
Abstract
Despite our knowledge of the risk factors for mortality associated with chronic obstructive pulmonary disease (COPD), the mortality rate for this condition continues to increase. This study aimed to investigate the predictive power of physiological variables on all-cause mortality in COPD patients compared to peak oxygen uptake (
Key messages
The use of peak oxygen uptake (
Introduction
Chronic obstructive pulmonary disease (COPD) is a prevalent chronic lung condition. In contrast to the declining mortality rates observed in many other chronic diseases, the mortality rate associated with COPD continues to rise.1,2 Several predictive factors for COPD mortality have been identified, including anthropometric measures, primary and secondary lung pathophysiology, symptoms, and clinically significant outcomes.3–25 These factors include lower body mass index (BMI), 5 emphysema, 15 poor lung function,3,4,10,11,15,20,26 reduced inspiratory and upper and lower limb muscle strength,20,27,28 hypoxemia/hypercapnia, 11 exertional oxyhemoglobin desaturation, 24 elevated dyspnea score, 17 exercise intolerance,4,6,8,15,24,27,28 poor health status, 7 acute exacerbation frequency, 22 and comorbidities. 16 Importantly, these factors can contribute individually or in combination.5,6,9,12–15,18,19,21–23,28,29
Among these factors, BMI, forced expiratory volume in one second (FEV1) % predicted (FEV1%) and exercise intolerance, as measured by the six-minute walking distance (6MWD) and peak oxygen uptake (
Furthermore, studies by Neder et al. and Ewert et al. have indicated that certain cardiopulmonary physiological variables are even more relevant to COPD survival.8,26 Therefore, in this study, we focus on other exercise-related cardiopulmonary physiological variables, such as ventilation efficiency (e.g., ventilation-to-oxygen uptake ratio at nadir or anaerobic threshold, denoted as
Through the use of high-quality physiological variables determined via stepwise Cox regression analysis, we aimed to provide valuable insights for making informed decisions related to patient care. 40
Methods
Study design
A retrospective observational study was conducted on patients with COPD from 1995 to 2021, with each subject being followed up for 10 years, unless censored. All data were obtained from the hospital's electronic medical records. This study was approved by the Institutional Review Board of Chung Shan Medical University Hospital (CS2-21018) and complied with the Declaration of Helsinki. The requirement for informed consent was waived by the IRB.
Subjects
We included patients with COPD between the ages of 40-80 years who underwent their first cardiopulmonary exercise testing (CPET) between Jan 1, 1995, and July 31, 2021, and followed each subject for up to 10 years unless they were censored. For those lost to follow-up before 10 years, we checked the National Death Index for their death date for up to 10 years. The National Death Index in Taiwan provides individual mortality data, including the date and cause of death, upon formal application, with local IRB approval. COPD was diagnosed according to the Global Initiative for Chronic Lung Disease (GOLD) criteria as FEV1/FVC <0.7 with a nonsignificant bronchodilator effect. 1 Eligible patients also had complete data on age, BMI, oxygen-cost diagram score, smoking status, lung function, and symptom-limited cardiopulmonary exercise tests. Patients with lung diseases other than COPD or COPD mixed ventilatory defects (i.e., total lung capacity (TLC) <80% predicted) and those with contraindications for CPET were excluded. To minimize confounding factors for exercise tolerance, patients were also excluded if they had significant comorbidities, including electrolyte imbalance, uncontrolled hypertension, congestive heart failure, renal failure, chronic liver disease, diabetes mellitus, autoimmune disease, and cancer, or had participated in any physical training program during the study period. Patients with mild anemia (i.e., hemoglobin level >10 g/dL) were included to avoid rejecting too many participants from the study.
Measurements
An Oxygen-cost diagram (OCD) was used to scale daily functional activities and was assessed by the patients themselves. The OCD is a 100-mm long vertical line with everyday activities listed alongside the line. 41 The distance from the zero point was measured and scored in centimeters.
