
Abstract
Introduction
Chronic obstructive pulmonary disease (COPD) is currently the third leading cause of death worldwide. 1 As the disease progresses, physical inactivity becomes a major problem leading to muscle weakness and deconditioning. Physical inactivity is thus the strongest predictor of all-cause mortality in COPD. 2
Pulmonary rehabilitation (PR) plays a pivotal role in enhancing self-management and exercise capacity in COPD. The cornerstones of PR are physical exercise, disease-specific education and change of behaviour. 3 However, the length and specific content of training programmes vary greatly between countries and authorities responsible for rehabilitation. 4
Recently, psychological interventions, such as mindfulness meditation, have been suggested to enhance COPD self-management. However, the effect of psychological interventions on physical capacity or symptoms is yet to be established. 5 Few studies have assessed breathing techniques in patients with COPD. In pursed lip breathing (PLB), the person exhales through tightly pressed lips and inhales through the nose with the mouth closed. The purpose is to create back-pressure inside the airways to keep them open during expiration, thus diminishing air-trapping and reducing the work of breathing. One study has shown that this breathing technique may have an effect on exercise capacity, quality of life and dyspnoea in patients with COPD. 6 In diaphragmatic breathing (DB), the person inhales deep and slow through the nose, at the count of 10 s, followed by a deep and slow exhalation. One randomised controlled trial showed an increase in exercise capacity, while positive trends were seen for quality of life and dyspnoea. 7 This may imply that PLB and DB could play a role in COPD rehabilitation programmes.
Shortness of breath in COPD not only causes considerable discomfort but it may also provoke anxiety. Hence, patients with COPD often do not exercise after completion of a PR programme. 8 In free diving, breathing techniques are used for free divers to be able to hold their breath for several minutes while swimming under water. Apart from packing the lungs with air, free divers also use DB ahead of diving experiences and maintain a distinct calmness during diving. These methods have inspired the development of breathing techniques tailored for COPD patients as a measure to reduce anxiety and discomfort. With the use of a conscious and distinct breathing pattern depending on desired gait speed or stair climbing, the goal is to enhance exercise capacity and long-term level of daily physical activity.
In this explorative pilot study, the safety and effectiveness on exercise capacity, symptoms and quality of life were evaluated in nine COPD patients completing a 6-week training programme consisting of free diving-inspired breathing techniques. The training techniques and protocol are newly developed, tailored for COPD patients and constructed for the study. We hypothesised that exercise capacity and quality of life increased comparable to conventional PR, while adherence to the programme was high.
Methods
Study population
This prospective pilot study involved 11 patients with moderate to severe COPD (Global Initiative for Chronic Obstructive Lung Disease 2007 classification) from the out-patient clinic at Department of Respiratory Diseases and Allergy at Aarhus University Hospital, Denmark, by simple and random approach. Inclusion criteria were stable COPD and kept walking capability. Exclusion criteria were severe comorbidity that specifically compromised walking and long-term oxygen supply. Nine patients completed the study, and two patients dropped out due to pneumonia and vertebral compression fracture; both events were unrelated to the study.
