
Abstract
Background
The effects of coronavirus disease 2019 (COVID-19) on the cardiorespiratory fitness of hospitalized and obese patients are of utmost relevance. This study aimed to analyze how hospital and intensive care unit (ICU) stay together with body mass index affect cardiorespiratory fitness in patients with COVID-19.
Methods
251 participants (males, n = 118; females, n = 133) were assigned to four groups: non-hospitalized COVID-19 patients (n = 65, age: 45.3 years), hospitalized COVID-19 patients (n = 63, age: 57.6 years), COVID-19 patients admitted to the ICU (n = 61, age: 56.9 years), and control group (n = 62, age: 49.8 years). An incremental cardiopulmonary exercise test was performed between 3 and 6 weeks after medical discharge from hospital.
Results
Higher peak oxygen uptake (VO2peak), ventilatory efficiency and power output were found in ICU patients with normal weight (NW) than in overweight (OW) (Mean difference: 0.1 L·min−1, −5.5, 29.0 W, respectively) and obese (OB) ICU patients (Mean difference: 0.1 L·min−1, −5.0, 26.2 W, respectively) (p < .05). In NW, OW and OB participants, higher VO2peak and power output were observed in control group compared with non-hospitalized (Mean difference: NW: 0.2 L·min−1, 83.3 W; OW: 0.2 L·min−1, 60.0 W; OB: 0.2 L·min−1, 70.9 W, respectively), hospitalized (Mean difference: NW: 0.2 L·min−1, 72.9 W; OW: 0.1 L·min−1, 58.3 W; OB: 0.2 L•min−1, 91.1 W, respectively) and ICU patients (Mean difference: NW: 0.1 L·min−1, 70.9 W; OW: 0.2 L·min−1, 91.1 W; OB: 0.3 L·min−1; 65.0 W, respectively) (p < .05).
Conclusions
The degree of severity of COVID-19, especially identified by hospitalization and ICU stay, together with obesity and overweight were key factors in reducing cardiorespiratory fitness in patients with COVID-19.
Keywords
Introduction
Approximately 90% of hospitalized patients with coronavirus 2019 disease (COVID-19) have more than one associated comorbidity, 1 with obesity and overweight being one of the most frequent and harmful. 2 People with obesity and overweight have a greater risk of their health being affected by COVID-19 than normal weight individuals. In fact, an elevated body mass index (BMI) is associated with a greater risk of hospitalization, admission to intensive or critical care, the need for mechanical ventilation, 3 severe pneumonia 4 and prognosis and higher mortality. 5
From a pathogenic perspective, the expansion of adipose tissue associated with obesity profoundly impacts the inflammatory response of the immune system. Obese individuals exhibit elevated circulating levels of proinflammatory cytokines, such as TNF-α, interleukin 1 (IL-1), IL-6, and IL-10, and chemokines. 6 The heightened activation of the inflammatory response can trigger a cytokine storm, potentially intensifying the severity of COVID-19.7,8
Several studies have shown that patients with obesity present a longer mean hospital stay than those without obesity, suggesting that the recovery time of obese patients with COVID-19 could be different from that of non-obese patients. 9 In addition, there is an important relationship between obesity and admission to the intensive care unit (ICU). 10 Hospitalization, admission to an ICU, and obesity seem to be determinant factors for the recovery of functional capacity in COVID-19 survivors.10,11 Furthermore, a high number of patients with COVID-19 admitted to the ICU and suffering from respiratory failure were overweight.12,13
Cardiopulmonary exercise testing (CPET) has become a reproducible and safe tool,14,15 necessary for the interpretation of altered cardiorespiratory fitness in COVID-19 survivors.16–18 Asymptomatic patients with COVID-19 have been shown to have significantly higher peak oxygen uptake (VO2peak) than those with long-term symptoms. 19 Other studies have shown that patients with COVID-19 hospitalized in the ICU had a lower VO2peak, as well as decreased exercise capacity compared to non-hospitalized patients. Even hospitalized patients with COVID-19 had significantly higher values of fat mass and percentage of body fat than non-hospitalized patients. 20 These studies have focused on evaluating cardiorespiratory fitness by comparing the severity of the cases (e.g., non-hospitalized vs hospitalized and ICU).