Complete pulmonary function tests (PFTs), including spirometry, lung volume, and diffusing capacity of the lung for carbon monoxide (DLCO), were performed by trained technicians at the pulmonary function laboratory. All lung function data were expressed as % predicted, as reported in our previous studies, to maintain consistency.42,43 At our institute, the currently employed predicted values are as follows: FEV1 and FVC were adjusted for race using 90% of the prediction equations developed by Knudson et al. 44 Predicted TLC and DLCO values were derived from the prediction equations by Goldman and Becklake 45 and Burrows et al., 46 respectively, at 85%. Thus, we did not use Global Lung Function Initiative reference values. 47
For cardiopulmonary exercise testing (CPET), the exercise protocol included a 3-min rest period, a 3-min period of unloaded cycling using a computer-controlled electronically braked cycle ergometer, and a ramp-pattern load exercise to the limit of the patient's tolerance. The work rate was selected at a slope of 5–20 watts per minute according to a predetermined fitness level based on our derived protocol formula.
48
Heart rate, oxyhemoglobin saturation, oxygen uptake (
Outcomes
The primary outcome was all-cause mortality.
Statistical analyses
The raw data supporting the conclusions of this study have been uploaded to the supplementary file. For baseline characteristics, continuous variables were summarized as mean ± standard deviation or median (IQR), as appropriate, and categorical variables were presented as percentages. The quantitative variables were categorized as follows: BMI (kg/m2) <18.5, 18.5-23.9, and ≥24. As the main objective of this study was to identify the physiological variables associated with all-cause mortality rather than to test the hypothesis of detecting an expected effect size in a clinical trial, our sample size consideration focused on ensuring stable and efficient regression coefficients. Thus, at least six to ten subjects per variable may achieve this goal.53–55 However, we also conducted retrospective power estimations separately for Cox proportional hazards regression, based on the variables
Univariate and subsequently multivariate analyses were conducted using stepwise Cox proportional hazard regression to assess both the unadjusted and adjusted hazard ratios (cHR and aHR) for mortality, along with 95% confidence intervals (95% CIs). The variables considered in this study encompassed a range of factors, such as age, smoking history, BMI, self-reported maximum daily physical activity, as well as cardiopulmonary functions. These cardiopulmonary functions were assessed through both lung function tests and cardiopulmonary exercise tests. We generated receiver operating characteristic (ROC) curves and calculated the area under the ROC (AUC) to compare the variables of interest, which were selected by stepwise Cox regression analysis, with
Results
A total of 244 male subjects were screened, of whom 62 were excluded for the following reasons: not meeting the inclusion criteria (n = 26, Figure 1), exclusion criteria (n = 26), and declined to participate (n = 10). The remaining 182 subjects were analyzed after completing the PFT and CPET and were followed up for a median of 6.8 years (IQR:3.9-9.2) (Table 1). A total of 120 subjects (65.9%) were aged over 65 years, and 138 subjects (75.8%) exhibited normal body habitus or were mildly overweight (i.e., BMI 24-27 kg/m2). The average cigarette consumption was 46.5 pack-years (33.0–60.0), and the average OCD was 7.0 ± 1.2, indicating brisk walking on level ground or engaging in heavy shopping. The average TLC%, IC%, and FVC% were within normal ranges, while the average FEV1/FVC ratio was decreased. Out of 179 subjects, 156 (87.2%) were classified as GOLD grades 2 and 3, with grades 1 and 4 being uncommon. The average RV/TLC was elevated, and there was mild impairment in DLCO%. They had impaired exercise and cardiopulmonary performance, that is, reduced Workpeak%, Flow chart of study inclusion. A total of 244 subjects with chronic obstructive pulmonary disease (COPD) were assessed for eligibility. For details regarding the inclusion and exclusion criteria of the participants, please refer to the text. Among them, 62 subjects were excluded for various reasons. The remaining 182 subjects completed the pulmonary function test (PFT) and cardiopulmonary exercise test (CPET). The PFT consisted of spirometry, lung volume measurement, and diffusing capacity of the lungs for carbon monoxide. Demographic characteristics, lung function, and exercise data in 182 subjects with chronic obstructive pulmonary disease. amedian (IQR). Abbreviations: TLC, total lung capacity; FRC, functional residual capacity; RV, residual volume; DLCO, diffusing capacity of lung for carbon monoxide; FVC, forced vital capacity; FEV1, forced expired volume in one second; GOLD; the global initiatives for obstructive lung disease; IC, inspiratory capacity; Causes of death in 62 of 182 (34.1%) patients with chronic obstructive pulmonary disease (COPD) during the 6.8-year follow-up. Abbreviations: AECOPD, acute exacerbation of COPD. Survival = 119 (65.4%); missing = 1 (0.5%); * causes of death were not specified or mentioned in medical records.


