
Abstract
Objectives
Treatment recommendations for chronic obstructive pulmonary disease (COPD) are based on single or combination long-acting bronchodilator therapy (β2-agonists [LABAs] or muscarinic receptor antagonists [LAMAs]), with inhaled corticosteroids (ICS) for those at risk of exacerbations. This study evaluated differences in patient characteristics and treatment patterns among US clinicians.
Methods
Medical record data for patients with COPD were abstracted via a retrospective cross-sectional survey by pulmonologists, internal/family medicine physicians, nurse practitioners (NPs) and physician assistants (PAs).
Results
Data on 700 patients were collected from 175 clinicians: 100 pulmonologists, 45 internal/family medicine physicians, 30 NP/PAs. Respondents classified patients as having Mild (11%), Moderate (51%), or Severe/Very Severe (38%) COPD, with highest perceived disease burden for patients with Severe/Very Severe COPD. Dual therapies were prescribed differently according to clinician type. Internal/family medicine physicians and NP/PAs prescribed LABA/ICS to a significantly higher proportion of patients than pulmonologists, who favored use of dual bronchodilator therapy. Regardless of clinician type, COPD management was complex, with patients starting and transitioning to multiple treatments throughout their care.
Conclusion
Differences in COPD treatment patterns exist across US clinicians. Despite current maintenance treatment, COPD had a profound impact on patients, indicating a need for improved therapies for COPD.
Introduction
Chronic obstructive pulmonary disease (COPD) is a heterogeneous lung condition characterized by chronic respiratory symptoms due to airway and/or alveoli abnormalities that cause persistent airflow obstruction.1,2 In the United States (US), COPD is the third leading cause of reduced disability-adjusted life years (DALYs), contributing to substantial morbidity and mortality.3,4 Approximately 1.3 million US emergency department visits in 2019 were for COPD-related conditions, highlighting the considerable strain on healthcare resources. 5 In 2018, nearly 5% of adults in the US had a confirmed COPD diagnosis with an estimated three-fourths of adults with COPD remaining undiagnosed, underscoring the burden of the disease.6–8
High symptom burden, including severe dyspnea, wheezing, chronic cough, sputum, and chest tightness are common in patients with COPD.9,10 However, as a heterogenous condition, each patient experiences varying COPD symptoms. Moreover, patients with COPD often experience exacerbations (i.e., acute worsening of COPD symptoms) that contribute to disease progression.1,11,12 As a result of this high clinical burden, COPD has been shown to have a substantial impact on health-related quality of life (HRQoL), even among patients with milder severity.13–16 Thus, the primary goals of COPD maintenance treatment are to reduce symptoms, decrease the risk of exacerbations, and improve health status.1,17
The Global Initiative for Chronic Obstructive Lung Disease (GOLD) strategy provides recommendations for medications for COPD management, including inhaled bronchodilators (e.g., long-acting β2-agonists [LABAs] or long-acting muscarinic receptor antagonists [LAMAs]) as single or dual maintenance therapy depending on symptom severity. 1 Escalation to triple therapy (LABA/LAMA + inhaled corticosteroids [ICS]) should be considered for patients who have eosinophil levels ≥300 cells/µL and experience multiple or severe exacerbations (≥2 moderate or ≥1 leading to hospitalization), as well as for patients with eosinophils ≥100 cells/μL who experience ongoing exacerbations despite dual bronchodilator therapy. 1 The benefits of ICS therapy for exacerbation prevention have been shown to have a continuous relationship with blood eosinophil count, and uncertainty around effects at eosinophils <100 cells/μL have led to existing threshold recommendations to help identify patients likely to experience clinical benefit with ICS.1,18–21 Real-world data indicates that ICS are frequently used in a wide range of patients with COPD,17,22,23 possibly due to the lack of other available anti-inflammatory therapies.
Prior studies have used medical records and claims data to evaluate the real-world management of patients with COPD and identify gaps in treatment recommendations.23–25 The aims of this study were to build upon these findings and further evaluate COPD management through the lens of different clinician groups, as well as to assess the clinician perceived impact of COPD on patients’ quality of life and how the disease burden is perceived to change across the spectrum of COPD severity. To achieve these objectives, this study utilized a quantitative questionnaire and case report form submitted by clinicians based on anonymized patient medical record data, enabling estimation of patients’ GOLD classification, symptoms, physical activity, exacerbation history, and treatment history. The review also allowed for identification of differences in patient characteristics and treatment patterns across US-based pulmonologists, internal/family medicine physicians, and nurse practitioners (NPs)/physician assistants (PAs).
