
Abstract
Objectives
Chronic respiratory diseases (CRDs) are a burden on both individuals and society. While previous literature has highlighted the clinical burden and total costs of care, it has not addressed patients’ direct payments. This study aimed to estimate the incremental healthcare costs associated with patients with CRDs, specifically out-of-pocket (OOP) costs.
Methods
We used survey data from the 2019 Korea Health Panel Survey to estimate the total OOP costs of CRDs by comparing the annual hospitalizations, outpatient visits, emergency room visits, and medications of patients with and without CRDs. Generalized linear regression models controlled for differences in other characteristics between groups.
Results
We identified 222 patients with CRDs, of whom 166 were aged 65 years and older. Compared with the non-CRD group, CRD patients spent more on OOP costs (238.3 USD on average). Incremental costs were driven by outpatient visits and medications, which are subject to a coinsurance of 30% or more and may include items not covered by public insurance. Moreover, CRD patients aged 50–64 years incurred the highest incremental costs.
Discussion
The financial burden associated with CRDs is significant, and outpatient visits and medications constitute the largest components of OOP spending. Policymakers should introduce appropriate strategies to reduce CRD-associated burdens.
Keywords
Introduction
Chronic respiratory diseases (CRDs) are among the leading causes of morbidity and mortality, constituting a serious public health issue worldwide. 1 Chronic obstructive pulmonary disease (COPD), asthma, and rhinitis are the most common CRDs and have become a major health priority in South Korea. 2 These CRDs result in a substantial economic burden for affected individuals. 3
The incremental approach uses a regression method to calculate the incremental utilization and costs incurred.4,5 Previous studies have suggested that this approach estimates the utilization and costs incurred more appropriately by reflecting the difference between people with and without diseases.4,5 Therefore, it is essential to understand the healthcare utilization and out-of-pocket (OOP) costs associated with CRDs using an incremental approach.
Research has demonstrated that CRDs are associated with a high disease burden.6–11 In asthma cases, hospitalization and medications are the most important drivers of direct costs. 6 Most direct costs associated with COPD were due to inpatient hospitalizations. 7 Furthermore, COPD patients report poor symptom control and considerable use of healthcare utilization. 7 Emphysema patients also undergo hospitalization, and medication costs account for the majority of their total healthcare costs. 8 Many studies have focused on patients with individual diseases such as COPD and asthma.9–11 As asthma, bronchiectasis, emphysema, and COPD are organically connected to one another, it may be necessary to consider healthcare utilization and costs as a whole.12,13 Most papers examined payments for covered National Health Insurance (NHI) coverage and patient copayments. Moreover, while the literature thus far has tended to highlight the clinical burden or total cost of care, it has largely failed to address payments made directly by patients. Hence, this study provides valuable insights from the patient’s perspective and emphasizes total OOP costs, including payments for uncovered NHI and statutory OOP costs.
This study aimed to estimate the incremental healthcare costs associated with CRDs using an incremental cost approach. As the incidence of CRDs notably increases with age and exhibits a strong increase in older individuals, 14 this study aimed to specifically identify and categorize incremental healthcare utilization and OOP costs by age group. In addition, this study aimed to determine the annual incremental OOP costs stratified by annual household income and comorbidities.
Materials and methods
Data source and study population
We used data from the 2019 Korea Health Panel Survey (KHPS), an official statistical investigation that has been conducted annually since 2008 under the supervision of the Korea Institute for Health and Social Affairs (KIHSA) and the National Health Insurance Service. 15 The KHPS aims to provide baseline data for the formulation and improvement of healthcare and health insurance policies by examining data on healthcare utilization, costs, and insurance coverage. 16 The KHPS employs two-stage stratified random cluster sampling based on the population and housing census, which covers the entire Korean population. The data include divers of variables such as individuals’ socio-economic characteristics, health behavior, and other related aspects of healthcare utilization. Additionally, the KHPS provides reliable data on healthcare costs as it prevents loss of information and recall bias errors thanks to health insurance data and receipt checks. 17 For this study, we only used public data from the KHPS that had no personally identifiable information. Ethical and governance approvals were granted by the KIHSA. All participants provided informed consent.
