
Abstract
Introduction
Chronic obstructive pulmonary disease (COPD) is a heterogeneous lung condition characterized by chronic respiratory symptoms (dyspnoea, cough, sputum production and/or exacerbation) due to airway (bronchitis, bronchiolitis) and/or alveoli (emphysema) abnormalities that cause persistent, often progressive, airflow obstruction. 1 COPD is a leading cause of morbidity and mortality worldwide. 2
People living with COPD are less physically active than healthy adults 3 and are also less active than individuals living with a range of other non-communicable diseases.4,5 A low physical activity level is associated with an increased risk of hospitalization and is the strongest predictor of all-cause mortality in individuals with COPD.6,7 The World Health Organization (WHO) defines physical activity as any bodily movement involving skeletal muscles that requires energy expenditure. 8 Physical activity is commonly classified according to energy expenditure as light (<3 metabolic equivalents of tasks [METs]), moderate (3–5.9 METs), or vigorous (≥6 METs).9–11 Importantly, individuals with COPD also maintain longer periods of sedentary behaviour, which is another factor associated with hospitalization and mortality in this population. 12 Sedentary behaviour is defined as any waking behaviour characterized by an energy expenditure ≤1.5 METs while sitting, reclining, or lying. 13
Individuals with COPD who exhibit low physical activity in daily life (PADL) and spend a high amount of time in sedentary behaviour present a high risk of all-cause and cardiovascular mortality. 14 In addition, these individuals present poorer clinical COPD outcomes, including more severe airway obstruction, worse dyspnoea, and reduced exercise capacity.15–17 Previous studies have suggested several cut-offs for daily steps, such as 4300, 18 4580, 19 and 5000 20 steps/day. Walking fewer than 5000 steps/day indicates a sedentary lifestyle in clinically stable individuals with moderate to severe COPD. 18 Other authors reported that taking fewer than 4580 steps/day is associated with severe physical inactivity in individuals with COPD and is considered a risk factor for adverse outcomes. 19 However, Nyssen et al. 21 showed that this cut-off was not sensitive for identifying predictors of mortality in this population. Another study demonstrated that a cut-off of 4300 steps/day might be more appropriate for identifying symptomatic individuals with moderate to severe COPD who would benefit from reducing sedentary behaviour or increasing PADL. 18
Despite all the previous evidence associating physical inactivity with hospitalization and mortality, the levels of physical activity related to health status in individuals with COPD remain unknown.7,22,23 This information could provide practical clinical information about patients’ health outcomes. Therefore, this study aimed to explore the associations between preestablished daily step count cut-offs and health status, dyspnoea, and psychosocial distress in individuals with COPD.
Methods
Participants
Individuals with COPD diagnosed according to the Global Initiative for Chronic Obstructive Lung Disease (GOLD) 24 criteria were invited to participate. The participants were previously informed about the study objectives and procedures; only those who signed the informed consent form were included. The inclusion criteria were individuals who were clinically stable (no exacerbation in the last 4 weeks) or those presenting cardiovascular or musculoskeletal limitations in performing physical activity. Those who were unable to understand the proposed assessments were excluded. Clinical and medical history was confirmed from the patient’s medical records. The study followed the principles of the Declaration of Helsinki, 25 and the Research Ethics Committee of the Hospital approved the study (#94403018.6.0000.0068).
Experimental design
This cross-sectional study included individuals consecutively recruited from a tertiary care hospital during routine medical consultations between July 2019 and April 2024. The assessments were carried out in two visits with an 8-day interval between them. At the first visit, the following questionnaires were completed: the modified dyspnoea scale Medical Research Council (mMRC), the COPD Assessment Test (CAT) or Clinical Control Questionnaire (CCQ), the Chronic Respiratory Questionnaire (CRQ), and the Hospital Anxiety and Depression Scale (HADS). After completing the questionnaires, the participants received an accelerometer and were instructed not to modify their PADL during the assessment week. After 8 days, the participants returned the accelerometer in person at the hospital.