Understanding how the association between hospitalization and ICU stay with BMI affects cardiorespiratory fitness is crucial to establishing effective treatment strategies in patients with COVID-19. However, how this association affects cardiorespiratory fitness in patients with COVID-19 compared to a control group (CG) of healthy people has not been explored.
The aim of this study was to analyze how the degree of severity of COVID-19, identified by hospitalization and ICU stay, together with BMI affect cardiorespiratory fitness in patients with COVID-19 compared to a healthy CG.
Methods
This was a cross-sectional, observational, descriptive study aimed at evaluating the functional capacity of COVID-19 survivors with a CPET.
The Committee of Ethics and Investigation of the Hospital approved this study (Codi CEIm: 16/21). The protocol was carried out according to the principles of the Declaration of Helsinki and Good Clinical Practice. The study followed the STROBE guidelines. 21 All patients signed the informed consent after receiving an explanation of all study procedures. The data were collected from January 1, 2021 to March 31, 2022 at the hospital of Mataró.
Participants
The study sample selection consisted of patients recruited at the hospital with a clinical and functional diagnosis of COVID-19. Initially, the study included 312 participants, however, the final sample for data analysis involved 251 participants (males, n = 118; females, n = 133).
Eligible patients were identified by the study coordinator and by a researcher of hospital. If necessary, the inclusion process was reviewed with a physician within the research team to prevent selection bias. Researchers involved in the study received training conducted by the study coordinator to ensure a standardized process for data collection and inclusion.
To establish the grade of severity of hospitalization in cardiorespiratory fitness the patients with COVID-19 were assigned to three groups as follows: group of non-hospitalized patients (NHC-19, n = 65), hospitalized group (HOC-19, n = 63), and hospitalized patients admitted to the ICU (ICUC-19, n = 61). All the patients in the ICUC-19 had been admitted to the ICU for presenting a syndrome of respiratory difficulty secondary to bilateral pneumonia by COVID-19.
The inclusion criteria included molecular diagnosis (reverse transcription polymerase chain reaction [RT-PCR]) of infection by acute coronavirus type-2 respiratory syndrome (SARS-CoV-2), patients over 18 years of age. The established exclusion criteria encompassed severe neurological diseases, active oncological conditions, neuromuscular disorders, and/or orthopedic issues hindering the normal development of CPET, along with the absence of a signed informed consent.
A CG of healthy patients who did not suffer from COVID-19 was included in the study (CG, n = 62). Posters or information brochures were placed in strategic locations in the hospital. Once they reported their intention to participate in the study at a hospital checkpoint, the study coordinator contacted them (phone call, email, etc.) to explain the purpose and benefits of their participation in the study.
The inclusion criteria for the CG were: healthy adult over 18 years of age. The exclusion criteria were the following: Having suffered from COVID-19, previous diagnosis of disease or associated comorbidities, performing sports activity that could increase cardiorespiratory fitness, taking any type of medication that could alter cardiorespiratory performance.
Data related to hospital admission were collected in all the patients with COVID-19 and the Acute Physiology and Chronic Health disease Classification System II (APACHE II) score was determined as a predictive system of severity and disease prognosis in patients in the ICU. 22
Outcomes measures
Cardiorespiratory fitness was assessed by performing an incremental CPET until volitional exhaustion, conducted 3 to 6 weeks after hospital discharge. The CPET was performed on an ergometric bicycle with an electromechanical brake (Ergoline900S, Ergoline GmbH, Bitz, Germany). 17 The exercise protocol was individualized in all the patients and adapted to the physical condition of each patient with load increases between 5 and 15 W per minute with a constant pedaling cadence of between 50 and 70 revolutions per minute.
