
Abstract
Keywords
Introduction
Chronic Obstructive Pulmonary Disease (COPD) is a chronic progressive lung illness and a major health problem that affects millions of people worldwide. In 2019, nearly 400 million people globally suffered from COPD. 1 The prevalence in Europe varied between 3.5% and 17.4%, 2 with Italy recording 3.5 million cases, contributing to 55% of deaths related to respiratory diseases. 3 Although traditionally linked to older adults, there’s a concerning uptick in COPD among younger individuals. 4 Despite its widespread impact, COPD is often underestimated in terms of both prevalence 5 and its effects on patients’ lives. 5 Beyond the physical symptoms, COPD significantly impacts psychological well-being, mainly stemming from severe limitations in daily activities and an overall decline in quality of life. 6 In this regard, it’s crucial to raise awareness of COPD risk factors. 7 While smoking is the main cause, 2 other factors, which are sometimes overlooked, 8 can also contribute to its development and exacerbation. A worrisome rise in COPD among non-smokers 9 underscores the necessity to assess other risk factors and customize treatments accordingly. A foundational aspect for introducing an integrated therapeutic model lies in the medical staff’s grasp of patients’ illness perceptions. These encompass dynamic beliefs regarding symptoms, causation, timing, consequences, and controllability, 10 which can significantly impact patients’ health outcomes and underpin the formation of illness expectations 11 —the anticipated progression of the condition based on the current situation. 12
Our study introduces a novel approach by delving into patients’ expressed expectations regarding their disease trajectory, thus shedding light on their coping strategies in managing COPD. Rather than solely focusing on the physical symptoms, we aim to understand the psychological impact of COPD, particularly how severe limitations in daily activities and a decline in quality of life shape patients' perceptions and expectations, and vice versa. Furthermore, our research seeks to identify factors that may serve as protective mechanisms in coping with COPD, exploring what contributes to the development of a sense of responsibility and acceptance, as discussed by Pinnock and colleagues in their interviews with patients facing similar challenges. 13 By capturing patients’ illness-related expectations comprehensively, our study offers insights into the evolution of their behaviors as the condition progresses. 14 This innovative perspective not only informs clinical strategies but also directs interventions that align with patients’ anticipated outcomes, ultimately enhancing the overall management of COPD.
Materials and methods
Ethical considerations
This study was approved by the Ethics Committee of the IRCCS Fondazione Don Carlo Gnocchi in Milan on December 9, 2022. Ethical safeguards, such as obtaining informed consent, ensuring anonymity through code assignment, and emphasizing voluntary participation with the right to withdraw, were implemented.
Study design
A qualitative approach, according to the Grounded Theory (GT) methodology was used, emphasizing the generation of a conceptual understanding derived from a bottom-up data analysis. 15 The intention was to use this model for designing patient-centred interventions, recognizing them as experts on their condition. Our study report conforms to COnsolidated criteria for REporting Qualitative research (COREQ) for reporting qualitative research 16 (Supplemental File 1).
Participants
Sampling and method of recruitment
Patients’ recruitment was carried out at the Heart-Respiratory Unit - IRCSS Santa Maria Nascente, Fondazione Don Carlo Gnocchi in Milan, Italy, between January and May 2023. Theoretical sampling was utilized both in participant recruitment and data collection. This approach allowed for the progressive selection of subjects based on emerging evidence, thereby facilitating the acquisition of valuable insights to substantiate and validate research findings. 17 For instance, participants were purposefully recruited to represent various stages of disease progression, socio-demographic backgrounds, and treatment regimens. This deliberate sampling strategy allowed for a comprehensive exploration of the complexities inherent in COPD management. Data saturation was pursued to ensure a comprehensive exploration of emergent themes, to achieve theoretical completeness, allowing for a thorough understanding of the complexities within the studied phenomena and facilitating the development of contextually rich insights. 18 Participants were recruited by a psychologist (VP), who, after explaining the purpose of the study and outlining the implications of participation, invited interested individuals to review and sign the informed consent form, providing them with a copy.
