
Abstract
Introduction
While research to treat the underlying cause of cystic fibrosis (CF) continues, symptom management and measures to improve quality of life remain the focus of care. 1 The impact of non-invasive ventilation (NIV) on clinical outcomes has been demonstrated,2,3 however, the lived experience of the adults using long-term NIV is yet to be investigated.
NIV was originally introduced as a ‘bridge’ to lung transplantation for people with CF in the early 1990s. 4 However, its use over the last 30 years as a treatment option has increased 5 and can slow the decline in FEV1.6,7 The benefits of NIV over invasive mechanical ventilation are that patients can be actively involved in treatment choices, whilst continuing to eat, drink and communicate. 8
Highly effective modulator therapies (HEMT), that treat the defective cystic fibrosis transmembrane regulator (CFTR) protein that causes CF, were first licenced in 2012 and have been more widely available for approximately 90% of adults with CF in the UK since 2020. 9 Randomised controlled trials (RCT) and real-world data have shown these can significantly improve FEV1. 10 However, despite this advance in treatment, some patients with CF of particular genotypes are ineligible, others cannot take modulators due to adverse interactions with other prescribed medications or are intolerant of their side effects. Recent data from the CF Trust shows respiratory disease is still the most common cause of death in adults with CF 9 indicating that NIV is still required as a form of supportive treatment. Consequently, clinical teams need to understand how the use of long-term domiciliary NIV affects quality of life and treatment burden.
An integrative literature review 11 did not identify any studies reporting the experiences of adults with CF using long-term NIV for respiratory failure. Research into the patient perception of NIV is essential if multi-disciplinary teams (MDT) are to provide appropriate support for these patients.
Methods
This is a descriptive qualitative study using a content analysis method to explore the lived experience of adults with CF using long-term domiciliary NIV.
Recruitment and sampling
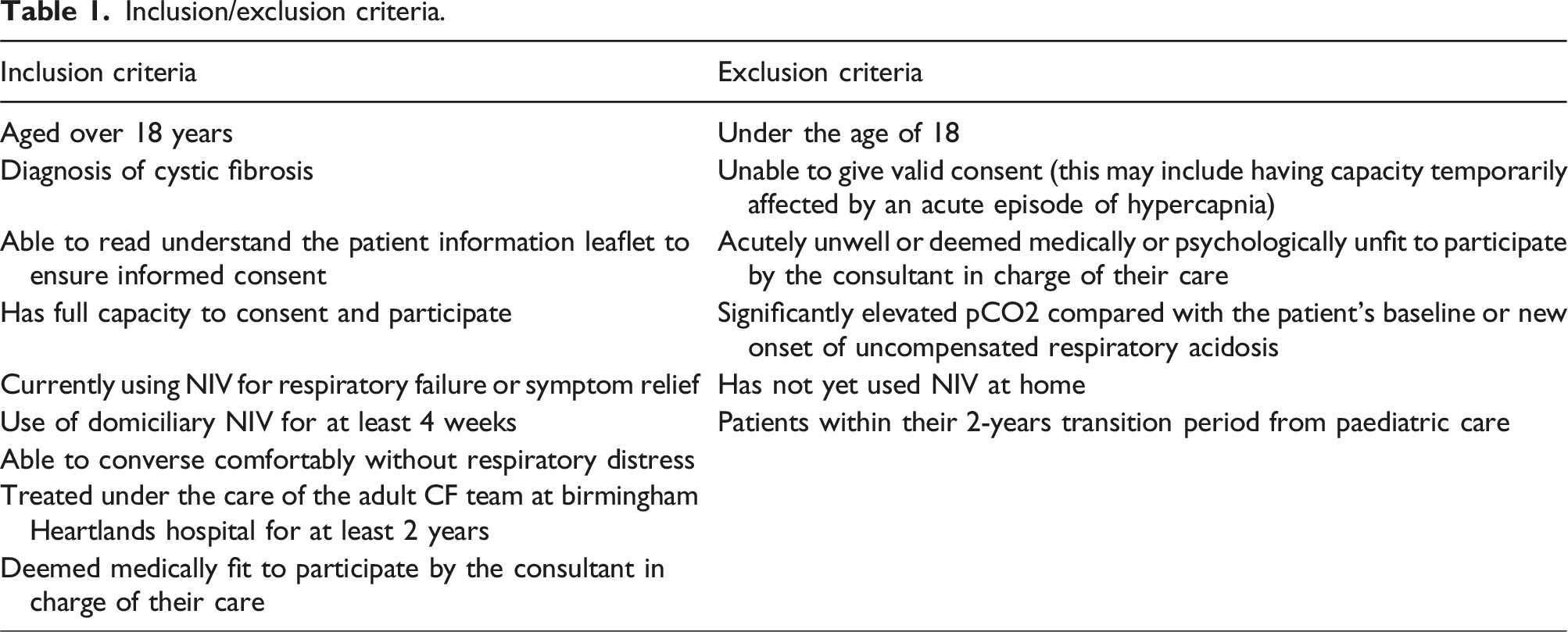
Adults with CF who had used domiciliary NIV, for respiratory failure, for more than 4 weeks, were suitable to take part. Using a database, held by the physiotherapy team, 11 patients were found to be eligible (Table 1). A purposive sample was selected 12 and a target sample size of 10 was set. 13
Inclusion/exclusion criteria.
Data collection
Interview guide.

