
Abstract
Background
Identifying clinical and socio-economic predictors of adverse health outcomes in chronic obstructive pulmonary disease (COPD) patients is imperative for reducing exacerbation and mortality rates.
Methods
The COPD Community Disease Management (COPD-CDM) clinical trial evaluated the efficacy of a disease management program among 1202 ambulatory COPD patients receiving recommended care. The study did not find disease management to be superior to recommended care only, in preventing COPD hospital admissions or mortality. This post-hoc analysis examined the association of clinical and socioeconomic parameters with the length of in-hospital stay and all-cause mortality by multivariable non-linear mixed and Cox proportional hazards models, adjusted for age, sex, study arm, recruitment and study period, and medical therapy.
Results
A one-point increment in the Modified Medical Research Council dyspnea scale was associated with a higher hazard for all-cause mortality, (Hazards Ratio [HR]:1.50, 95% confidence interval [CI]: 1.22–1.85); longer in-hospital stay for COPD or all causes; Rate Ratio (95% CI): 1.64 (1.36–1.98), and 1.36 ( 1.19–1.55), respectively. A 50 m increment in six-minute walking distance was associated with fewer days in-hospital for both COPD and all causes; Rate Ratio (95% CI); 0.94 (0.89–0.99) and 0.95 (0.92–0.99), respectively. Unemployment and lower educational attainment were associated with a longer in-hospital stay both for COPD and all causes.
Conclusions
Clinical and socioeconomic parameters were associated with the number of days in hospital for COPD and all-causes, and all-cause mortality in ambulatory COPD patients. Our findings support the importance of a multi-disciplinary pulmonary approach to improve clinical outcomes among COPD patients.
Introduction
Chronic obstructive pulmonary disease (COPD) is a persistent, often progressive airway obstruction manifested by chronic respiratory symptoms. 1 Exacerbation of these symptoms heightens the risk of disease progression, emergency department visits, hospital admissions, and mortality.2–6 Viral infections are the primary triggers for symptom exacerbations followed by bacterial infections and environmental factors such as air pollution.7,8 Treatment recommendations include Long-acting beta-agonists (LABA), long-acting muscarinic antagonists (LAMA), and inhaled corticosteroids (ICS) to reduce the frequency of COPD exacerbations. 1
Clinical parameters such as breathlessness, frequently measured by the modified Medical Research Council (mMRC) dyspnea scale, help to evaluate the risk of exacerbations.9,10 The level of airflow obstruction, as well as comorbidities, are known to increase the risk for hospitalization6,11–13 and mortality 14 in COPD patients.
Socioeconomic status (SES) was found to be negatively associated with COPD outcomes with at least twice the risk for morbidity and mortality in patients in the lowest compared to the highest SES class. 15 In a recent study from Japan, among older men screened for COPD, living alone, lower education, and less social participation were associated with higher mortality risk. 16 Lange et al. found that fewer years of schooling in Denmark were associated with a higher risk of COPD exacerbations and all-cause mortality compared to university education. 17 In another study from Sweden, low annual income and rented versus self-owned housing were associated with a higher risk for COPD incidence. Also, compared to married subjects, divorced and widowed individuals had an increased risk for hospitalization due to COPD. 18
The COPD- community disease management (COPD-CDM) was a multicenter clinical trial that examined the efficacy of disease management added to recommended care over recommended care alone in 1202 COPD Jewish and Arab patients with moderate to very severe airflow limitation. 19 The Arab community in Israel, mostly urban, is the largest ethnic minority group, accounting for about 21% of the total population. Compared to the Jewish majority group, the Arab minority is socioeconomically disadvantaged, with a high prevalence of cigarette smoking among men, and higher chronic morbidity and mortality rates. 20
Pulmonary care of the patients in both study arms was provided in two community-based designated COPD study centers by pulmonary specialists and included a pulmonary rehabilitation program The disease management intervention was delivered by nurses that conducted face-to-face and remote sessions with the patients, monitoring respiratory symptoms, providing advice in case of symptom exacerbations, motivating adherence to medical therapy and healthy lifestyle and providing self-care education. The addition of disease management was not superior to recommended care alone in reducing the risk of first hospital admission for respiratory symptoms or all-cause mortality (composite primary endpoint).
In this post-hoc analysis, we explored the association between clinical, demographic and socio-economic characteristics and the burden of COPD, i.e., in-hospital days for COPD and for all-causes, and mortality from any cause, in the entire study cohort.