Outcomes and outcome measures
Lung function spirometry
The spirometric data were obtained by consulting the medical records to confirm the COPD diagnosis. Spirometry was performed according to the recommendations of the American Thoracic Society and European Respiratory Society (ATS/ERS). 26 The forced expiratory volume in 1 s (FEV1) and FEV1/the forced vital capacity (FVC) ratio were expressed as percentages of the predicted values for the Brazilian population. 27
Dyspnoea
The mMRC is a unidirectional 0–4-point scale that assesses daily activities that provoke dyspnoea. 28 It has also been used in clinical practice to categorize COPD symptomatic burden and provide useful information about COPD-induced disability. 1 In addition, it is a parameter that can be used to recommend different therapies for patients with “less dyspnoea” (mMRC 0–1) and “more dyspnoea” (mMRC ≥ 2). 29
Health status
Health status was assessed using either the COPD Assessment Test (CAT) or the Clinical COPD Questionnaire (CCQ). The CAT score assesses physical symptoms (cough, phlegm, chest tightness, breathlessness), activity limitations, energy and confidence in leaving home, and sleep quality. CAT has a total maximum score of 40 points (maximum impairment). Higher scores indicate worse health status. 30 The CCQ is a valid, reliable, and responsive instrument for detecting clinical changes in people with COPD. A higher score represents poorer clinical control. 31
Health-related quality of life (HRQoL)
The Chronic Respiratory Questionnaire (CRQ) is a validated instrument that provides a valid and reliable self-reported measure of HRQoL in individuals with COPD. The CRQ comprises four domains: dyspnoea, fatigue, emotional function, and mastery. Higher scores indicate better HRQoL. 32
Psychosocial distress
Psychosocial distress was assessed by the Hospital Anxiety and Depression Scale (HADS). The HADS consists of 14 items divided into two subscales (seven questions for anxiety and seven for depression). Each item is scored from 0 to 3, with a maximum score of 21 points for each subscale. A score equal to or greater than 8 on each subscale suggests a possible clinical diagnosis of either anxiety and/or depression. 33
Physical activity and sedentary behaviour
A triaxial accelerometer was used to objectively assess physical activity in daily life (PADL) and sedentary behaviour (ActiGraph model GT3X, ActiGraph LLC, Pensacola, FL, USA). The participants were instructed to wear the device in a belt around the waist for seven consecutive days during waking hours and remove it overnight and during water-related activities. The device was initialized to collect raw data at a sampling rate of 30 Hz, and the data were subsequently processed into 60-s epochs using ActiLife software (version 6.9.5; ActiGraph, Pensacola, FL, USA). The number of steps per day, time spent (minutes/day) in sedentary behaviour (defined as <100 counts/minute), and time spent in moderate to vigorous physical activities (MVPA, defined as >1952 counts/minute) were calculated. 34 Counts are a unit of measurement used by accelerometers to represent the intensity of movement and are calculated on the basis of changes in velocity over time within a defined time interval (epoch), typically between 10 and 60 s. 35
Data from at least five valid days, with a minimum of 8 h of recorded activity per day, were included in the analyses.36–38 Non-wear time was identified using the algorithm proposed by Troiano et al. 39
The participants were divided into active and inactive groups according to the number of steps per day on the basis of each previously described cut-off point (4300, 18 4580, 19 and 5000 20 steps/day).
Statistical analysis
Statistical analyses and data summaries were performed via GraphPad Prism version 9.1.1 for Mac OS X (GraphPad Software, Boston, Massachusetts, USA). The Kolmogorov‒Smirnov test was applied to assess the normality of the data. Data are reported as the means for parametric distributions, the medians for nonparametric distributions, mean differences with 95% confidence intervals (CIs), and percentages. The t-test or Mann–Whitney U test was used to compare groups when appropriate, whereas the chi-square test for proportions was employed to analyse differences between the active and inactive groups. Multiple linear forward regression analysis was performed with independent variables (age, FEV1, and the average number of steps per day) considered for inclusion if their linear correlation with the outcome (CAT score) had a p-value <0.2. Multiple linear regression analysis was performed to identify the independent factors associated with the CAT score (dependent variable); the independent variables analysed were age, FEV1, and step/day. The variance inflation factor (VIF) was calculated to assess multicollinearity among the independent variables in the regression model, ensuring that predictor variables did not exhibit collinearity that could bias the results, and a VIF ≥2.5 was considered to indicate considerable collinearity. 40 The likelihood (odds ratio) of having worse dyspnoea, health status, anxiety, and depression symptoms was calculated by the cut-off values of steps per day.
