% to 100%. On both univariate and multivariate Cox’s regression analyses, lower FEV1/FVC was significantly associated with better survival (hazard ratio of 1.07 and 1.04 and 95% confidential interval of 1.03–1.10 and 1.01–1.08, respectively). Even on analysis with backward selection, FEV1/FVC remained a significant prognostic factor. FEV1/FVC is widely distributed and negatively predicts survival in IPF. A FEV1/FVC should be assessed in “real-world” general practice. Also, the effect of smoking on the clinical course of IPF should be investigated further.
Introduction
Idiopathic pulmonary fibrosis (IPF) is one entity of idiopathic interstitial pneumonia without a known etiology. 1 The clinical course of IPF is usually progressive, and the prognosis is poor despite many past therapeutic challenges. 2,3
Several prognostic factors have been reported in previous studies. Not only lung physiology such as forced vital capacity (FVC) and diffusing capacity, but also the severity of dyspnea in daily life, exercise capacity, and the extent of fibrosis on high-resolution computed tomography (HRCT) of chest are important indicators of longevity in those with IPF. 4 –10 Furthermore, longitudinal decline in pulmonary function is also a significant marker of survival. 4,6,11,12
IPF is one of the restrictive lung diseases. Therefore, lung volume and diffusing capacity have been the focus of clinical IPF evaluations. However, in general practice, some IPF patients are current or former smokers. In some such subjects, airway obstruction can theoretically occur, and this can affect the results of pulmonary function tests, weaken exercise capacity, and restrict daily activity of the subjects. Because IPF subjects with airflow limitation are usually excluded from prospective clinical trials, the effects of airway obstruction on IPF were not specifically evaluated.
The effect of smoking on IPF physiology is presumed important. Combined pulmonary fibrosis and emphysema (CPFE) is one of the recent topics in the IPF field. 13,14 However, there is considerable disagreement as to whether being with CPFE is a better or worse indicator of prognosis than with IPF alone. 15 –17 These reports regarding CPFE were basically evaluating the disease severity according to emphysema on HRCT of the chest. Forced expiratory volume in 1 second (FEV1)/FVC was not greatly focused on despite the fact that it is an important and appreciable indicator of airway obstruction in pulmonary function test variables. Therefore, we have retrospectively evaluated the association between the degree of airway obstruction and longevity in IPF subjects, with the hypothesis that FEV1/FVC has a definite impact on prognosis in a general practice setting.
Methods
Subjects
One hundred and fourteen consecutive IPF subjects who had been diagnosed with IPF and had undergone evaluation including pulmonary function test, as is the general practice in the Kinki University Hospital, were included in the study. The study lasted from January 2008 to May 2013. The diagnosis of IPF was made according to the recent official statement 3 using the following criteria: (1) exclusion of other known causes of interstitial lung disease such as domestic and occupational environmental exposures, connective tissue disease, and drug toxicity, (2) the presence of usual interstitial pneumonia pattern on HRCT in subjects who did not undergo surgical lung biopsy, and (3) a specific combination of HRCT and surgical lung biopsy pattern in subjects who underwent surgical lung biopsy. Subjects were excluded if they had active coronary artery disease and/or unresolved malignancy. Those who had emphysema on chest HRCT and/or obstructive lung disease on pulmonary function test were included because this study aimed to reveal the prevalence and significance of airflow limitation in the IPF population. Subjects who had started long-term oxygen therapy before diagnosis were also included. The informed consent requirement was waived, because this study is based on a retrospective analysis of case records in our university hospital. Approval for the use of these data and the analysis was provided by the ethics committee of the Kinki University Faculty of Medicine (No. 25-179).
Pulmonary function tests
Pulmonary function tests included spirometry, single-breath measurements of diffusing capacity of the lung for carbon monoxide (DLCO; CHESTAC-8800; Chest, Tokyo, Japan), and arterial blood gas analysis, which were all performed according to the American Thoracic Society standards.
18,19
Results were expressed in absolute values and as percentage of Japanese normal predictive values.