Stepwise Cox proportional hazard model analysis for risk of all-cause mortality.
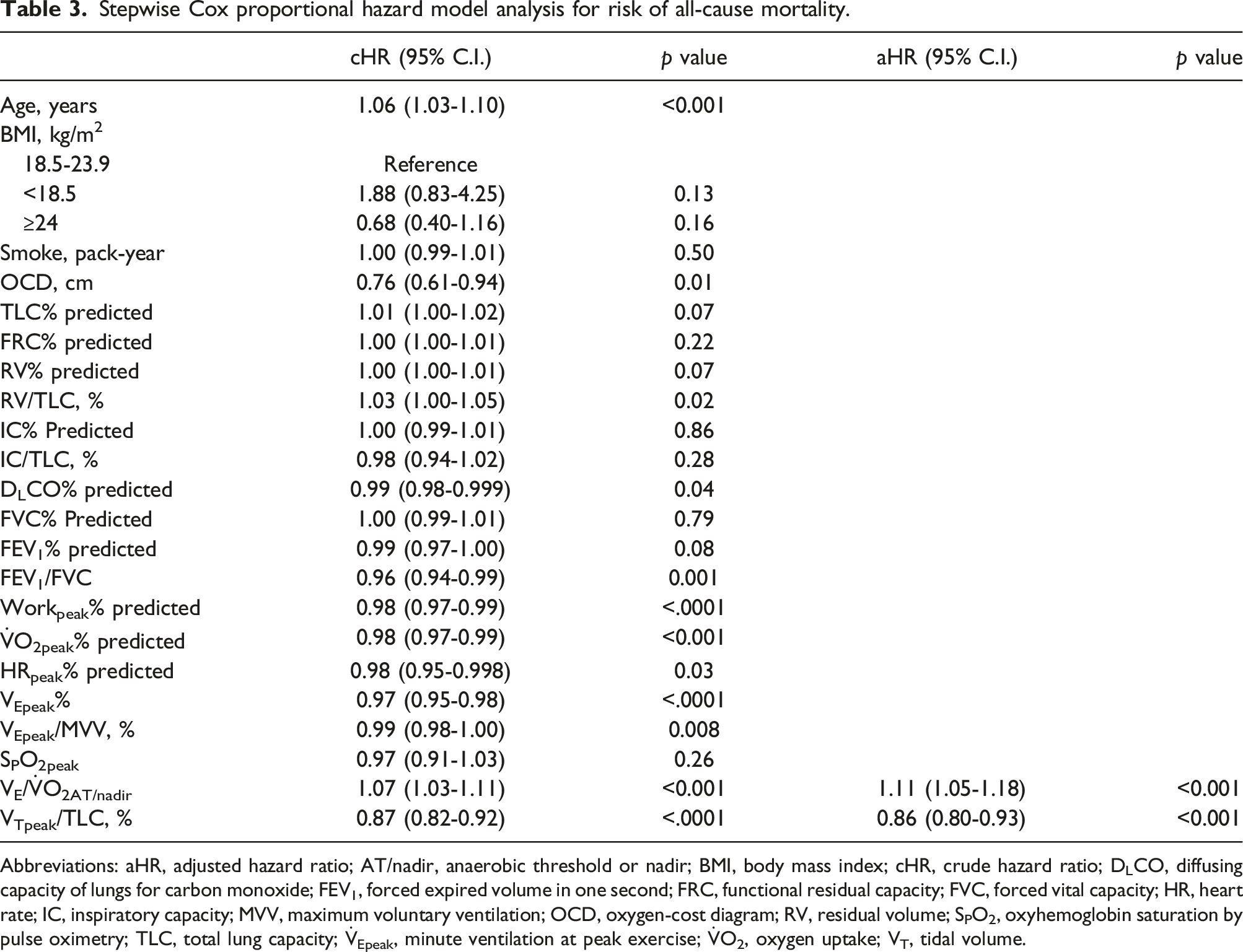
Abbreviations: aHR, adjusted hazard ratio; AT/nadir, anaerobic threshold or nadir; BMI, body mass index; cHR, crude hazard ratio; DLCO, diffusing capacity of lungs for carbon monoxide; FEV1, forced expired volume in one second; FRC, functional residual capacity; FVC, forced vital capacity; HR, heart rate; IC, inspiratory capacity; MVV, maximum voluntary ventilation; OCD, oxygen-cost diagram; RV, residual volume; SPO2, oxyhemoglobin saturation by pulse oximetry; TLC, total lung capacity;

The area under the receiving operating characteristic (ROC) curve for survival analysis indicated that the ratios of tidal volume at peak exercise to total lung capacity (VTpeak/TLC) and minute ventilation to
The mortality prediction model was formulated as follows:
Comparisons of the area under the receiver operating characteristics curves (AUC) for VTpeak/TLC% and

Abbreviations: AT, anaerobic threshold; FEV1, forced expired volume in one second; TLC, total lung capacity;
Discussion
The results of this study indicated that cardiopulmonary exercise testing (CPET) was a valuable tool for predicting mortality in male patients with COPD in Taiwan over a 6.8-year period. Tidal lung expandability, quantified by VTpeak/TLC, was identified as a significant predictor of survival. In contrast, ventilatory inefficiency, measured by
