
Abstract
Introduction
Chronic obstructive pulmonary disease (COPD) is characterized by airflow obstruction. 1 In 2019, COPD had an estimated global prevalence of 391 million 2 and was the third leading cause of death worldwide. 3 The clinical features of airflow limitation, lung hyperinflation, respiratory muscle weakness, and dyspnea, contribute to the exercise intolerance often present in COPD. 4 Exercise capacity as measured by the 6-min walk test (6MWT)5,6 and the level of physical activity 7 are predictors of mortality in COPD patients.
Along with the respiratory manifestations described, COPD is a systemic disease that is often accompanied by extrapulmonary sequela including cognitive dysfunction. 8 The reported prevalence of cognitive impairment in COPD patients is variable ranging between 10 to 61%, 9 and as high as 77% in hypoxemic populations. 10 Moreover, impairment ranges from mild to severe cognitive impairment and dementia, as well as deficits in both global and specific cognitive domains.11–13 Regarding specific cognitive domains, two systematic reviews both corroborate the frequent prevalence of memory and attention-related deficits in COPD.13,14
Related to diminished cognitive performance is dual tasking, an experimental paradigm used to evaluate decrements in cognition when an individual is required to perform a cognitive and motor task simultaneously. Dual task interference arises when there is reduced performance in either task relative to their single task equivalent. 15 There are several cognitive theories postulated to explain the reduced performance observed relative to single tasks. 16 One of the theories, the central capacity sharing model, posits that internal processing of the concurrent events is capacity-limited due to the requirements of parallel processing.17,18 Importantly, processing speed is correlated with broad cognitive measures, such as fluid intelligence. 19 Thus, a systematic review evaluating older adults with mild cognitive impairment (MCI) observed greater dual task interference during walking relative to healthy controls. 20 Furthermore, individuals with MCI display worse postural, gait, and fine motor control relative to their non-MCI counterparts. 21
Given the heightened prevalence of cognitive decline in COPD, and the apparent relationship of MCI and worsened dual task performance and motor control in non-COPD, it is pertinent to evaluate how cognitive capacity influences motor control in COPD patients. Additionally, as COPD patients almost invariantly exhibit dyspnea, 22 it is critical to include dyspnea within our conceptual definition of physical performance. Indeed, dyspnea is not only a physical symptom but also an interoceptive stimuli that requires cortical and subcortical processing.23,24 In COPD, hypoxemia may lead to cognitive dysfunction through neuronal injury. 25 The aim of this scoping review was to investigate the relationship between cognitive function and motor control in COPD patients, and whether treatments improve cognitive and physical function. As cortical control is necessary for purposeful movement, 26 we hypothesize that COPD patients that exhibit cognitive impairments will have more impaired motor control compared to those without cognitive impairments.
Methods
Protocol
The draft protocol and finalized review utilize the established scoping review framework set by Arksey and O’Malley and their updated enhancements.27–29 The draft protocol was registered prospectively with Open Science Framework on 6 September 2021 (https://osf.io/ng765/). Draft revisions were conducted after consultation and feedback from the review team.
Identifying the research question
The primary objective addressed by this scoping review was to examine how cognitive capacity influences physical performance in COPD patients. The following sub-questions were addressed: 1) what is the relationship between cognitive test measures and physical performance; 2) did physical performance indicators differ when COPD patients were stratified by cognitive test scores; 3) does dual tasking influence physical performance in COPD relative to healthy adults; and 4) does baseline cognition influence cognitive and physical changes with interventions?
Information sources and search strategy
The search strategy was developed by a research librarian (AO-C) with the following key concepts: COPD, cognition, and exercise capacity. The search was executed on 20 July 2021, and a second search on 14 February 2022, in the databases: Ovid MEDLINE; Ovid Embase; Cochrane Database of Systematic Reviews; Cochrane Central Register of Controlled Trials (CENTRAL); APA PsycINFO; CINAHL complete (EBSCOhost). Conference and book materials were removed from Embase. The reference lists of retrieved publications were also examined. The searches were not limited to study design and year but were limited to humans, adults, and English language. Please see the Supplementary Appendix for the comprehensive search strategy.