Inclusion criteria
• Italian adult outpatients/inpatients diagnosed with COPD, including mild, moderate, severe, and very severe, as classified by Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria
1
; • Individuals with COPD who may or may not be utilizing Non-Invasive Ventilation (NIV) or Continuous Positive Airway Pressure (CPAP), and/or oxygen therapy.
Exclusion criteria
• People with significant psychiatric comorbidities, following the medical records; • People with other organic pathologies where COPD wasn’t the primary health concern, following medical records; • Indicators of significant cognitive and/or behavioral dysfunction, as evidenced by a Mini-Mental State Examination (MMSE) score below 21.
19
Data collection
Duration and setting
Data collection involved face-to-face semi-structured interviews and visual tools (Symptoms Traffic Light and PRISM) administered by a female licensed psychologist (VP), who had not previously engaged with participants, as new admissions at the mentioned department. No one else was present.
Research tools
Socio-demographic information
Socio-demographic and clinical information [sex, age, marital status, employment status, housing arrangement, presence of children, Forced Vital Capacity (FVC), Forced Expiratory Volume in the First Second (FEV1), Total Lung Capacity (TLC), Oxygen Desaturation Index (ODI), Oxygen saturation (SpO2) and the lowest oxygen saturation a patient drops to (Nadir SpO2)] were collected.
Symptoms traffic light (STL)
The STL is a specially designed tool that enables participants to assess the severity of their symptoms on a visual scale. Initially, each participant was presented with a sheet depicting an Italian traffic light, featuring three circles: red at the top, yellow in the middle, and green at the bottom. Subsequently, they were provided with a list of 17 COPD symptoms and asked to place them on the red circle if they significantly impacted their daily life, on the yellow circle if the impact was moderate, and on the green circle if the symptoms were mild or absent.
Pictorial representation of illness and self measure (PRISM) – modified version
A modified version of the Pictorial Representation of Illness and Self Measure (PRISM), which is a pictorial tool already used in other chronic conditions, such as diabetes, 20 was used to assess illness burden. 21 Participants were provided with standardized instructions while being presented with a white sheet of paper, symbolizing a representation of their current life. Positioned at the bottom right-hand corner was a yellow circle, symbolizing the participants themselves. 22 A smaller red circle (50 mm diameter), symbolizing their COPD symptomatology, was provided for participants to place wherever they felt appropriate in response to the question: “Where would you position your current illness condition in your life at this moment?”. The measurement of self-illness separation (SIS) was determined by the distance between the centres of the two circles, with SIS values ranging from 0 to 256 mm. 22 Following recent research, SIS values were classified into three groups based on the location chosen to place the red circle, reflecting the COPD perceived severity. 23
In Group 1 (SIS ≤10 mm), the red circle partially overlapped with the yellow self-circle or was entirely contained within it: COPD is perceived as a constant and severe threat to the quality of life.
In Group 2 (11 mm<SIS <60 mm), patients positioned the red circle near the yellow self-circle, though not entirely encompassing it. This metaphorically represented a perceived threat deemed to be in proximity but having a lesser impact than the one in Group 1.
In Group 3 (SIS >60 mm), the red circle was positioned outside and far from the yellow self-circle, representing the least severe condition (see Figures 1(a) and (b)). The pictorial representation of illness and self measure. (b). Three PRISM groups.
Additionally, participants were given four other categories: the role of family, work, relationships, and interests. They were instructed to mark the perceived impact of COPD on each aspect of their lives with an ‘X,' following the placement of the COPD-related circle on the sheet.
Semi-structured interviews
Semi-structured interview.

Data analysis
VP and EV conducted data analysis simultaneously with the data collection phase, facilitating an ongoing refinement of the focus of the interviews. Data analysis followed Strauss and Corbin’s GT approach. 24 Initially, a line-by-line open coding of each of the initial eight transcriptions was independently conducted by VP and EV. Consensus on the codebook was achieved through meetings with all authors, utilizing the constant comparative method. In the axial coding phase, these codes were grouped into categories based on similarities, facilitating the formulation of hypotheses. In the selective coding a core phenomenon was chosen and interconnected with other phenomena. 24 Data analysis was assisted by the computer package Dedoose. In addition to that, during the analysis phase of the conducted interviews, VP, EV, and GB engaged in the process of triangulating results, involving careful integration and comparison of data collected through interviews with those from other data collection tools such as the Symptom Traffic Light system and the PRISM. Through this comprehensive process, researchers were able to enrich and consolidate their findings, ensuring a more comprehensive and accurate understanding of the studied phenomenon.