A total of, 14,741 individuals were retrieved from the 2019 KHPS database. We excluded those who answered, “I don’t know,” declined to answer the questions included in the study or had missing data. The final sample consisted of 11,320 individuals.
Dependent variable
Incremental healthcare utilization and OOP costs were calculated as the difference between the two groups over a 1-year period. Direct non-medical costs were not included, in accordance with the study purpose. The outcome measures were (1) 1-year incremental healthcare utilization for hospital admissions, emergency room (ER) visits, and outpatient visits and (2) 1-year incremental healthcare OOP costs for hospital admissions, ER and outpatient visits, and prescription medication use. 1 Healthcare OOP costs are defined as payments for uncovered NHI and statutory OOP costs. The Korean won (KRW) was then converted into USD by applying an exchange rate of 1272 KRW per 1 USD (as of June 13, 2023).
Variable of interest
The variable of interest was the presence or absence of CRDs. The KHPS classifies asthma, COPD, emphysema, and bronchiectasis as CRDs. 18 Likewise, in this study, the presence of CRDs was defined as the prevalence of at least one of these conditions. Participants without the aforementioned diagnoses were included in the non-CRD group.
Control variables
In this study, we selected control variables that appeared to be related to individuals’ healthcare utilization and OOP payments in previous studies,12,18 including sex, age group, marital status, educational status, insurance type, purchase of private health insurance, household income, job, smoking status, and comorbid diseases.
Statistical analysis
All analyses of the complex sample survey data were performed by applying weights according to the complex samples provided by the KHPS. Frequency distributions were developed, and Rao–Scott chi-square tests were used to assess the statistical differences between participants with and without CRDs, specifically to determine the differences in annual healthcare utilization and healthcare costs according to the presence of CRDs. We used a generalized linear regression model adjusted for the control variables. We employed a generalized estimating equation with a robust standard error to avoid overestimating the standard errors of the parameter estimates. In addition, a subgroup analysis was performed to determine the annual incremental OOP costs, stratified by age group, annual household income, and comorbidities. All calculated p values were two-sided, and p values <0.05 were considered significant. All analyses were performed using SAS software (version 9.4; SAS Institute, Cary, NC, USA).
Results
Distribution of individuals by characteristics
Distribution by characteristics for the total sample and CRD and non-CRD groups (n = 11,320).

CRDs: chronic respiratory diseases.
Statistically significant values are bolded.
Differences in annual healthcare utilization and OOP costs
Differences in annual healthcare utilization.

CRDs: chronic respiratory diseases; CI: confidence interval; OOP: out-of-pocket payment; ER: emergency room.
Statistically significant values are bolded.
Differences in annual OOP costs.

*The Korean won was converted to USD by applying an exchange rate of 1272 KRW per 1 USD (as of June 13, 2023).
CRDs: chronic respiratory diseases; CI: confidence interval; OOP: out-of-pocket payment; ER: emergency room.
Statistically significant values are bolded.
The CRD group had significantly higher inpatient (96 USD; p = .0006), ER visits (13.8 USD; p = .0208), and total OOP (377.7 USD; p < 0.0001) costs than the non-CRD group.
Association between CRDs and incremental annual healthcare utilization
Association between CRDs and annual incremental utilization and OOP costs.

*We adjusted for all the covariates including age, sex, socioeconomic status, and comorbidities. The Korean won was converted to USD by applying an exchange rate of 1272 KRW per 1 USD (as of June 13, 2023).
CRDs: chronic respiratory diseases; CI: confidence interval; OOP: out-of-pocket payment; ER: emergency room.
Statistically significant values are bolded.