Eligibility criteria
The following studies were included if they examined COPD patients of any severity: 1) by evaluating the relationship between their cognition and physical performance; 2) compared their physical performance according to stratification of their cognitive test scores; 3) examined dual task paradigms; 4) assessed cognition and physical outcomes after an intervention; and 5) evaluated the relationship between baseline cognition with physical changes with an intervention. Exclusion criteria used: 1) regression models that had cognition as an outcome variable; 2) COPD lung transplant recipients; 3) intervention studies that did not include both cognitive and physical post-treatment scores unless inclusion criterion above was met; and 4) non-English language studies. Case series, grey literature, conference proceedings and abstracts, and dissertations were excluded.
Study selection
Search results were imported into EndNote 20 and duplicates were removed using EndNote’s automation tool. Pairs of reviewers (PR, SA, EF, UM, RLFF, MK) independently screened the titles and abstracts and subsequently the selected full-text articles for inclusion. Disagreement among reviewers were resolved by a third reviewer.
Data charting process
Pairs of reviewers (PR, SA, EF, UM, RLFF, MK) independently abstracted data from the full-text articles and disagreements were resolved by a third reviewer. Data abstraction included: study design, study location, inclusion and exclusion criteria, baseline characteristics (age, sex, number of participants, COPD severity, comorbidities), study protocol, and outcome measures (correlation coefficients, hypothesis testing outcomes, beta-coefficients, dual task results, and treatment outcomes).
Quality assessment
Quality assessment was performed using a 15-item modified Downs and Black checklist 30 or the full Downs and Black 31 checklist (27-items) 31 depending on study design, the latter was used for randomized trials, randomized controlled trials (RCTs), or non-randomized controlled trials. This checklist queries study quality, external and internal validity, and power. Quality assessment was conducted by pairs of independent reviewers (PR, SA, EF, UM, MK) and disagreements were resolved by a third reviewer.
Data synthesis
Baseline characteristics and assessments.

ACE-R: Addenbrooke’s Cognitive Examination-Revised; AECOPD: Acute Exacerbation of COPD; AT: Aerobic Training; CDT: Clock Drawing Test; CI: cognitively impaired; CF: cognitive functioning; CN: cognitively normal; CT: Combined training (Aerobic + Resistance); CTHI: continuous training at high intensity; CTVT: continuous training at the ventilatory threshold; DSST: Digit Symbol Substitution Test; EAA: Essential Amino Acid supplementation; ESM: education and stress management; EXESM: exercise and ESM; HIIT: high-intensity interval training; LVRS: Lung Volume Reduction Surgery; Mainten: Maintenance; MMSE: Mini-Mental State Examination; MoCA: Montreal Cognitive Assessment; mo: month; PR: Pulmonary Rehabilitation; RAVLT: Rey Auditory Verbal Learning Test; SCWT: Stroop Color and Word Test; S-MMSE: Standardized MMSE; T-ICS: Interview for Cognitive Status; SMBM + T/O + Ex: self-management behaviour modification + tiotropium/olodaterol + exercise training; TMT: Trail Making Test; TUG: Timed Up and Go; WAIS: Wechsler Adult Intelligence Scale; WAIS-R: WAIS-Revised; WM: working memory; WMS-R: Wechsler Memory Scale-Revised.
aValues for total combined group (CI and CN COPD).
Cross-sectional studies showing relationships between cognitive test scores and physical performance.

6MWD: 6-min walk distance; AIR: average impairment rating; AP: anteroposterior; BBS: berg balance scale; CGNR: clinician’s global neuropsychologic Rating; CoP: center of pressure; DLCO: diffusing capacity for carbon monoxide; DWR: delayed word recall; IWR: immediate word recall; mMRC: modified medical research council dyspnea scale; NS: non-significant; NTB: neuropsychological testing battery; UCSD-SOBQ: The University of California, San Diego shortness of breath questionnaire; VAS: visual analogue scale.