Interviews were conducted in a quiet, private room in the patient’s usual hospital by a member of the specialist CF physiotherapy team (JC), taking an average of 1 h per participant. To support reflexivity JC made field notes immediately after each interview.
Data analysis
The qualitative data were subject to thematic analysis using Braun and Clarke’s six-phase approach. 15 Interviews were transcribed verbatim and reviewed line by line to familiarise the researchers (JC, AH and AS) with the content and identify initial codes. Transcripts were then read and re-read and each member of the team coded each data set independently. The team then met to collate the codes and group them into potential themes with each researcher presenting extracts of coded data to support each theme. The codes were entered into a matrix to summarise the large descriptive data set, enabling JC to systematically identify and refine themes and subthemes in the dataset. The themes were then, reviewed and cross-checked, to confirm their dependability and credibility 16 with regard to the aim of the research.
This work was conducted following the principles of the Declaration of Helsinki and was granted ethical approval by East Midlands Research Ethics Committee 17/EM/0321 (IRAS Reference 225,296). The findings are reported in accordance with the COREQ guidelines.
Results
Participant demographics.

Two patients initially expressed an interest but subsequently declined and were not interviewed. One had become more unwell and was heavily reliant on the NIV, so was unable to manage prolonged periods off the ventilator for the interview, and the second felt the interview would overburden her during what for her was an already emotionally and physically difficult period of her life. Of the nine participants, eight had been referred for lung transplant assessment; five were on an active lung transplant list and three were under regular review. Despite being eligible, one patient had declined a transplant. The participants had been using domiciliary NIV for a median of 48 months (12-60) prior to the interviews. No patients were taking CFTR modulator therapies, such as Kaftrio, at the time of interview. Although objective adherence to, or time spent on, NIV was not formally measured in this study, it was felt all patients spoke honestly about how often they used NIV, discussing the benefits and side effects based on their own experience.
Development of the themes
Summary of themes and subthemes.

Themes
Gratitude
The theme of gratitude was derived from four subthemes: the ability to live a fulfilling life, relationship and communication with the MDT, physical benefits of NIV, and relationship with NIV.