To further evaluate the ability of the step count to discriminate poor health status, receiver operating characteristic (ROC) curve analysis was performed with CAT scores ≥18 as the classification criterion. The area under the curve (AUC), standard error, 95% confidence interval (CI), and p value were calculated. The optimal threshold was identified using the Youden index, which maximizes the overall rate of correct classifications (sensitivity + specificity −1). 41 Given that false-negatives may have greater clinical implications in this context, we prioritized sensitivity when selecting the threshold. The minimum specificity constraint of 50% was maintained to apply clinical applicability, as recommended when trade-offs between sensitivity and specificity must reflect diagnostic priorities.42,43 A p-value <0.05 was considered to indicate statistical significance.
Results
Participant characteristics
Characteristics of COPD individuals based on the stratification of daily step counts.
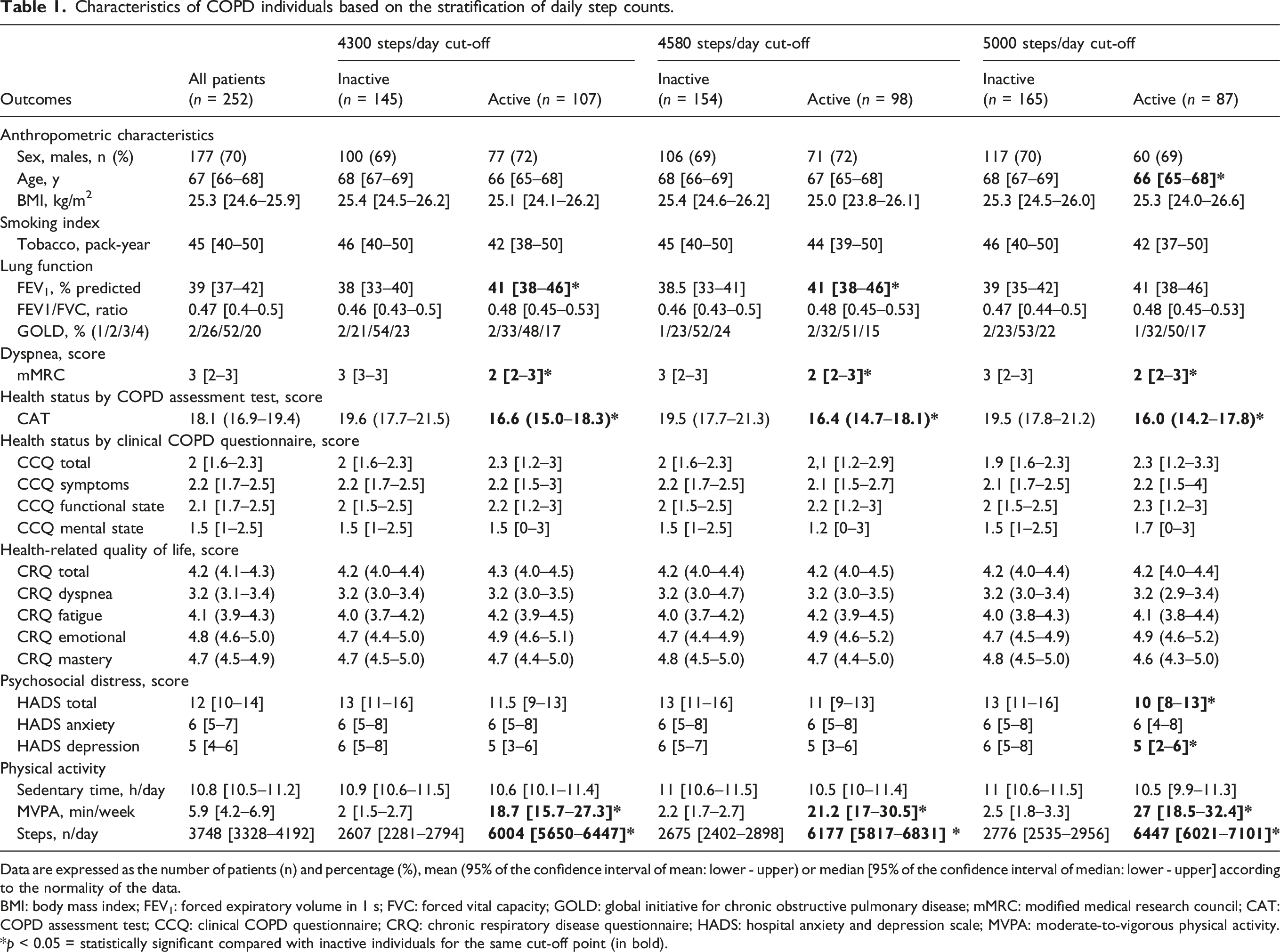
Data are expressed as the number of patients (n) and percentage (%), mean (95% of the confidence interval of mean: lower - upper) or median [95% of the confidence interval of median: lower - upper] according to the normality of the data.