20
A composite physiologic index (CPI) was derived from the following formula as previously reported:
HRCT image analysis
Inspiratory HRCT (1-mm-thick) images were obtained at 1-cm intervals with the subject in the supine position. The mean extent of ground glass opacity, reticular abnormality, honeycombing, and emphysema was scored to the nearest 5% visually in upper, mid, and lower areas in each lung. Emphysema was defined as a hyperlucent area of lung that lacked a distinct wall. The upper area was defined as at or above the aortic arch, the mid area was defined as between the aortic arch and pulmonary veins, and the lower area was defined as at or below the pulmonary veins. The average of fibrosis and honeycombing scores in each of the six areas produced a total fibrosis score. 10 This visual analysis was performed by three pulmonologists, and the consensus reached was adopted as the final score.
Assessment of survival
Survival was assessed through October 2013. Deaths and causes of death were identified by reviewing hospital chart records of subjects who had been regularly visiting our hospital, because documentation of their survival could be obtained. For subjects who moved to another hospital, we tried to obtain their survival status by telephone interviews with their family members. If the patient was dead, we also tried to obtain the date of death, even if the cause of death could not be obtained. The survival time was calculated as the period from the diagnosis to death. If a subject was still alive, his or her survival time was calculated as the period from the diagnosis to the last day the subject visited our hospital during the study period, but he or she was labeled as a censored case in the analysis.
Statistical analysis
Continuous variables were summarized by mean ± standard deviation (SD). Categorical variables were summarized by frequency. Survival time was calculated from the time of enrollment until death. Subjects were censored if there was no death in the medical record and we could not obtain the date of death even by contacting the subject’s family. Univariate and multivariate Cox proportional hazards regression analyses were performed. Two types of multivariate Cox proportional regression analyses were performed: one using variables with p < 0.1 on univariate analysis and the other using backward selection. Each analysis was performed while excluding subjects who had missing values in their baseline variables. All tests were performed at a significance level of 0.05. Analyses were performed with the PASW statistical package version 18 (SPSS Japan Inc., Tokyo, Japan).
Results
Of the total114 subjects, 94 were males and 20 were females. Their baseline characteristics at registration are summarized in Table 1. The mean age was 73.8 years (SD 6.7). The smoking status was obtained from 100 subjects consisting of 13 current, 73 former, and 14 never smokers. Mean FVC was 74.8% predicted and DLCO was 69.8% predicted, showing mild restrictive lung disorder. The mean FEV1/FVC was 82.0%. Values of FEV1/FVC ranged from 48.6% to 100%, a distribution slightly skewed toward a high value (Figure 1). Fifteen (13.2%) subjects showed a FEV1/FVC of less than 70%, which meant that their disease coincided with obstructive lung disorder. Surgical lung biopsy was performed only on three (2.6%) subjects. Three subjects were undertaking long-term oxygen therapy with 2, 2.5, and 4 L/min of oxygen through nasal cannula, respectively. The mean observation period was 880 days (SD 547). Among 61 (54.3%) subjects who died in this observation period, 8 (13.1%) died of respiratory failure, 9 (14.8%) of acute exacerbation of IPF, 6 (9.8%) of pneumonia, 7 (11.5%) of cancer, and 9 (14.8%) of other causes. The reasons for death of the other 22 (36.1%) subjects were not confirmed because they died in other hospitals.
Baseline characteristics of study population.a

BMI: body mass index; FVC: forced vital capacity; FEV1: forced expiratory volume in 1 second; DLCO: diffusing capacity of the lung for carbon monoxide; PaO2: partial pressure of oxygen; CT: computed tomography; CPI: composite physiologic index; Hg: mercury.
an = 114 except for DLCO (n = 81), PaO2 (n = 89), and CPI (n = 81). All PaO2 values were taken from subjects breathing ordinary room air with the exception of three subjects. Values of these three subjects were taken with oxygen inhalation through nasal cannula of 2, 2.5, and 4 L/min, respectively. Continuous variables are expressed as mean values with standard deviations in parentheses.