Methods
Detailed information on the study population, assessments, and outcomes was previously reported. 19 In brief, the study was a multicenter open-label randomized trial (Trial registration: NCT00982384). COPD patients, living in two central mainly urban districts and insured by the largest health plan in Israel were eligible if they were ≥40 years old, with severe or very severe airflow limitation according to the Global Initiative for Chronic Obstructive Lung Disease (GOLD) 21 (GOLD stage 3 or 4), or if they had a moderate airflow limitation (GOLD stage 2) and an unstable disease; a history of current or past cigarette smoking, and no history of childhood-onset asthma. Patient recruitment occurred between 2009 and 2012. Assessments were conducted at three urban out-patient COPD study centers at baseline and every 6 months thereafter. Baseline assessment included patient medical and tobacco exposure history, demographic and socio-economic parameters. Patient dyspnea level using the mMRC dyspnea scale, a 6 min-walk test (6MWT), and a post-bronchodilator spirometry test were assessed at baseline and every 6 months thereafter. Information on purchases of prescribed inhalers (ICS, LABA and (LAMA), hospital admissions and mortality during follow-up was obtained from the health plan electronic records and updated until the end of study. Over 98% of the hospital discharge summaries were classified by two independent investigators as due either to COPD exacerbation or other causes. Data on hospital admissions were collected until the end of the trial (2014). The total number of in-hospital days for COPD or all causes was calculated for each 6 months follow-up period. The information on mortality from any cause was obtained from the Israel population registry and updated in 2022.
Statistical analysis
All analyses were performed using SAS (version 9.4, SAS Institute Inc., Cary, NC). Continuous variables are presented as median with interquartile range (IQR). Categorical variables are presented as N (%). If one of the mMRC dyspnea scale, GOLD stage, and 6MWT parameters were missing at the beginning of the 6 month period, the value from the previous period was carried over.
The Cox proportional hazards model was used to test predictors for all-cause mortality, adjusting for age and sex. Additional candidate variables considered included ethnicity (Jewish or Arab), education, marital status, number of pack-years, employment status, Charlson comorbidity index (CCI), asthma, COPD center, randomization year, study period and the study arm. GOLD stage, mMRC dyspnea scores and purchases of prescribed inhalers were included in the model as time depended covariates. To create a parsimonious multivariable predictive model, candidate variables were entered in a stepwise hierarchical manner, unless otherwise specified. Variables that were not significantly associated with the outcome (p < 0.1) were excluded in the next step.
The assumption of proportional hazards between the treatment arms was ascertained by including a time dependent variable for each covariate of interest to test the assumption of no time dependent effect. No violation was found.
The number of days in hospital for COPD or all causes was summarized in 6 months intervals. We used nonlinear mixed models (NLMIXED procedure; SAS, version 9.4, SAS Institute), to test the associations between the patient clinical and socioeconomic characteristics, and the number of in-hospital days for COPD and for all causes. The models included a random subject intercept term to account for the correlation between periods in each patient. A negative binomial distribution was assumed to account for overdispersion frequent in hospital admission data. 22 Models were adjusted for sex, center, age, GOLD stage (at baseline and at the beginning of each 6 months follow-up period), randomization year, and time since randomization. Model coefficients represent the adjusted log rate ratio over a 6 month period.
All models were adjusted for the study center, study period, recruitment year, the original study arm, and the use of inhalers (ICS, LABA, LAMA).
Results
Basic characteristics of 1145 COPD patients included in the post hoc analysis.
