
Abstract
Background
COVID-19 demonstrated the possibility of neurological complications such as loss of sense of smell and taste, together with respiratory problems. Respiratory training and rehabilitation of neurological sequelae are essential to improve respiratory function and thus quality of life, and the aim of this study is to evaluate the efficacy of a pulmonary and neurological rehabilitation program.
Objectives
To apply a treatment to reduce dyspnea, increase exertional capacity, increase vital capacity and respiratory muscle strength, together with an increase in olfactory and gustatory sensitivity in post-SARS-CoV-2 patients.
Methods
A randomised controlled experimental study was conducted in 220 patients with a medical diagnosis of COVID-19 and more than 5 months of evolution, dyspnoea or perceived fatigue, including olfactory and gustatory perception problems, of whom 200 patients completed the study. 100 patients were randomly assigned to the intervention group, consisting of an inspiratory training treatment plan (Powerbreathe Plus®) combined with aerobic exercise and olfactory gustatory treatment for 31 days, and 100 patients to the control group, for 31 days without any type of therapy.
Results
The study was conducted in post-Covid-19 patients for 5 months. Two hundred patients were divided into an intervention group (n = 100) and a control group (n = 100). The comparison between the groups showed significant differences in spirometric variables; forced vital capacity (p < .001; Eta2 (0.439); Mean: 0,6135), the ratio between both FEV1/FVC (p < 0.01; Eta2 (0.728); Mean:9,313), peak inspiratory pressure (p < 0.01; Eta2 (0.906); Mean:4,526); changes were observed in dyspnoea measured with the modified Borg scale (p < 0.01; Eta2 (0.811); Mean:1,481) and the modified Medical Research Council scale (p < 0.01; Eta2 (0.881); Mean: 0.777); finally, changes were found in neurological variables, in the questions of the Singapore Smell and Taste Questionnaire, How was your sense of smell after treatment? (p < 0.01; Eta2 (0.813); Mean: 1,721) and How is your sense of taste after treatment? (p < 0.01; Eta2 (0.898); Mean: 1,088).
Conclusion
The implementation of a respiratory rehabilitation treatment plan with the Powerbreathe Plus® device, aerobic exercise and neurorehabilitation with olfactory and gustatory training, is a therapeutic option against respiratory and neurological sequelae in patients who have suffered such sequelae due to the SARS-CoV-2 virus. Clinicaltrials.gov: NCT05195099. First posted 18/01/2022; Last Update Posted 29/06/2022.
Introduction
SARS-CoV-2 is a virus of the genus Betacoronavirus of the family Coronaviridae that causes an acute respiratory syndrome known as COVID-19. Common symptoms include fever, dry cough, sputum production, dyspnoea, anosmia, ageusia, dysgeusia, sore throat, headache, myalgia, arthralgia, nausea and vomiting. 1
Many people who have suffered from COVID-19 disease, according to studies, may suffer from Long-Covid syndrome as early as 4 months after diagnosis, in which various clinical manifestations are noted that can occur in all systems of the human body, as shown in the systematic review and meta-analysis by O'Mahoney LL et al. 2 Cardiac manifestations may be direct or indirect sequelae of inflammatory and/or thrombocytopenic changes, including myocarditis, heart failure, arrhythmias, acute coronary syndrome, pericardial effusion and cardiac tamponade, while musculoskeletal manifestations may be due to the direct effect of SARS-CoV-2 on muscle and nerve cells or to systemic changes induced by the infection. 3 Prolonged hospitalisation can lead to deterioration of the muscular system associated with muscle atrophy and progression to sarcopenia, leading to the onset of fatigue and decreased exercise endurance, 4 and respiratory manifestations can include upper respiratory tract infection, sore throat and cough, which can progress to moderate or severe cases. 5 Moderate cases may include pneumonia, fever and severe manifestations of COVID-19 include acute respiratory distress syndrome, and several factors determine the severity of pulmonary manifestations, such as viral load, comorbidities, age and gender. 6 Neurological manifestations constitute a risk that compromises functional capacity and can lead to severe sequelae such as anosmia, ageusia, headache, stroke, Guillain-Barré syndrome, seizures and encephalopathy. 7 According to the systematic review and meta-analysis by Malik P, et al. 8 68% of patients experience changes in their quality of life, mainly as a result of pain-distress, depression-anxiety and mobility problems in their daily activities.