Dual task studies—performance of COPD patients relative to healthy controls (Con).
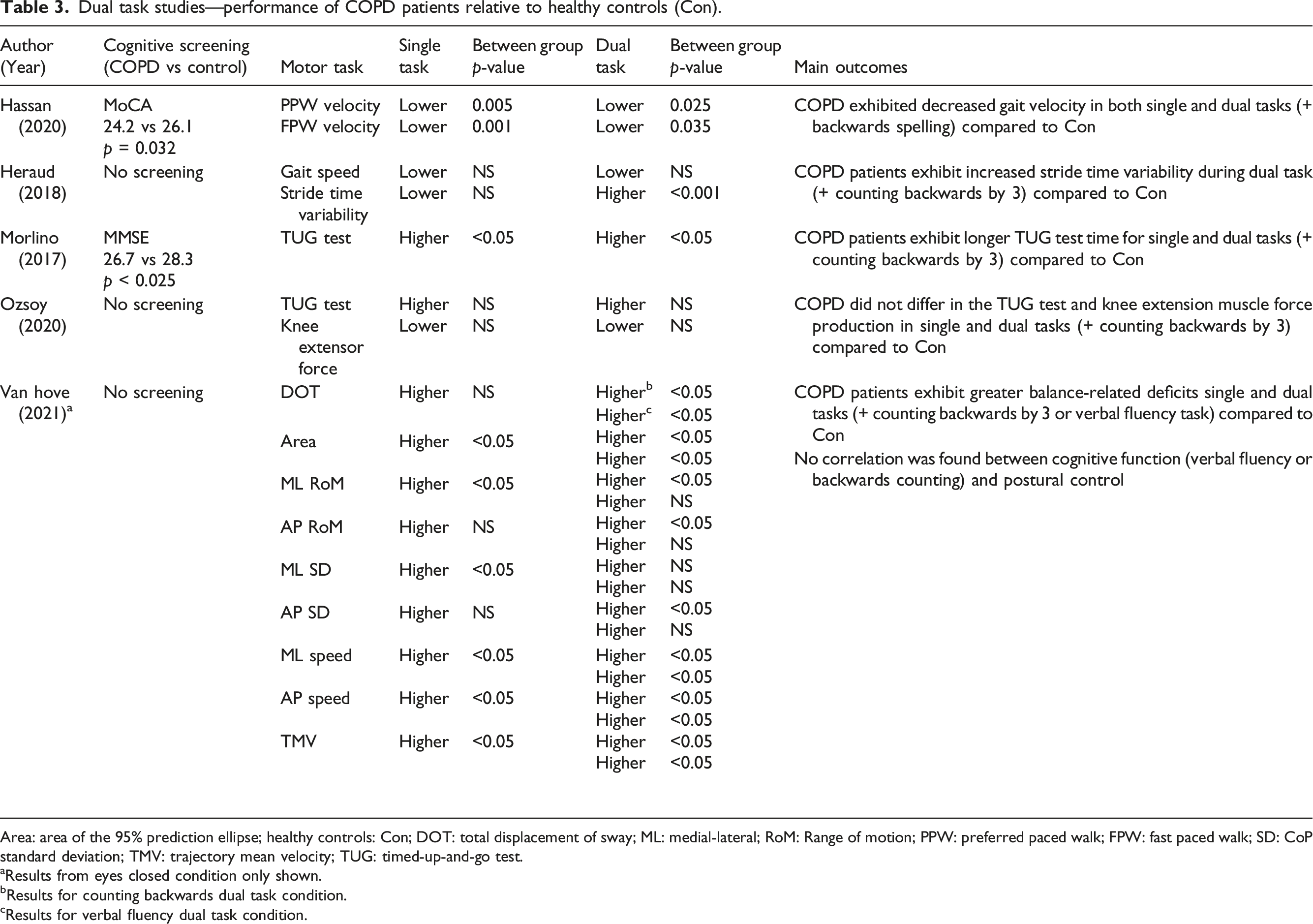
Area: area of the 95% prediction ellipse; healthy controls: Con; DOT: total displacement of sway; ML: medial-lateral; RoM: Range of motion; PPW: preferred paced walk; FPW: fast paced walk; SD: CoP standard deviation; TMV: trajectory mean velocity; TUG: timed-up-and-go test.
aResults from eyes closed condition only shown.
bResults for counting backwards dual task condition.
cResults for verbal fluency dual task condition.