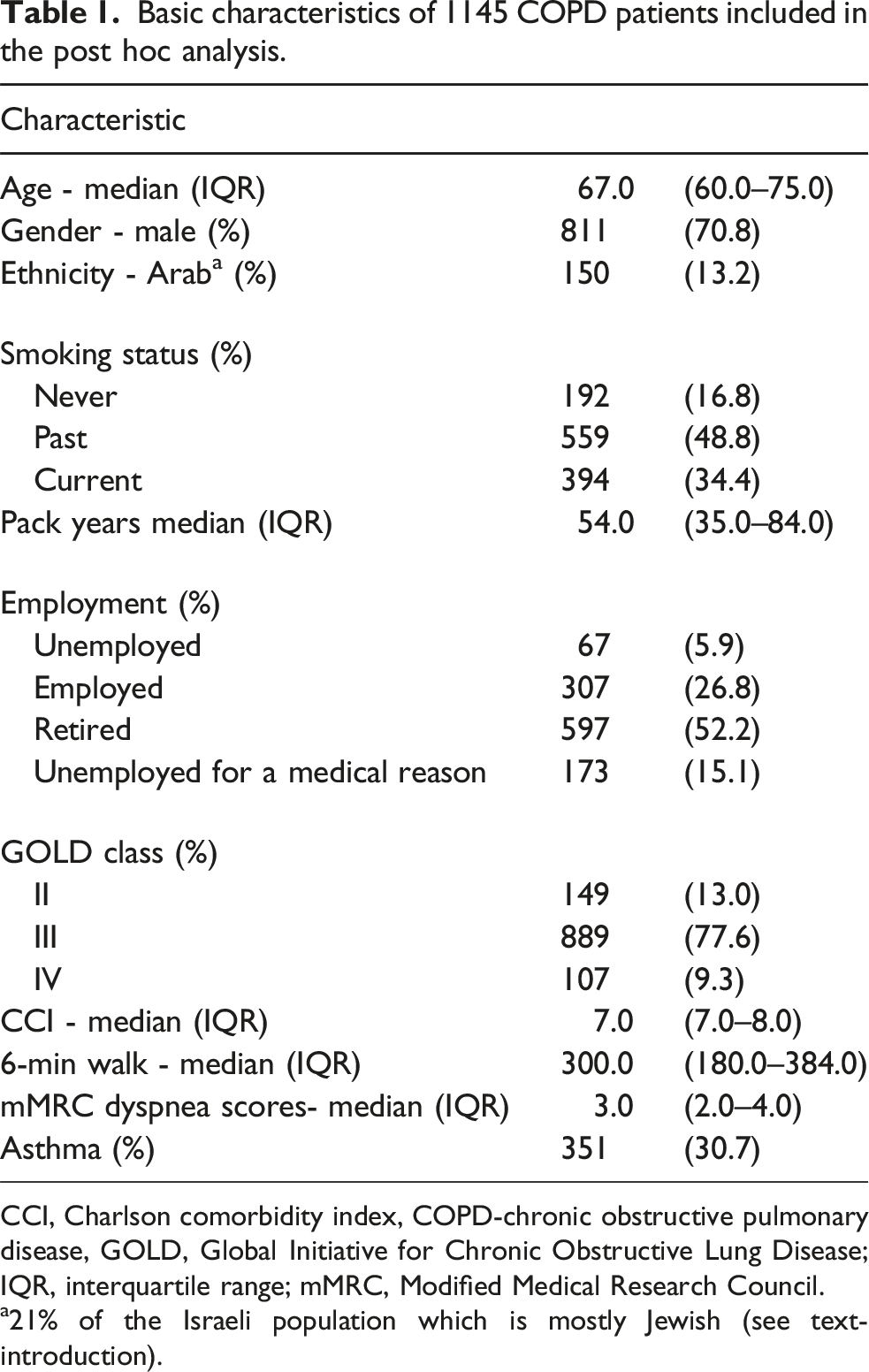
CCI, Charlson comorbidity index, COPD-chronic obstructive pulmonary disease, GOLD, Global Initiative for Chronic Obstructive Lung Disease; IQR, interquartile range; mMRC, Modified Medical Research Council.
a21% of the Israeli population which is mostly Jewish (see text-introduction).
All-cause mortality
Multivariable analysis of all-cause mortality among 1142 COPD patients a .

CCI, Charlson comorbidity index; CI, confidence interval; GOLD, Global Initiative for Chronic Obstructive Lung Disease; HR, hazard ratio; ICS, inhaled corticosteroids; LABA, long-Acting beta agonist; LAMA, long-acting muscarinic antagonists; mMRC, Modified Medical Research Council.
a3 patients were excluded due to at least one missing value.
bfrom previous period.
Of the clinical parameters, only the mMRC score in the prior 6 months and the baseline CCI were significantly associated with all-cause mortality during follow-up. All-cause mortality hazard was 1.5 times higher (95% CI: 1.22–1.85) for a 1-point mMRC scale increment and 1.4-times higher (95% CI: 1.2–1.62) for a 1-point increment in CCI. Diagnosis of asthma at baseline and the GOLD stage were not significantly associated with all-cause mortality. All analyses were adjusted for the use of inhalers (ICS, LABA, LAMA), recruitment year, study center and study arm (guidelines recommended care, or guidelines recommended care plus disease management).