Most of the participants in this study had a normal body habitus and were heavy smokers, yet they maintained the ability to engage in brisk walking and heavy shopping in their daily lives. Most were diagnosed with COPD at GOLD stages 2 and 3, and they demonstrated normal FVC and TLC but exhibited signs of air trapping. In addition, they exhibited mild impairments in diffusing capacity of the lungs for carbon monoxide (DLCO) and cardiorespiratory exercise performance. Notably, while most of the COPD participants had minimal or no comorbidities at the beginning of the study, approximately 1/4 and 1/6 of the causes of death during the 6.8 years of follow-up were attributed to malignant neoplasms and cardiovascular diseases, respectively.
E/
O2AT/nadir and VTpeak/TLC versus
O2peak% and FE V1%
The parameters
Furthermore, it is noteworthy that the addition of VTpeak/TLC to
Another study by Casanova et al. reported that resting IC/TLC was related to COPD survival.
4
In addition, the oxygen uptake efficiency slope (OUES), derived from the formula
In this study, IC/TLC was measured at 0.30 ± 0.08 and VTpeak/TLC at 0.22 ± 0.06 (Table 1), and a strong correlation was established between these two parameters (r2 = 0.25, p < .0001). VTpeak/TLC is a recently developed marker for inverse dynamic lung hyperinflation in patients with COPD,38,39 and it is a primary lung function marker that is hierarchically related to exertional dyspnea and exercise intolerance.