Interventions showing within subject changes in cognition and physical performance.

6MST: 6-min stepper test; BNT-SF: Boston Naming Test-Short Form; CET: cycle-endurance test; CFIT: Culture Fair Intelligence Test; DR: delayed recall; ESWT: endurance shuttle walk test; IR: immediate recall; MT: medical therapy; PEmax: maximal expiratory pressure; PImax: maximal inspiratory pressure; RTI: Reaction Time Task; SPPB: Short Physical Performance Battery; SNIP: sniff nasal inspiratory pressure; WL: waiting list. Some of the abbreviations are shown for Table 1.
aData from the same study.
bEffect sizes reported instead of p-values.
cNon-significant pre-to-post measures for all study groups.
Results
The PRISMA diagram (Figure 1) summarizes the screening results.
32
The initial and second searches yielded 10,045 and 1207 articles, respectively. The number of duplicates removed was 3619. Screening resulted in 133 full-text articles to be screened for eligibility and 44 articles met the inclusion criteria.10,33–75 Studies were excluded due to lack of a relationship between cognition and physical outcomes (n = 84); regression models utilizing cognition as an outcome rather than an explanatory variable (n = 2); drug intervention studies that evaluated pre- and post-cognitive outcomes to assess safety (n = 2); and a study that evaluated cognitive but not physical outcomes after rehabilitation. Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram summarizing search strategy results.
Of the 31 studies evaluated using the modified Downs and Black checklist (see Supplementary Appendix), quality assessment scores ranged from 43.8% to 87.5%, with a mean of 65.5%. All 31 studies scored points for: stating the study hypothesis or study aim(s); clearly delineating study outcomes; clearly describing the main findings; using appropriate statistical tests; and using valid and reliable study measures. Studies demonstrated poor external validity and internal validity (confounding) with a combined mean percentage of 14.6% and 32.3%, respectively. The 31 studies had a mean score of 74.2% for internal validity (bias), with no studies receiving points for blinding outcome measures.
Of the 13 studies evaluated using the full Downs and Black checklist, quality assessment scores ranged from 46.4% to 89.3%, with a mean of 60.7%. These studies scored high for internal validity (bias) with a mean of 83.5%. The studies demonstrated poor external validity with a mean of 12.8%. Only two of the 13 studies demonstrated sufficient statistical power.
Baseline characteristics of study participants and cognitive assessment used are summarized in Table 1. Regarding the type of cognitive assessment used in the cross-sectional and longitudinal (non-intervention) studies, three studies used a comprehensive neuropsychological testing battery, seven studies used the Mini-Mental State Examination (MMSE), four studies used the Montreal Cognitive Assessment (MoCA) test, and nine studies used a combination of the Stroop Test, Trail Making Test (TMT), Digit Symbol Substitution Test (DSST), clock-drawing test (CDT), a verbal fluency test, and word recall. For the dual task studies, one applied backwards spelling, four used backwards subtraction by threes, and one of these four also applied a verbal fluency task. Among the intervention studies, 10 utilized neuropsychological testing batteries, nine utilized either the MoCA or MMSE, one used the Culture Fair Intelligence Test, and one used the AD8 dementia screening tool.
The relationship between cognitive test scores and physical performance are summarized in Table 2.