In-hospital days due to COPD
In-hospital days due to COPD a .

CCI, Charlson comorbidity index; CI, confidence interval; COPD, chronic obstructive pulmonary disease; GOLD, Global Initiative for Chronic Obstructive Lung Disease; mMRC, Modified Medical Research Council.
aCompete data available for 1131 COPD patients.
bRate ratios between the adjusted mean number of in-hospital days.
c21% of the Israeli population which is mostly Jewish (see text-introduction).
dduring the previous 6 months.
Of the clinical parameters, the risk of having a relatively higher number of in-hospital days due to COPD increased by 1.64 for each increase in the mMRC score (95% CI: 1.36–1.98) and by 1.3 for each increase in the GOLD stage (95% CI: 1.01–1.67). Each 50-m increment in 6MWT distance was associated with a 6% lower number of in-hospital days for COPD (95% CI: 0.89–0.99). The number of in-hospital days was more than two times higher (95% CI: 1.61–2.55) among patients who experienced hospitalization due to COPD in the previous 6 month period.
In-hospital days for all causes
In-hospital days due to any-cause a .

CCI, Charlson comorbidity index; CI, confidence interval; GOLD, Global Initiative for Chronic Obstructive Lung Disease; mMRC, Modified Medical Research Council.
aCompete data available for 1131 COPD patients.
bRate ratios between the adjusted mean number of in-hospital days.
c21% of the Israeli population which is mostly Jewish (see text-introduction).
dduring the previous 6 months.
Of the clinical parameters, the rate of in-hospital days for any cause increased by 1.15 (95% CI: 1.01–1.31) for one point increment of the CCI and by 1.36 for 1-grade increment in the mMRC score (95% CI: 1.19–1.55). As for COPD hospitalizations, each 50-m increment in 6MWT distance was associated with a 5% lower number of in-hospital days for any cause (95% CI: 0.92–0.99). The likelihood for longer hospitalization was 1.52 higher (95% CI: 1.34–1.72; p < 0.0001) for patients admitted for any cause in the previous 6 month period. Baseline diagnosis of asthma was associated with a higher number of in-hospital days for all causes (RR 1.34, 95% CI: 0.99–1.81). GOLD stage and using inhalers (ICS, LABA, LAMA) had no association with the number of hospital days for all causes. All analyses were adjusted for the study center, study period, recruitment year, and the original study arm.
In comparison of the associations of various predictors with in-hospital days for COPD and for all causes, older age was significantly associated with more in-hospital days for all causes but not for COPD. Fewer years of schooling were associated with more in-hospital days for COPD but not for all causes. Otherwise, there were no substantial differences between the risk factors for in-hospital days for all-causes and for COPD (Appendix Table 1).
Discussion
In this post hoc analysis, we found that socioeconomic, functional, and clinical parameters are predictors of all-cause mortality and longer in-hospital stays due to COPD and due to all causes. Age and smoking, as expected, were significantly related to a longer in-hospital stay. In this study, 17% of the patients were never smokers. This is consistent with the literature that risk factors for COPD other than smoking such as industrial area, genetic and familial are responsible for less than 80% of the patients. 23 Approximately 31% of the patients had an asthma diagnosis. Asthma and COPD have been reported as a second diagnosis in 15%–32% of the patients with either disease. 24
Socioeconomic parameters, significantly associated with longer hospital stays, included lower education, retirement and unemployment due to medical reasons. Being married was only weakly associated with fewer days in hospital due to COPD compared to being single. Our results align with several previous studies. In a Swedish study, 61% and 30% higher risk for hospitalization due to COPD was observed in divorced and widowed individuals, respectively, compared to married subjects. 18 People who are widowed or divorced are living alone more often than people who are married. Living alone could delay hospital discharge due to the lack of family support. 25 A study from Italy found that being married was associated also with shorter in-hospital stay among male COPD patients. 26 The authors attributed this fact to the role of women as principal caregivers.