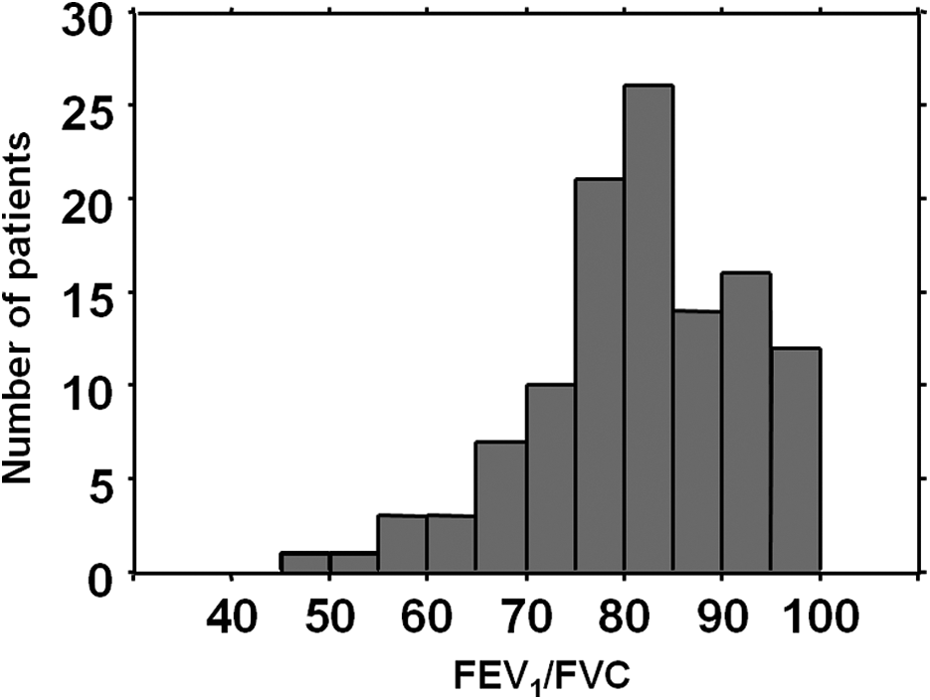
Frequency distribution histograms of FEV1/FVC. FEV1: forced expiratory volume in 1 second; FVC: forced vital capacity.
Scores of each HRCT finding are also shown in Table 1. Scores of fibrosis and emphysema showed similar values of 7.9% and 8.2%, respectively.
Univariate predictors of survival are listed in Table 2. Female sex, higher body mass index (BMI), higher % predicted FVC, lower FEV1/FVC, higher partial pressure of oxygen (PaO2) value, and higher fibrosis score on HRCT were significantly associated with longer survival. There were no highly correlated (correlation coefficient was 0.6 or greater) variables among them. On multivariate analysis including sex, BMI, % predicted FVC, FEV1/FVC, and fibrosis score as independent variables, female sex, higher BMI, higher % predicted FVC, lower FEV1/FVC, and higher fibrosis score were significantly associated with longer survival. In a backward selection model, female sex, % predicted FVC, and FEV1/FVC were found to be significant predictors of survival (Table 3). Multivariate analysis with the addition of PaO2 values in independent variables was also performed, although PaO2 data were lacking in some subjects. On this model with 89 subjects, female sex and lower FEV1/FVC were significantly associated with longer survival. In the backward selection model, female sex, FEV1/FVC, and PaO2 value were selected as significant (Table 4). Kaplan–Meier survival curves based on the FEV1/FVC value (≥ and < the median value of 83%) are shown in Figure 2. The median survival estimates for subjects with FEV1/FVC ≥83% and <83% were 755 and 1452 days, respectively.
Predictors of survival time in univariate analysis.a

CI: confidence interval; BMI: body mass index; FVC: forced vital capacity; FEV1: forced expiratory volume in 1 second; DLCO: diffusing capacity of the lung for carbon monoxide; PaO2: partial pressure of oxygen; CPI: composite physiologic index; Hg: mercury.
an = 114 except for smoking status (n = 99), DLCO (n = 81), and PaO2 (n = 89). Hazard ratios in smoking status refer to never smoking status.
Predictors of survival time excluding PaO2 value in multivariate analysis.a

CI: confidence interval; BMI: body mass index; FVC: forced vital capacity; FEV1: forced expiratory volume in 1 second.
an = 114.