Cognition and exercise capacity
Inconsistent findings were reported for the relationship between 6MWD and stratification of subgroups using cognitive screening tools (MoCA or MMSE) or a comprehensive neuropsychological testing battery. Observational studies did not identify a difference in 6MWD in cognitively impaired (CI) and cognitively normal (CN) subgroups.38,42,75 Two cross-sectional studies62,74 identified a difference in 6MWD between CI and CN subgroups when stratified by the MMSE, with the CI group having a lower mean 6MWD. However, this relationship was negated in one report after adjusting for age and education. 62 Of note, cross-sectional studies identified significant weak-to-moderate correlations between cognitive screening tools and 6MWD,42,66,74 while another study did not find an association between the MoCA and 6MWD. 71 When using a comprehensive neuropsychological testing battery, cross-sectional studies did not identify a difference in 6MWD between CI and CN individuals.36,40
Other cognitive tests used to evaluate relationships with 6MWD also showed mixed results. A longitudinal study organized patients into low or high baseline TMT part B (higher scores indicate greater impairment for TMT A and B) scores (measure of executive function) and reported varying improvements in their cognitive test scores over 3 years, with those improving having higher baseline 6MWD. 64 A cross-sectional study found differences in 6MWD when stratifying COPD patients by TMT part A scores (measure of psychomotor speed) but not according to TMT part B scores; COPD patients with impaired TMT part A had lower 6MWD than patients categorized with a normal TMT part A score. 69 Moreover, TMT part A but not TMT part B was found to have a weak inverse correlation with 6MWD. 65 Another cross-sectional study found a weak correlation between TMT and 6MWD. 66 Two cross-sectional studies found the DSST, a measure of psychomotor speed, to be weakly associated 53 and weakly correlated with 6MWD. 66 The CDT, a measure of memory, attention, and visuospatial abilities had a weak correlation with 6MWD. 74
Regarding gait speed, in a cross-sectional study using multivariate linear regression, all covariates, which included delayed word recall, immediate word recall, measurement of orientation or executive function, were not significant. 50
Regarding cycle ergometry, Average Impairment Rating, a global index of impairment (higher score indicates greater CI), and an independent global rating by clinicians, demonstrated a weak negative correlation with maximum work. 10 TMT part A was also reported to have a weak negative correlation with maximum work, while the relationship with TMT part B was not significant. 65
The Stroop-Color Word Test (SCWT), a measure of executive function and cognitive flexibility, and TMT part B, were both found to have a moderate inverse correlation with leg extension force. 41
Cognition and dyspnea
Categorizing COPD patients into CI and CN subgroups according to cognitive test scores had mixed results regarding Modified Medical Research Council (mMRC) Dyspnea scores. Higher mMRC Dyspnea scores were found in CI COPD when stratifying by MMSE 67 and TMT part B, 69 while MoCA,35,75 a comprehensive neuropsychological testing battery, 40 and TMT part A69 stratification showed no significant differences.
Regarding other measures of dyspnea, categorizing subgroups based on a comprehensive neuropsychological battery, one cross-sectional study did not identify a difference in their Visual Analogue Scale (VAS) dyspnea scores. 36 Categorizing patients into high or low TMT part B baseline scores with varying trajectories of cognitive improvement, did not find a significant difference between their University of California, San Diego Shortness of Breath Questionnaire (UCSD-SOBQ) scores 64 ; with TMT part B being weakly correlated with the UCSD-SOBQ, while TMT part A was not. 65
Cognition and balance
An investigation of postural and functional balance through center-of-pressure displacement and Berg Balance Scale (BBS), respectively, found moderate correlations with Stroop interference. 63 Multiple linear regression modelling showed associations with Stroop interference score and center-of-pressure, adjusted for other covariates (see Table 2). 63 In a younger COPD cohort (mean of 57 years), the MMSE was weakly correlated with BBS, and MMSE was associated with BBS through simple linear regression. 54 Moreover, another cross-sectional study using multivariate linear regression, found an association between delayed word recall and tandem stance time. 50
Cognition and hand function
In COPD patients categorized by TMT part A and TMT part B scores, grip strength was significantly higher in CN individuals. 69 Additionally, through multivariable regression, borderline impaired TMT part A scores and borderline impaired and impaired TMT part B scores were independently associated with decreased grip strength (Table 2). 69 Along with handgrip strength, cognition measured through MMSE had a moderate negative correlation with placement and turning dexterity in a hypoxemic cohort, with the dexterity correlation not being different in those with mild and moderate hypoxemia. 70