In a study from Denmark, patients living alone were 20% less likely to receive all relevant care processes in a mandatory national quality improvement initiative for COPD patients 27 and were at a higher risk of poor adherence and non-use of inhaled maintenance medications. 28
In the current study, patients with eight or less years of schooling had longer in-hospital stay due to COPD exacerbations compared to patients with ≥ 13 years of education. Our findings are in line with other studies that reported an association between lower education and poor COPD outcomes. In a study from California, lower education was associated with 50% higher risk of acute COPD exacerbation. 29 Lange and colleagues reported a higher risk for admission due to COPD among patients with less than 8 years of education compared to patients with university education. 17 While we did not find any significance relationship between the level of education and mortality, Lange et al. reported a 1.86 higher mortality risk (95% CI: 1.20–2.90) among patients with less than 8 years of education compared to patients with university education. This difference might be explained by a larger study population (6590 vs 1145) and longer follow-up period compared to this study (mean 4.3 vs 3 years).
In the current study, retirement and unemployment due to medical reasons were associated with longer hospital stays due to COPD or all causes. Early Retirement was previously reported to be associated with increased risk for poor COPD outcomes. 30 A vicious cycle between acute exacerbation of COPD (AECOPD), disability, and retirement could explain the increased risk of readmissions and unemployment due to medical reasons in our study. In a study from Denmark, 17% of patients with AECOPD retired from the workforce for a disability during 3 years of follow-up. Other predictors of disability retirement included older age, a larger number of comorbidities, emphysema, depression, cardiac comorbidity, and more advanced inhalation medication treatment step. 31
The relationship between low SES and poor outcomes among COPD patients is multifactorial. For example, smoking prevalence and the greater amount of smoking are more strongly associated with lower SES.32,33 Patients with a lower SES are more likely to live in communities with greater exposure to air pollution. 34 In addition, patients with a lower SES are more likely to be exposed to lower indoor air quality 35 or to be occupied with more manual work with higher exposure risks for harmful inhaled particulates.18,36 The complex relationship between risk factors such as smoking, lower education and health literacy, indoor and outdoor air pollutants, crowding, poor nutrition and among patients at the lower SES could play an important role not only in the development of COPD but also in disease-related outcomes, i.e., exacerbations, hospitalizations and mortality.
The 6 MWT, CCI, and GOLD stage, in the current study, were partially related to the study’s clinical outcomes while the mMRC score was consistently correlated with all outcomes. As in other studies, the level of breathlessness was strongly associated with COPD morbidity and mortality, and a simple tool such as the mMRC scale was found to correlate with exacerbation and hospitalizations.9,10,37
Higher performance in the 6 MWT had a minor but significant association with shorter length of hospitalization (overall, and COPD related). As known from previous studies, poor performance on the 6 MWT is related to worse prognosis such as hospitalization and mortality in patients with COPD and other pulmonary diseases, while improving the test performance can alter the outcomes.38,39
The GOLD stage, classified at the time of the study, based on forced expiratory volume in one second (FEV1), was found to be significantly associated with longer hospital stays due to COPD. FEV1 has a weaker linear correlation with COPD than the physiologic performance tests such as the mMRC scale, however, the risk of exacerbations, hospitalization, and mortality was found to be associated with worsening airflow obstruction.1,6
Our finding of a correlation between CCI and mortality and longer stay in hospital for all-causes is in line with previous reports in which comorbidities and higher CCI was found to be related to higher risk for exacerbations, hospitalization and mortality.11–13,40
We found prior recent hospitalization due to COPD to increase the overall risk of readmission. Frequent exacerbations in the previous year were found to predict further exacerbations.4,41 In a study by Gershon and colleagues in Canada, previous hospitalizations due to COPD were risk factors for 30 days readmission or mortality. 42 In fact, one in five COPD hospital discharges resulted in a readmission of which about 60% were due to COPD. 42 Also, several socioeconomic domains (such as patients living in areas of highest residential instability, highest material deprivation, and highest ethnic concentration) and certain comorbidities were associated in the same study with an increased risk for readmission or mortality.
Although our findings are in line with those of previous publications, the data were driven from a prospective multicenter study, which was unique, to the best of our knowledge, because of its comprehensive evaluation of both clinical and socioeconomic parameters every 6 months. However, there are several limitations to this study. First, albeit using clinical trial data that were carefully and systematically collected, the post hoc nature of our study does not allow us to interpret our results as causative. Second, the study sample was chosen to provide statistical power to test the original trial objective. It may not provide enough statistical power to test the associations of a larger set of predictors, such as smoking status, ethnicity, and SES, etc. with the study outcomes. The associations found in our study should be validated in future studies. Another limitation is the GOLD classification based on spirometry according to the guidelines at the time of the study. The current classification, based on former exacerbations, could have a better relation to the study outcomes.