Ability to live a fulfilling life
Participants were grateful that NIV enabled them to continue to live fulfilling lives. They felt NIV allowed their body and lungs to “fully rest”, and they were able to wake up with energy “feeling refreshed”. For example: “you’re able to have a full night’s sleep, you’re able to have a break and a body rest….you’re not working so hard, and then to start your day off good” (P7)
Self-care was reported to be less of a struggle and participants were able to engage in a range of activities: “I can do things more through the day that I want to be doing” (P3)
Relationship and communication with the MDT
For most participants (6/9), NIV was initiated by a CF specialist physiotherapist with whom they had developed a trusting relationship. Participants commented in positive terms about their care and stated how grateful they were to have a familiar member of staff introduce them to the NIV. The extracts below illustrate how this was key to them accepting and continuing the treatment: “I had found that having a familiar physio show me how to do it and found having someone I knew and I trusted really really beneficial. I think if it was someone I didn’t know so well I would have been even more wary” (P9)
and “I can’t sing its praises enough, because if you feel confident with somebody, for me personally that’s half the battle because you’re trusting somebody” (P5)
However, participants acknowledged the difficulties faced by the clinical team in identifying the best time to start NIV due to the unpredictability of the progression of the disease. Participants valued the MDT’s knowledge and support in choosing an appropriate time to initiate treatment. Those who started NIV during an acute exacerbation indicated they would not have wanted to start it any earlier as they had not appreciated how ill they were. “I wouldn’t have needed it before because my lungs changed really quickly, so like a week before that I had been running around at meetings and I’d been in London, so if someone had said to me then ‘oh do you want some NIV?’ like I’d just been like ‘erm no, shut up’” (P8)
While the patients had a good quality of life they would have been unwilling to accept the introduction of a new intrusive treatment. However, once NIV was started and its benefits felt, they recognised their condition would have deteriorated were it not for the timely introduction of NIV. “I think I’d be long gone [without the NIV] to be honest. I think I would have really really struggled” (P9)
and “I think if I hadn’t had it I would have had major problems” (P1)
Physical benefits of NIV
Participants reported improvements in their sleep quality with NIV. They experienced deeper and more settled sleep and woke up feeling more energetic and “alive”: “I don’t wake up with my heart racing unable to breathe properly” (P7)
and “I think it’s a lot better, I can get into a deeper sleep and not worry” (P3)
As participants became more confident in using NIV independently at home, they felt more relaxed when wearing the device, “it relaxed me, because I realised when I put it on I felt more comfortable” (P5)
One participant was even able to stop taking anxiolytics because the NIV was effective in preventing their panic attacks, “there is nothing out there that can give you the sense of ‘wow’ like that did” (P7)
Relationship with NIV
Participants talked fondly about their NIV, expressing how grateful they felt to have the treatment: “It’s a bit of a comfort blanket…it’s nice to know it’s there, it makes me feel safer”(P4)
and “I’d be lost without it” (P8)
However, they also discussed that starting NIV forced them to acknowledge their deteriorating health as a consequence of their illness trajectory. “without it you’d basically be like a cabbage on the sofa” (P3)
and “I still don’t like I’m at the stage that I’ve got to be on it, but I know that it is doing its job. If I’ve got to wear this 24/7 then what sort of life am I going to have, it’s quite frightening” (P2)
They reported that previously effective treatments were becoming less so over time, and believed their condition would have deteriorated more rapidly without NIV. “even though I was getting medication with my IVs, I wasn’t bouncing back” (P5)
They explained how they relied on it and described the profound effects it had on their emotional well-being and life. “…it’s a massive cog, because it has had a good effect on my life…it’s been positive without a shadow of a doubt” (P5)
The positive response to treatment expedited adaption to using NIV long-term, which is explored further below.
Determination despite challenges
The second main theme to emerge, determination despite challenges, is comprised of 2 subthemes: determination to accept treatment despite frightening preconceptions, and determination to continue with NIV despite its unpleasant side effects.
