
Abstract
Background
Chronic obstructive pulmonary disease (COPD) is an inflammatory and irreversible lung disease. For next of kin caregiver burden can be a consequence of the situation of being close to a person affected by a chronic disease and in need of help. When there is an imbalance between stressors and resources to cope with the situation, caregiver burden emerges. Knowledge is sparse about how the caregiver burden is experienced by the next of kin. Therefore, the aim of this study is to identify and describe the caregiver burden experienced by next of kin of persons with severe COPD.
Method
Qualitative interviews with 21 next of kin were conducted. Thematic analysis was used in accordance with the six steps of Braun and Clarke.
Results
The next of kin experience caregiver burden as 1) changed roles in daily life 2) putting life on hold 3) to stand aside. The next of kin are in need of support to manage daily life.
Conclusions
The caregiver burden affect the next of kin physically and emotionally. To prevent advance consequences, person-centered care can be used to support the next of kin in the situation.
Introduction
Chronic Obstructive Pulmonary Disease (COPD) is an inflammatory and irreversible lung disease, involving airway obstruction and reduced lung function. 1 COPD is the third leading cause of death worldwide. 2 The disease has a substantial impact on daily life, with breathlessness, cough and increased mucus production. The affected person will not obtain normal lung function again, despite medical treatment, which affects the lives of both the affected person and the next of kin. 1
A next of kin is a spouse, partner, child, parent, or parent-in-law but can also be a person with whom one considers oneself to have a close relationship. 3
Caregiver burden is a consequence of the life situation of being close to a person affected by a chronic disease. It increases internal stressors and consumes energy. When there is an imbalance between the stressors and possibilities to cope with the situation, caregiver burden emerges. 4 Negative coping styles lead to a higher caregiver burden 5 Caregiver burden includes aspects of emotional, social, physical, spiritual, and financial functions. 6 Thus, the caregiver burden is multidimensional 7 and the experiences are individual. 8 An increased caregiver burden has an immediate negative effect on the quality of life. 5 Next of kin of those with advanced COPD has a higher subjective caregiver burden than those of persons with COPD in earlier stages. 9 The next of kin needs strategies to support the affected person which develops over time. There is also a need for strategies to handle the emotional burden for the next of kin. 10 The next of kin need their own time, help in the home and a break from the caregiving overnight 11 There is a need to find a balance between being partners, relatives, and informal caregivers and at the same time, they also must take care of their own lives and health. 12
The caregiver burden5,11 together with the disease progression, the irreversibility and symptom deterioration over time is special for COPD. 13 This and the situation for next of kin of needing to meet the affected person’s requirements demands well-balanced support, 14 using a holistic approach. 10 The health care personnel need to understand the next of kin´s need for support. 15 Education may have good effects on the burden 16 and emphasizes the need for knowledge to design and develop interventions for support in health care. To understand and gain more knowledge about the next of kin’s perspective we need to let them express themselves. Therefore, the aim of this study is to identify and describe the caregiver burden experienced by the next of kin of persons with severe COPD.