Predictors of survival time including PaO2 value in multivariate analysis.a
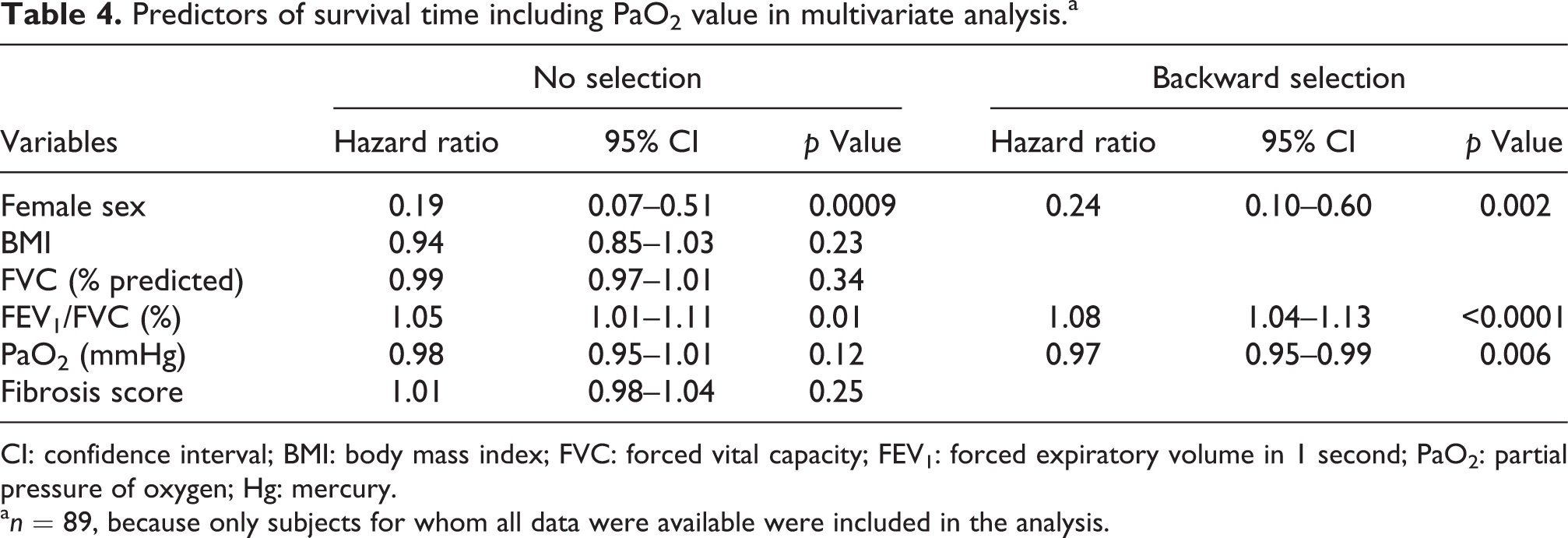
CI: confidence interval; BMI: body mass index; FVC: forced vital capacity; FEV1: forced expiratory volume in 1 second; PaO2: partial pressure of oxygen; Hg: mercury.
an = 89, because only subjects for whom all data were available were included in the analysis.