Dual tasking in COPD patients compared to healthy controls
In one study, COPD patients exhibited decreased walking velocity during both single and dual task (walking and backwards spelling) conditions compared to healthy controls, 51 while another study did not report differences in gait speed in both task conditions, but did find greater stride time variability for COPD patients during dual tasking (walking and backwards counting by 3). 52 Mixed results were also found for the Timed Up and Go (TUG) test, whereby one study reported COPD patients having a longer TUG completion time in both single and dual tasks relative to healthy controls, 60 while the other did not report a difference in single and dual task conditions for the TUG test and knee extension muscle force. 61 Both studies utilized backwards counting as their cognitive task paradigm.60,61 Regarding balance assessed through CoP displacement during dual tasking, COPD patients exhibited greater balance deficits in both single and dual tasks relative to healthy controls. 73
Effects of interventions on cognitive outcomes in COPD patients
Pulmonary rehabilitation (PR) resulted in variable improvements among the studies assessing specific cognitive domains.35,44–46,57 PR showed improvements in global cognition,35,38,49,55,59 attention and processing speed,44,45,57 executive function,35,44–46 visuospatial skills,35,57 and language ability. 57 Among the five PR studies showing improvements in global cognition,35,38,49,55,59 two studies demonstrated improvements only in CI COPD patients.38,49 All PR interventions resulted in significant improvements in physical outcomes,35,38,39,44–46,48,49,55,57,59 with three studies35,38,39 reporting no difference in 6MWD post-rehabilitation between CI and CN COPD patients, while investigation 38 reported CN COPD patients having significantly greater post-rehabilitation 6-min stepper test (6MST) scores than CI COPD patients. Studies evaluating whether cognition is associated with PR physical improvements showed mixed results.38,48 Improvements in MoCA scores were not associated with changes in exercise capacity as measured by 6MWD and 6MST in hospital-based PR, 38 while baseline MMSE scores were significantly correlated with improvements in maximum cycling effort (watts) (r = 0.46, p < 0.05) and VO2max (r = 0.41, p < 0.05) in home-based PR. 48
Exercise interventions had variable cognitive outcomes.37,47,68 Endurance training was shown to improve fluid intelligence,37,47 global cognition, 68 visuospatial abilities,37,68 working memory, 68 attention, 37 delayed recall, 37 and executive function. 37 Combined aerobic and resistance training resulted in greater improvements in delayed recall, fluid intelligence, and visuospatial abilities compared to aerobic training alone. 37
Working memory (WM) training versus sham WM training was also studied. 72 WM refers to the short-term memory that is required to do things in the moment. Although WM span increased over 24 weeks in the intervention group, this was not reflected in improvements in cognitive test scores. 72 Moreover, physical capacity as measured by 6MWT and Short Physical Performance Battery (SPPB) showed no improvements. 72
Other interventions such as behavioral modification, 58 lung volume reduction surgery, 56 oxygen (O2) therapy, 33 amino acid 43 and piracetam supplementation 34 resulted in cognitive improvements. Moreover, all these therapies also improved physical outcomes except O2 supplementation.33,34,43,56,58
Discussion
COPD, 6MWD, and balance
Our findings indicate that CI and CN COPD patients have comparable 6MWT scores,36,38,42,75 with studies finding no association between cognitive impairment and 6MWD.40,62 These findings are corroborated by the low-order correlation between global42,74 and domain-specific65,74 cognitive test scores and 6MWD. Similarly, dyspnea scores were comparable between CI and CN COPD patients,35,36,40,64,74,75 with low, 65 moderate, 54 and non-significant correlations found. 74 Importantly, lower cognitive test scores were associated with impairments in balance parameters.50,54,63
Of clinical importance, a recent meta-analysis found that COPD patients had greater deficits in their balance compared to healthy controls. 76 Nonetheless, while shorter 6MWDs are correlated with impairments in balance function,77–79 and a 6MWD <300 m being a predictor for balance impairments as measured by the BBS and TUG, 80 the reviewed studies indicate no difference in 6MWDs between CI and CN COPD patients. Given the importance of balance in daily activities, further exploration of interventions to improve the relationship between CI and falls are required.
