
Abstract
Introduction
Chronic cough (cough lasting >8 weeks) affects an estimated 5−10% of the world’s population, predominantly women. 1 Chronic cough is a well-established risk factor for stress urinary incontinence (SUI) in women,2–5 which is defined as the involuntary loss of urine due to a sudden increase in intra-abdominal pressure caused by effort, exertion or upon sneezing or coughing. 6 In populations with chronic cough or associated conditions such as chronic obstructive pulmonary disease (COPD), urinary incontinence was present in about half the women7,8; and in an even higher proportion (63%) when women were queried directly by their physician about cough-related SUI. 9 As chronic cough and SUI are both associated with anxiety, depression, social isolation and work limitations, there may be cumulative impairment to patients’ quality of life (QoL).10–12
To understand the burden of cough for the health system and patients, we conducted an observational study of patients with refractory or unexplained chronic cough who attended outpatient clinics in Spanish hospitals. For context, refractory chronic cough (RCC) refers to a cough that persists despite optimal treatment for its presumed cause in a patient who is adherent to medical recommendations. Unexplained chronic cough (UCC) denotes cough when no diagnosable cause has been found despite extensive assessment for common and uncommon causes. 1 Cough-related SUI was documented in 18.4% of patients’ clinical charts, with 2-fold greater frequency in women than men (21.1% vs. 9.1%). 13 In a parallel patient survey, 38.1% of women but the same percentage of men (9.1%) reported that cough-related SUI occurred ‘frequently’ or ‘mostly/always’, 14 further suggesting that cough-related SUI is underdiagnosed in women. This prompted us to examine the matter in greater detail. The current analysis aimed to determine the frequency of underdiagnosis of cough-related SUI, whether the profile of women with undiagnosed SUI is similar or different to that of women with diagnosed cough-related SUI, and the relationship between cough-related SUI and women’s general health status and QoL.
Methods
The aforementioned retrospective, multicenter, non-interventional study focused on the burden of RCC and UCC to the healthcare system and patients. Methods and main outcomes have been reported previously.13,14 Briefly, patients were recruited in allergy and pulmonology outpatient hospital clinics from the Spanish National Healthcare System. Consecutive adult patients (>18 years-old) with a diagnosis of RCC or UCC, who had cough of more than 1 year’s duration, and who had cough on the day of the visit, were invited to participate. Active smokers or individuals who had stopped smoking in the previous 12 months were excluded. Other exclusion criteria were treatment with ACE inhibitors; chronic cough related to COPD, cancer, active infection, bronchiectasis, interstitial lung disease, cystic fibrosis, or Gilles de la Tourette syndrome; current participation in interventional studies; or conditions that, in the judgment of the treating physician, advised against participation (e.g., cognitive impairment, major depression, end-stage disease). The study protocol was reviewed and approved by the Research Ethic Committees of all participating hospitals. Enrolled patients provided signed informed consent before data collection began.
Information was collected from patients’ clinical records and from a printed survey that patients and relatives completed without investigator or treating physician overview. Information collected from clinical charts comprised patients’ characteristics, comorbidities, cough characteristics and cough-related diagnostic procedures and treatments. The predefined period for chart review was up to 3 years before study inclusion. Information collected from the printed patient survey included the impact of chronic cough on daily life activities, QoL, and a range of physical items.
The presence of cough-related SUI was explored either as a diagnosis documented in clinical charts and as a physical complication reported by patients in the printed survey. Women with a diagnosis of cough-related SUI in their clinical chart (yes/no) were considered to have ‘Diagnosed cough-related SUI’. Women without a diagnosis of SUI in their clinical chart but who responded ‘frequently’ or ‘mostly/always’ to the survey question “Do you ever have urinary incontinence (loss of urine) due to your cough?” were considered to have ‘Undiagnosed cough-related SUI’. Women without a diagnosis of SUI in their clinical chart and who did not select ‘frequently’ or ‘mostly/always’ in response to the survey question on cough-provoked urine incontinence were considered to have ‘no SUI’.