BMI: body mass index; FEV1: forced expiratory volume in 1 s; FVC: forced vital capacity; GOLD: global initiative for chronic obstructive pulmonary disease; mMRC: modified medical research council; CAT: COPD assessment test; CCQ: clinical COPD questionnaire; CRQ: chronic respiratory disease questionnaire; HADS: hospital anxiety and depression scale; MVPA: moderate-to-vigorous physical activity.
*p < 0.05 = statistically significant compared with inactive individuals for the same cut-off point (in bold).
Lung function, dyspnoea, and health status
Lung function assessed by FEV1 (as a percentage of the predicted value), which was lower in the groups of individuals classified as inactive at the cut-off values of 4300 steps/day (p = 0.016) and 4580 steps/day (p = 0.011) than in the groups of active individuals, is shown in Table 1. However, this difference was not observed at the 5000 daily steps cut-off (p = 0.054). No difference was observed in the FEV1/FVC ratio between active and inactive individuals at any step count.
The odds ratio of dyspnea and health status according to daily step count cut-offs.
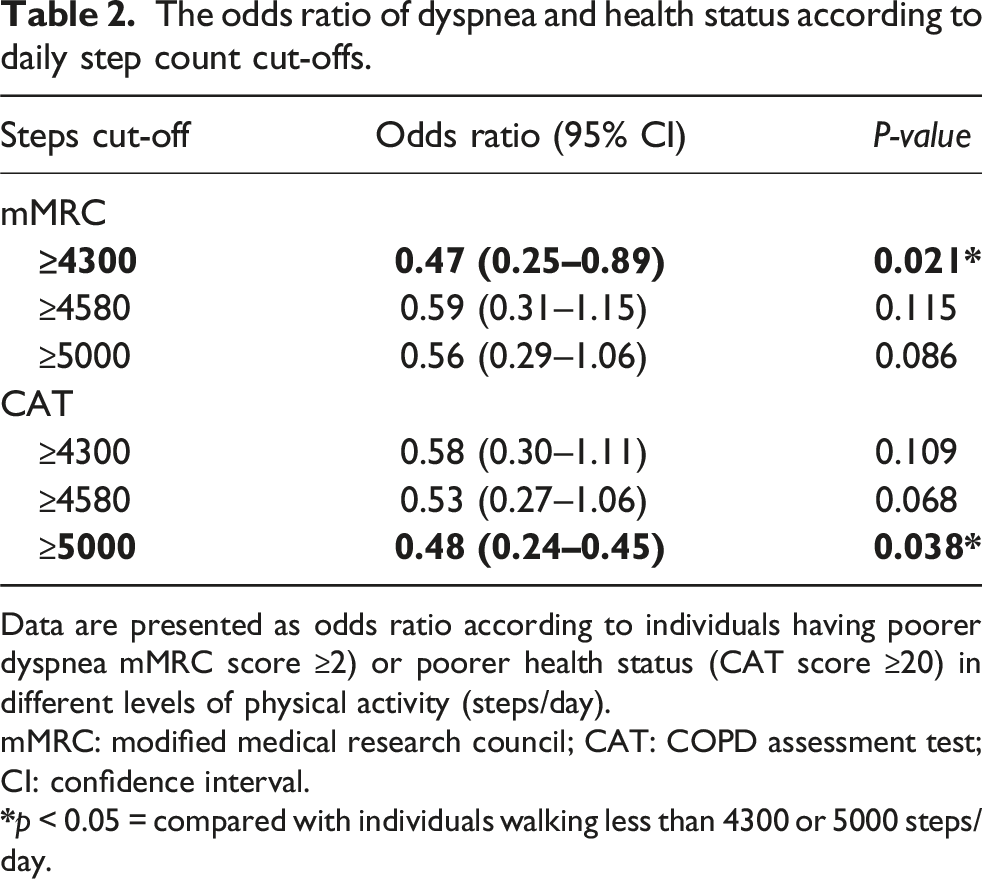
Data are presented as odds ratio according to individuals having poorer dyspnea mMRC score ≥2) or poorer health status (CAT score ≥20) in different levels of physical activity (steps/day).