Intervention
Briefly, the intervention consisted of a 6-week programme with one weekly group session and home-inspired training the remaining 6 days of the week (Figure 1). The free diving-inspired breathing techniques consisted of 1) inhalation to total lung capacity (TLC), expiration with pursed lip until residual volume (RV) and then performing side bends for 10 s while holding the breath. 2) Expiration with pursed lips to RV, performing a slow inhalation to TLC using the diaphragm and then performing side bends for 10 s while holding the breath. 3) Breathing in a rhythm adapted to the gait pace and physical activity, for example, walking three steps per inhalation/exhalation in flat terrain; if going uphill, walking two steps per inhalation/exhalation. The philosophy of the breathing techniques is for the COPD patients to experience shortness of breath in a safe environment while performing moderate exercise (holding the breath while performing side bends) and anticipate hypoxaemia and exhaustion when walking (breathing rhythm adapted to the gait pace). The rationale is that when patients adapt the breathing rhythm to their activity level (such as slow walking, fast walking or stair climbing) before they experience shortness of breath, they are expected to experience less symptoms and be able to walk longer distances. Participants were instructed to perform the same exercises at home for 30 min per day at moderate intensity. Six weeks training programme. 6MWT: 6-min walk test; CAT: COPD Assessment Test; CSES: COPD self-efficacy scale.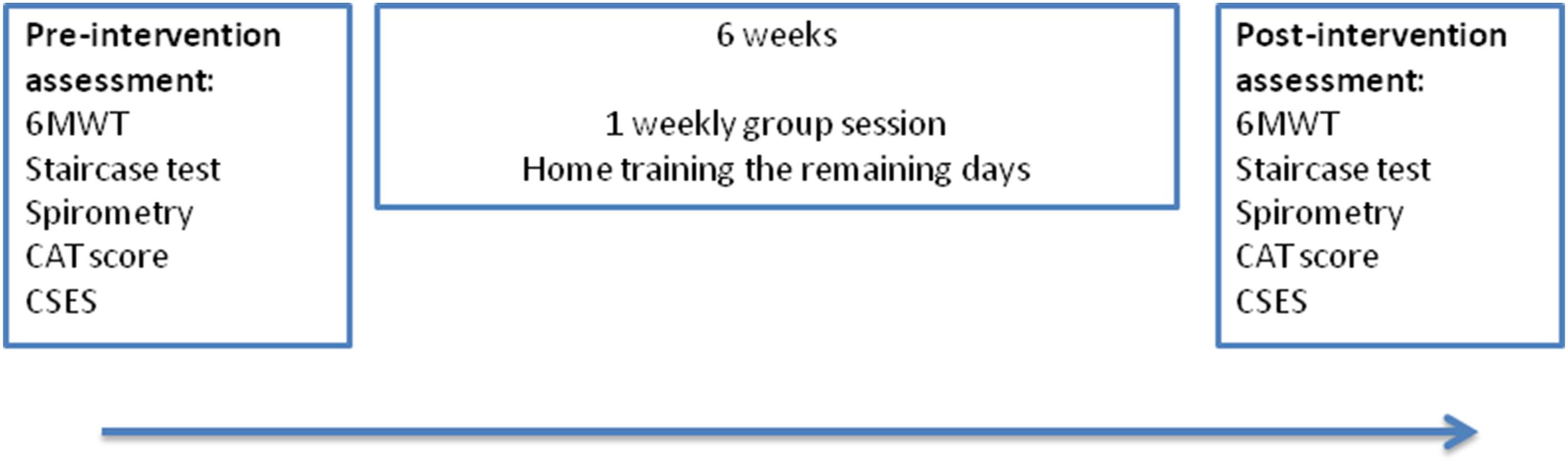
The techniques were developed by a team of free divers, part of the Danish national free diving team and have previously been presented for COPD patients in a non-formal setting with positive feedback from patients. For a detailed description of the philosophy and teaching principles behind the training programme, see Supplemental Appendix A.
Outcomes
The primary outcomes were the distance walked in 6 min (6MWT) and the time to complete a staircase test constructed for the study (Figure 2). The rationale behind the staircase test was to test whether patients were faster in a course where they did a combination of walking and stair climbing, which is a cornerstone of the philosophy. During the exercise tests, participants were evaluated by means of respiratory rate, exercise exertion using the Borg scale, exercise-induced desaturation by pulse oximetry (H100B, EDAN, USA) and end tidal CO2 (ETCO2) (Capnostream 20, Medtronic, USA). Furthermore, spirometric measurements (Pneumotrac, Vitalograph, UK), COPD Assessment Test (CAT)
9
and COPD self-efficacy scale (CSES)
10
were assessed before and after the intervention; reduction in scores is an improvement in outcome. Adherence to the group sessions was recorded as well as any adverse events during the study. Staircase exercise test. Participants walk 25 m, turn 180° around a cone, walk 15 m and then climb 20 steps. Then they turn around, go down the stairs and use the same route back to start, before they turn back and walk the same route, finishing on top of the staircase.
Statistical analysis
A power calculation was not performed as this was a pilot study. Data in tables are presented as mean ± standard deviation. Results were compared using the paired t-test. A p value below 0.05 was considered statistically significant. Statistical analyses were performed using GraphPad Prism (v.4.03 GraphPad Software Inc., CA, US).
Results
Baseline characteristics
Baseline characteristics of study population.