Method
Sample and participants
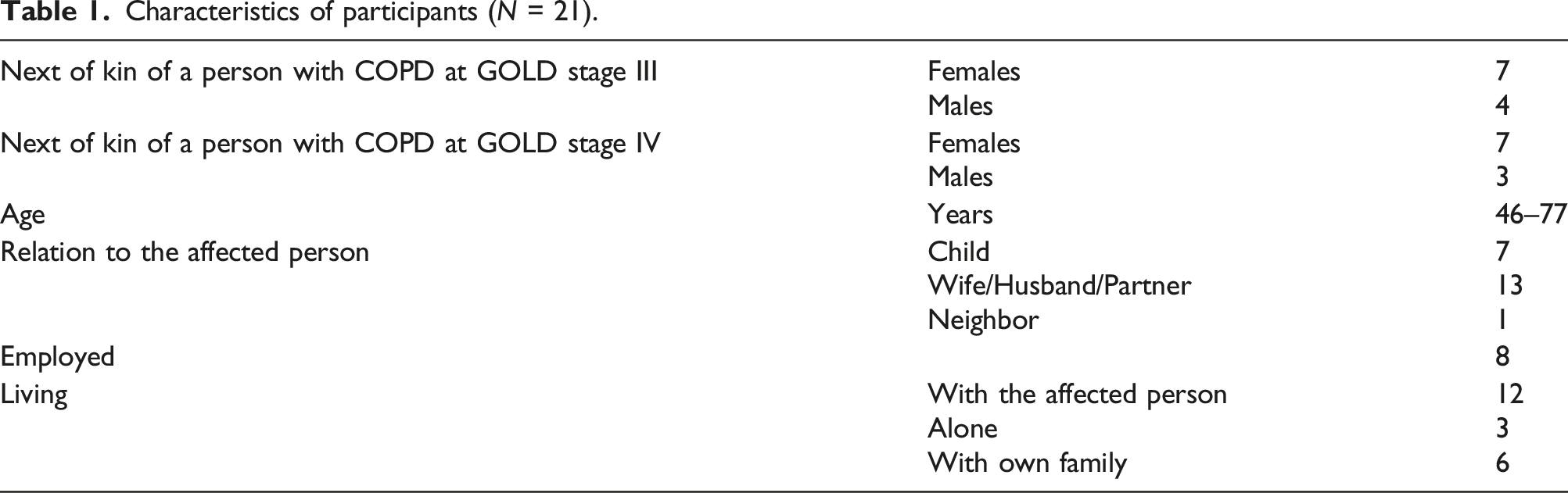
Participants were next of kin of persons with COPD at GOLD stages III and IV, who were recruited at the lung speciality receptions of seven hospitals in the south of Sweden with a purposive and strategic sample. 17 The participants would be the next of kin of a person living with COPD, in stage III or IV, they would be women or men and they would have a variation in the time they lived with the disease. The affected persons were informed about the study by a physician or a nurse at the reception. The only inclusion criterion was being chosen as a next of kin by a person affected with COPD. The next of kin were informed by the affected person and consented to participation by sending the signed informed consent form back in a pre-paid envelope to the first author. The participants were contacted by telephone, informed verbally about the study, and their participation was confirmed. There was no relationship between participants and researchers before or after the interview. The study was conducted with the permission of the ethical committee, record no: 2016/394-31. All participation was voluntary and the data were handled with confidentiality.
Procedure
Twenty-one individual interviews were performed between July 2015 and July 2019. The interviews were conducted at a place and time chosen by the next of kin, mainly in the next of kin’s home with no other person present. 20 interviews were conducted face-to-face and one by telephone. All interviews were performed by the first author who is a registered nurse with working experience with persons affected by COPD and their next of kin.
Characteristics of participants (N = 21).
An interview guide was used during the interviews. This was constructed in a larger project and tested on 25 persons affected by COPD regarding symptom burden and then in this study, it was adapted to caregiver burden instead. The interview started with an open question: “Please tell me about your daily life of being a next of kin of a person affected by COPD?” This initial question was intended to cover the area of caregiver burden without directing the interviewees in a specific way. Supplementary questions and probes were used such as “Please tell me more” and repetition of what was said. The interviews lasted between seven and 71 min and had a median time of 33 min. The interviews were digitally recorded, and then transcribed verbatim.
Data analysis
The transcripts of the interviews were analyzed using thematic analysis in accordance with the six steps of Braun and Clarke.18,19 1. The researchers (all authors) familiarized themselves with the data by reading the transcribed material several times. 2. Initial codes were systematically generated from each interview. Here, the researchers searched for any imbalance between stressors and resources affecting the situation to be next of kin.
18
Figure 1 Examples of data extract and code.
3. Analysis of the initial codes and aggregation of potential themes. Caregiver burden in the sense of, resources and stressors that described the same thing were brought together and a thematic map was generated. 4. Reviewing and refining the themes to find those which were unrelated. These steps were followed for each interview and a thematic map generated Figure 2, all data were amalgamated, and steps one to four were repeated.