As part of the printed survey, patients were asked a series of questions about the impact of cough on everyday life (e.g., home, work, social activities). The 15 items were adapted from questions reported in previous studies,15,16 or were created ad hoc for study purposes under the guidance of cough experts. Patients were instructed to respond to the questions according to the impact of cough as a chronic condition in their everyday lives, and not to restrict their responses to a specific time interval. Response options ranged from 1 = Not at all to 7 = Extremely high.
Patients also completed the EQ-5D-5-L questionnaire (https://euroqol.org/eq-5d-instruments/eq-5d-5l-about/), which is a generic measure of general health status. The EQ-5D descriptive system comprises five dimensions: mobility, self-care, usual activities, pain/discomfort and anxiety/depression. Patients self-assess each dimension by selecting one of five levels ranging from ‘no problems’ to ‘extreme problems’. The accompanying EQ visual analogue scale (EQ-VAS) is labelled vertically from 0 = ‘The worst health you can imagine’ to 100 = ‘The best health you can imagine’, and is used as an overall quantitative measure of general health that reflects the patient’s own judgement (https://euroqol.org/eq-5d-instruments/eq-5d-5l-about/). A EQ-5Q index value for each patient was calculated using the value set for health states of the EQ-5D-5-L based on preferences of the Spanish population. 17
Patients also completed the Leicester Cough Questionnaire (LCQ), a validated 19-item instrument used to assess the impact of cough on QoL. 18 The LCQ comprises three domains: physical, psychological, and social. Patients assess their cough symptoms and impact of cough on their QoL over the previous 2 weeks using a 7-point Likert-type scale for each item. Mean scores of each domain are calculated as the average of their items, yielding values from 1 to 7. The LCQ total score is the sum of the three individual mean scores, ranging from 3 to 21. Lower LCQ scores indicate poorer QoL due to cough. A change from baseline of 1.3 in the LCQ total score is the minimal clinically important difference. 19 The LCQ has been used in clinical trials of patients with RCC/UCC as a measure of cough-related QoL.20,21
Statistical analysis
Variables are summarized descriptively as mean ± standard deviation (SD) or as number and percentage. The impact of cough on women’s everyday life is described according to the number (percentage) of women who responded ‘quite a bit’, ‘very much’ or ‘extremely high’ to each of the 15 items on the questionnaire. Differences between groups (diagnosed cough-related SUI, undiagnosed cough-related SUI, no SUI) were assessed using the chi-square test. General health status and QoL of respondents is described by the proportion of women who indicated any problem in the EQ-5D dimensions, and by the mean ± SD EQ-VAS score. The impact of cough on women’s QoL is described according to mean ± SD LCQ scores (physical, psychological, social and total). Differences between the three groups were analyzed using the analysis of variance (ANOVA) test.
Multiple linear regression models were used to examine the relationship between cough-related SUI, general health status (EQ-VAS score) and cough-related QoL, with EQ-VAS and LCQ scores as dependent variables. Explanatory variables were those with potential to influence health status and cough-related QoL. Cough severity as perceived by patients was measured using a 100 mm cough severity VAS score from ‘no cough’ (0 mm) to ‘worst cough’ (100 mm) and was introduced into the model as a discreet variable by increments of 10 units. Beta coefficients ±SD with p values are provided.
All analyses were performed using the IBM SPSS 20.0.0 statistical program.
Results
Of 152 women who entered the study, five did not complete the printed survey. Data for 147 women were valid for the current analysis. Mean age was 57.9 ± 13.3 years and mean duration of cough was 6.2 ± 4.5 years. The number (%) of responses to the survey question “Do you ever have urinary incontinence (loss of urine) due to your cough?” were: never/hardly ever: 36 (24.5%); rarely: 17 (11.6%); sometimes: 38 (25.9%); frequently: 30 (20.4%) and mostly/always: 26 (17.7%).
Thirty-two women (21.8%) with a diagnosis of urinary incontinence documented in their clinical chart formed the diagnosed cough-related SUI group. Thirty-three women (22.4%) without a diagnosis of urinary incontinence in their clinical chart but who responded that their cough provoked urinary incontinence ‘frequently’ or ‘mostly/always’ constituted the undiagnosed cough-related SUI group. The remaining 82 women (55.6%) without a diagnosis of urinary incontinence in their clinical chart and who responded other than ‘frequently’ or ‘mostly/always’ to the question on cough-provoked urinary loss formed the ‘no SUI’ group.