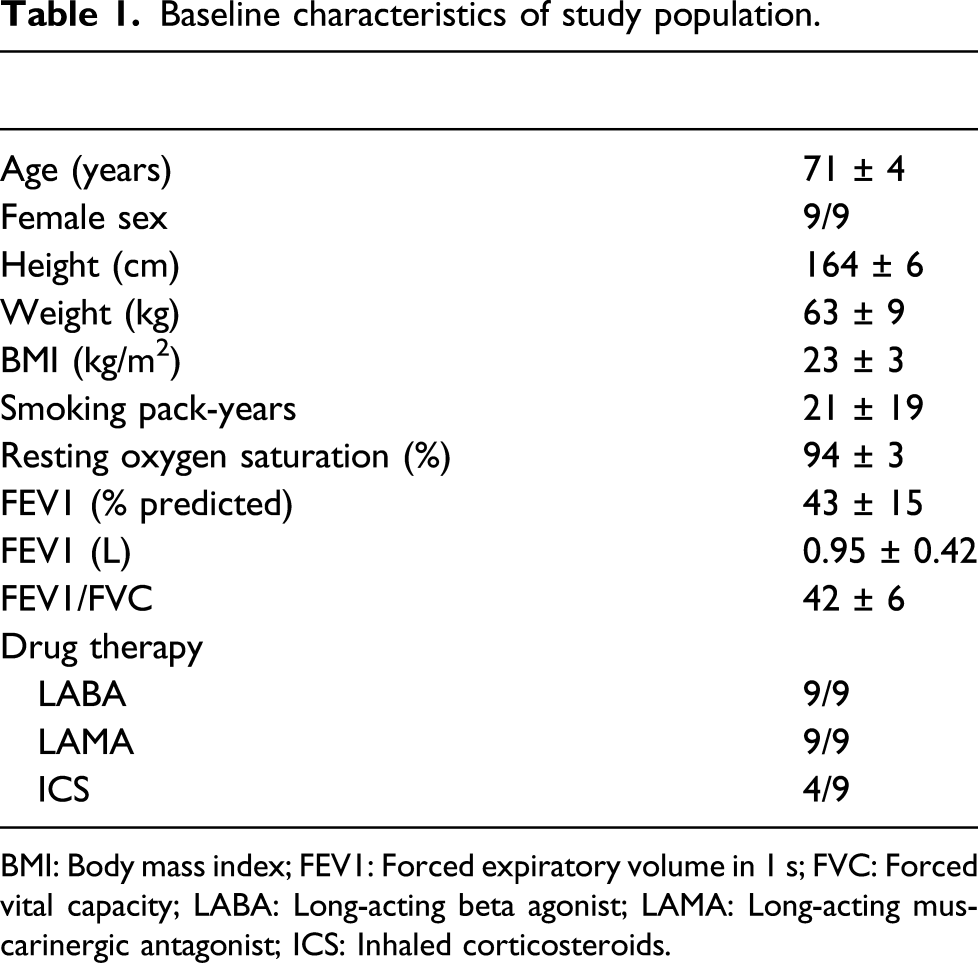
BMI: Body mass index; FEV1: Forced expiratory volume in 1 s; FVC: Forced vital capacity; LABA: Long-acting beta agonist; LAMA: Long-acting muscarinergic antagonist; ICS: Inhaled corticosteroids.
Primary outcomes
Outcome measurements.

6MWT: 6-min walk test. Mean (standard deviation).

Exercise tests, QoL and dyspnoea scores before and after the intervention. 6MWT: 6-min walk test; CAT: COPD Assessment Test; CSES: COPD self-efficacy scale. Boxplot of mean and SE.
Measurements during exercise tests
A significant reduction in respiratory rate from 22 to 19 was seen during the recovery period after the 6MWT (minute 6 to minute 9), while the overall respiratory rate did not differ during exercise (Figure 4). Perceived exertion using the Borg scale, oxygen saturation and ETCO2 measurements remained unchanged. Respiratory rate during and after 6-min walk test.
Quality of life questionnaires
The CSES score diminished 14 points (98 vs 84, p < 0.05) (Figure 3). A reduction in CAT score of 1.6 point was not statistically significant (19.6 vs 18, p = 0.17). Question 9 of the CSES (the perceived exertion during physical exercise) showed a non-significant reduction (3.7 vs 2.9, p = 0.06).
Adherence to group sessions
During the 6-week training programme, adherence to group sessions was very high (96.3%). In total, two patients each missed one group session.
Safety
No adverse events were documented during the training programmes neither during group sessions nor at home.