mMRC: modified medical research council; CAT: COPD assessment test; CI: confidence interval.

Comparison of CAT scores across different daily step count cut-offs ((A) 4,300, p = 0.01; (B) 4,580, p = 0.01; (C) 5,000, p = 0.007). The dashed lines represent the cut-off point for the disease’s health impact. Data are expressed in mean with a 95% confidence interval. *p < 0.05 between inactive (lower steps/day: <4,300, <4,580, and <5000) and actives (higher steps/day: ≥4300; ≥4580; ≥5000) groups. CAT: COPD assessment test.
The ROC curve analysis for identifying individuals with poor health status (CAT ≥18) yielded an area under the curve (AUC) of 0.662 (standard error: 0.044; 95% CI: 0.574–0.750; p = 0.0007) (Figure 2). The optimal cut-off point was determined to be 4965 steps/day based on the highest Youden index, with a minimum specificity constraint of 50%. This threshold demonstrated a sensitivity of 72.7% and a specificity of 51.4%. Receiver operating characteristic (ROC) curve assessing the ability of daily step count to discriminate individuals with poor health status, defined as a COPD Assessment Test (CAT) score ≥18.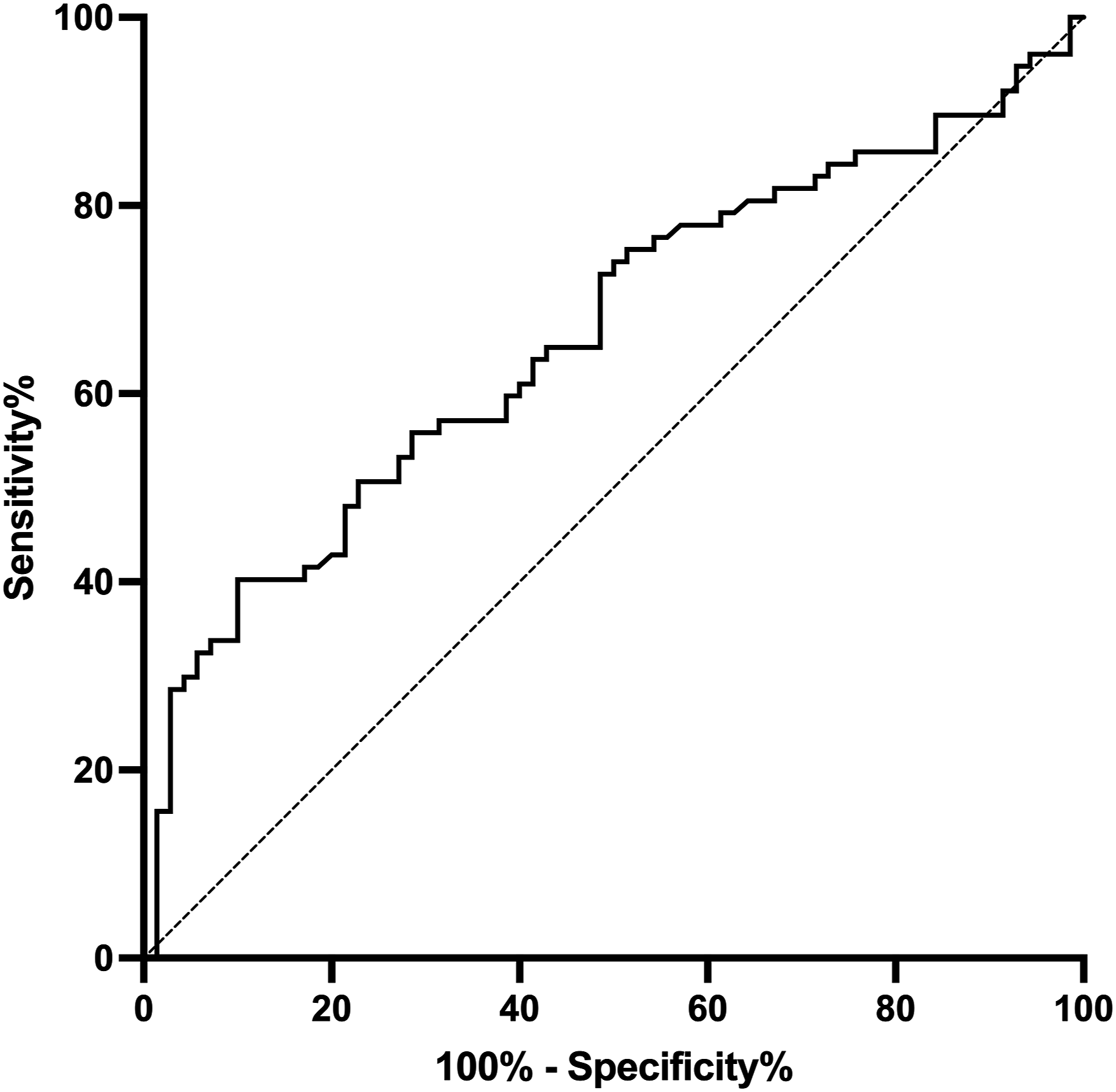
Psychological distress and HRQoL
The HADS total score indicates a low level of psychological distress in the total sample (Table 1). Table 1 and Figure 3 present the scores for anxiety and depression symptoms in each cut-off stratification. Compared with inactive participants, active participants, defined by a threshold of 5000 steps/day, presented lower HADS total scores (p < 0.03) and HADS-D scores (p = 0.04). Comparison of anxiety and