The data of pulmonary gas exchange were registered during the CPET using an open circuit breath-by-breath gas analyzer (Ergostik, Geratherm Respiratory, Bad Kissingen, Germany) calibrated prior to each test. Along the test, the patients were under continuous 12-lead electrocardiographic monitoring and blood pressure was determined every 3 min. The following variables were evaluated during the CPET.
Primary outcomes: absolute and relative values of VO2peak, power output and exercise time during CPET. Ventilatory efficiency was calculated as follows: The slope of VE·VCO2−1 was established as the slope of the relationship between the VE and the VCO2. 23
Secondary outcomes: ventilation per minute (VE), ventilatory equivalent for oxygen (VE·VO2−1), ventilatory equivalent for carbon dioxide (VE·VCO2−1), respiratory exchange rate (RER), partial oxygen and carbon dioxide pressure at the end of expiration (PetO2 and PetCO2, respectively), heart rate and oxygen saturation.
Statistical analysis
The Kolmogorov-Smirnov test was used to evaluate the distribution of the data which were presented as means and their standard deviation and means and their confidence intervals (95% CI). The homogeneity of the variances was analyzed using the Levene test. Where appropriate, a logarithmic transformation of the data was performed. An analysis of covariance (ANCOVA) was applied to evaluate the interaction effect (hospitalization·BMI) and the main effects of the hospitalization and BMI variables adjusted for the covariables of age and sex in the cardiorespiratory variables and in the descriptive data.
To determine the grade of involvement of obesity in functional capacity, the participants were classified according to the categories of the World Health Organization (WHO) 24 : Underweight, BMI <18.5; normal weight, BMI ≥18.5 and <25 kg/m2; overweight, BMI ≥25 kg/m2 and <30 kg/m2; obese, BMI ≥30 kg/m2. Bonferroni adjustment was used to identify multiple comparisons among the study groups. The magnitude of response in the different groups was estimated by partial eta-squared (ηp2). Th scale of ηp2 classification was small (ηp2 = 0.01), moderate (ηp2 = 0.06) and large (ηp2 = 0.14). 25 Statistical power (SP) was also calculated.