Potential mechanisms underlying cognitive-physical relationship
As depicted from the results, COPD patients who display decreased cognitive capacity are more likely to exhibit impairments in balance and hand function, rather than functional exercise capacity or physical conditioning as measured by the 6MWT. Our results do not reflect a lack of relationship with 6MWD, but that the relationship with cognition and 6MWD is less pronounced. One plausible mechanism is the increased cortical sensorimotor connectivity demonstrated while standing versus walking. 81 This heightened cortical connectivity suggests greater attention is needed for balance and postural control, while walking may depend more on spinal neural networks. 81 COPD patients exhibit reduced white matter integrity and impairments in gray matter functional connectivity 82 ; thus, CI COPD patients may lack the cortical resources to sustain adequate balance.
A regression model investigating cognitive-balance relationships demonstrated an association between better delayed word recall and increased tandem stance time. 50 The 10-word list used for delayed recall is often utilized to detect mild CI by assessing hippocampal and entorhinal cortical functions. 83 Poor delayed recall is associated with hippocampal84,85 and entorhinal atrophy.86,87 Importantly, hippocampal atrophy and its association with CI has been reported in COPD. 88 The hippocampus and entorhinal cortex receive input from the vestibular system. 89 Notably, hippocampal and entorhinal atrophy is associated with impaired vestibular function, a system important for maintaining balance. 90
Additionally, another regression model depicted poorer TMT scores (worse executive function) associated with weaker handgrip strength. 69 The prefrontal cortex (PFC) facilitates executive function, 91 and PFC impairments can lead to worse motor planning and recruitment, and thereby reduced strength.92,93
Dual tasking
Similarly, cognitive-motor dual tasking induced static balance deficits in COPD patients. 73 Balance 76 and postural control94,95 are often impaired in COPD. While several factors have been implicated in balance impairments, such as age,96,97 dyspnea, 98 inspiratory muscle weakness, 99 and lower limb muscle strength, 98 the influence of cognition has not been investigated as thoroughly. Although, a cognitive screening test was not conducted in the dual task study by Van Hove et al., 73 COPD patients had lower verbal fluency task scores than healthy controls.
Impairments when performing a concurrent task may arise due to processing constraints within the brain, such as the PFC. In a single-cell recording study in monkeys, dual tasking resulted in concurrent activation of the same lateral PFC region suggesting cognitive capacity limitations. 100 Related to limitations in capacity, Hassan et al. 51 observed that COPD patients did not increase dorsolateral PFC oxygenated hemoglobin (O2Hb) from single to dual tasks, while healthy individuals did increase O2Hb. Therefore, this observed ceiling effect in neural activity may be pivotal to the constraints in simultaneous processing. In addition to limited cognitive capacity, impairment has been reflected by reduced PFC automaticity (decrease in O2Hb seen in tasks requiring less executive function) during single and dual task walking in COPD and older adults, respectively.101,102
Pulmonary Rehabilitation
In this review, the predominant intervention to facilitate cognitive-physical improvements was PR. All PR studies found significant improvements in cognition. However, of the four studies35,38,49,57 assessing differences in PR outcomes between CI and CN COPD patients, three38,49,57 found cognitive improvements only in CI COPD patients. Thus, the efficacy of PR cognitive improvement may also, among other factors, rely on baseline cognition.
Notably, the physical improvements that arise from PR seem to be independent from baseline cognition, as all studies specifically evaluating PR in CI COPD patients note an improvement in physical performance.35,38,39,49 Although, Ferrari et al. 48 did find a moderate correlation between baseline MMSE scores and improvements in exercise capacity in a minimally supervised home PR setting. While compliance was assessed, potential CI may have influenced proper completion of the training sessions in a minimally supervised setting, hence the moderate correlation between MMSE scores and exercise capacity. Furthermore, Cleutjens et al. 39 found that CI COPD patients had an increased rate of PR dropout compared to CN COPD patients.