Determination to accept treatment despite frightening preconceptions
Participants explained that before starting NIV, they had negative preconceptions and were frightened of using it. Yet despite this, participants were determined to try NIV to get relief from their debilitating symptoms. “…when people said they were on it on the ward, probably within a couple of weeks they were dead!” (P2)
and “I was very wary, I was a bit unsure because when you see people with it you always think that they are kind of at the end stage” (P9)
However, many were positive about NIV and had not found it to be as frightening as they expected. They suggested that those considering its adoption should be reassured and their anxieties allayed. “Don’t be frightened. You’ve got to think if it helps you, stick with it, ‘cos in the long run it will help you” (P1)
and “don’t be frightened, it becomes your friend” (P2)
They considered NIV to be a challenging, but viable alternative to invasive mechanical ventilation. “it’s the lesser of two evils, I was going to be intubated and once cystics get intubated, they don’t come off, they were my options…have this or you'll die” (P6)
The participants acknowledged that NIV would not suit everyone, but they all recommended other patients in a similar situation try NIV. “I think you should give it a good go and then you can say yay or nay, if you don’t give it a good go you can’t really say to be honest” (P5)
and “usually when they start me on new equipment I haven’t usually got much good to say about it, but this I would strongly suggest go for it” (P4)
and “…go for it, because the benefits of it are a lot more than you probably initially think and it will be able to give you like more energy to do things that you want to do” (P3)
Determination to continue with NIV despite unpleasant side effects
All participants experienced unpleasant physical side effects from NIV including abdominal bloating, night-time disturbance caused by the noise of the machine, and facial pressure sores caused by friction from the mask. However, they continued using NIV because of its benefits of symptom relief and improved quality of life. “I was getting a rash from the mask...I was at my wits end with the rash” (P2)
and “I have to be careful because I do get really bloated and it is painful” (P4)
One participant joked that NIV gave them “serious farts” but felt humour helped minimise the negative psychological impact and helped them cope with the continuing treatment.
Participants also experienced psychological side effects from the NIV including low self-esteem (3/9). “I must have looked like some sort of freak and I thought, I can’t cope with this”(P2)
and “I’ve got a bit of a warped way of looking at things, like I’m a lesser person” (P5)
Others (4/9) mentioned that their partners had responded negatively to the NIV, which was upsetting, “my girlfriend punches me in the middle of the night if the mask has been farting” (P6)
and “he moans when I get him cold, so I will turn the opposite way so it’s not blowing on him” (P3)
and two participants commented on the impact NIV had on the intimacy with their partners: “I don’t think it’s helped our sex life because he won’t sleep in the same room as me now” (P9)
and “we are not as touchy-feely as we used to be” (P2)
Despite these distressing psychological side effects, all nine participants continued using NIV and reported their determination to derive as much benefit as possible from the treatment.
Discussion
It is known that NIV can improve a variety of clinical parameters including nocturnal CO2, dyspnoea scores, and exercise performance, whilst slowing the decline in FEV1.3,6,7,17,18 However, there is currently limited evidence of the qualitative practical and psychosocial impact of this treatment on patients' lived experiences.
This is the first study we are aware of that has investigated the experiences of adults with CF using long-term domiciliary NIV for respiratory failure. The insights provided by the participants in this study supplement existing evidence and add to our understanding of the implications of NIV for this group of patients. NIV can reduce hypercapnia 19,20 and the participants in this study reported that it also relieved shortness of breath and anxiety and improved their sleep quality. Having more restful sleep meant they woke with more energy which enabled them to engage in enjoyable activities such as crafts and shopping, which in turn improved their mood and gave a feeling of fulfilment.
However, NIV can have unpleasant side effects, 21 with the participants in this study reporting abdominal bloating, night-time disturbance caused by the noise of the machine and facial pressure sores. The respondents also reported the psychological and emotional impact of NIV. They experienced embarrassment, felt vulnerable, and noted the negative effect it had on their self-esteem and relationships. Yet despite these adverse effects, the participants continued with NIV, suggesting its benefits outweigh its disadvantages. Knowledge of these potential effects is important for practitioners, so they can provide informed holistic care, and offer appropriate psychological and emotional support for patients and their close persons. Despite the increase in treatment burden with NIV, 5 and its side effects, all the respondents expressed their determination to continue with NIV.