Validity of the analysis
Validating the data involved a thorough review and examination to identify biases. While the GT approach avoids hypotheses, an acknowledged assumption was considered, particularly regarding potential influences on data gathering, analysis, and interpretation, such as a preference for socially acceptable responses in interview reports. Coding and emergent findings underwent routine evaluation, with ongoing reflexive discussions by authors. Triangulation for analysis improvement involved consulting a clinician (PB) and another psychologist (GB). After extensive discussions, a final consensus was reached on all disparities.
Results
Participants
Twenty-eight Italian COPD patients were included. Sample selection process is provided in Figure 2. Sample selection process.
The mean age was 72.82 years (range: 53-86), including 57.14% males and 42.86% females.
Sample characteristics.
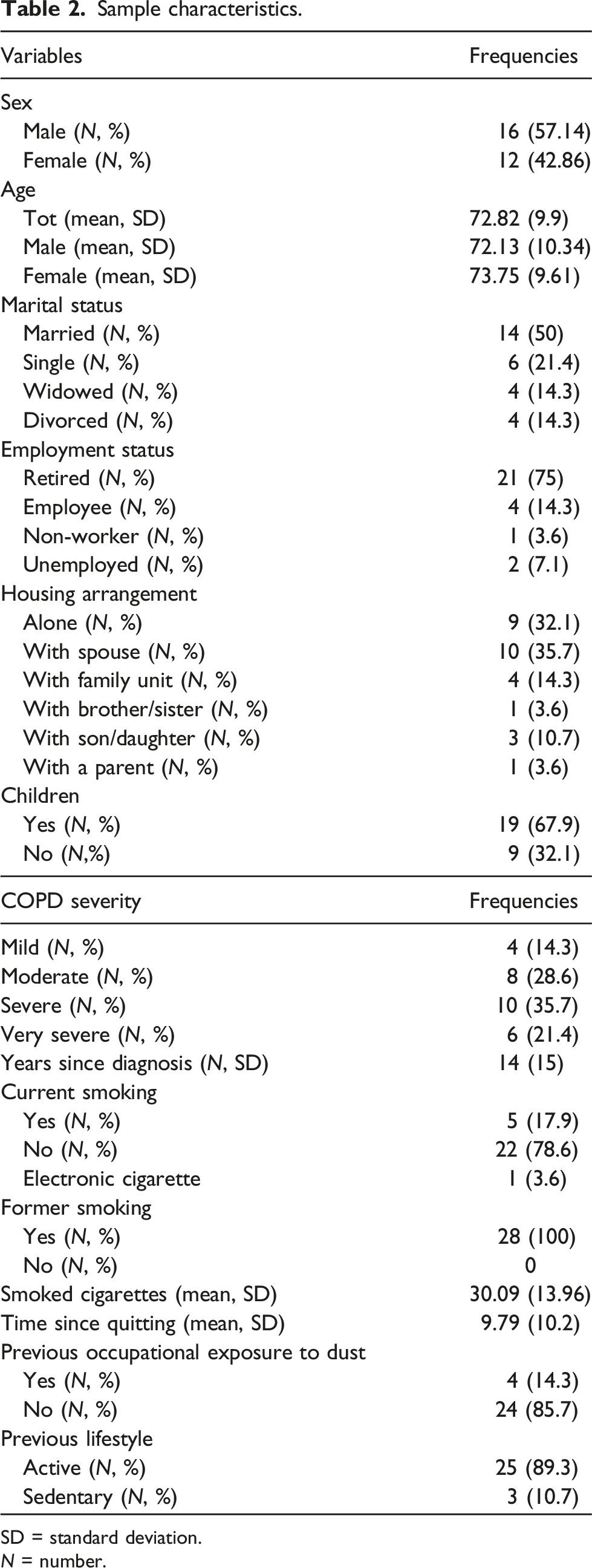
SD = standard deviation. N = number.