depression symptoms scores across different daily step count cut-offs ((A) 4300; (B) 4580; (C) 5000). The dashed lines represent the cut-off point for presenting symptoms. Data are expressed as median and 95% confidence interval. *p < 0.05 between inactive (lower steps/day: <4300; <4580; <5000) and actives (higher steps/day: ≥4300; ≥4580; ≥5000) groups. (A) 4300 – anxiety, p = 0.474 and depression, p = 0.111; (B) 4580 – anxiety, p = 0.367 and depression, p = 0.067; (C) 5000 – anxiety, p = 0.210. HADS: hospital anxiety and depression scale.
The odds ratio of having anxiety and depression symptoms (HADS score) according to the classification of daily steps count cut-offs.

Data are presented as odds ratio according to individuals having poorer anxiety and depression symptoms (Hospital Anxiety and Depression Scale for anxiety or depression score ≥8) in different levels of physical activity (steps/day).
CI: confidence interval.
The HADS total score indicates a low level of psychological distress in the overall sample (Table 1). Table 1 and Figure 3 present the scores for anxiety and depression symptoms across each cut-off stratification. Compared to inactive participants, active participants—defined by a threshold of 5000 steps/day—showed lower HADS total scores (p < 0.03) and HADS-D scores (p = 0.04). Despite these differences observed in HADS total and HADS-D scores at the 5000 steps/day cut-off, when analyzed by symptom severity stratification (≥8 indicating the possible presence of anxiety/depression), no differences were found in the odds ratio for anxiety (p = 0.56) or depression (p = 0.05).