18
Example of a thematic map from the interviews.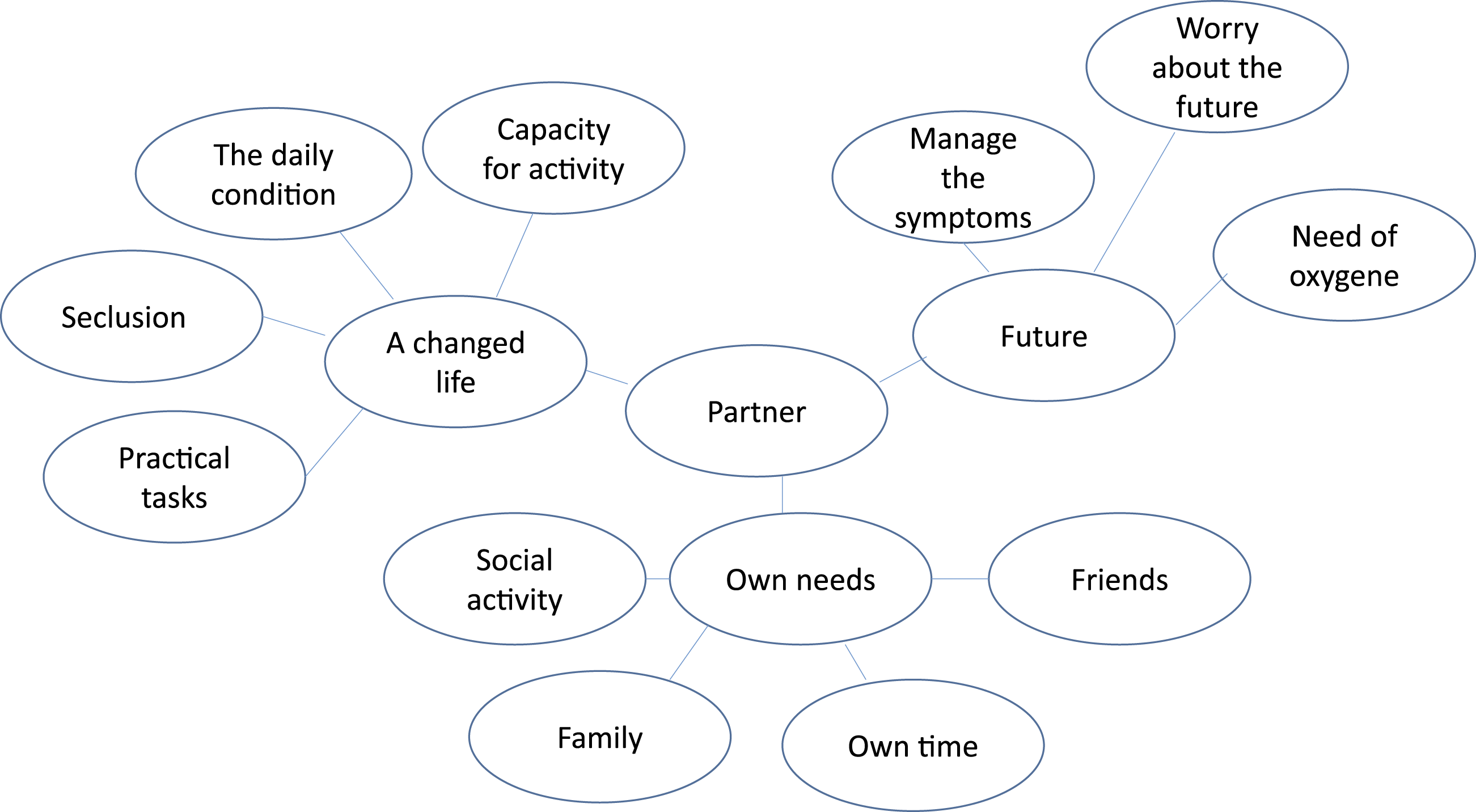
5. Every theme was defined and labelled, and a thematic map with five themes was generated. These themes were reviewed and refined, and finally, three themes were left.
18
Figure 3 Visualize the themes, how they relate and influence each other.
6. Processing and reporting the findings. 18 When there is more than one researcher involved in the analytic process it is collaborative and reflexive to develop a richer and more nuanced reading of the data more than seeking a consensus of meaning. 19 The research group were all registered nurses with different specializations and competencies and were experienced in qualitative methods.
Results
Example of quotations from the three themes.

Changed roles
To be a next of kin of a person affected by COPD suggests changing roles in everyday life due to the affected person´s daily condition. The daily condition depends on the symptom burden of the affected person, which leads to the affected person being unable to live as before. Practically it suggests that the next of kin often needs to take over practical chores concerned with daily living, personal needs, and other duties. … all chores are on me … well all chores are on me… (partner 74 years)
In daily life, personal needs can include assisting with clothing and personal hygiene. These changes affect the whole life situation of the next of kin who need to assist all the time and support the affected person. There is also a need for assistance with cooking and a responsibility to serve energy-rich food. The roles change gradually between the affected person and the next of kin. There are role changes in what previously, conservatively speaking, were men’s or women’s areas concerned with the household and gardening. These practical chores may prompt the need for adapted accommodation to facilitate everyday life. … we should not have this three-floor house and the garden we cannot manage. It would be easier with an apartment… (partner 66 years)
The change in roles may depend on the kind of relationship that exists before the onset of COPD. Those who previously did most things together are not as influenced as those who have lived more separate lives. For the next of kin who live apart, it can be hard to find and take on the needed role. Next of kin who have family, and their own children struggle to be a parent, partner and next of kin simultaneously. It is hard for them to find a balance between the different roles. … my sister has children and family and jobs and such, but we try to be there as much as we can (visiting the parent) (daughter 52 years)
Next of kin also gradually take on the role of surveillance of the affected person’s breathing, daily symptoms and need for support and assistance with medication. The role changes from being a partner, child, or neighbor to an informal caregiver. To take this role or to be forced into a changed role as a caregiver with extended responsibilities leads to specific needs.