Methods
Study design
A 45-min quantitative questionnaire was fielded between April 2023 to May 2023 with US-based pulmonologists, internal/family medicine physicians, NPs, and PAs who currently manage and treat patients with COPD. Respondents were compensated for the time spent in the study. The survey collected information on clinicians, including their current prescribing habits, behaviors, attitudes, demographic information, and patients’ characteristics. Since all patient chart data were de-identified and this study was conducted as market research with clinicians, the data are not defined as human subject research per the Department of Health & Human Services Common Rule for the protection of human subjects in research [45CFR 46.102(e)(1)].
This study captured responses from a total of 175 clinicians across the US (Northeast [22%], South [35%], Midwest [22%], West [21%]). To qualify for this study, respondents were required to have 3-35 years of clinical experience and spend at least 80% of their time in direct patient care. All pulmonologists and internal/family medicine physicians were board certified. Pulmonologists and internal/family medicine physicians were required to treat or manage a minimum of 60 and 30 patients with COPD in an average month, respectively. NPs and PAs were not required to be affiliated with a pulmonology office but needed to treat or manage a minimum of 30 patients with COPD in an average month.
For study participation, clinicians were required to review four current medical records of patients with COPD and answer survey questions based on this review. All patient-related data were submitted anonymously. To qualify, reviewed records were required to be for patients actively managed and/or evaluated by that clinician over the prior month, and for whom the clinician was the primary treatment decision-maker. Patients must have been diagnosed with COPD and have been receiving maintenance therapy for COPD. At least one of the four patients selected for medical record review was required to currently be prescribed dual bronchodilator or triple therapy for maintenance treatment of COPD. For the purposes of this study, internal/family medicine physicians have been grouped together and NP/PAs have been grouped together.
Statistical analysis
Descriptive statistics were used to evaluate the patients’ and clinicians’ characteristics and clinician prescribing behaviour using means, medians, maximum/minimum ranges, and frequencies. A 95% confidence interval was used for statistical comparisons between subgroups for study outcomes. A t-test with False Discovery Rate (FDR) adjustment was conducted for all variables. Specifically, the FDR adjustment was applied to any comparison in the study when more than two groups were compared. All statistically significant differences were reported at α = 0.05 with no adjustment for multiple comparisons.
Outcome variables were as follows: • Patient demographic data and characteristics such as age, gender, smoking history, relatives with COPD, employment, physical activity, comorbidities, number of exacerbations in the prior year, COPD phenotypes (emphysema, chronic bronchitis, both or none), and COPD severity according to severity of airflow obstruction
1