A multivariate linear regression model was used to estimate the beta coefficients with 95% CI of the variables related to BMI. The model was adjusted for all clinically significant covariates that exhibited p < 0.10 in univariate analysis.
The Chi-square statistical test was used to determine the association between sex and comorbidities with the BMI in patients with COVID-19 and the CG when appropriate. Statistical significance was set at p < 0.05. All the statistical analyses were performed using the software package SPSS version 25.0 for Mac (SPSS Inc., Chicago, IL, USA).
Results
Participants
Of the 251 participants, 189 patients with COVID-19 (females, n = 105; males, n = 84) who had different grades of severity at the Hospital were included in the study. Sixty-one participants did not complete the evaluation test for illness, death and withdrawal from the study (Figure 1). Flowchart of patients with COVID-19 and control group (STROBE Guidelines).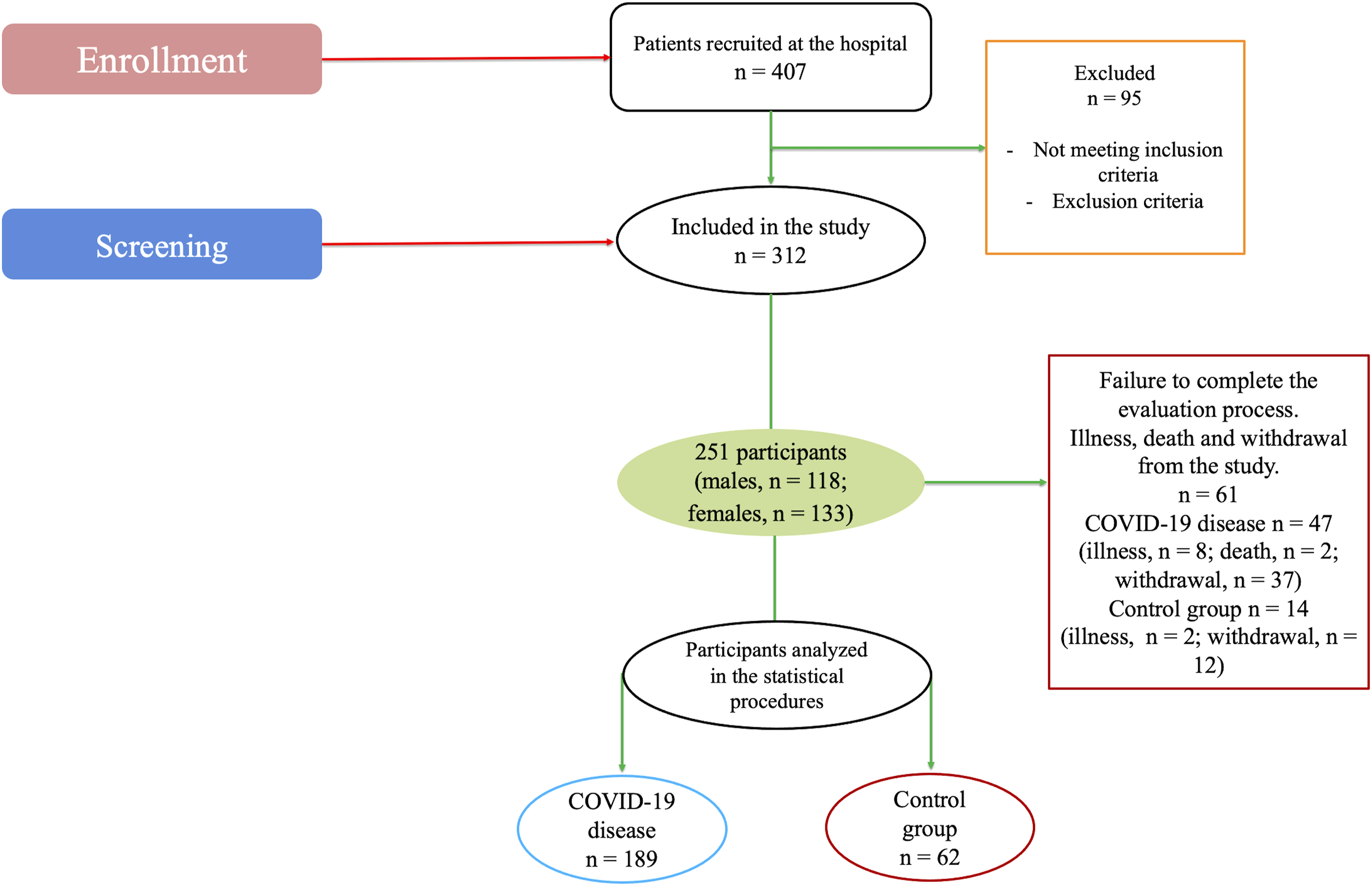
Descriptive data of patients with COVID-19 and control group (n = 251).

Data are provided as mean and 95% confidence intervals (95% CI). Abbreviations: BMI = body mass index; CG = Control group; HOC-19 = hospitalized COVID-19 group; ICUC-19 = intensive care unit COVID-19 group; NHC-19 = non-hospitalized COVID-19 group; NW = normal weight; OB = obesity; OW = overweight.
ap-values for multiple pairwise comparisons.
bp-values for interaction effect hospitalization·BMI.
ccompared to HOC-19.
dcompared to HOC-19, ICUC-19 and CG.
ecompared to NHC-19.
fcompared to NHC-19 and CG.
gcompared to NHC-19, HOC-19 and ICUC-19.
hcompared to NW;
icompared to NW and OW.
Clinical characteristics of patients with COVID-19.

Abbreviations used: ICU = Intensive care unit; SD = standard deviation.