Recruited from the cardiorespiratory department, while 32.1% (n = 9) were from the outpatient clinic during monitoring visits. Detailed information about clinical characteristics is presented in Supplemental File 2.
Symptoms traffic light (STL)
The STL assessed symptoms as perceived by patients. “Climbing a flight of stairs” (82.14%), “Shortness of breath” (64.29%), and “Doing daily activities” (53.57%) were perceived as major threats to their quality of life. “Cough” (60.71%) and “Hoarseness” (57.14%) had a moderate impact, while “Pain in swallowing” (75%) and “Pharyngitis” (71.43%) had the lowest. From a psychological standpoint, “Sleep disturbances” (35.71%) were the primary threat to quality of life, followed by “Anxiety” (28.57%) and “Depression” (25%) (See Figure 3). Perceived threat frequency of symptoms.
Pictorial representation of illness and self measure (PRISM)
Regarding the PRISM results, 17 individuals (60.71%) fell into Group 1, perceiving COPD as profoundly impactful. Group 2, comprising 7 participants (25%), saw COPD as a moderate-impact condition, with some maintaining hobbies and social engagement. Only four cases (10.71%) placed COPD in Group 3, perceiving it as low-impact, possibly due to defence mechanisms such as denial. Family dynamics significantly influenced participants across all groups. In Group 1 (N = 11, 39.29%), they played a vital role by providing emotional and physical support, though in some cases (N = 4, 14.29%), the family’s health issues diverted attention from the COPD patient, leading to caregiving responsibilities. Limited family involvement occurred in two cases due to emotional disunity or feelings of powerlessness. Regarding personal interests, nearly all participants (N = 20, 71.43%) distanced themselves from their interests, citing fears of respiratory crises or fatigue. Few participants found solace in