The HRQoL, assessed by the CRQ score for the subdomains of dyspnoea, fatigue, emotional function, and mastery, is detailed in Table 1. The step count thresholds were not discriminative for the CRQ total and domains.
Daily physical activity
All participants presented sedentary behaviour time (median of 10.8 h/day), with no between-group difference between inactive and active individuals at any cut-off threshold (steps/day: 4,300, p = 0.69; 4,580, p = 0.33; 5,000, p = 0.18). However, all three analysed cut-off points differed between inactive and active participants in daily MVPA (4300; 4580; and 5000 steps/day p < 0.001) and daily step counts (4300; 4580; and 5000 steps/day p < 0.001) (Table 1).
Potential confounding variables
Multiple linear regression analysis was performed via CAT, which is defined as the dependent variable, and age, FEV1 (in % pred), and the average number of steps per day were used as the independent variables. The regression model (p = 0.009) indicated that only the average number of steps per day was significantly associated with the CAT score (p = 0.033). Neither age, FEV1 or steps/day revealed no evidence of multicollinearity (VIF for Age = 1.09; FEV1% predicted = 1.17; Steps/day = 1.11) or violation of the normality of residuals (p > 0.05).
Discussion
To the best of our knowledge, this is the first study associating physical activity in daily life (PADL) (in steps per day) with health status in a large population of individuals with COPD. Our results revealed that 5000 steps per day is the best physical activity cut-off associated with better health status and less psychological distress. Additionally, we observed that walking 4300 steps per day is associated with lower dyspnoea severity.
Our results add novelty in that individuals who walk more than 5000 steps per day present better health status. Tudor-Locke et al. 20 reported that 5000 steps/day represent a transition between sedentary and active lifestyles, reinforcing the role of this cut-off point in improving overall health in healthy individuals. 44 In contrast to our results, Neale et al. 45 did not find an association between the 5000 steps per day cut-off and health status or distress symptoms (CAT and HADS) in individuals with COPD. A possible reason for the divergence between these studies may be related to the small sample size (n = 148) and the reduced number of active individuals (n = 18) in the study of Neals et al. 45 compared with our study, which had a larger sample size (n = 252) and a greater number of active participants (n = 87). Consequently, our study demonstrated a strong association between walking more than 5000 steps/day and good health outcomes.
Our results concerning the 4300 steps per day cut-off indicate that individuals with a PADL above this threshold experience less dyspnoea. Cheng et al. 18 demonstrated that 4300 steps per day is an optimal cut-off value for identifying a sedentary lifestyle in individuals with COPD who would benefit from specific guidance on reducing sedentary behaviour and increasing physical activity. However, the associations between the cut-off of 4300 steps per day and health-related clinical outcomes have never been investigated. Previous studies have demonstrated that this population’s mean number of steps per day is close to 4300.18,19,21 Our findings suggest that this number of steps per day is associated with reduced clinically relevant dyspnoea symptoms and can be an easily achievable cut-off. 18
With respect to the cut-off of 4580 steps, the average CAT and mMRC scores were higher in the inactive individuals than in the active individuals, similar to the other thresholds. However, no difference in health outcomes was observed between active and inactive individuals when this cut-off was used. The 4580 steps/day threshold was proposed by Depew et al., 19 and it is representative of a metabolic equivalent of <1.4 METs, 7 which identifies severely physically inactive individuals. This PADL has also been reported as the best individual predictor of all-cause mortality over 48 months in individuals with COPD. 7 However, in our study, this cut-off did not effectively discriminate health status, dyspnoea symptoms, or psychological distress, as did the other cut-off values investigated.
The lack of significant associations observed for the 4580 steps/day threshold, despite being close to the other cut-off values, may be explained by several factors. Although the difference between thresholds is only 700 steps/day and represents approximately 20% of the median daily step count in our sample, it may have clinical relevance. Demeyer et al. 46 reported a minimal important difference (MID) of approximately 600 steps/day in individuals with COPD, suggesting that even modest variations can reflect meaningful changes in clinical outcomes such as hospitalization risk. Furthermore, because the 4580 steps per day threshold was derived from a physiological parameter (1.4 METs)7,19 rather than from direct clinical outcomes, it could be less sensitive in detecting differences in subjective aspects such as symptoms, perceived health status, and psychological distress.