(based on post-bronchodilator FEV1) • Clinician-perceived patient symptom burden such as dyspnea, wheezing, chronic cough, sputum, and chest tightness • Clinician-perceived impact of 1) COPD on overall quality of life (1-7 scale) and 2) COPD symptom severity on quality of life (0-7 scale) • Latest COPD maintenance treatment prescribed and the clinician’s rationale for the prescription
Results
Patient demographics and characteristics
Patient characteristics.
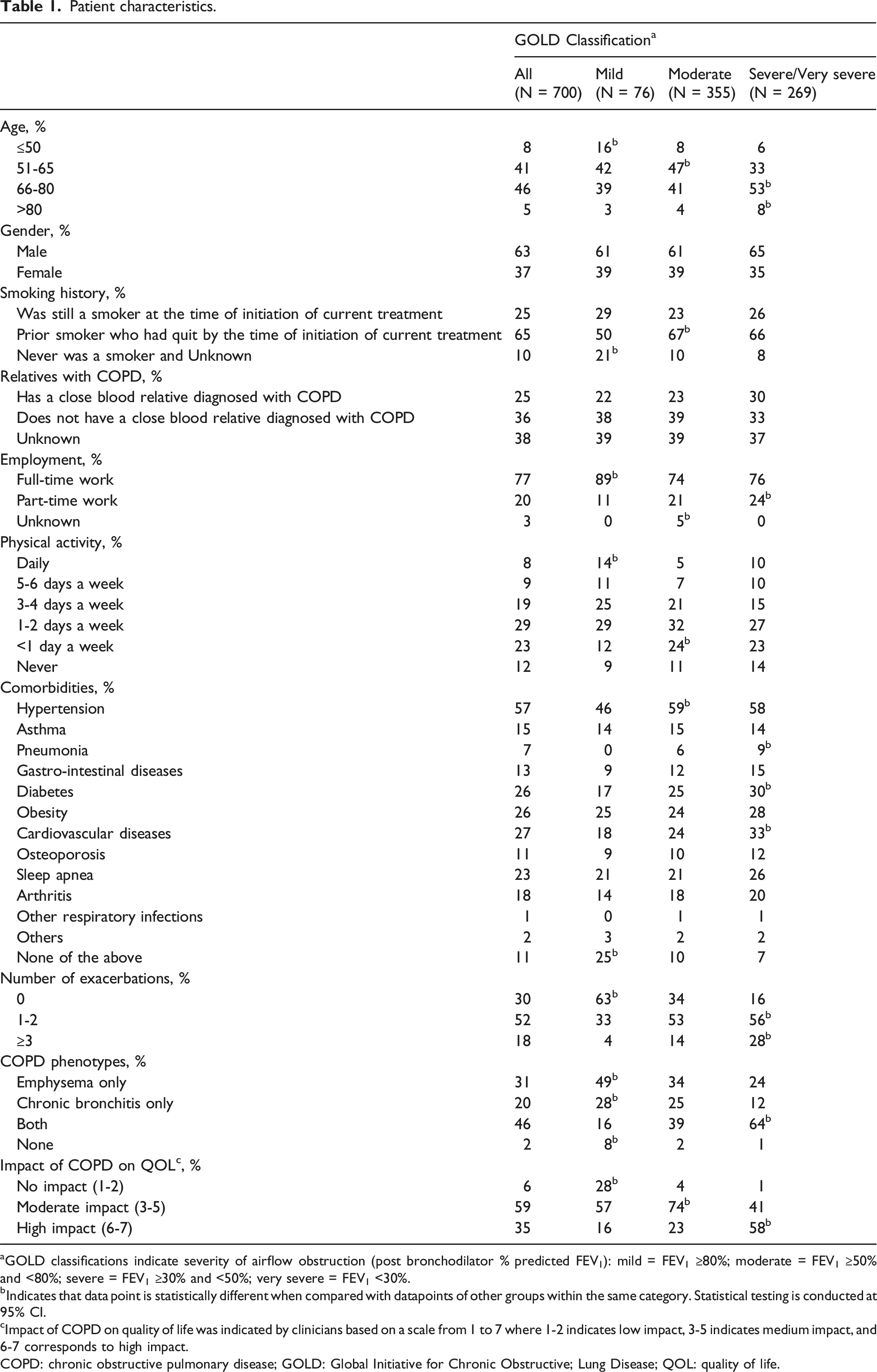
aGOLD classifications indicate severity of airflow obstruction (post bronchodilator % predicted FEV1): mild = FEV1 ≥80%; moderate = FEV1 ≥50% and <80%; severe = FEV1 ≥30% and <50%; very severe = FEV1 <30%.
bIndicates that data point is statistically different when compared with datapoints of other groups within the same category. Statistical testing is conducted at 95% CI.
cImpact of COPD on quality of life was indicated by clinicians based on a scale from 1 to 7 where 1-2 indicates low impact, 3-5 indicates medium impact, and 6-7 corresponds to high impact.
COPD: chronic obstructive pulmonary disease; GOLD: Global Initiative for Chronic Obstructive; Lung Disease; QOL: quality of life.
Table 1 depicts patients’ characteristics according to disease severity. There was a directional trend towards greater disease severity with advancing age. While the proportion of patients with COPD under 50 years old was low, significantly more patients with Mild COPD were ≤50 years old, whereas a greater proportion of patients with Severe/Very Severe COPD were between 66 and 80 years of age and >80 years old. In total, 63% of patients were male. The majority of patients were prior smokers who had quit before initiation of their current treatment (65%). However, a greater percentage of patients with Mild COPD had never smoked, were employed full-time, or were physically active on a daily basis.
Comorbid disease burden was lowest among patients with Mild COPD, possibly due to their younger age (Table 1). In contrast, patients with Severe/Very Severe COPD had significantly higher rates of multiple comorbid conditions, including cardiovascular diseases, diabetes, and history of pneumonia. The number of exacerbations that patients experienced over the past year also increased significantly with greater disease severity (Table 1). The majority of patients with Mild COPD did not have any exacerbations in the past year (63%), whereas more than half of patients with Severe/Very Severe COPD had 1 to 2 exacerbations (56%), with nearly one-third (28%) experiencing ≥3 exacerbations. A significantly higher proportion of patients with Severe/Very Severe disease (64%) also had a COPD phenotype as classified by the clinician that included both emphysema and chronic bronchitis than patients with Moderate (39%) or Mild (16%) disease.
Impact of symptoms on patient quality of life. a

aImpact of COPD symptom severity on quality of life was indicated by clinicians based on a scale from 0 to 7 where 0-2 indicates ‘did not experience symptom’/low impact, 3-5 indicates medium impact, and 6-7 corresponds to high impact.
bIndicates that data point is statistically different when compared with datapoints of other groups within the same category. Statistical testing is conducted at 95% CI.
GOLD: Global Initiative for Chronic Obstructive Lung Disease.