Characteristics of women with RCC or UCC according to diagnostic status of cough-related stress urinary incontinence.

Data are expressed as mean ± SD or n (%).
*p < .05 compared to no SUI group in post hoc multiple comparisons.
RCC: refractory chronic cough; SD: standard deviation; SUI: stress urinary incontinence; UCC: unexplained chronic cough; VAS, visual analogue scale.
aContinuous: Patient suffers from cough every day or nearly every day. Intermittent, but not seasonal: Patient suffers periods of cough and periods of remission, but the cough is not present at specific periods in the year. Intermittent, seasonal: Patient has a chronic cough at specific times or seasons.
Impact of cough on women’s everyday life. Number (%) of women with RCC or UCC and diagnosed, undiagnosed or no cough-related stress urinary incontinence who selected the response options ‘quite a bit/very much/extremely high’ for each item.

Data are expressed as n (%). Not all patients responded to all items. Percentages are calculated according to the total number of respondents (as indicated) per item.
Response options per item were: (1) Not at all; (2) Slightly; (3) Somewhat; (4) Moderately; (5) Quite a bit; (6) Very much; (7) Extremely high.
RCC: refractory chronic cough; SUI: stress urinary incontinence; UCC: unexplained chronic cough.
General health status. Number (%) of women with RCC or UCC and diagnosed, undiagnosed or no cough-related stress urinary incontinence who indicated any problem (slight problem, moderate problem, severe problem, extreme problem/unable to perform) in EQ-5D dimensions; mean EQ-VAS scores and mean EQ-5Q index values.

Data are expressed as n (%) and mean ± SD.
The EQ-5D-5L descriptive system of 5 health dimensions includes 5 response categories of no problem, slight problems, moderate problems, severe problems, and extreme problems/unable to perform. A lower EQ-VAS score indicates worse perceived general health status.
*p value <.05 compared to no SUI in post hoc multiple comparisons. For multiple comparisons between diagnosed and undiagnosed cough-related SUI groups, there were no significant differences.
EQ-VAS: EuroQoL visual analogue scale; RCC: refractory chronic cough; SUI: stress urinary incontinence; UCC: unexplained chronic cough.
aThe EQ-5Q index was calculated based on data sets for Spain (value from 0 to 1, where 1 is the best state of health).
Quality of life as measured by the Leicester Cough Questionnaire in women with RCC or UCC and diagnosed, undiagnosed or no cough-related stress urinary incontinence.

Lower LCQ scores indicate poorer quality of life due to cough.
*p value <.05 compared to no SUI in post hoc multiple comparisons. For multiple comparisons between diagnosed and undiagnosed cough-related SUI groups, there were no significant differences (all p values >.4).
LCQ: Leicester Cough Questionnaire; RCC: refractory chronic cough; SUI: stress urinary incontinence; UCC: unexplained chronic cough.
Multivariate analysis: multiple linear regression model for the EuroQoL visual analogue scale (EQ-VAS).