Primary outcomes
In absolute VO2peak (Figure 2), an interaction effect (hospitalization·BMI) was detected (p < 0.001, F = 4.3, ηp2 = 0.1, SP = 1.0). Bonferroni adjustment determined a significantly higher VO2peak in normal weight patients compared to overweight (p = 0.007) and obese patients (p = 0.019) in ICUC-19 group. A significantly higher absolute VO2peak was observed in CG compared to NHC-19 (p < 0.001), HOC-19 (p ≤ 0.003) and ICUC-19 (p ≤ 0.012) groups in normal weight, overweight and obese participants (Figure 2(a)). Differences in absolute peak oxygen uptake (VO2peak, logarithmic transformation of the data) (a) and ventilatory efficiency (VE·VCO2−1 slope) (b) during cardiopulmonary exercise test in COVID-19 patients. Experimental groups: non-hospitalized COVID-19 patients (NHC-19), hospitalized COVID-19 patients (HOC-19), intensive care unit COVID-19 patients (ICUC-19) and control group. Significant differences: ★ for ICUC-19 group. ✦ for all BMI condition.⍫ for HOC-19 and ICUC-19 groups. ⍬ for overweight and obese participants.
Relative peak oxygen uptake and secondary outcomes assessed in patients with COVID-19 patients and control group.

Data are provided as mean and 95% confidence intervals (95% CI). Abbreviations: BMI = body mass index; CG = Control group; HOC-19 = hospitalized COVID-19 group; ICUC-19 = intensive care unit COVID-19 group; Log = logarithmic transformation of the data; NHC-19 = non-hospitalized COVID-19 group; ηp2 = magnitude of response; NW = normal weight; OB = obesity; OW = overweight; PetCO2 = End-tidal CO2 pressure; PetO2 = End-tidal O2 pressure; RER = respiratory exchange ratio; SP = statistical power; VE = minute ventilation; VO2 = relative oxygen uptake. p-values indicate evidence of between-subjects effects.
ap-values for multiple pairwise comparisons.
bp-values for interaction effect hospitalization·BMI.
ccompared to NHC-19, HOC-19 and ICUC-19.
dcompared to NHC-19 and HOC-19.
ecompared to NHC-19 and ICUC-19.
fcompared to OW and NW.
gcompared to OW and OB.
hcompared to OB.
icompared to NW and OB.
In the VE·VCO2−1 slope (Figure 2), an interaction effect (hospitalization·BMI) was revealed (p = 0.046, F = 2.3, ηp2 = 0.1, SP = 0.8). Bonferroni adjustment determined a significantly lower VE·VCO2−1 slope in normal weight participants compared to overweight and obese participants in HOC-19 (p = 0.016 and p = 0.010, respectively) and ICUC-19 (p = 0.026) groups. A significantly lower VE·VCO2−1 slope was detected in CG compared to HOC-19 (p ≤ 0.036) and ICUC-19 (p ≤ 0.026) groups in overweight and obese participants (Figure 2(b)).
In exercise capacity (Figure 3), no interaction effect (hospitalization·BMI) (p = 0.074) was found (p > 0.05) (Figure 3(a)). Differences in total exercise time (a) and power output (b) during cardiopulmonary exercise test in COVID-19 patients. Experimental groups: non-hospitalized COVID-19 patients (NHC-19), hospitalized COVID-19 patients (HOC-19), intensive care unit COVID-19 patients (ICUC-19) and control group. Significant differences: ⍬ for obese participants.★ for ICUC-19 group. ✦ for all BMI condition.
In power output (Figure 3), an interaction effect (hospitalization·BMI) was observed (p = 0.048, F = 2.2, ηp2 = 0.1, SP = 0.8). Bonferroni adjustment determined a significantly higher power output in normal weight participants compared to overweight (p = 0.046) and obese (p = 0.048) participants in ICUC-19 group. A significantly higher power output was observed in CG compared to NHC-19 (p ≤ 0.041), HOC-19 (p ≤ 0.002) and ICUC-19 (p < .001) groups in normal weight, overweight and obese participants (Figure 3(b)).