In the context of COVID-19, respiratory training plays a crucial role in the management and recovery of subjects. Some authors highlight the importance of respiratory training, such as diaphragmatic breathing, nasal inspiration, active contraction of abdominal muscles, together with instrumental respiratory training, to improve the strength of respiratory muscles and lung capacity, thus alleviating respiratory symptoms in virus-infected individuals, and strongly recommend pulmonary rehabilitation due to its positive results on lung function parameters.9–11 Instrumental respiratory training involves the use of specialised equipment or tools to support and optimise respiratory function. These devices, such as positive expiratory pressure devices or inspiratory muscle training devices, provide targeted breathing exercises and facilitate lung expansion. They can help improve lung volumes, strengthen respiratory muscles and improve airway clearance. Some studies have investigated the effect of this training in different pathologies, such as multiple sclerosis, 12 chronic obstructive pulmonary disease (COPD), 13 spinal cord injuries, 14 or asthma. 15
Respiratory training with exercise and neurorehabilitation have shown promising results in improving respiratory and neurological outcomes in patients with COVID-19. The aim of this study is to test the efficacy of a respiratory physiotherapy treatment protocol based on instrumental breathing training and aerobic exercise, together with neurorehabilitation exercises focused on anosmia and ageusia, compared with no training in subjects with Long-Covid syndrome.
Materials and methods
Study design
A randomized controlled experimental study was carried out, complying with the guidelines described in the Consolidated Standards of Reporting Trials (CONSORT) checklist, following trial it has been recorded on the clinicaltrials.gov website and has been admitted with the following identifier number: NCT05195099.
Participants
Participants were recruited from the laboratories of the Catholic University of Avila located in Avila (Spain), following these inclusion criteria: (1) More than 5 months of evolution of COVID-19 medically diagnosed by polymerase chain reaction (PCR) test for SARS-CoV-2 virus, (2) patients perception of symptoms of dyspnoea, (3) perception of loss or decrease of smell, (4) perception of loss or decrease of taste, (5) be aged between 18 and 45 years.
Exclusion criteria are: (1) Severe exercise intolerance, (2) ischaemia during low intensity exercise, (3) severe pulmonary hypertension, (4) severe COVID-19 related symptoms, (5) recent cardiovascular events, (6) Cancerous processes, (7) muscular diseases, (8) severe neurological disease.
Group assignment
Participants were informed of the study and agreed to participate by signing the informed consent form. They were randomly assigned into two groups; intervention group: received a respiratory treatment based on aerobic exercise and treatment of the inspiratory musculature and a neurorehabilitative treatment focusing on the sense of smell and taste and control group: did not receive any treatment.
The randomisation of the groups was performed by drawing a folded piece of paper in an opaque box, where two numbers could appear (1: intervention group; 2: control group). The researchers at the time of assessment are blinded to the assignment, as is the statistician when he receives the data from both groups, except for the physiotherapist who will teach the performance of the respiratory and neurological exercises to the intervention group.
To determine the sample size, it was calculated using the sample size calculation software G* Power 3.1.4.9.4 (University of Kiel, Germany), using the primary variable FVC from a previous study in post-COVID-19 patients
16
were sought with a two-tailed test, an α-error of 0.05 and a desired statistical power of 90% with an effect size of 0.5. A total of 98 participants were needed in each group. To avoid losses, an increase of 15% was planned, but in the end 209 patients were recruited. Finally, 200 patients finished the study and were divided into CG (n = 100; age 22 ± 13, being female 42 - male 58 and time to diagnosis after SARS-CoV-2 in days 220.52 ± 46.86) and IG (n = 100; age 23 ± 14, being female 59 - male 41 and time to diagnosis after SARS-CoV-2 in days 211.50 ± 40.52). The reasons for ineligibility and loss of subjects are indicated in the flow chart (Figure 1). Consort 2010 flow diagram.
Treatment protocol
A treatment plan was carried out for 31 days (Figure 2), in which the intervention group (IG) together with the control group (CG) were assessed in the laboratories of the Catholic A 31-day treatment plan was carried out (Figure 2), in which the intervention group (IG) together with the control group (CG) were assessed in the laboratories of the Catholic University of Avila at the respiratory and neurorehabilitative level on day 1 and day 31, on day 2 and day 30, both groups sent their dyspnoea-related scores via email to the investigators. The respiratory and gustatory-olfactory exercises were taught individually to the IG on day 1 in the laboratories of the Catholic University of Avila, and then they were asked to perform the exercises at home unsupervised on the remaining days, and then they were asked to perform the exercises at home unsupervised on the remaining days, as in previous studies in which they were taught face-to-face lung training on the first day and unsupervised on the remaining days in patients with bronchiectasis
17
or post-COVID-19.