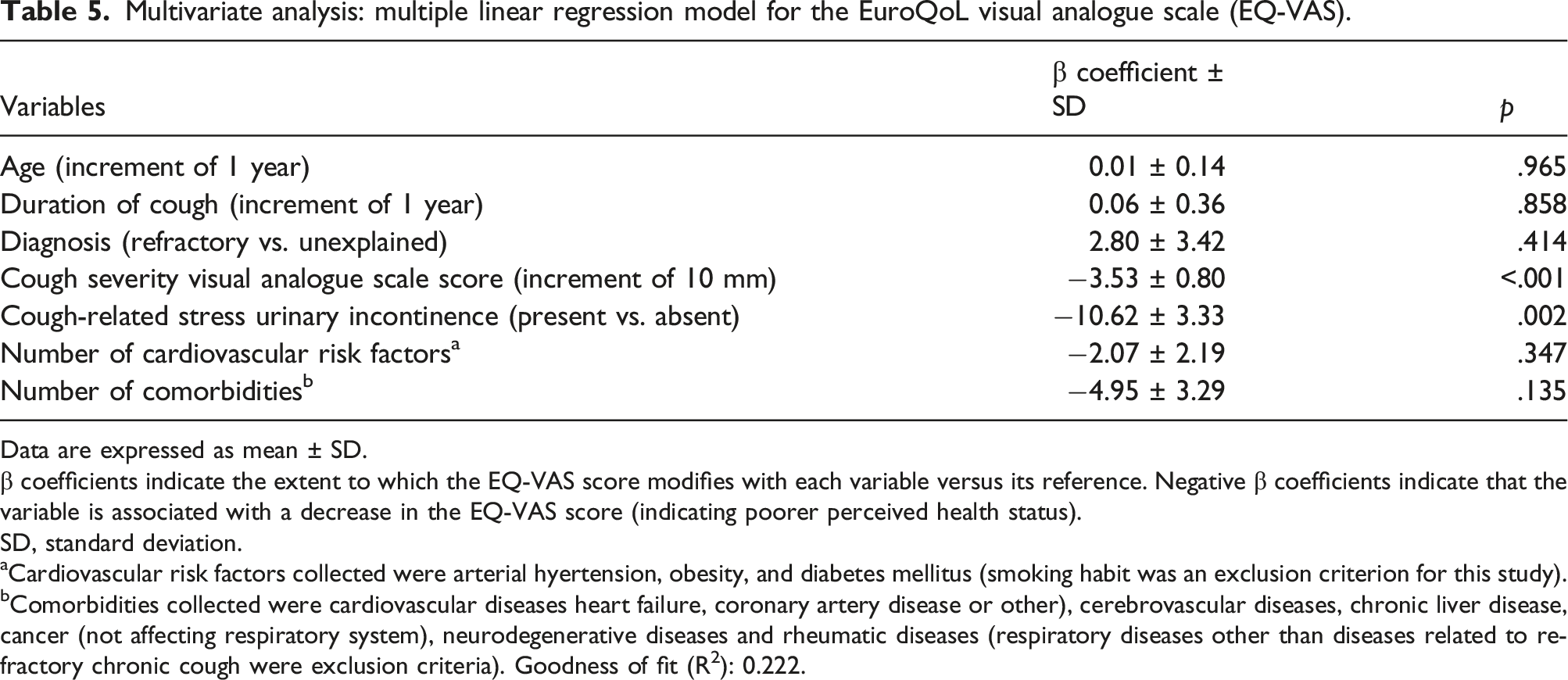
Data are expressed as mean ± SD.
β coefficients indicate the extent to which the EQ-VAS score modifies with each variable versus its reference. Negative β coefficients indicate that the variable is associated with a decrease in the EQ-VAS score (indicating poorer perceived health status).
SD, standard deviation.
aCardiovascular risk factors collected were arterial hyertension, obesity, and diabetes mellitus (smoking habit was an exclusion criterion for this study).
bComorbidities collected were cardiovascular diseases heart failure, coronary artery disease or other), cerebrovascular diseases, chronic liver disease, cancer (not affecting respiratory system), neurodegenerative diseases and rheumatic diseases (respiratory diseases other than diseases related to refractory chronic cough were exclusion criteria). Goodness of fit (R2): 0.222.
Multivariate analysis: multiple linear regression model for Leicester Cough Questionnaire (LCQ) total and domain scores.

Data are expressed as mean ± SD.
β coefficients indicate the extent to which the LCQ score modifies with each variable versus its reference. Negative β coefficients indicate that the variable is associated with a decrease on LCQ scores (indicating poorer quality of life). Goodness of fit (R2) for the LCQ total score: 0.376; Physical domain: 0.321; Psychological domain: 0.332; Social domain: 0.335.
LCQ: Leicester Cough Questionnaire: SD, standard deviation; SUI: stress urinary incontinence.
Discussion
Our analysis found that one in five women with RCC/UCC had diagnosed cough-related SUI as recorded in their clinical chart, while a similar proportion had undiagnosed cough-related SUI as reflected in the patient survey. The 44.2% total frequency of cough-related SUI in this patient cohort (65/147 women) is broadly in line with frequencies reported in other chronic cough populations.7–9 The total number of women with SUI (n = 65) is higher than the sum of women who responded ‘frequently’ or ‘mostly/always’ to the question on cough related SUI (n = 56) because nine patients in the diagnosed SUI group responded ‘sometimes’. As the study focused mainly on the identification and description of diagnosed and undiagnosed cough-related SUI, these nine women were retained in the diagnosed group for analysis. A major finding of the study was that, independently of cough severity, the presence of diagnosed or undiagnosed cough-related SUI was associated with significantly worse general health status and worse cough-related QoL.