Secondary outcomes
In VE (Table 3), an interaction effect (hospitalization·BMI) was confirmed (p = 0.001, F = 3.7, ηp2 = 0.1, SP = 1.0). In ICUC-19 patients, Bonferroni adjustment revealed higher VE in normal-weight than in overweight and obese patients (p ≤ 0.045).
No interaction effect (hospitalization·BMI) was identified in the rest of the cardiorespiratory variables (p > 0.05) (Table 3).
In multivariate linear regression analysis (supplemental file 2), absolute VO2peak and PetCO2 were independently associated with BMI (β = 30.28, 95% CI: 23.68 to 36.88, p < 0.001; (β = 0.09, 95% CI: 0.01 to 0.16, p = 0.019, respectively).
Discussion
The main finding of this study was that an association was found between the degree of severity of COVID-19, identified by hospitalization and ICU stay, and BMI on the impaired cardiorespiratory fitness. In the ICUC-19 group, patients with COVID-19 with normal weight had higher absolute VO2peak, power output and ventilatory efficiency than obese and overweight patients.
As expected, CG had a higher VO2peak and power output compared to NHC-19, HOC-19 and ICUC-19 groups in normal weight, overweight and obese participants. CG had higher ventilatory efficiency compared to HOC-19 and ICUC-19 groups in overweight and obese participants. In addition, absolute VO2peak and PetCO2 were independently associated with BMI. Contrary to expectations, no association was found between the degree of severity of COVID-19 and BMI on exercise capacity.
The VO2peak value has shown to be a determinant variable for the evaluation of cardiorespiratory fitness and to predict mortality.26,27 The relative VO2peak values obtained were similar to previous findings with a small sample, 17 and lower than those described in other studies (24 mL·Kg−1·min−1) with a mixed sample of younger men and women with 57% of hospitalized patients with COVID-19, which seems reasonable considering the difference in age between the two studies. 28 However, in other studies with similar samples were observed higher absolute VO2peak (2.4 and 2.3 L·min−1) and relative VO2peak (28.7 and 23.6 mL·Kg−1·min−1) in more severe patients with COVID-19. 29 Similar absolute and relative VO2peak were confirmed in patients with COVID-19 with a more impaired cardiorespiratory fitness (1.3 L·min−1; 17.7 mL·Kg−1·min−1, respectively). 30 In both studies the CPET was performed 3 months after medical discharge from hospital and the mean age of the sample was similar to that reported in our study in hospitalized and ICU-admitted patients. Age is usually a parameter that conditions VO2peak levels; in our study, it could be a differential factor between patients with COVID-19 admitted to the ICU. ICUC-19 group was older than non-hospitalized COVID-19 patients with obesity and overweight.
The low VO2peak values observed were likely influenced, at least in part, by the relatively early timing of the CPET following discharge. This suggests that the recovery process in obese and overweight ICUC-19 patients might have been incomplete. The duration of recovery after discharge, alongside the rehabilitation process, emerges as a crucial factor in enhancing VO2peak among patients with post-COVID-19 sequelae. 31
With respect to obesity among patients with COVID-19, some studies have observed that the population was mainly obese, 29 although they did not specifically analyze the effect of obesity on the VO2peak compared with normal weight patients with COVID-19, obese participants and a CG. The expansion of adipose tissue associated with obesity has proven to be one of the most frequent and harmful comorbidities, contributing, at least in part, to enhancing the inflammation process characteristic of patients with COVID-19.2,7,8 Exploring the connection between proinflammatory cytokines and VO2peak may contribute to the understanding of factors that influence the severity of COVID-19, as occurs in patients with stable chronic heart failure. 32 More studies are needed to corroborate these claims.