32
Notably, impaired VTpeak/TLC alone was a stronger predictor of all-cause mortality in our patients with COPD than
Although
Although previous studies have shown a negative correlation between COPD mortality and parameters such as FEV1%, IC%, IC/TLC and DLCO%,3,4,10,11,15,20,26 we did not find that FEV1%, IC% and IC/TLC were predictive of mortality. Instead, we identified FEV1/FVC and RV/TLC as significant predictors. It is worth noting that FEV1/FVC, RV/TLC, IC/TLC, and FRC/TLC are closely inter-related. 42 The discrepancies between the previous studies and the present study may stem from the fact that we only included a limited range of COPD severity.
BMI and SpO2%peak
A low BMI (≤21 kg/m2) has been associated with an increased risk of mortality in patients with COPD, while a high BMI (>21 kg/m2) has been associated with improved survival. 5 In addition, computed tomography measurements of the mid-thigh muscle cross-sectional area and FEV1% have been associated with survival, indicating the importance of fat-free muscle mass.50,51 However, in the current study, BMI was not found to be a significant contributor to mortality, possibly due to the small number of cases with BMI <18.5 kg/m2 or the use of BMI categories.
Exertional oxyhemoglobin desaturation is also a known predictive factor for COPD mortality24,25; however, we did not find that SPO2peak was a significant predictor. This discrepancy may be due to mild oxyhemoglobin desaturation that occurred at peak exercise in the present study.
Causes of death
At the beginning of the study, the participants had no comorbidities or minimal comorbidities. However, during the 6.8-year follow-up period, lower respiratory tract diseases including infections, malignant neoplasms, and cardiovascular diseases including cerebral vascular disease were the top three causes of death. This finding is in line with previous studies in which AECOPD,22,50 cancers, and cardiovascular disease 61 were identified as the primary causes of death in patients with COPD, accounting for approximately 2/3 of cases. These findings are important, and clinicians should be aware that patients with COPD may develop cancer and cardiovascular diseases over time, even if they do not initially present with these conditions. The mortality rate in this study was 34.1% over a 6.8-year follow-up period. This may be interpreted as a mortality rate of approximately 5% per year, which is consistent with previous reports from Europe and Canada, and suggests that mortality does not notably vary by geographical location.8,26
One of the strengths of this study is the large sample size and the long follow-up period. In addition, a comprehensive set of CPET and lung function variables was analyzed using Cox regression and stepwise selection, providing a more robust analysis compared to previous studies. For example, one previous study initially only used a limited set of CPET variables, such as
The current study has several limitations. First, female subjects were not enrolled, and data on emphysema score,
15
acute exacerbation,
62
dyspnea score,
17
inspiratory, upper and lower limb muscle strength20,25,26 and health status
7
were not obtained before entry. Therefore, the study results cannot exclude the potential contribution of these variables to COPD mortality. However, the study focused on the contributions of physiological factors to clinically important outcomes according to the American Thoracic Society/European Respiratory Society Statement: Research Questions in COPD.
40
Second, the respiratory causes of death were not provided in the current study, although the risk factors were similar to those reported in previous studies of all-cause mortality.
26
Third, since this was a retrospective study, we were unable to identify the specific causes of death in 16 patients, or the confirmed causes of death in another five patients. Finally, as mentioned above, we did not use
Conclusion
The study showed that VTpeak/TLC and
Footnotes
Author contributions
MLC initiated and designed the study, analyzed and interpreted the data, wrote the manuscript, and approved the version to be published. YHW analyzed and interpreted the data, wrote the manuscript, and approved the version to be published.
Authors’ note
Registered at this site: Chung Shan Medical University Hospital, Taichung, Taiwan.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The funding sources did not influence the study design, data collection, data analysis, data interpretation, or report writing. The MLC had complete access to all study data and took full responsibility for submission for publication.
Ethical statement
Review board
The Institutional Review Board of Chung Shan Medical University Hospital.