The absence of a diagnosis in half the women with cough-related SUI in our cohort is of concern given the substantial impact of SUI on women’s health status and QoL.10–12 Potential reasons for SUI to be undiagnosed in women, including those with chronic cough, are the associated embarrassment or stigma (preventing women from coming forward), a lack of active screening by the treating physician, and the perception by many women that incontinence is a normal consequence of aging or childbirth.3,22 The finding that general health status and cough-related QoL are similarly impacted in undiagnosed and diagnosed women is relevant since cough-related SUI can benefit from new cough-specific therapies, 23 suggesting value in screening women for this complication.
The additional mental and physical burden of cough-related SUI was clearly exposed by investigating the impact of cough on patients’ everyday lives according to diagnosis. Compared to the no SUI group, significantly more women with cough-related SUI, whether diagnosed or not, reported that cough made them feel anxious or depressed, and that it interfered with everyday activities, professional development, leisure time activities, and ability to perform tasks requiring concentration. The presence of cough-related SUI was also associated with poorer QoL due to cough as evidenced by significantly lower mean LCQ scores in diagnosed and undiagnosed SUI groups compared with the no SUI group. Numerically, the largest difference in QoL was in the LCQ social domain, consistent with the social and recreational withdrawal that is known to occur in women with SUI. 24 The extent of impairment to general health status, daily life and QoL was similar between the diagnosed and undiagnosed cough-related SUI groups, suggesting that a relevant proportion of female patients with chronic cough ‘suffer in silence’ about their SUI and are potentially missing opportunities for effective management.
In multivariate analysis, greater cough severity (VAS) and the presence of SUI were key factors associated with lower EQ-VAS and LCQ scores. The association of cough-related SUI with poorer health status and poorer QoL was independent of cough severity. This finding emphasizes the importance that patients place on the secondary physical effects of cough such as SUI relative to more simple measures such as cough frequency or severity. 25
The current range of treatment options for cough-related SUI is limited, underlying the need for new therapeutic approaches. 26 Alleviating repetitive daily cough-induced increases in intra‐abdominal pressure may reduce episodes of incontinence. An interesting observation was that BMI was approximately 2 kg/m2 higher in women with than without cough-related SUI. A high BMI was identified as a risk factor for de novo SUI in a large longitudinal study involving 25,000 Chinese women, 6 and was associated with a greater likelihood of cough-induced SUI in a cohort of female patients with chronic cough. 9 Since BMI is a modifiable risk factor, reducing BMI among women in the overweight/obese range, may improve SUI. As regards pharmacological therapies, the efficacy and safety of the cough-specific P2X3 antagonist gefapixant was evaluated in 375 women with RCC/UCC and cough-related SUI. At week 12, gefapixant-treated participants experienced a greater percentage reduction in mean self-reported daily cough-related SUI episodes compared with placebo recipients.23,27
Limitations of observational studies include the absence of a control group, incomplete or missing data, and potential for selection bias. Specific to the current study, cough-related SUI was diagnosed based on information recorded in clinical charts or by patient self-reporting and was not verified by specific SUI diagnostic tests. Although the survey question posed to women specified a relationship between cough and urinary incontinence, we cannot exclude that some cases of urge urinary incontinence may have been mislabeled as SUI. No data were collected about potential pharmacological or non-pharmacological measures to relieve urinary incontinence in women with diagnosed SUI. The fact that all women had a cough duration >1 year and cough on the day of the visit (inclusion criteria), and that there were no differences in the cough severity VAS between those with diagnosed and undiagnosed SUI, suggests that cough is the driver of urinary incontinence in these women. Some data regarding the impact of cough were collected using validated instruments (e.g., EQ-5D-5 L for general health status and LCQ for QoL), whereas other data were derived from unvalidated sources. Questions to assess the impact of cough on everyday life activities were developed specifically for study purposes; validated patient-reported instruments to assess anxiety and depression were not used. Although the questions and instruments were intended to assess the impact of cough on SUI, the contribution of other risk factors to SUI is uncertain. As some instruments assessed only the moment that patients responded (VAS cough severity score, EQ-VAS), or the previous 2 weeks (LCQ), we acknowledge that a longitudinal study may provide a more complete picture of the impact of cough-related SUI on everyday life and QoL. Statistical comparisons must be interpreted with caution given that the 147 women included in this analysis represented a subgroup of the total number of patients required to provide statistical power (n = 196) as reported previously. 13 Results of multivariate analyses should be considered descriptive in nature and fundamentally as hypotheses generators of factors that may influence the health status and QoL of women with RCC/UCC. Lastly, because the study involved outpatients attended at cough clinics with potentially greater symptomatology, the results may not be generalizable across the wider RCC/UCC population.