Evaluation of ventilatory efficiency is another principal factor for the diagnosis of cardiorespiratory diseases, mainly to understand the phenomenon of VE and lung perfusion. Assessment of VE·VCO2−1 slope is considered a reference method for predicting mortality, ventilatory inefficiency and tolerance to exercise in cardiorespiratory diseases.33,34 The VE·VCO2−1 slope values greater than 34 are used as a reference to determine important impairment in different diseases. 34 The VE·VCO2−1 slope was ∼36 in obese and overweight hospitalized and ICU patients. Conversely, the values were lower than 34 (mean of ∼31) in the rest of the patients, which suggests that obesity and overweight could increase the risk of mortality among those admitted to hospital and ICU as occurs in other cardiorespiratory diseases.33,34
The results of our study showed a VE·VCO2−1 slope higher than that of other studies in a sample of similar characteristics in which CPET was performed 3 months after hospital discharge. 29 The differences detected in ventilatory efficiency between the two studies could be due to the time at which CPET was performed. In our study CPET was carried out between 3 and 6 weeks after medical discharge from hospital. The VE·VCO2−1 slope values might be considered pathological at 3-6 weeks in hospitalized and ICU patients with obesity and overweight who have recovered from COVID-19 and normalized 3 months after hospitalization 29 as patients recover their health.
In addition, mechanical efficiency and muscle fatigue may be other exercise-limiting components associated with ventilatory inefficiency.17,18 In this sense, overweight and obese patients admitted to the ICU also decreased their pedaling power output compared to patients with normal weight. In addition, all patients with COVID-19, hospitalized or no hospitalized, showed lower pedaling power output compared to the healthy people. The association between obesity, overweight and COVID-19 justifies a reduction in pedaling power output and, therefore, a greater predisposition to muscle fatigue.
All the parameters evaluated in a CPET are affected several months after hospital discharge, 30 conditioning the quality of life of patients with COVID-19. The alarming values shown in the VO2peak, the poor ventilatory efficiency and pedaling power output presented by obese and overweight patients with COVID-19 compared to the reference values for normal weight persons in the same condition and age, demonstrate the risk of mortality26,27 and, thus, the need to establish cardiopulmonary rehabilitation exercise programs as quickly as possible.
Several limitations warrant consideration. Given the complexity and labor-intensive nature of the study, sample loss due to factors such as illness or dropout occurred during the CPET assessments. Regrettably, the reasons behind the dropout of certain participants could not be ascertained. As a result, there is a possibility of completion or self-selection bias influencing the reported results, potentially leading to imprecision in the final analysis and interpretation of the data.
In conclusion, obesity, overweight and the degree of severity of COVID-19, especially identified by hospitalization in the ICU, are key factors in reducing cardiorespiratory fitness in patients with patients with COVID-19. Patients with COVID-19, hospitalized or no hospitalized, presented worse cardiorespiratory fitness compared to healthy people.
Supplemental Material
Supplemental Material - Hospital and intensive care unit stay associated with body mass index affect cardiorespiratory fitness in patients with COVID-19
Supplemental Material for Hospital and intensive care unit stay associated with body mass index affect cardiorespiratory fitness in patients with COVID-19 by Eulogio Pleguezuelos, Amin Del Carmen, Mateu Serra, Eva Moreno, Marc Miravitlles and Manuel V Garnacho-Castaño in Chronic Respiratory Disease
Footnotes
Acknowledgments
We would like to thank the study participants for their participation in such a difficult pandemic time.
Author contributions
Conception or design: EP and MVG-C; Acquisition, analysis, or interpretation of data: All authors; Drafting or revising; EP, MM and MVG-C; Final approval of the version: All authors. Agreement to be accountable for all aspects: All authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Consejo Superior de Deportes, Ministerio de Cultura y Deporte, convocatoria “Ayudas para proyectos de investigacion en ciencia y tecnología aplicada a la actividad física beneficiosa para la salud (AFBS) y la medicina deportiva. EXP_74866”.
Ethical statement
Data availability statement
All data of this study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.