18
Neurorehabilitation and respiratory treatment plan.
Intervention group
The rehabilitation programme (Figure 3) carried out in the IG consisted of olfactory and gustatory training, based on smelling a food odour, such as onion, and a non-food odour, such as detergent, once a day; on the other hand, it was also based on tasting four different tastes in a spoon, introducing each taste on the tongue: Sweet with sugar, salty with salt, sour with orange juice and bitter with coffee powder; this tasting was performed once a day and between each tasting the patients had to rinse their mouth with water to discriminate each taste. With regard to inspiratory muscle training, this was carried out with 5-min exercises using an inspiratory training device (PowerBreathe®, Powerbreathe España, 20140, Andoain, Spain) with individually marked resistance levels, depending on the specific assessment of each subject, in relation to the spirometric values of the MIP, from day 1 to day 30, where the treatment plan was 30 breaths, once a day for seven consecutive days, followed by a day of rest, after the inspiratory intervention, aerobic exercise “walking” was performed for 40 min from day 2 to day 30, once a day for five consecutive days, followed by a day of rest, as demonstrated by the cardiorespiratory study by Ress K, et al.
19
, at an intensity of 60%–75% of maximum heart rate and 50%–60% of maximum heart rate. The rehabilitation programme.
The treatment plan was based on previously published protocols, such as the study by Abodonya AM, et al. 20 Using an inspiratory training device for 2 weeks, consisting of two daily sessions, 5 days a week, in recovered intensive care unit (ICU) patients with COVID-19 after weaning from mechanical ventilation improved lung function, dyspnoea, functional capacity and quality of life. The systematic review by Alawna M, et al. 21 Shows that COVID-19 patients should follow a regular aerobic exercise programme for 20-60 min. This programme should consist of cycling or walking at an intensity of 55%–80% of VO2 max or 60%–80% of maximal heart rate. This programme should be repeated 2-3 times a week, as these parameters safely improve immune function without causing exhaustion in the study by Hummel et al., 22 neurological rehabilitation in patients with olfactory loss consisted of daily exposure to 4 odours (phenylethyl alcohol, eucalyptol, citronella and eugenol) over a period of 12 weeks, and Sheen F et al. 23 conducted a taste rehabilitation study in which post-COVID-19 patients received small amounts of powders selected to represent four prototypical tastes: “sweet” (table sugar), “salty” (table salt), “bitter” (granulated table salt, coffee powder) and “sour” (lime powder) for 28 days.
Outcome measures
Spirometry
The main variables studied and the process of carrying out the test are: Forced vital capacity (FVC), being the maximum volume of air exhaled at maximum effort, after having performed a maximum inspiration, represented in litres; the maximum volume of exhaled air (FEV1) in the first second of the forced vital capacity, represented in litres, the ratio between both FEV1/FVC, represented in % and the maximum inspiratory pressure (PImax) represented in cmH2O, to assess the inspiratory muscles. 24 The pulmonary function of the 200 patients was evaluated using the Datospir Touch Easy spirometer, with a transducer for individual disposable Lilly mouthpieces from Spirolab and PImax evaluation using the specific accessory of the same brand, in a 76 m2 room with outdoor ventilation, with the researcher wearing a disposable gown and gloves and an FFP2 mask. When the individual test was completed, the spirometer and its accessories were disinfected with cidex® opa solution and calibrated with Spirolab’s S3000 3L calibration syringe.
Modified borg scale
In relation to dyspnea and aerobic endurance, the subjects were assessed using the modified Borg subjective scale, for dyspnea and lower limb fatigue, ranging from grade 0 indicating rest to grade 10 indicating extreme effort and dyspnea. 25
Specifically, dyspnoea-related measurements were made on day 2 and day 30 in the post-intervention IG and non-intervention CG.
Modified medical research council (MMRC)
The scale provides specific data on dyspnoea and its relation to exercise or exertion, with grades ranging from 0 to 4, grade 0 being when dyspnoea appears only during very intense physical activity, i.e. heavy exertion, and grade 4 when dyspnoea appears during minimal exertion in activities of daily living such as dressing or activities that prevent the patient from leaving the home. 26
In detail, this was done on day 2 and day 30, in the post-intervention IG and in the non-intervention CG.