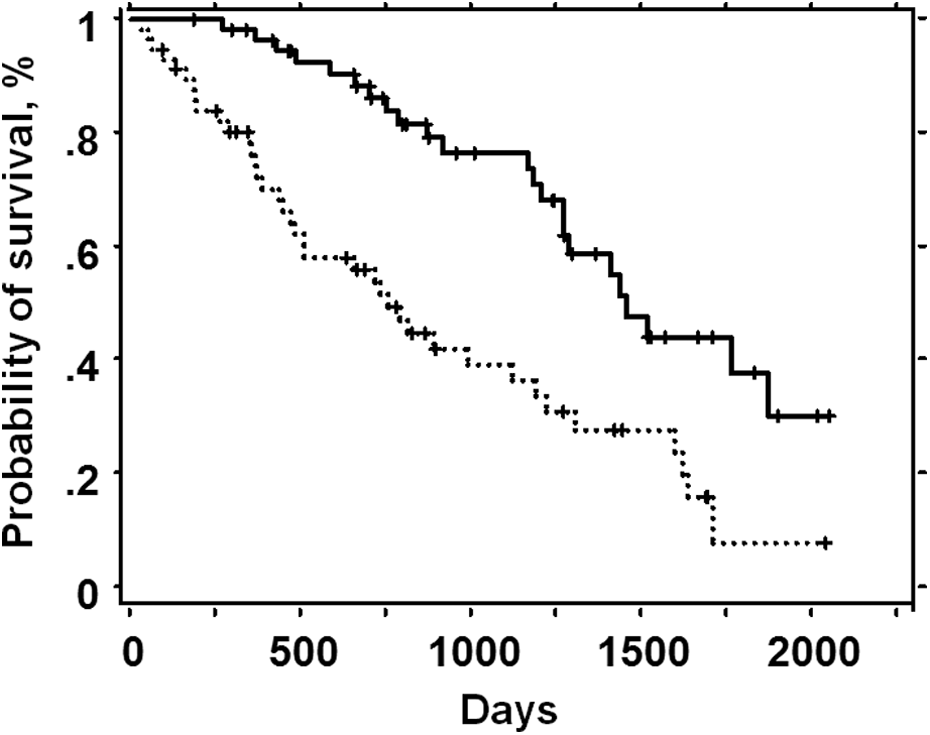
Kaplan–Meier survival curves according to FEV1/FVC value (—: less than 83%; …: equal or more than 83%; p < 0.0001). Survival curves were compared with log-rank statistic. +: censored; FEV1: forced expiratory volume in 1 second; FVC: forced vital capacity.
Discussion
Presumably because IPF is a conceptually restrictive lung disease, evaluation of FEV1/FVC has not been the focus and has mostly been relatively ignored in both clinical studies and general practice. However, the effect of smoking on lung function cannot be dismissed in general IPF practice, because there are subjects who are currently smoking or who had previously smoked to a certain extent. For this reason, we conducted a retrospective study focusing on FEV1/FVC, which is considered to be an indicator of obstructive lung disorder.
In the current study, the value of FEV1/FVC was widely distributed, ranging from 48% to 100%. In fact, the value of FEV1/FVC was below 70% in 15 (13.2%) subjects, although they had been excluded from clinical studies to date. In other words, many subjects with IPF, whose FEV1/FVC decreased, exist in “real-world” practice. A decrease in FEV1/FVC might be caused by smoking. Interestingly, lower FEV1/FVC was significantly associated with longer survival in the present study. Moreover, the prognostic value of FEV1/FVC was independent, indicating that it was not simply high FEV1/FVC that was a result of the negative prognostic value of low FVC. As for the other factors including female sex, % predicted FVC, PaO2 value, BMI, and the fibrosis score on HRCT, which were revealed to be prognostic in the present study, the results were the same as in previously reported studies. 4 –6,9,10,22
The number of patients whose FEV1/FVC<70%, which is generally recognized as a threshold of an obstructive lung disorder, was relatively small in the current study. If the survival was compared between patients with FEV1/FVC≥70% and FEV1/FVC<70%, a tendency to better survival was found in patients with FEV1/FVC<70% (data not shown), although statistical significance was not reached (Log-rank p = 0.06). Therefore, we think that the results of our study were not necessarily because the number of patients with FEV1/FVC<70% was small. The same results would be obtained even with more patients whose FEV1/FVC <70%, although it must be confirmed further in patient series with more severe airway obstruction. If patients with FEV1/FVC <70% were excluded from the analysis, FEV1/FVC was selected as a significant predictor of survival (data not shown). This means that FEV1/FVC still has a positive impact on survival among patients with only very mild airway obstruction.