Maintenance treatment prescribing patterns among clinicians
As shown in Figure 1, patient segmentation according to COPD severity varied across clinicians. Pulmonologists managed a significantly higher proportion of patients with Severe/Very Severe COPD than internal/family medicine physicians and NP/PAs across the patient journey, both at the time of initial COPD diagnosis (26% vs 17% and 15%, p = 0.008) and at the time of the survey (44% vs 30% and 32%, p = 0.001). In contrast, internal/family medicine physicians and NP/PAs managed significantly more patients classified as having Mild COPD at initial diagnosis (33% and 34% vs 20%, p = 0.0002) and Moderate COPD at the time of the survey (59% and 53% vs 47%, p = 0.02) as compared to pulmonologists. Pulmonologists also managed a greater percentage of patients with dyspnea that was perceived to exert a high impact on their quality of life, although differences were not statistically significant. Patient characteristics across clinicians. Characteristics of the patient records submitted by all clinicians (n = 175), and across pulmonologists (n = 100), internal/family medicine physicians (n = 45), and NP/PAs (n = 30). Numerical markers (1, 2, 3) indicate that a metric in this group is significantly higher than one or more of the comparison groups represented numerically as pulmonologists (1), internal/family medicine physicians (2), or NP/PAs (3). aImpact of COPD symptom severity on quality of life was indicated by clinicians based on a scale from 0 to 7, where 0-2 indicates ‘did not experience symptom’/low impact, 3-5 indicates medium impact, and 6-7 indicates high impact. COPD: chronic obstructive pulmonary disease; GOLD: Global Initiative for Chronic Obstructive Lung Disease; NP/PA: nurse practitioner/physician assistant.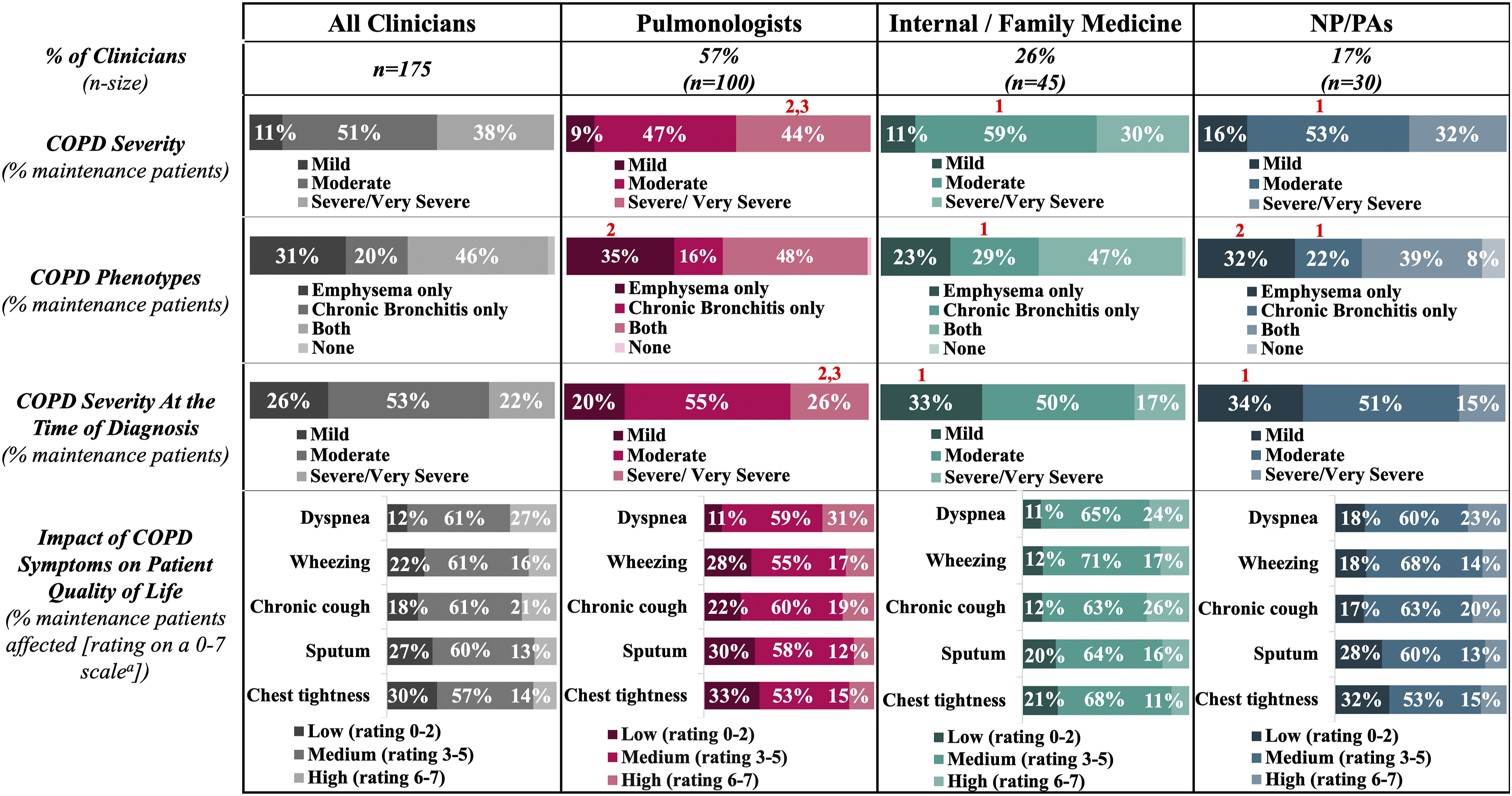
Current maintenance treatment patterns according to clinician type are illustrated in Figure 2. Across all respondents, ICS-containing therapies were the most frequently utilized, with 65% of patients treated with ICS. LABA/LAMA/ICS triple therapy was utilized in 49% of patients with COPD, with no significant differences across clinicians. A significantly higher proportion of pulmonologists prescribed LAMA/LABA dual therapy than internal/family medicine physicians and NP/PAs (24% vs 14% and 9%, p = 0.004), whereas internal/family medicine physicians and NP/PAs had significantly higher utilization of LABA/ICS than pulmonologists (19% and 28% vs 9%, p = 0.001). Oral phosphodiesterase-4 (PDE4) inhibitors were prescribed for 3%–7% of patients. Other COPD medications (e.g., bronchodilator and ICS monotherapy, dupilumab) were utilized in <10% of patients. Across all clinicians, the two most influential factors reported in treatment decision-making were severity of COPD symptoms (26%) and exacerbation frequency (17%). Current COPD maintenance treatment preferences across clinicians. Current maintenance therapies prescribed to patients with COPD, and reasons for prescribing (ranked as #1 reason), across all clinicians (n = 175), and by pulmonologists (n = 100), internal/family medicine physicians (n = 45), and NP/PAs (n = 30). Across current COPD maintenance treatments, 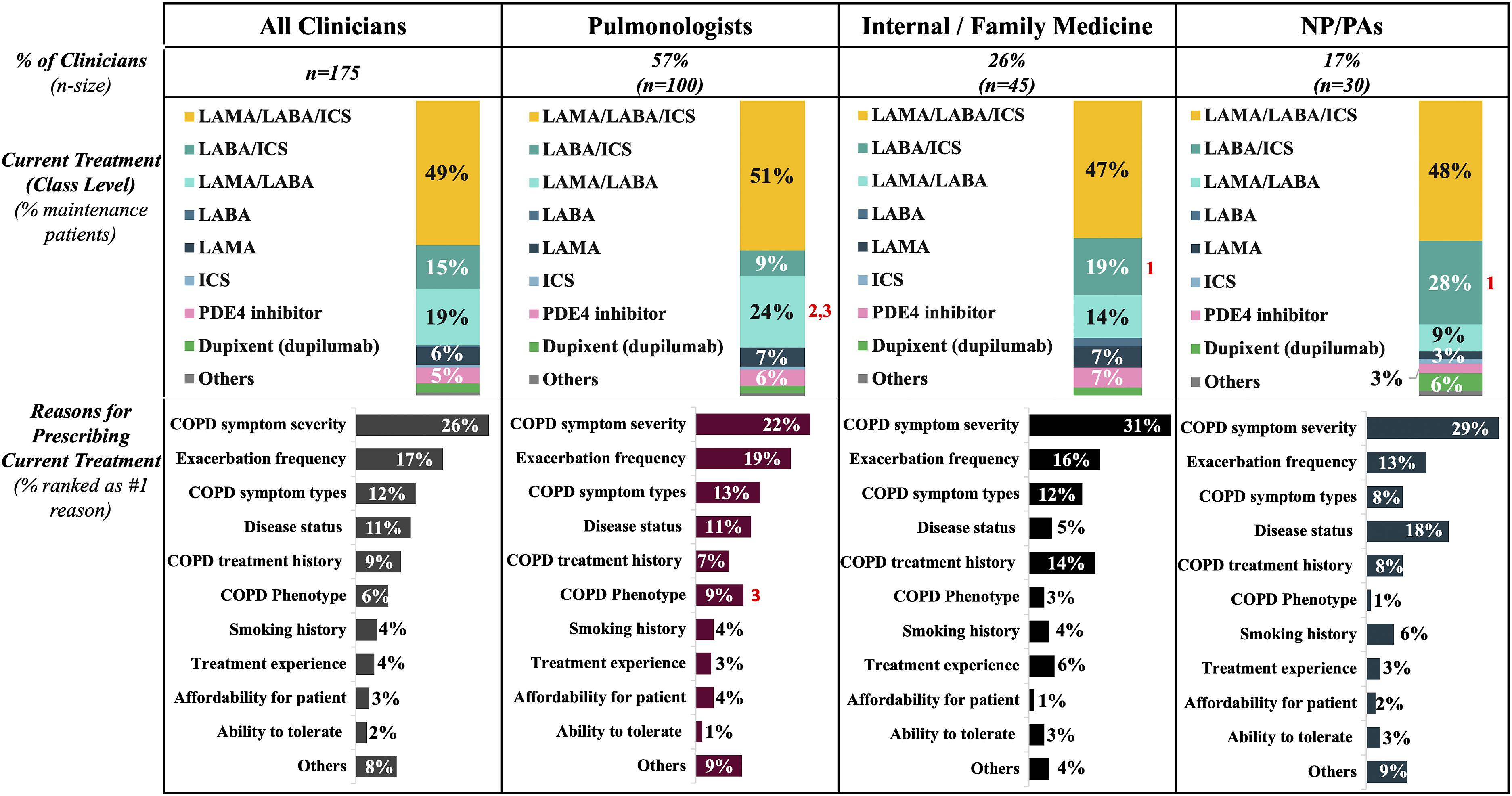
Clinicians were also asked to report any prior maintenance treatments that patients may have received. In total, 71% of patients (n = 497) had received at least one prior maintenance treatment, 27% (n = 189) had received at least two prior treatments, and 11% (n = 74) had received at least three prior treatments. As illustrated in Figure 3(a), management of patients with COPD is complex, regardless of clinician type, with patients starting and transitioning to multiple different treatments throughout the course of their care. Across all clinicians, respondents reported prescribing a variety of first-line treatments, including LABA/ICS, ICS monotherapy, LAMA monotherapy, LAMA/LABA, and LABA monotherapy. LAMA/LABA/ICS triple therapy was not used frequently as a first line treatment, but rather, patients were sequenced to these after one or two prior treatments. PDE4 inhibitors, while making up a small proportion of the overall therapies, were typically reserved as a second- or third-line therapy for those patients who were previously treated with LAMA/LABA/ICS triple therapy. Figure 3(b)–(d) depicts the variability in prescribing sequence across pulmonologists (Figure 3(b)), internal/family medicine physicians (Figure 3(c)), and NP/PAs (Figure 3(d)). COPD treatment journey across clinicians. Sequencing of COPD maintenance treatments across (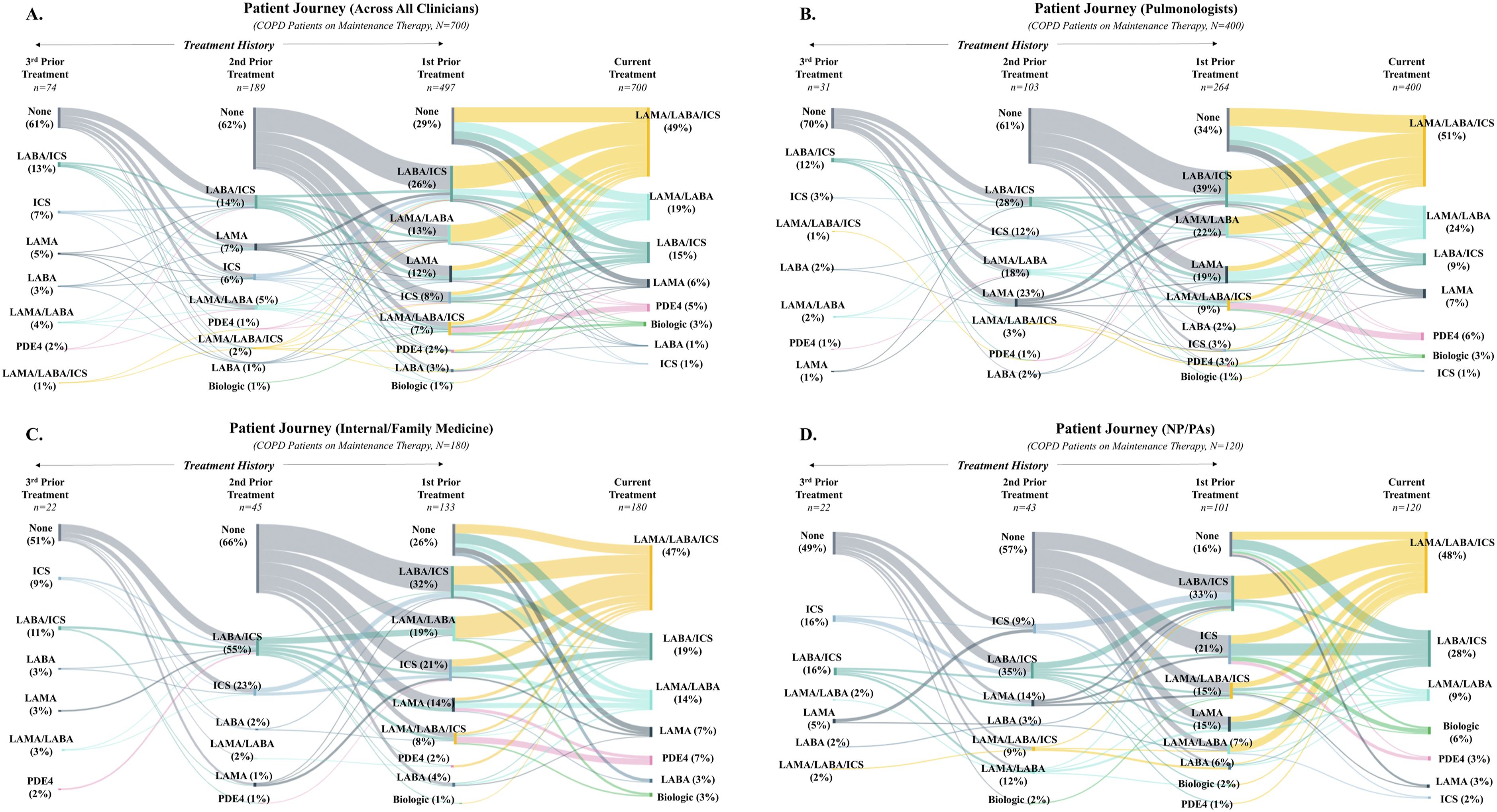
As shown in Figure 4, maintenance COPD treatment switch patterns were similar across clinician groups. Regardless of designation, clinicians reported that most of their patients had 0 or 1 treatment switches over the past year. Pulmonologists, internal/family medicine physicians, and NP/PAs also had similar reported behaviors regarding device versus treatment switches, with the majority changing either