The Singapore smell and taste questionnaire (SSTQ)
Is a test for the patient to record via telematics the recent changes in the senses of smell and taste at the beginning and end of treatment, asking the questions: How is your sense of smell before treatment?; How is your sense of taste before treatment?; How was your sense of smell after treatment?; How is your sense of taste after treatment?; with a score from 0 no sense of smell or taste to 10 excellent sense of smell and taste. 23
In detail, the measurement was carried out on day 1 and day 31, in both groups.
Statistical analysis
The statistical analysis utilized IBM SPSS Statistics for Windows, version 28.0 (IBM Corp, Armonk, NY). The significance level was established at 0.05 (95% confidence interval [CI]), with a desired power of 80% (b error of 0.2). To assess the normality of the data, Kolmogorov-Smirnov test was initially employed. Descriptive analyses were conducted for both quantitative variables (minimum, maximum, mean, and standard deviation [SD]) and qualitative variables (absolute and relative frequency). For variables exhibiting normal distribution and homogeneity of variances (determined through Levene’s test), group comparisons were performed using either Student’s t-test or chi-square tests. When the distribution of the quantitative variables did not follow normality, Mann-Whitney U was employed for group comparison. A linear general model of analysis of variance (ANOVA) was employed to examine the effects of time (measurement moments: Pre and Post intervention) and intervention group (IG group and CG group). Intrasubject effects (measurement moments) and intersubject effects were evaluated using a repeated measures ANOVA or mixed factorial ANOVA, complemented by the Huynh-Feldt sphericity correction analysis. The effect size was estimated using the Eta2 Coefficient (0-0.3 small/0.4-0.6 medium, 0.7-1 large).
Results
Baseline comparison between groups (sociodemographic, descriptive and outcome measures).

Abbreviations: CG: Control Group; IG: Intervention Group; FVC: Forced vital capacity; FEV1: the maximum volume of exhaled air in the first second; FEV1/FVC: the ratio between both; PImax: the maximum inspiratory pressure; MBS: modified Borg Scale; MMRC: modified Medical Research Council; HS: How is your sense of smell before treatment?;HT: How is your sense of taste before treatment?.
aData expressed as Mean (standard deviation).
bData expressed as Median (interquartile range).
cX2 Test was applied.