Nonetheless, despite the potential risk for PR dropouts, physical improvements were observed in CI COPD, with the 6MWT being the most frequent treatment outcome. While this scoping review identified balance as a potential factor that is impaired in CI COPD patients, most PR studies included in our review did not conduct balance assessments. Of interest, a report that examined physical outcomes but not cognition before and after PR in COPD patients, found that the small improvement in BBS were not related to improvements of 6MWD. 103 Thus, including balance outcomes, along with usual exercise capacity measures, may be warranted, especially in CI COPD patients.
Aerobic and resistance training
An interesting finding regarding exercise is the enhanced cognitive benefits found in combining aerobic and resistance training versus aerobic training alone in COPD patients. 37 This approach is corroborated by studies of those with stroke 104 and dementia, 105 as well as a meta-analysis of healthy individuals that showed a larger effect size of combined aerobic-resistance training than aerobic training alone. 106
Working memory training
Cognitive training, specifically WM training, has been recently investigated in COPD patients. While van Beers et al. 72 found an improvement in WM trained task, the improvements did not generalize to overall cognitive improvements as measured by the Cambridge Neuropsychological Test Automated Battery. Additionally, secondary outcomes measuring exercise capacity showed no improvements. A previous study investigating cognitive training in hypoxemic COPD also found no cognitive improvements relative to the control group (no cognitive training). 107 A review investigating cognitive training also affirms that, while cognitive training can improve the specific trained task, there may be a lack of generalizability. 108
Limitations
There are some limitations in this scoping review. To develop a broader descriptive scope of the differences between CI and CN COPD patients, results from independent t-tests, Mann-Whitney U tests, and correlation coefficients were included. While these results help characterize the relationship between cognition and physical performance, they cannot delineate the underlying mechanisms. Secondly, there was a large degree of heterogeneity in study designs and outcomes that prevented a meta-analysis of the interventions. Moreover, the low statistical power in many of these interventions precludes conclusions of actual treatment effects. Regarding dual task studies, the comparator groups were healthy individuals rather than CN COPD patients, thus the impact CI has on dual tasking cannot be stated. Importantly, most of the data was collected from cross-sectional studies, thus determining the causality between cognition and physical performance is not possible.
Conclusions and future directions
Limited cognitive capacity in COPD was more likely to be associated with impairments in balance, hand function, and dual tasking rather than exercise capacity. Due to the inherent limitations in study design and statistical analysis, causal mechanisms cannot be determined. Pulmonary rehabilitation was the most common treatment, which resulted in variable cognitive improvements. Given the increased incidence of falls in COPD, 109 and the possible relationship between cognitive impairment and balance deficits, future interventions may incorporate balance assessment in COPD patients that present with cognitive decline and impairment.
Supplemental Material
Supplemental Material - Impact of cognitive capacity on physical performance in chronic obstructive pulmonary disease patients: A scoping review
Supplemental Material for Impact of cognitive capacity on physical performance in chronic obstructive pulmonary disease patients: A scoping review by Peter Rassam, Eli M. Pazzianotto-Forti, Umi Matsumura, Ani Orchanian-Cheff, Saina Aliabadi, Manjiri Kulkarni, Rachel L. Fat Fur, Antenor Rodrigues, Daniel Langer, Dmitry Rozenberg and W Darlene Reid in Chronic Respiratory Disease
Footnotes
Authors’ contributions
PR, DR and WDR conceived and designed the study. AO-C performed the data base searches. PR, EF, UM, SA, MK, RLFF screened eligibility of titles and abstracts and PR, EF, UM, SA, MK screened for full text exclusion and abstracted data including the quality assessment for the included articles. PR wrote the initial manuscript and WDR contributed to the writing of the manuscript. PR revised the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed funding support from the RAMP Trust fund, Canadian Institutes of Health Research (PCS 183427), Canadian Institute of Health Research Operating Grant (PJM 179846). Dmitry Rozenberg receives research support from the Sandra Faire and Ivan Fecan Professorship in Rehabilitation Medicine.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.