The negative relationship between FEV1/FVC and survival in IPF subjects was actually observed in two previous studies, although FEV1/FVC was not focused on as a primary study outcome in them. Schwartz et al. demonstrated that lower FEV1/FVC was associated with better survival in IPF, similar to our study. 23 However, the authors speculated that their result simply reflected the overlapping, or duplicative, information derived from physiologic measures. More importantly, their study was conducted before the concept of nonspecific interstitial pneumonia was established, and their diagnosis of IPF was therefore presumably inaccurate. Lower FEV1/FVC was also indicated as a predictor of better survival in another study by King et al., although the FEV1/FVC value was not mentioned. 24 It is presumed that the authors thought this result was an accidental event. Therefore, our study was the first to be conducted with FEV1/FVC as a primary outcome after the current diagnostic guideline was published. 3
The result of the present study that demonstrated a significant relationship between FEV1/FVC and survival in IPF subjects seems to be in fact correct, because it is very consistent with findings from previous studies. 23,24 Furthermore, our subject series was composed of IPF subjects who were diagnosed according to the current statement. 3 It is important that FEV1/FVC negatively predicts mortality in IPF subjects diagnosed specifically according to the new guideline. The reason for the negative relationship between FEV1/FVC and survival remains unclear. However, some conjectures can be made. King’s study documented that current smokers had a better prognosis than former smokers and never smokers. 24 Some recent reports also demonstrated better survival in subjects with CPFE compared to IPF subjects without emphysema. 16,25 According to these reports, smoking seems to have had a good effect on the survival of IPF subjects. Also, a low incidence of acute exacerbation was suggested as a reason why CPFE subjects survived longer. 16 Delay of the decrease in lung function in CPFE subjects was also demonstrated. 26 However, limited data exist regarding the effect of smoking on pathophysiology in IPF, although one report demonstrated that cigarette smoke inhibits lung fibroblast proliferation. 27 The better prognosis in subjects with lower FEV1/FVC that was observed in the present study might be coincident with the good effect of smoking in IPF, which was reported in the previous studies. In fact, smoking history was not predictive of survival in the present study. That might be because of the vague categorization of current, former, and never smokers. If a detailed analysis was performed to assess the amount of smoking, like the Brinkman Index, the results might have been different. The fact that smoking history was unclear in some subjects might have also affected the result. Also, the emphysema score did not predict survival in the present study. This may suggest that obstructive lung disorder is more important than emphysematous change where effects on longevity are concerned. The other possible reason for our result is that high FEV1/FVC was a result of the negative prognostic value of low FVC. In restrictive lung disease, not only FVC but also FEV1 decreases as disease progresses. It is possible that FVC decreases faster than FEV1, resulting in FEV1/FVC being a negative prognostic factor. However, the prognostic value of FEV1/FVC was revealed to be independent in the multivariate analysis, which indicates that a high FEV1/FVC value did not simply reflect the result of a low FVC. It is also interesting that the CPI, which is known to be prognostic in IPF, 21 did not significantly associate with survival in the present study. In general practice with patients who have a history of smoking, FVC, FEV1, and DLCO are assumed to relate to each other in a complicated manner. It is therefore possible that the CPI did not represent the extent of the IPF disease.
There are some limitations in the present study, including the lack of serial changes in physiologic parameters in the analysis. Longitudinal changes in physiology reportedly predict survival. 4,6,28,29 A different result would have been obtained if serial changes in physiologic parameters were included in the analysis. Second, detailed smoking history including the amount of cigarettes such as the exact number of packs smoked per year was lacking, and some subjects’ smoking history was unknown. Third, analysis of the causes of death could not be performed, because a certain number of subjects had died at other hospitals, and the causes of death were not precisely ascertained, because deaths were checked only by telephone interview with the families of the deceased. Fourth, the observation period was relatively short, although more than half of all subjects were dead. Reassessment with a longer observation period will be needed. Finally, the retrospective study design is another limitation, because faulty assessment of several data such as DLCO and PaO2 values was made with it. Collection of additional prospective data is warranted to confirm our findings.
In light of conflicting data regarding prognosis of CPFE subjects, 13,15 –17,25 the effect of smoking on the clinical course of IPF should be investigated more. Basic research in terms of the relationship between smoking and the fibrosis process in IPF is also crucial. Given the results of our study, not only emphysema on HRCT but also obstructive disorder should be made a focus. This indicates that FEV1/FVC should be assessed in real-world clinical practice.
In conclusion, FEV1/FVC is widely distributed and negatively predicts survival in general practice of IPF.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.