dStudents t-test for independent samples was performed.
eMann-Whitney U test was applied.
For all analyses, p – value <0.05 (for a confidence interval of 95%) was considered as statistically significan.
Effectiveness of intervention versus control and differences in outcomes; time and group-time effects.
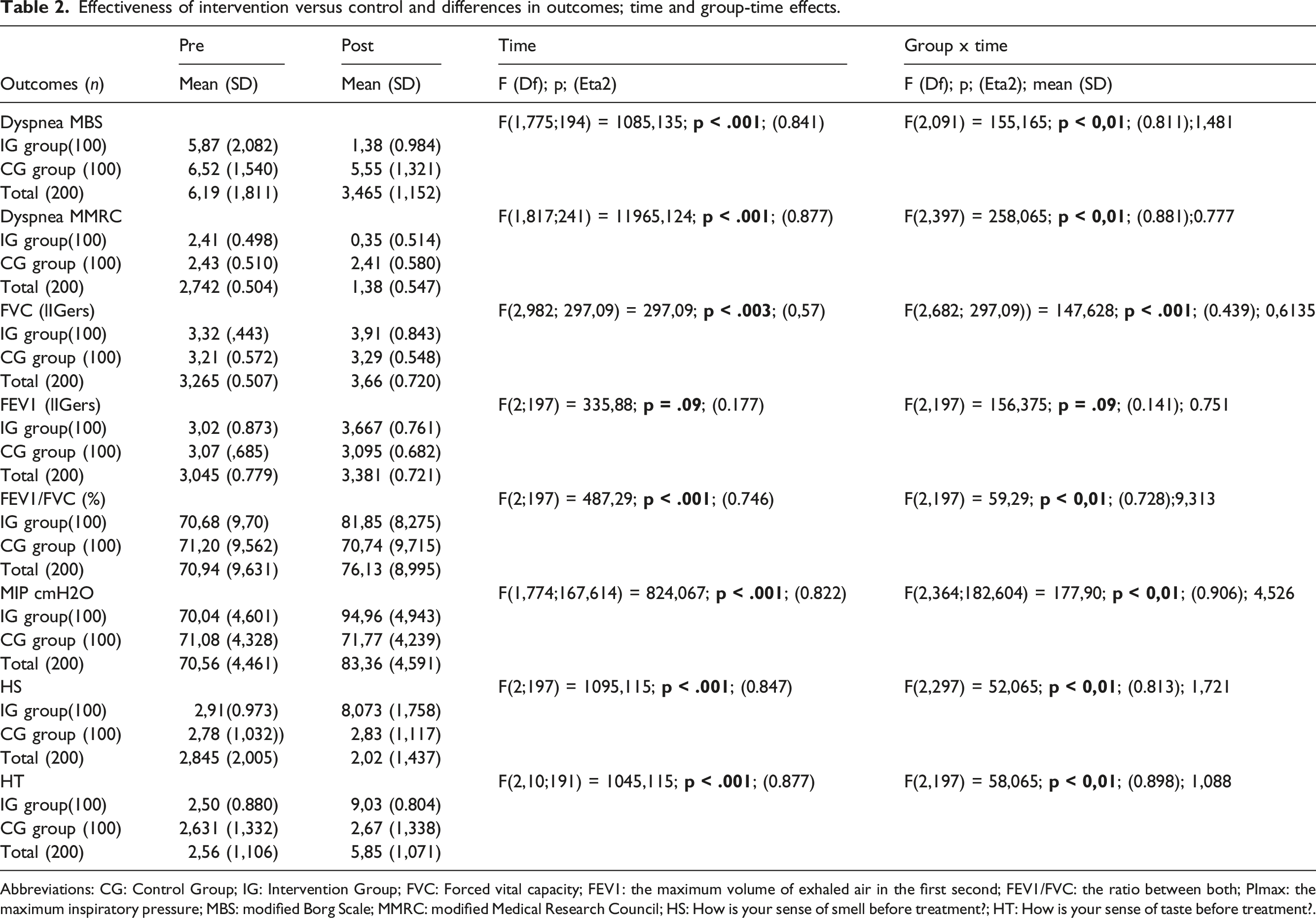
Abbreviations: CG: Control Group; IG: Intervention Group; FVC: Forced vital capacity; FEV1: the maximum volume of exhaled air in the first second; FEV1/FVC: the ratio between both; PImax: the maximum inspiratory pressure; MBS: modified Borg Scale; MMRC: modified Medical Research Council; HS: How is your sense of smell before treatment?; HT: How is your sense of taste before treatment?.
When considering the interaction between group and time, the IT group showed statistically significant differences in terms of improvement compared to the CG group, except for FEV1. The size effects are high, except for FVC (Eta2 = 0.439).
Discussion
Observational studies, such as those by Frizzelli A, et al. 27 and Güneş M, et al. 28 in subjects with previous SARS-CoV-2 infection who subsequently complained of unexplained and prolonged dyspnoea, with changes in resting and exercise breathing patterns measured by spirometry and a disability profile, suggest that pulmonary rehabilitation, including respiratory control techniques, could be helpful in reversing this unpleasant condition; related to loss of smell and taste, in the meta-analysis work by Tan BKJ, et al. 29 suggesting that these are major problems that could negatively affect quality of life, personal-social functioning, mental health and general health, as a significant population of patients could develop long-lasting dysfunction, thus recommending timely identification and personalised treatment; Therefore, the aim of this randomised controlled trial was to evaluate the effects of a respiratory and neurological rehabilitation programme, including a tool specifically designed for the inspiratory phase, aerobic exercise and gustatory and olfactory rehabilitation, compared to no treatment in patients after COVID-19. The IG programme improved dyspnoea parameters (MBS, MMRC) and spirometric values (FVC, FEV1/FVC and MIP) together with the neurological approach (HS, HT). The results support the benefits of using assistive technology along with aerobic exercise for respiratory training and neurological rehabilitation of taste and smell, showing statistically significant differences in all variables except FEV1.