Discussion
In this explorative pilot study, nine patients with COPD successfully completed a 6-week training programme consisting of free diving-inspired breathing exercises. Adherence to group sessions was very high and no adverse events occurred. After completion of the programme, the 6MWT increased 48.5 m, which exceeds the minimum clinically important difference of 14–35 m. 11 A significant reduction was seen in the CSES, while the CAT score did not decrease significantly.
The proposed mechanisms for the increase in exercise capacity are that the COPD patients have been exposed to shortness of breath in a safe environment and feel more secure increasing their exercise effort at the 6MWT. Furthermore, they are taught to increase respiratory effort prior to physical activity, varying respiratory rate consciously depending on the type of exercise, thereby anticipating exhaustion. ETCO2 measurements during 6MWT were unchanged, implying that the physiological cause is not different in CO2 retention, but could be due to less dynamic hyperinflation during exercise. A reduction in respiratory rate in the recovery period of the 6MWT could also back this physiological explanation, although a reduction of 3/min in respiratory rate may not prove clinically significant.
The increase in the 6MWT of 48.5 m is in accordance with results from conventional COPD PR programmes. In patients with few symptoms and moderately impaired pulmonary function, the increase in the 6MWT was around 25 m,12–14 while in patients with substantial symptoms and severely impaired pulmonary function the increase in the 6MWT was around 44 m. 15 However, patients completing conventional COPD PR programmes have trouble enhancing their daily physical activity,16,17 which is a major objective of the PR programmes. Efforts to solve this problem through the use of tele-rehabilitation have shown conflicting results, with one study showing a low adherence to exercise programmes of just 21%, 18 while another study reported adherence of 92% 19 ; this underlines the importance of an adequate and personalised organisation of exercise programmes.
Adherence is a problem in PR of patients with COPD. Drop-out rates in PR and maintenance exercise programmes range between 35% and 40%.20,21 The main causes are related to lack of motivation and transportation problems. Patients dropping out typically have poorer exercise capacity test results prior to PR, more exacerbations and a higher use of oral corticosteroids and are more frequently smoking. In this study, absence from the weekly group sessions was very low at 3.7%. However, adherence to home training sessions for 30 min per day was not recorded.
The focus of conventional PR programmes is muscle and cardio-respiratory training. However, the symptoms of COPD make engagement in physical activity unpleasant and after completion of the PR programme, it is difficult to keep patients motivated to continue to exercise. The length of the effect on exercise capacity after completion of the PR programme is unknown. Intense efforts are made to improve understanding of how to optimise motivation in COPD patients to keep exercising. 22 Breathing exercises tailored for COPD patients could be a valid alternative to conventional PR, especially in patients poorly motivated for physical exercise programmes or patients with substantial shortness of breath despite completion of PR. These techniques do not require patients to be highly motivated for cardio-respiratory workout and are designed to be incorporated in daily life activities.
This pilot study has some limitations. The study did not include a control group receiving usual care. The sample size was small, thus introducing the risk for type II errors. All participants were female; the motivation to participate in this type of intervention may differ in the male population.
This pilot study tested the feasibility of free diving-inspired breathing techniques for COPD patients and proved well tolerated by participants with high adherence to the weekly group sessions. Furthermore, after learning the techniques, patients were able to walk a longer distance in the 6MWT. We believe the results are promising and encourage a randomised trial in a larger setting, comparing the efficacy of the free diving-inspired breathing exercises to conventional PR or usual care. The primary outcome would be exercise capacity, with secondary outcomes such as quality of life, adherence to programme sessions and electronically measured daily activity before, during and several months after the intervention.
Supplemental Material
sj-pdf-1-crd-10.1177_14799731211038673 – Supplemental Material for Free diving-inspired breathing techniques for COPD patients: A pilot study
Supplemental Material, sj-pdf-1-crd-10.1177_14799731211038673 for Free diving-inspired breathing techniques for COPD patients: A pilot study by Morten Borg, Tue Thastrup, Kurt L Larsen, Kristian Overgaard, Ole Hilberg and Anders Løkke in Chronic Respiratory Disease
Footnotes
Ethics approval and consent to participate
The study was performed in accordance with the Helsinki Declaration. The protocol was approved by the Central Denmark Region Committee on Biomedical Research Ethics. All participants gave informed written consent.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
List of abbreviations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.