Putting life on hold
Putting life on hold suggests that the next of kin put their own life on standby. They may have to refrain from their activities, social interaction with friends, hobbies, work, or their own family activities. These activities are difficult to prioritize, limit life and sometimes lead to a more isolated life at home for those who live together.
The next of kin who live with the affected person refrain from social activities since they are needed at home to help and support the affected person. It is seen as an obligation to be there for better or worse. At the same time, they express a wish to get away from home, which leads to feelings of guilt. … when I go away … I usually make a few visits to a friend … and then I feel a little …yes, what should I say…… I get bad conscience… (partner 69 years)
Next of kin who had also taken a caring role expressed feelings of isolation, as they could not live as before. They are expected to be present and assist 24 h a day. This results in a feeling of insufficient time for their rest. Even if the affected person is in hospital, there is a feeling of being responsible for that person. The next of kin wishes to be informed about the status of the affected person before they can take a decision about the need for care planning and help in the home. The hospitalization is at the same time regarded as a respite from the usual situation at home. There is a need to be involved in the planning process and health care. they can call the day after to say that there should be a care planning conference, and it is also stressful as a relative, but oh my God, he has just entered the hospital (partner 66 years)
For next of kin who live apart from the affected person, taking care of their own home and family is put on hold. They do not prioritize their own activities. That time is taken up with visits and help for the affected person. All this can be a puzzle and can result in one´s own life being put aside. … but it affects your whole life, … affects everything, ... it is always at the back of one´s mind ... (daughter 46 years)
The activities the next of kin used to engage in with the affected person are no longer possible to the same extent as before the disease. To be unable to do things that were possible earlier in life, or to do things together as a couple or as a child and parent is burdensome. … not being able to take her out and have a coffee in the city or go and look at flowers or some of those little mothers and daughter things… (daughter 57 years)
The next of kin put their own life on hold to have time to help and support the affected person with personal needs, taking care of the home and participating in visits to health care. All these are obvious tasks. They described doing all this as a kind of payback for everything they had received. … it is a contrast with the life you have ... because it is my turn to help them, they have always helped me … (daughter 54 years)
Standing aside
Stand aside and see the affected person experiencing the symptom burden and the limitation in daily life affects the next of kin emotionally. Emotions and thoughts about the future and feelings of helplessness are stressful and frustrating for them. It can be frustrating to stand aside without being able to help or relieve breathing problems. … you would like to help him in some way ... there is not much you can do ... I usually breathe (with him) … (son 48 years)
Sometimes the breathing problem was horrifying, and the cough and increased mucus production were disgusting. Some next of kin felt guilt and shame about having these feelings. Standing aside, wanting to help but not having the opportunity led to ambivalent feelings.
At the same time, not being able to help and having a fear about what will happen next to the affected person can increase the caregiver burden. To manage the situation, the next of kin needs more knowledge about the disease, the prognosis and what will happen when the condition deteriorates and this knowledge should be appropriate to their situation. They expressed a feeling of worry about the future when deterioration would occur, and about future needs regarding more practical help, medication, and the need for oxygen therapy. ... and then it is hard because you know, …I think I know that the prognosis is not so good ... ... that 1 day she may need oxygen ... (daughter 47 years)
Discussion
The current findings demonstrate that the next of kin are forced into role changes by taking over practical chores in daily life as well as a caring role for the affected person, thus they experience a changed life situation. These role changes sometimes force the next of kin to be informal caregivers and is something different to being a partner, child, or friend. To be a next of kin who provides care without formal competence and payment is to be an informal caregiver. 20 This role can be unclear, making it difficult to know what to expect. 21 To be forced into this role can be stressful and may affect the whole life situation. All are next of kin but the line between being next of kin and an informal caregiver can be challenging to recognize, understand and decide about.