Association between CRDs and incremental annual OOP costs
Table 4 also illustrates the association between CRDs and incremental annual OOP costs adjusted for covariates, including age, sex, socioeconomic status, and comorbidities. The annual total OOP costs were significantly higher for individuals with CRDs than those without CRDs at 238.3 USD (p = .0105). The annual costs according to visits were greater for individuals with CRDs, including inpatients (57.9 USD; p = .3647) and outpatients (93.6 USD; p = .0958); however, this difference was not statistically significant. Annual ER costs were significantly higher for individuals with CRDs (12.0 USD; p = .0004). Annual medication costs were significantly higher for individuals with CRDs (74.8 USD; p < 0.0001).
Results of subgroup analysis stratified by age group, annual household income, and comorbidities
Figure 1 shows the findings of the incremental annual healthcare utilization stratified by age group, annual household income, and comorbidities. The results showed incremental healthcare utilization for individuals with and without CRDs in the same age group, household income, and status of comorbidities analyzed by adjusting control variables. Association between CRDs and incremental annual healthcare utilization stratified by age group, annual household income, and comorbidities. * The results showed incremental healthcare utilization for people with and without CRD in the same age group, household income, and status of comorbidities analyzed by adjusting control variables.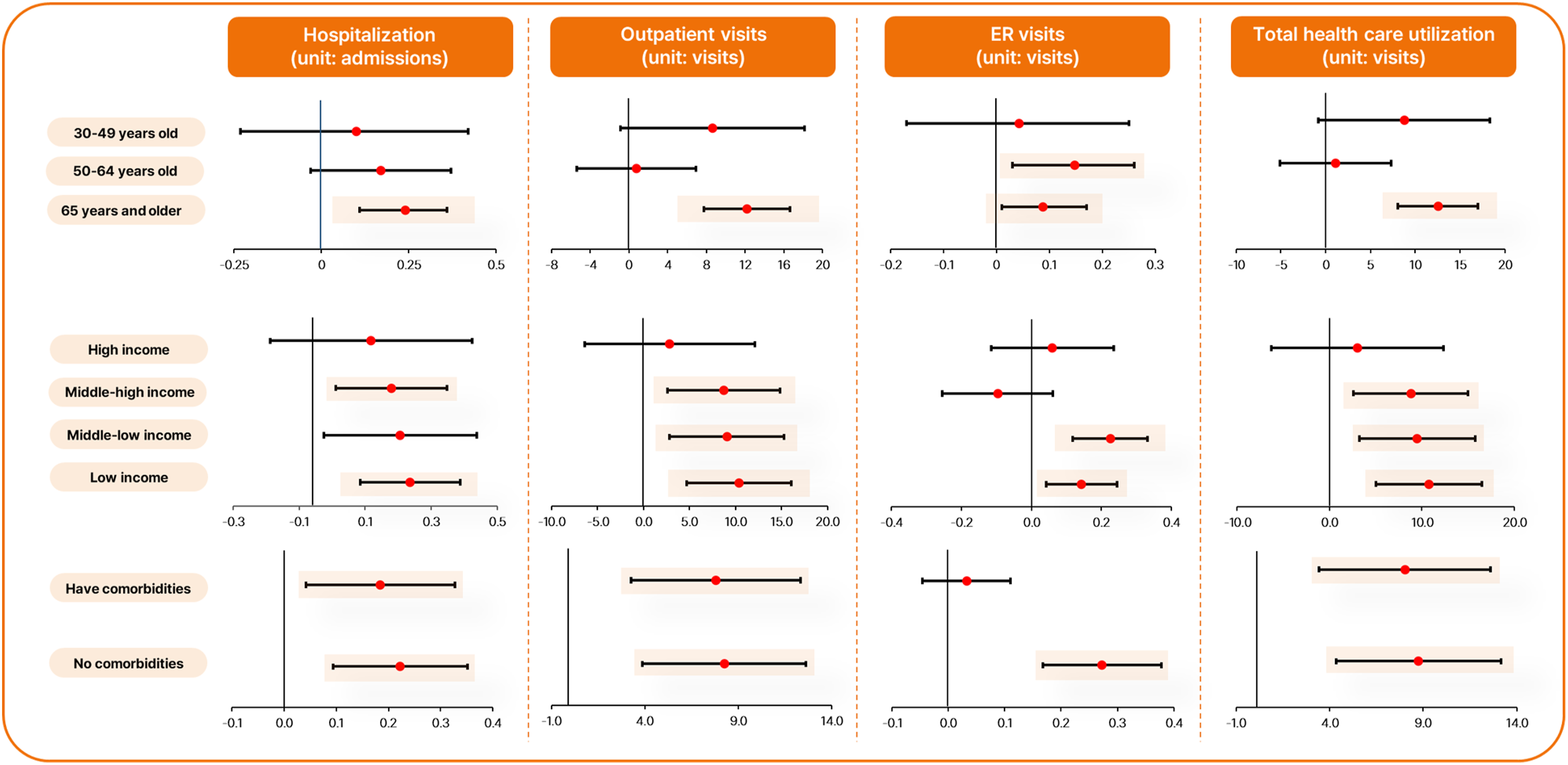
The annual incremental healthcare utilization showed a significant difference for CRD patients aged 65 years and older in hospitalizations (0.24 admissions; p = .0002), outpatient visits (12.21 visits; p < 0.0001), and ER visits (0.09 visits; p = .0336). The annual incremental healthcare utilization showed a significant difference for CRD patients aged 50–64 years in ER visits (0.15 visits; p = .0122). Total healthcare utilization (12.53 visits; p < 0.0001) was significantly increased in patients aged 65 years and older with CRDs.