In summary, in this post hoc study among COPD patients, chronic co-morbidity and the severity of COPD symptoms predicted higher hospitalization burden and mortality. Additional predictors of the number of days spent in hospital included COPD stage, physical performance and sociodemographic characteristics including lower education, unemployment, and being unmarried. Our findings are in line with central role of multi-disciplinary pulmonary approach addressing physical and psycho-social needs that may improve clinical outcomes among COPD patients. We suggest that health caregivers would stratify COPD patients according to their risk profile, including predictors such as smoking, unemployment and family support and provide interventions (e.g., telecommunication, education, reduction of smoking and environmental exposures) to reduce the risks for poor disease outcomes.
Footnotes
Ethics approval
The study was approved by Clalit Health Services (approval number 83/09) and the Sheba Medical Center (approval number: 7120-09-SMC) Ethic Committees.
Informed consent
All participants provided informed consent prior to inclusion in the COPD-CDM clinical trial.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The COPD-CDM clinical trial was supported by the Medical Research infrastructure Development and Health Services Fund by the Sheba Medical Center (Ramat-Gan, Israel).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Except for statistical analysis, the data underlying this article cannot be shared publicly due to privacy issues such as personal details of the study participants.
Appendix
Data analysis flow diagram.
Comparison of the associations of various predictors with in-hospital days for COPD and for all causes. aModel was adjusted for study period, recruitment year, treatment with LABA, LAMA and ICS, and study intervention type (recommended care plus disease management vs. recommended care only). bType-3 comparisons.
In-hospital days for COPD
a
In-hospital days for all-causes
a
Rate ratio (95% confidence interval)
Sociodemographic characteristics
Age (10-years increment)
0.96 (0.74, 1.24); p = 0.75
1.36 (1.13, 1.62); p = 0.0009
Sex (female vs male)
1.12 (0.72, 1.75); p = 0.62
0.87 (0.63, 1.20); p = 0.40
Arab vs Jewish
1.61 (0.92, 2.80); p = 0.094
1.42 (0.95, 2.11); p = 0.086
Years of education:
p < 0.0001
b
p = 0.11
b
0–8 vs ≥ 13
3.46 (1.99, 6.02)
1.47 (1.01, 2.14)
9–12 vs ≥ 13
1.95 (1.14, 3.34)
1.20 (0.84, 1.73)
Married vs. not married
0.69 (0.46, 1.03); p = 0.069
0.85 (0.64, 1.13); p = 0.27
Employment status:
p = 0.071
b
p = 0.0017
b
Unemployed vs employed
1.08 (0.48, 2.46)
2.03 (1.15, 3.59)
Retired vs employed
1.73 (1.04, 2.87)
1.56 (1.09, 2.23)
Unemployed for medical reason vs employed
1.90 (1.07, 3.37)
2.07 (1.38, 3.13)
Tobacco exposure history
Cigarette smoking pack-years
p = 0.18
b
p = 0.068
b
1–20 vs 0
1.95 (0.93, 4.06)
1.58 (0.95, 2.64)
21–59 vs 0
1.57 (0.89, 2.79)
1.25 (0.84, 1.86)
≥60 vs 0
1.84 (1.02, 3.33)
1.62 (1.08, 2.44)
Clinical parameters
Asthma-COPD overlap
1.25 (0.81, 1.92); p = 0.31
1.34 (0.99, 1.81); p = 0.057
Charlson comorbidity score (1-point increment)
1.09 (0.91, 1.31); p = 0.35
1.15 (1.01, 1.31); p = 0.036
MRC (1-point increment)
1.64 (1.36, 1.98); p < 0.0001
1.36 (1.19, 1.55); p < 0.0001
6-min walk-test (50 m increment)
0.94 (0.89, 0.99); p=0.028
0.95 (0.92, 0.99); p = 0.020
Hospital admission for COPD in the previous 6-month period
2.03 (1.61, 2.55); p < 0.0001
___
Hospital admission for any cause in the previous 6-month period
___
1.52 (1.34, 1.72); p < 0.0001