Conclusions
A substantial proportion of women with RCC or UCC have cough-related SUI. Current practice suggests that about half the women with RCC or UCC managed at outpatient hospital clinics in Spain have undiagnosed cough-related SUI. SUI associated with RCC and UCC adversely impacts women’s general health status, QoL and ability to perform everyday life activities. Since the burden of cough-related SUI is the same irrespective of diagnostic status, removing obstacles to a SUI diagnosis is essential to identify patients with unmet needs who can benefit from new therapies to suppress cough. Educational campaigns may increase awareness of cough-related SUI in general and instill women with the confidence to come forward about their condition. Women with chronic cough should be screened regularly for SUI.
Footnotes
Acknowledgments
Professional medical writing assistance was provided by Kerry Dechant, ISMPP CMPP™, on behalf of Content Ed Net (Madrid, Spain) with funding from MSD Spain.
Author contributions
Ebymar Arismendi participated in data collection, data interpretation and drafting and editing of the manuscript. Luis Puente-Maestu, Christian Domingo, Ignacio Dávila and Santiago Quirce participated in study design, data collection, study analysis and editing of the manuscript. Francisco Javier González-Barcala and Astrid Crespo-Lessmann participated in data collection, data interpretation and drafting and editing of the manuscript. Marta Sánchez-Jareño, Cristina Rivas-Pardiñas and Luis Cea-Calvo participated in study design, study analysis, data interpretation and drafting and editing of the manuscript. All authors approved the final version.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Ebymar Arismendi has received honoraria for consultancy and conferences from AstraZeneca, Gebro-Pharma, GSK, Menarini, MSD, Novartis, and Sanofi-Genzyme. Luis Puente-Maestu has received consulting fees from MSD; payments for lectures from Chiesi, Grifols, and Pulmonx; grants from AstraZeneca, Chiesi, GSK, and Pulmonx. Christian Domingo has received consultant and speaker’s honoraria from Allergy Therapeutics, ALK, AstraZeneca, Boehringer Ingelheim, Chiesi, GSK, Menarini, MSD, Novartis, and Sanofi. Ignacio Dávila has received consulting fees from Allergy Therapeutics, AstraZeneca, GSK, MSD, Novartis, and Sanofi; payments for lectures from Allergy Therapeutics, AstraZeneca, Chiesi, Diater, GSK, LETI, Novartis, and Sanofi; grants to his institution from ISCIII, Junta de Castilla de León, and ThermoFisher. Santiago Quirce has received speaking, lecture and consulting fees from Allergy Therapeutics, AstraZeneca, GSK, Mundipharma, Novartis, Sanofi, and Teva. Francisco Javier González-Barcala has received consulting fees and speaker’s honoraria from ALK, AstraZeneca, Bial, Chiesi, GebroPharma, GlaxoSmithKline, Menarini, Novartis, Rovi, Roxall, Sanofi, Stallergenes-Greer and Teva. Astrid Crespo-Lessmann has received speaker’s honoraria from AstraZeneca, Boehringer Ingelheim, Chiesi, GSK, MSD, Novartis, Orion Pharma, Sanofi, and Zambón; conference travel and attendance expenses from Gebro, GSK and Novartis; funds/grants for research projects from several state agencies, non-profit foundations, AstraZeneca, and GSK. Marta Sánchez-Jareño, Cristina Rivas-Pardinas, and Luis Cea-Calvo are full-time employees of MSD Spain.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the MSD Spain.