The results of the present study support the use of an inspiratory device in combination with aerobic exercise in post-COVID-19 patients, as demonstrated by spirometry in the study by Toor H, et al. 30 in which 48 post-COVID-19 subjects performed an unsupervised home exercise programme with an inspiratory device, 20 min of walking and postural drainage to prevent upper airway obstruction, with a duration of the pulmonary programme of 30 days, showing improvement in peak inspiratory volume, or as in the study by Li J, et al. 31 in which the intervention was based on a 6-week unsupervised home exercise programme, similar to the present study. Where the intervention was based on a 6-week unsupervised home exercise programme, similar to the present study, but no significant effects on FEV1, FVC and FEV1/FVC ratio were observed. Discrepancies with our results could be explained by the fact that their intervention was exclusively online, whereas participants in the present study received more extensive individual training in person (on day 1). Despite the many advantages of telerehabilitation, as noted in the study by de la Plaza San Frutos, et al. 32 it is important to note that breathing exercises must be performed accurately to obtain their full benefits. On the other hand, Vorona S, et al. 33 carried out a review-meta-analysis of the efficacy of using an inspiratory muscle trainer, such as the Threshold® device, where, according to the scientific evidence, a significant increase in inspiratory muscle strength in critical patients was found, as well as an increase in the duration of ventilation or vital capacity, while in our study, we also found significant changes when using a device such as the Threshold® device, we also found significant changes when using an IMT device such as the Powerbreathe Plus® in post-SARS-CoV-2 patients, where after the treatment plan, spirometric values increased, therefore, dyspnoea decreased, effort capacity increased and, as there was a significant increase in PIMax, it indicates an increase in the strength of both the diaphragm and the external intercostal muscles.
In this study, no information was available on previous levels of physical activity. However, a recent study by Owen R, et al. 34 concluded that physical activity prior to infection may not offer significant advantages in the recovery process. With respect to the performance of aerobic exercise, the perception of dyspnoea and effort capacity were assessed using the MBS and MMRC scales, significantly improving the GI in 100% of patients with values of less than 5 in MBS and less than 2 in MMRC, unlike the study by Lau HMC, et al., 35 where aerobic exercise was performed in 133 patients after severe acute respiratory syndrome who were divided into 2 groups: one work group and one control group, assessing the effectiveness of aerobic training in the work group for 1 h, 4 or 5 days a week, with the aim of reducing dyspnoea, increasing effort capacity, vital capacity, and increasing respiratory muscle strength, significantly improving 80% of the patients in the work group.
The neurological approach to smell and taste, as assessed by the SSTQ questionnaire, supports the effectiveness of neurorehabilitative treatment as an innovative and promising approach. Moreover, this method is adaptable and may be the most convenient compared to other treatments aimed at restoring these senses, such as the use of corticosteroids, as demonstrated by Asvapoositkul V, et al. 36 in their meta-analysis, which may lead to dependence and cause side effects in at least a proportion of subjects. Additionally, this approach to improving or restoring smell and taste can be used in a variety of settings, both clinical and non-clinical. For example, it may be beneficial in neurodegenerative diseases, as demonstrated by Fatuzzo I, et al. 37 where olfactory dysfunction is a possible early marker, marker of disease progression and cognitive impairment of the onset of neurodegenerative diseases. 38 One aspect of our study that deserves some attention is the importance of testing this intervention on a relatively large number of participants and the inclusion of breathing exercises during the intervention sessions, which may have Finally, it should be noted that patients who manifest persistent symptoms with more than 5 months of evolution (Long-Covid) and do not receive any rehabilitative treatment may maintain their symptoms or worsen them as in the CG of this study, as also demonstrated in the systematic review by Oliveira Almeida K, et al. 39 the decrease in quality of life in post-Covid 19 patients, being of vital importance rehabilitation plans to improve disability, increase muscle strength and effort, as proposed by Fugazzaro S, et al. 40 in their systematic review, with an emphasis on increasing qualitative and quantitative studies to further demonstrate the importance of rehabilitation in Long-Covid patients.
The limitations of our study are that we did not carry out a third evaluation in both groups at the end of the study to observe whether the results obtained were maintained over time, and we did not evaluate exercise tolerance or health-related quality of life before and after the intervention. The participants included in this research were considered eligible for enrollment 5 months following their diagnosis of COVID-19. The study did not evaluate patients with severe symptoms.
In terms of the strengths of our work, the treatment plan that was applied produced very significant results, both at the respiratory, olfactory and gustatory levels. Despite the strict inclusion criteria, we were able to recruit 200 patients and the 100 patients randomised to GI followed the proposed treatment plan in its entirety.
Conclusion
The application of a respiratory rehabilitation treatment plan with the Powerbreathe® device, aerobic exercise and neurorehabilitation, is a therapeutic option against respiratory sequelae such as dyspnea and the approach to neurological sequelae with olfactory training with two smells and gustatory training with four tastes is also a therapeutic option against decreased gustatory and olfactory sensitivity in patients who have suffered such sequelae due to SARS-CoV-2 virus.
Footnotes
Acknowledgements
To all the participants who took part in the study and to the Catholic University of Avila, for making their laboratories available for the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.