Annual incremental healthcare utilization was significantly different for CRD patients with middle–high annual household income in hospitalizations (0.18 admissions; p = .0364), outpatient visits (8.71 visits; p = .0053), and total healthcare utilization (8.79 visits; p = .0053). The annual incremental healthcare utilization was significantly different for CRD patients with low–middle income in outpatient visits (9.06 visits; p = .0043), ER visits (0.23 visits; p < 0.0001), and total healthcare utilization (9.49 visits; p = .0030). Annual incremental healthcare utilization was significantly different for CRD patients with low income in hospitalizations (0.24 admissions; p = .0022), outpatient visits (10.36 visits; p = .0004), ER visits (0.14 visits; p = .0056), and total healthcare utilization (10.74 visits; p = .0002).
Annual incremental healthcare utilization was significantly different for CRD patients without comorbidities in hospitalizations (0.22 admissions; p = .0007), outpatient visits (8.26 visits; p = .0002), ER visits (0.27 visits; p < 0.0001), and total healthcare utilization (8.76 visits; p = .0001). Annual incremental healthcare utilization showed a significant difference for CRD patients with comorbidities in hospitalizations (0.18 admissions; p = .0113), outpatient visits (7.81 visits; p = .0008), and total healthcare utilization (8.03 visits; p = .0006).
Figure 2 shows the annual incremental OOP costs stratified by age group, annual household income, and comorbidities. The results showed incremental OOP costs for individuals with and without CRDs in the same age group, household income, and status of comorbidities analyzed by adjusting control variables. The annual incremental OOP costs were significantly different in patients with CRDs aged 65 years and older in terms of inpatient costs (242.2 USD; p = .0454), ER costs (35.2 USD; p < 0.0001), and total OOP costs (534.6 USD; p = .0078). Annual medication costs were greater among patients aged 30–49 years with CRDs (112.7 USD; p < 0.0001) than among those aged 30–49 years without CRDs. Additionally, annual medication costs were found to be higher in patients with CRDs aged 65 years and older (89.5 USD; p < 0.0001). Association between CRDs and incremental annual OOP costs stratified by age group, annual household income, and comorbidities. * The results showed incremental OOP costs for people with and without CRD in the same age group, household income, and status of comorbidities analyzed by adjusting control variables.