the device or the treatment only, rather than both the device and treatment simultaneously. COPD treatment switching across clinicians. Percentage of clinicians that had 0 – 4+ treatment switches and their reasons for switching (e.g., for new device only, treatment only, both device and treatment) across pulmonologists (n = 100), internal/family medicine physicians (n = 45), and NP/PAs (n = 30). There were no significant differences between clinician type in number of treatment switches or type of switch (device, treatment, or both) at 95% CI. COPD: chronic obstructive pulmonary disease; NP/PA: nurse practitioner/physician assistant.
Discussion
This study captured real-world data on disease burden and current management of patients with COPD. Our results confirm the substantial impact of COPD, particularly for patients with Severe/Very Severe disease, including frequent exacerbations and high symptom burden. This study also reveals there are notable differences in patients’ characteristics and COPD treatment patterns across clinicians.
In the present study, differences in clinician-perceived symptom burden across COPD severity groups were an important determinant of quality of life. Patients with Severe/Very Severe disease experienced a significantly higher impact from all COPD symptoms assessed than patients with Mild or Moderate disease. Dyspnea was considered by clinicians to have the greatest effect on quality of life, which is consistent with prior literature confirming an inverse correlation between the degree of dyspnea and HRQoL in COPD.13,26–28 Our data revealed that for patients with severe disease, each COPD symptom exerted a significant additional influence on their overall health status. This is a meaningful concern given that patients with COPD can experience >10 symptoms of their disease at one time.29,30 In addition, although the burden of COPD was highest among patients with more severe disease, quality of life for all patients in our study was perceived to be impacted, regardless of disease severity. Importantly, our findings are consistent with patient-reported literature describing the substantial impact of COPD on health-related quality of life.13,31,32