new interests compatible with their condition, such as photography, painting, or volunteering (N = 5, 17.86%). Concerning work, some feared work-related respiratory crises (N = 4, 14.29%), while others considered it as a distraction from their health (N = 2, 7.14%) or a risk factor (N = 2, 7.14%). In terms of social relationships, most participants distanced themselves from relationships (N = 19, 67.86%) due to worsening symptoms. However, for a smaller subset, friendships served as a distraction (N = 6, 21.43%), especially as family support decreased.
The evolving process detailing the influence of perceptions and expectations on COPD adaptation
Our model presents a dynamic theoretical framework for understanding the interplay between COPD patients’ illness expectations and perceptions. It unfolds in four progressive phases, from diagnosis to disease management, capturing distinct dimensions of patients’ experience. This framework serves as a valuable tool for healthcare professionals to tailor interventions, promoting patient-centered care aligned with the evolving needs and perceptions of those affected by this chronic condition. Furthermore, it facilitates a deeper understanding of patient point of view and enables the prediction and prevention of potential risk behaviors and beliefs, such as underestimating the future impact of COPD in its early stages. Associated with exacerbations and poor treatment adherence (See Figure 4). Evolution of illness perceptions and expectations in COPD patients: A journey from diagnosis to active management.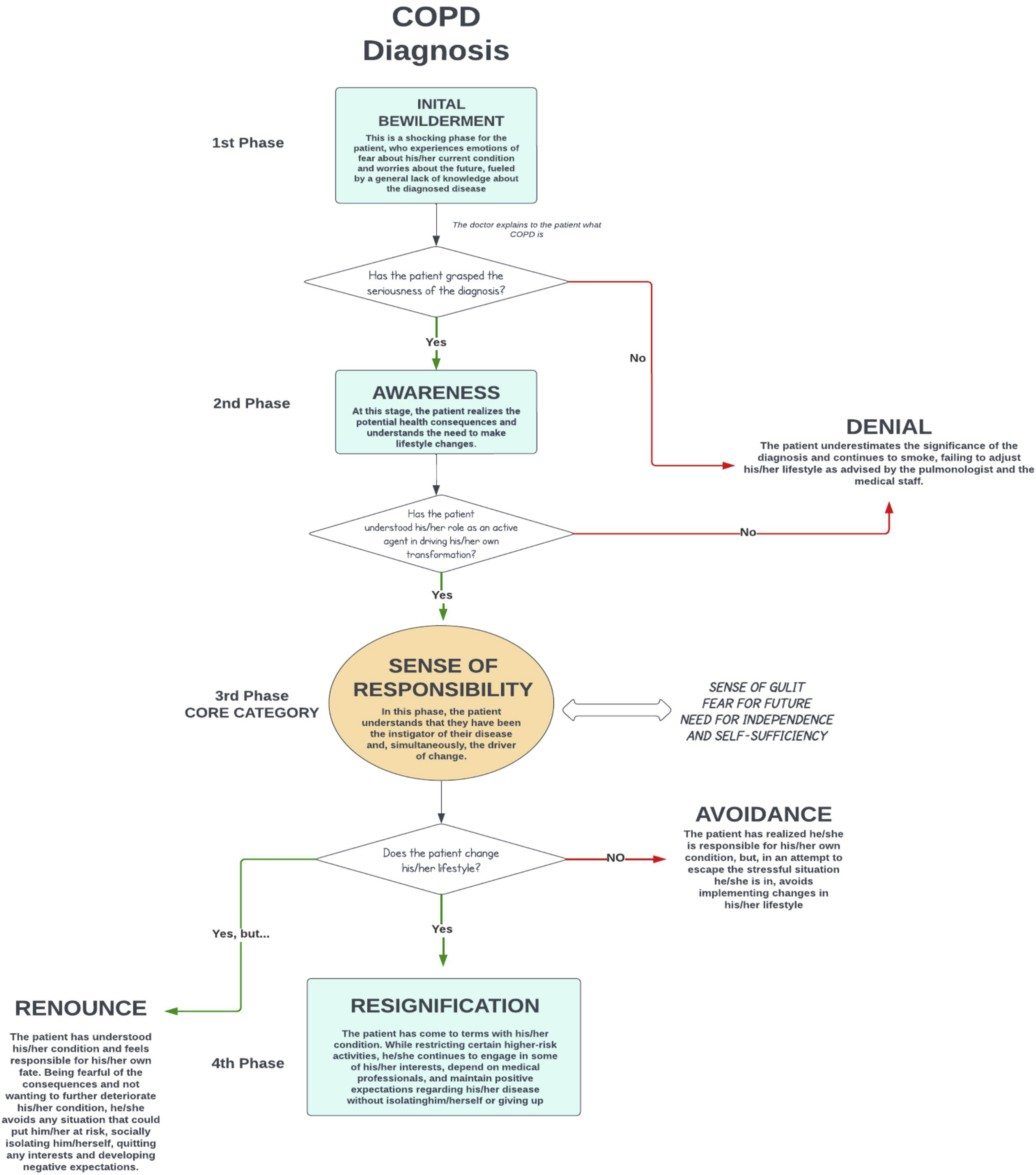
Initial bewilderment
Codes and extracted quotes from patients’ interviews on “limited knowledge of COPD” category.

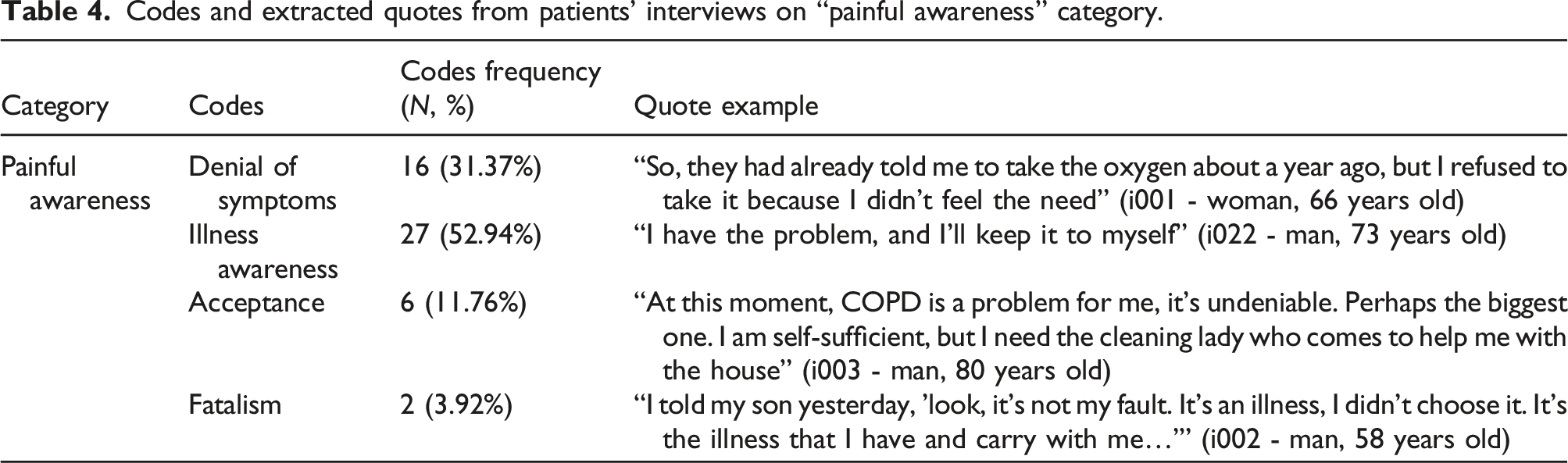
Denial of painful awareness
Codes and extracted quotes from patients’ interviews on “painful awareness” category.