The annual incremental OOP costs were significantly different for CRD patients with high income in terms of outpatient costs (787.5 USD; p = .0002), medication costs (81.6 USD; p = .0092), and total OOP costs (816.6 USD; p = .0246). The annual incremental OOP costs were significantly different for CRD patients with low–middle income in terms of ER costs (40.9 USD; p < 0.0001), and medication costs (57.7 USD; p = .0080). Annual medication costs were greater among CRD patients with middle–high income (112.3 USD; p < 0.0001) than among those with low–middle income without CRDs. Additionally, the annual medication costs were found to be higher in CRD patients with low income (62.7 USD; p < 0.0001).
There was a significant difference in annual incremental OOP costs for CRD patients without comorbidities in terms of outpatient (219.4 USD; p = .0267), ER (32.4 USD; p < 0.0001), medication (62.3 USD; p < 0.0001), and total OOP costs (536.7 USD; p = .0001). Annual medication costs were higher among CRD patients with comorbidities (77.3 USD; p < 0.0001) than among those without comorbidities.
Discussion
This study aimed to estimate the annual incremental healthcare utilization and OOP costs associated with CRDs, including the most common types such as asthma, COPD, emphysema, and bronchiectasis. We found that the individuals with the highest percentage of CRDs were male, 65 years of age and older, and less educated. Older age has been well documented as a factor that influences the effects of CRDs, such as COPD, which tend to increase among older adults.7,13,19–24 Participants with CRDs had a higher frequency of low income, current smoking status, and comorbidities. Previous research has reported that smoking and socioeconomic status have a substantial impact on increasing respiratory diseases, and children of smokers living in poor housing environments are more likely to develop respiratory diseases.6,10,14,16,18 Lung infection and related respiratory disorders have been shown to be most strongly linked to diabetes and cardiovascular diseases,5,23,25,26 which are particularly likely to increase healthcare utilization and costs if they are present as comorbidities.
Our findings provide the latest incremental estimates of healthcare utilization and OOP costs for CRDs after adjusting for demographic characteristics and comorbidities. Overall, consistent with the findings of previous studies, patients with CRDs had higher healthcare utilization and OOP costs than those without CRDs.5,7–9 However, these results are not directly comparable with those of other studies because of differences in health insurance policies, methodologies, and data sources.
Individuals with CRDs had significantly higher incremental annual utilization in all healthcare settings than those without CRDs. Outpatient visits (8.71 visits), hospitalization (0.21 times), and ER visits (0.1 visits) were statistically significant among individuals with CRDs. The high frequency of outpatient visits likely stems from the fact that patients need to regularly visit outpatient clinics to assess and follow up on disease progression, medication side effects, and acute exacerbations of comorbidity progression.6,19
The incremental OOP costs were 238.3 USD in the CRD group, when excess costs were adjusted for comorbidities and other factors. Additionally, as discussed previously, outpatient visits and medication costs account for a substantial portion of CRD costs. Previous studies have shown similar findings for asthma and COPD in the Asia-Pacific region.3,15 A study investigating the economic burden of CRDs found management costs to be the main driver of CRDs-related costs.3,15 Previous studies also estimated that medication prescriptions accounted for a greater proportion of total respiratory-related multimorbidity medical costs compared to other diseases.3,9–11,20,21 However, the higher medication costs were due to new or more expensive treatments according to disease severity.
Our findings on annual cost differences revealed that hospitalization costs were higher than outpatient and ER visits for patients with CRDs. Higher inpatient costs are associated with respiratory diseases, such as COPD and asthma, depending on the severity of the conditions. As per previous studies, higher hospitalization costs for COPD and related cases were also reported: 8238 USD for asthma and 27,597 USD for COPD in the USA, 22 4936 USD in Canada, 23 1952 USD in China, 27 and 474 USD in Iran. 28 Thus, high hospitalization costs for CRD patients are linked with age, length of stay, disease severity, and complications. Certain aspects can be categorized as self-factors, whereas others are linked to hospital treatment procedures. Estimating the direct cost of CRD while providing suggestions for reducing the economic burden on patients’ needs requires in-depth knowledge of hospitalization costs and related factors for CRD cases.