An important consideration of our findings is whether differences in the types of patients that clinicians managed resulted in differences in prescribing approach and/or treatment patterns. Our results indicate broad ICS usage among US-based clinicians. Many patients with COPD do not appear to fit the typical criteria for triple therapy; in a prior retrospective cohort analysis of US patients, only 11% had ≥2 exacerbations or an exacerbation related hospitalization and blood eosinophil levels ≥300 cells/µL. 33 Given that pulmonologists in our study treated a greater proportion of patients with Severe/Very Severe COPD who experience frequent exacerbations, this may account for their high use of triple therapy. Indeed, COPD symptom severity was the primary driver of prescribing behavior across all clinicians. It is also possible that our findings reveal deviations from the GOLD strategy due to lack of awareness of current recommendations. Data from several recent studies have also indicated similar divergence from GOLD recommendations for COPD treatment in the US.17,34 We did not collect data on eosinophil counts making it difficult to comment on adherence to clinical best practice even in those patients with frequent exacerbations across clinician groups.
Although utilization of triple therapy (LAMA/LABA/ICS) was similar across clinicians, marked differences emerged for dual therapies. Internal/family medicine physicians and NP/PAs prescribed LABA/ICS to a significantly higher proportion of their patients than pulmonologists, who favored use of dual bronchodilator therapy (LAMA/LABA). Indeed, similar prescribing patterns have been observed between pulmonologists and primary care physicians (PCPs) previously. In a survey of 171 US-based pulmonologists and PCPs managing patients with COPD, Mannino et al. found that PCPs more frequently prescribed LABA/ICS treatment, whereas pulmonologists more commonly prescribed dual bronchodilation and triple therapy. 34 In fact, PCPs were more likely to prescribe LABA/ICS irrespective of whether the patient was treatment-naïve, had exacerbation history/risk, or had certain COPD symptoms (e.g., severe dyspnea). 34 In the discussion of their findings, Manino et al. suggest that PCPs may be more likely to prescribe LABA/ICS as they may not have regular access to pulmonary function testing or patient-reported outcomes for disease stratification and/or may feel uncertain in applying symptoms or exacerbation history to guide treatment choice. 34 It is also possible that differences in the prevalence of co-existent asthma accounted for some of the treatment differences across providers in our study. It will be important in future studies to further explore potential factors contributing to LABA/ICS treatment among providers to assess appropriate use of ICS in patients with COPD.