The emergence of a sense of responsibility in the patients
Codes and extracted quotes from patients’ interviews on “self-attribution of responsibility” category.

Rediscovering life’s purpose: Embracing COPD challenges
Upon assuming responsibility in COPD patients, diverse responses manifest driven by expectations of future illness. Some find it overwhelming, leading to half-hearted adherence, treatment avoidance, and occasional smoking relapses. The perception of manageable efforts reduces the urgency for active treatment engagement. Conversely, others embrace significant lifestyle changes, shaping a redefined self-identity. They acknowledge new limitations, develop coping strategies, trust in therapies, and pursue less demanding interests, fostering positive health expectations with realistic stability goals. In contrast, a “restart” response involves social isolation and interest abandonment to avoid health risks, evoking profound hopelessness. Driven by negative expectations, many patients experience a sense of confinement due to ongoing COPD challenges, leading to heightened social isolation and contributing to lived depression and nostalgia (See Supplemental File 3).
Discussion
As COPD progresses, patients undergo a dynamic shift in their perception and management of the illness, transitioning from initial diagnosis to reintegrating into daily life. This study, conducted at the Complex Cardio-Respiratory Rehabilitation Unit of the Don Gnocchi Foundation in Milan, aimed to investigate the evolving landscape of COPD patients’ perceptions and expectations over time, involving individuals at various stages of disease progression. The approach facilitated the development of a dynamic model illustrating nuanced changes in patients’ illness perceptions as the condition advances, highlighting the fluidity of temporal representations in interaction with patient experience. 25 Understanding these dynamic processes is crucial due to the significant impact of illness perceptions and expectations on health outcomes, as demonstrated in prior research. 26 To gain deeper insight into patients’ current perceptions of their symptoms, the Symptom Traffic Light and PRISM were also administered. Based on this model, healthcare professionals can adeptly tailor interventions to meet the evolving scenarios of COPD patients, thereby enhancing disease management and outcomes.
Similar to previous models addressing the perspectives of COPD patients, such as those by Lindqvist 27 and Arne, 28 the theoretical model proposed here delineates four progressive phases, elucidating the transition from a passive to an active role in the healthcare journey. 29 Despite the heterogeneous disease stages, the sample consistently characterized their condition as significantly impacting daily life. This observation remained salient even among individuals who had attained a commendable level of acceptance of their condition, managing to maintain a certain quality of life by cultivating interests compatible with their circumstances. Within the PRISM framework, and as often emerges from the literature on the experiences of chronic patients, 30 the disease was frequently perceived as a formidable threat, imposing limitations not only physically but also in terms of social relationships and interests.
Anxiety and depression emerged as pervasive and impactful symptoms in over 25% of the sample, reflecting existing literature findings. The core of our model lies in the sense of responsibility assumed by patients, wherein they feel accountable for their state and envision themselves as architects of their future. Actively engaging in their condition empowers patients to cultivate a heightened sense of self-efficacy throughout their treatment journey, substantially elevating their expectations regarding future outcomes, as noted by Marklund et al. 31
It is noteworthy that awareness of the severity of one’s condition does not necessarily entail resignation towards life 32 ; rather, it entails a journey of acceptance, as highlighted by Arne. 28 Many participants with severe and very severe stages of COPD often exhibited remarkable resilience and determination in forging new paths towards a fulfilling life, despite the challenges posed by their illness. The desire for independence can aid in the reframing of their existence, often uncovering latent resources and new interests compatible with their condition and inner strength.