In addition, the adjusted age and related control variable-based subgroup analysis results revealed that incremental healthcare utilization was greater among individuals aged 65 years and older, whereas incremental OOP costs were higher among middle-aged individuals aged 50–64 years. This finding has been replicated in studies of other diseases. 19 Given their physiology and frequent comorbidities, older individuals often require prolonged hospitalization and thus incur higher healthcare costs. 29 For incremental OOP costs, we can speculate that the impact of CRDs seems to be weakened by other comorbidities in older patients because the risk of chronic disease increases with age. Another possibility is the Korean NHI system, a universal and compulsory health insurance scheme that covers 97% of the Korean population. 25 Older adults depend heavily on healthcare services to treat various illnesses and are economically vulnerable because they are no longer economically active. 30 Consequently, under the NHI, the coinsurance model is converted to a co-payment model with lower fees after the age of 65 years, thereby reducing the relevant economic burden for older adults.31,32 For instance, if an outpatient visit costs less than 15,000 KRW (11.8 USD), older patients pay only 1500 KRW (1.2 USD); similarly, if a prescription drug costs less than 12,000 KRW (9.4 USD), older patients pay only 1000 KRW (0.8 USD). 33 The incremental approach was used to estimate incremental OOP costs for older persons with CRDs, which might explain the smaller estimates for younger persons with CRDs.
The subgroup analysis revealed that low-income groups were more likely to utilize healthcare services and total OOP costs than the high-income groups. Studies have reported a strong relationship between socioeconomic status and healthcare access among older adults with lower incomes who had lifelong respiratory diseases.30,31 Comorbidities in patients with CRDs indicated a greater cost. Although the total OOP costs are significant, individuals with CRDs are unlikely to have comorbidities. It reflects a spectrum of comorbidities and illness severity, with OOP costs ranging from mild to severe.9,14,21,22 Our findings suggest that improving health outcomes in older persons may be attainable if financial barriers to healthcare access are addressed, such as through the inclusion of health insurance coverage or additional benefits.
Although this study provided important information on the incremental annual healthcare utilization and OOP of CRDs in Korea, some limitations must be considered when interpreting the results. First, the survey data were entirely patient-reported and, thus, might be subject to recall bias. Second, this study analyzed cross-sectional data and, thus, could not draw definitive causal inferences between CRDs, healthcare utilization, and OOP costs. Third, the KHPS, a secondary data source, defined CRD only as asthma, COPD, emphysema, bronchiectasis, and rhinitis. Consequently, this study did not include some of the most significant respiratory problems, such as interstitial lung disease, pulmonary hypertension, and sleep and ventilatory disorders. As we focused on the entire population of CRD patients, this may have impacted the population size and limitations in determining OOP costs. Therefore, considering the heterogeneity of CRDs would allow us to explore increased healthcare utilization and OOP costs for individuals in future research. Regarding the implications of this study, we focused on the healthcare use and OOP expenditure of patients with CRDs in the entire population and identified several variations in the care that is currently being provided. We believe that our findings and population-based measurements may be useful for other countries or regions interested in identifying disparities in CRD care based on their organizational structure and financial circumstances.
To the best of our knowledge, this is the first study to assess the incremental annual healthcare utilization and OOP costs of CRDs in Korea. The financial burden associated with CRDs is significant, with outpatient visits and medications constituting the largest component of OOP spending. As CRDs are a serious health threat, policymakers should introduce appropriate strategies to reduce their associated burdens. Our study builds on a larger body of empirical research on CRD-related utilization and costs and may lead to additional studies that provide stronger evidence.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Institute of Information & communications Technology Planning & Evaluation (IITP) grant funded by the Ministry of Science and ICT, the Korea government (No.2022000972, Development of flexible mobile healthcare software platform using 5G MEC).