Some next of kin do not prioritize their activities but instead focus on being there and helping the affected person, which can lead to social isolation and can affect their own health negatively and be a stressor. This confirms that the next of kin feel inadequate in performing the changed role with everything it entails while simultaneously trying to maintain their own life. 4 Next of kin who have their own family and children can be influenced in several ways, which in turn can cause feelings of guilt. These findings concerning physical and mental health as well as emotional aspects are similar those presented in earlier studies.22,23 Support from health care and society is needed for next of kin as it may help them to handle the situation better and reduce caregiver burden, which Lee et al. 24 confirm. Standing aside and watching the affected person struggle to get daily life to work. The symptoms affect the ability of the person with COPD’s to take part in ordinary activities, and the deterioration over time has an impact on the next of kin. Standing there without being able to do something is burdensome. There is a fear that the person affected by COPD may die and leave them alone. When this fear arises, the experience of helplessness and a feeling of lack of knowledge is overwhelming. Few previous studies have described this helplessness and frustration; they are more concerned with a lack of knowledge.25,26 Next of kin of persons in palliative care felt a sense of security because of the knowledge they had gained from the palliative team. 27 This was a feeling the next of kin of the person affected by COPD in this study did not express. This shows the need for more knowledge about the illness and the future need for oxygen therapy and more support to handle different situations. Being aware of these needs can be a resource for involvement. When the next of kin understands they can be more active in the situation, but action both from the affected person and the health care are needed to facilitate the understanding. It signals a need for more interventions for the next of kin from health care. Person-centered care with the involvement of the next of kin can lead to a feeling of security and can further develop the role of informal caregivers.
Today, support is often from a COPD team focusing on the affected person and on giving information about the diagnosis and self-care from the perspective of the affected person. This study shows a need to develop support also for the next of kin, to see their needs and to give them a feeling of security in the situation. This can be in the form of knowledge about the diagnosis, disease progression and how to handle the symptoms and provide support in self-care.
Person-centered health care with the involvement of the next of kin can be a successful intervention. Providing person-centered care involves the next of kin, letting them become secure. and knowledgeable partners can be successful for both the affected persons and the next of kin. This can reduce the caregiver burden and its multidimensional impact. This is in accordance with Cruz et al., 28 who showed the importance of involving the whole family in the care to promote health for both parties.
Strengths and limitations
The strengths of the study are the number of informants and the comprehensive and very informational and rich interviews. The seven-minute interview was performed by telephone; it was short but informative and concise. Another strength is that it includes a great variety of relationships with persons with COPD in both GOLD stages III and IV, including partners, children, and neighbors of different ages (Table 1). Next of kin were recruited from a large geographical area from seven hospitals of varying sizes where affected persons received health care. The data collection took a long time, which may have been because of the strenuous situation for the next of kin. It is known that they are hard to involve in research and are very time-consuming to recruit. 29 The time required for data collection can lead to a risk that the situation may change over time, but the results are similar across all interviews, so this is not thought to have influenced the results. The next of kin who participated were grateful to share their experiences, and that someone was interested and listened to them. Few studies of caregiver burden examine groups with the same disease, 30 this study can help to fill that gap in understanding caregiver burden in the next of kin of persons with COPD. Most of the studies today are quantitative and there is a need for both qualitative and mixed methods studies. 30 The interviews were conducted by one of the persons in the research team, who is a registered nurse with working experience with persons affected by COPD and their next of kin. This practical experience and those encounters with the next of kin formed the research question about how COPD affect the next of kin. So, the interviews were open-minded, and there were no preconceived notions. The interview and the transcription process are the start of the analysis, and the interviews were reflected upon in the research group. As we were several researchers involved, the analytic process was collaborative and reflexive. This approach gives a more nuanced reading and analysis, using reflexivity instead of seeking consensus on meaning, 19 A limitation could be that the study was conducted in Sweden and was thereby situated in a certain policy context, but caregiver burden seems to be a universal phenomenon.
Conclusion
Being a next of kin of a person with severe COPD is life-altering and complex, with many effects on daily life, including both physical and emotional aspects. In the planning and development of COPD health care, it is vital to make sure that the next of kin is recognized as a part of the affected person’s whole life situation. When working with person-centered care the next of kin should be involved.
Footnotes
Acknowledgements
Grateful thanks go to the next of kin who shared their experiences, the affected persons and the colleagues for their assistance with the recruitment process.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Region Östergötland and Forskningsrådet i Sydöstra Sverige