In conclusion, a diagnosis of COPD is undoubtedly a traumatic moment for patients, yet it marks the beginning of a journey towards self-care that has long been neglected. Awareness of one’s condition fosters the development of a sense of responsibility that can offer the patient the opportunity to emerge from the guilt of self-inflicted suffering. Such evolution can be facilitated by clear communication from medical personnel, as emphasized by Lindqvist, 27 and the support of friends and relatives, 33 who enable the patient to maintain their dignity and independence. The patient must be informed 34 and supported immediately, including at the psychological level, 35 guided towards acceptance of new limitations, and the discovery of new resources. 36
Strength and limitations
While this study marks the first qualitative investigation conducted on COPD patients in Italy, its significance lies in delving into the dynamic phases of COPD. By offering crucial insights, it equips healthcare practitioners with valuable knowledge to adopt a compassionate, patient-centered approach. Beyond merely addressing physical symptoms, this approach acknowledges and addresses emotional challenges like bewilderment and self-blame, enhancing patient care holistically. However, it’s essential to acknowledge some limitations. Firstly, while the developed model provides valuable insights, uncertainties exist regarding its applicability to COPD patients across different cultural settings. Cultural factors play a significant role in shaping illness perceptions, and variations across diverse populations must be explored to ensure the model’s relevance and generalizability. Secondly, the reliance on a single interview per participant may present a limitation in capturing the nuanced evolution of illness perceptions over time. COPD is a chronic condition characterized by fluctuations in symptoms and experiences, which may not be fully captured through a single interview. Longitudinal studies with multiple interviews over time could provide a more comprehensive understanding of how these perceptions evolve and influence COPD management and outcomes. Moreover, while the PRISM tool has been utilized in other chronic conditions, its adaptation and application to the COPD population represent a novel approach. However, further research is needed to validate its effectiveness in capturing the multifaceted impact of COPD on patients’ lives. This validation process will ensure the reliability and validity of the assessment tool, thereby enhancing its utility in clinical practice and research settings. 33
Conclusion
COPD journey is profoundly shaped by patients’ perceptions and expectations. Collaborative efforts between healthcare practitioners and patients are crucial in establishing achievable goals and restoring a sense of control and responsibility. Fostering positive life expectations can facilitate this transformative process. Active patient participation, personalized treatment plans, and family involvement empower individuals to navigate challenges, showcasing human capacity for growth in adversity.
Supplemental Material
Supplemental Material - Exploring perceptions and expectations of COPD patients: A Grounded Theory approach for personalized therapeutic interventions
Supplemental Material for Exploring perceptions and expectations of COPD patients: A Grounded Theory approach for personalized therapeutic interventions by Valentina Poletti, Gaia Bresciani, Paolo Banfi and Eleonora Volpatoin Chronic Respiratory Disease.
Supplemental Material
Supplemental Material - Exploring perceptions and expectations of COPD patients: A Grounded Theory approach for personalized therapeutic interventions
Supplemental Material for Exploring perceptions and expectations of COPD patients: A Grounded Theory approach for personalized therapeutic interventions by Valentina Poletti, Gaia Bresciani, Paolo Banfi and Eleonora Volpatoin Chronic Respiratory Disease.
Supplemental Material
Supplemental Material - Exploring perceptions and expectations of COPD patients: A Grounded Theory approach for personalized therapeutic interventions
Supplemental Material for Exploring perceptions and expectations of COPD patients: A Grounded Theory approach for personalized therapeutic interventions by Valentina Poletti, Gaia Bresciani, Paolo Banfi and Eleonora Volpatoin Chronic Respiratory Disease.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Italian Ministry of Health (“Ricerca Corrente”). The publication of this article was supported by the “Ricerca Corrente” funding from the Italian Ministry of Health.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.