Beyond current treatment patterns, our results also revealed considerable variability and heterogeneity in treatment history and sequencing across clinicians. This is unsurprising given that COPD symptom severity and exacerbation frequency were reported to be the most important motivations for treatment decisions across all respondents. As a result, treatment sequencing appeared to be highly individualized across patients.
Taken together, our findings have important implications for disease management. Since COPD is a chronic and progressive condition, the primary goals of maintenance treatment are to reduce symptoms, decrease the risk of exacerbations, and improve health status. 1 Yet, COPD was reported to have a moderate to high impact on quality of life for 94% of patients in our study. An important point to underscore is that half of patients included in this study were receiving maximal inhaled treatment under current standard of care (LAMA/LABA/ICS triple therapy), and nearly one-third of patients had received at least two prior treatments beyond their current maintenance therapy. For patients who experience persistent symptoms and exacerbations despite triple therapy, treatment options are severely limited. 1
Although this study captured new insights on COPD burden and treatment practices across different clinicians, it has several potential limitations. First, the sampling was more heavily weighted to pulmonologists than internal/family medicine physicians and NP/PAs. Data were not collected on NP/PAs’ site of practice, e.g. pulmonology clinics versus primary care sites. Additionally, respondents were required to submit data from at least one medical record of a patient currently on dual or triple therapy, possibly resulting in a sample that is not broadly generalizable to all clinicians. This sample was also limited to clinicians who were willing and able to participate in research. Clinicians were also asked to submit anonymized medical records of patients treated within the past 1 month, which may not have been a direct representation of their typical patient load.
Lastly, the present study was unable to capture all potential factors which may have impacted treatment decisions and prescribing behaviors of clinicians, such as infectious history and/or utilization of non-pharmacologic approaches to care (e.g., pulmonary rehabilitation). Therefore, while our data provides insights into COPD maintenance therapy patterns across different providers, we cannot determine the underlying rationale for individual treatment decisions. Despite these limitations, our findings are in line with previously published research and help to further elucidate the patient’s treatment journey across different clinician groups.
Conclusions
This research revealed that clinicians consider COPD to have a substantial adverse impact on patient quality of life across the disease spectrum. Furthermore, this study identified distinct differences in treatment patterns and patient demographics among US-based pulmonologists, internal/family medicine physicians, and NP/PAs. Use of ICS-containing regimens, particularly triple therapy, was higher than expected based on current GOLD recommendations, possibly reflecting implementation gaps and/or a significant need for additional therapies to allow treatment escalation due to insufficient COPD symptom management.
Footnotes
Acknowledgments
Medical writing assistance was provided by Emily Sharpe, PhD (Trinity Life Sciences).
Ethical statement
Author contributions
All authors made significant contributions to the study conception and design, as well as the analysis and interpretation of the data. SMR and MQAR drafted the manuscript, and all authors critically revised the manuscript. All authors read and approved the final manuscript.
Funding
Support for this research and development of this manuscript was funded by Verona Pharma, Raleigh, NC, USA.
Declaration of conflicting interest
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SMR and MQAR are employed by Trinity Life Sciences and received consulting fees from Verona Pharma. MC: American Lung Association, AstraZeneca, Gala Therapeutics, Genentech, GSK, NIH, Novartis, PCORI, Pulmatrix, sanofi-aventis, Shionogi, Theravance Biopharma – research support; Allakos, Amgen, Arrowhead Pharmaceuticals, Genentech, GSK, Merck, Novartis, OM Pharma, Pfizer, Pioneering Medicines, sanofi-aventis, Teva – consultant; Amgen, AstraZeneca, Genentech, Regeneron Pharmaceuticals Inc., Sanofi, Teva – speaker fees; Aer Therapeutics – royalties. BPY has received consulting fees and served on advisory boards related to COPD for Boehringer Ingelheim, GlaxoSmithKline, TEVA and AstraZeneca and travel support for presentations related to COPD from Boehringer Ingelheim and GlaxoSmithKline. She has received writing support for manuscript preparation from GlaxoSmithKline and AstraZeneca outside this work. KA and ALD are employees of Verona Pharma and may own stock.
Data Availability Statement
An anonymized data set used and/or analyzed for the current study may be made available from the corresponding author upon reasonable request.