The findings of our study have important clinical implications for the management of individuals with COPD, particularly in relation to health status and psychological well-being. Identifying 5000 steps/day as a practical cut-off point highlights its potential as a target for promoting general health. The complementary ROC curve analysis reinforced the clinical relevance of the 5000 steps/day threshold. An AUC of 0.64 suggests that the daily step count has a moderate ability to discriminate individuals with poor health status (CAT ≥18). The optimal cut-off identified (4965 steps/day) aligns with the findings from the categorical analysis and with previous literature that proposed 5000 steps as a marker of a sedentary lifestyle in individuals with COPD. 20 Thus, the use of this threshold is supported by both literature-based evidence and data from our cohort.
The observed differences in MVPA between the ≥5000 and ≥4300 steps/day groups may be partially explained by underlying differences in exercise capacity. Although this variable was not directly assessed in our study, individuals with higher functional capacity are more likely to engage in sustained or higher-intensity activities, thus accumulating more MVPA and reaching higher step counts. Furthermore, the ≥1952 cpm threshold commonly used to define MVPA may overestimate exertional intensity in individuals with COPD, 47 potentially underrepresenting lower-intensity activities that still contribute meaningfully to physical functioning and overall health in this population.
Although this study has provided new insights into physical activity thresholds for individuals with COPD, causal relationships cannot be established due to the cross-sectional design of this study; thus, future longitudinal studies are needed. Furthermore, the potential for a type 2 error could be suggested because the active group had fewer participants at the 5000-step cut-off. However, the average step count for individuals with COPD is approximately 430018,19,21 steps per day, and it is understandable that the higher the cut-off point is, the fewer individuals who fall into the active group. Nevertheless, our results do not suggest that this occurred because the beta value between inactive and active individuals at the cut-off of 5000 steps/day was 94.2% for the mMRC, 92.8% for the CAT, and 91.5% for the HADS-D. In addition, at the 4580-step cut-off, it was 95.9% for the mMRC and 88% for the CAT, and at the 4300-step cut-off, it was 99.6% for the mMRC and 85.3% for the CAT. Therefore, the high beta values support the robustness of the observed differences between inactive and active individuals. Importantly, data collection occurred during the COVID-19 pandemic, which may have affected physical activity and psychological outcomes; however, it did not take place during the strict lockdown, and recruitment spanned both the pre- and postpandemic periods, partially mitigating this effect. Finally, because a smaller proportion of participants completed the CCQ than the CAT did, the ability to detect associations involving clinical control may have been limited. Future studies could benefit from a more detailed analysis of sedentary time in different contexts and its interaction with light- to moderate-intensity physical activity.
Our findings indicate that a cut-off of 5000 daily steps is the threshold most strongly associated with better health status and fewer depressive symptoms, whereas a cut-off of 4300 steps is linked to less severe dyspnoea. These results support the potential use of the step count as an objective health-related status indicator in individuals with COPD. However, given the cross-sectional design, no causal inferences can be drawn, and further research is needed to explore the impact of increasing physical activity on clinical outcomes in this population.
Footnotes
Ethical statement
Author contributions
The conception and design were performed by Juliana de Melo Batista dos Santos, Fabiano Francisco de Lima, Regina Maria Carvalho-Pinto, and Celso Ricardo Fernandes de Carvalho. Material preparation, data collection and analysis were performed by Juliana de Melo Batista dos Santos, Caroline Maschi de Censo, Eloise Arruda dos Santos, Juliana Tiyaki Ito, and Rafaella Fagundes Xavier. The first draft of the manuscript was written by Juliana de Melo Batista dos Santos, Fabiano Francisco de Lima, and Celso Ricardo Fernandes de Carvalho and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by São Paulo Research Foundation (FAPESP) (Grant numbers: JMBS #2022/09628-1, FFL #2021/04198-6, CMC #2020/08827-5 and CRFC #2018/17788-3) and by the National Council for Scientific and Technological Development (CNPq) (Grant number: CRFC #312.279/2018-3).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.