These results reinforce those from a study investigating the experiences of adults with CF using NIV as an adjunct to airway clearance. 22 The main theme in the findings was “Becoming friends with NIV”. The participants reported having feelings of doubt and were initially motivated by fear of deterioration, but as they became more experienced with using the device, they appreciated its benefits for their physical health and quality of life. In a study 23 involving patients with Chronic Obstructive Pulmonary Disease (COPD) who had either had at least 2 episodes of acute NIV or had past or current domiciliary NIV use, participants were interviewed about their experiences. They reported some negative side effects of NIV (such as discomfort, oral dryness and noise), however the positive impact on their symptoms outweighed these and they continued to use the NIV.
The Cochrane review of the use of NIV in CF 2 concluded further research was needed to establish its long-term benefits. The median length of NIV use in the present study was 48 months, with four participants having over 5 years’ experience of domiciliary NIV. All participants reported sustained benefits, indicating there are longer-term benefits of NIV than those identified in previous research.
Strengths and limitations
The rigorous sampling of participants ensured those with relevant experience were recruited. Interviews were well tolerated, and participants were relaxed and willing to discuss their experience of using NIV. The potential risk of researcher bias, in relation to the COREQ guidelines, was acknowledged. 24 As the interviewer was known to participants, they may have responded in a way they felt was more socially acceptable or may have avoided talking about their experience negatively so as not to offend the clinical team, and/or potentially jeopardise their future treatment. However, the participants seemed confident in talking openly about their experience and having a trusted clinician as the interviewer put participants at ease, facilitating a more insightful and honest discussion. Interviews gave participants time and space to discuss their experiences, producing “thick description” 25 of what life is like when using long-term domiciliary NIV. The credibility of the data analysis was enhanced by analyst triangulation. 26
The sample size could be regarded as a limitation however, there is no consensus on sample size in qualitative research. Guidance states that “judgement and experience” should determine a sample size sufficient to provide effective evaluation and support the aims of the research26,15 suggesting that interviewing 6-10 participants is appropriate for an exploratory project such as this. Given that 82% of the eligible subjects in our large centre took part, this requirement was met. Similar themes emerged in the interviews indicating data saturation was achieved. A follow up, multi-centre study involving more participants would be helpful in further confirming the transferability of these themes.
The requirement for this study was that participants were currently using NIV, however, there is a group of patients who have used NIV, but for a range of reasons had stopped using it. These include poor tolerance of masks or pressures, adverse events or contraindications such as pneumothorax or severe haemoptysis, or the patient has chosen to discontinue treatment. A preliminary search found no studies reporting the experiences of this group. It would be helpful to explore how their experiences compare to the participants of this study.
The single-centre design meant that all the participants were treated by the same clinical team and used the same model of NIV machine (ResMed StellarTM 150), therefore a larger, multi-centre study would be helpful to explore the experiences of patients from other units, cared for by different teams and using a variety of machines and modes.
Implications for future practice and further research
A large multi-centre study would provide an opportunity to explore the recommendation from the Cochrane review 2 to investigate which subgroups may benefit most from NIV and how the use of NIV may evolve as the clinical condition deteriorates. Such a study would also explore the research priority “What is the best approach for end-of-life care in people with cystic fibrosis?”. 27 In particular, it is important to investigate if individuals listed for transplantation reflect on their experiences of using NIV differently from those who have either decided they do not want a transplant or are not eligible for one for clinical reasons. Larger studies, in the post-CFTR modulator era, would explore how these medications affect the natural progression of CF as a multi-system disease and if the role of NIV has changed significantly since their introduction.
Such information will help guide teams to make complex decisions, in partnership with patients, providing insight into their wishes for end-of-life care and help inform advance care plans.
Conclusion
The physical benefits of NIV in CF are now widely recognised. While originally used as a short-term ‘bridge’ to transplant it is now part of routine care, often initiated earlier in the disease process to maximise airway clearance and treat early signs and symptoms of respiratory failure. Clinical teams must take a patient-centred approach when treating adults with CF 28 and discuss the initiation of a treatment they may need to use for many months or even years towards the end of their life. Whilst the findings of this study provide initial insights about patients’ experience of NIV, they also highlight the need for further research to ensure patients who could benefit from its use are introduced to NIV at the optimal time and given the best holistic care during this difficult phase of their disease.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.