
Abstract
The Centers for Medicare and Medicaid Services has identified early rehospitalization of patients with chronic obstructive pulmonary disease (COPD) exacerbations as a performance measure for hospital care. We retrospectively reviewed patients with COPD who were admitted to University Medical Center, Lubbock, Texas, USA, between October 2010 and March 2011. There were 81 COPD patients with 103 hospitalizations. The mean age was 73.9 years. Pulmonary function tests using the Global initiative for chronic Obstructive Lung Disease criteria had been done in 36 patients (44.4%) and revealed 1 mild (2.8%), 7 moderate (19.4%), 20 severe (55.6%), and 8 very severe (22.2%) cases. Only 38.4% of the patients had prior influenza vaccine. Most patients were treated with antibiotics (81.8%) and corticosteroids (87.9%). The mean length of stay was 4.9 days, and 4 patients died. Most of the patients were discharged home (63.6%) with a median follow-up interval of 14 days. Thirty-two percent did not have long-acting bronchodilators and/or inhaled corticosteroids prescribed on discharge. There were 14 early rehospitalizations within 30 days. Logistic regression analysis indicated that a history of coronary artery disease (odds ratio (OR) 6.4, 95% confidence interval (CI) 1.1–37.4) and unilateral pulmonary infiltrates (OR 12.8, 95% CI 1.9–86.4) significantly increased the early rehospitalization rates. Acute exacerbations of COPD in patients with a history of ischemic heart disease or unilateral pulmonary infiltrates are at increased risk for early readmission. These risk factors should be identified during hospitalization; early follow-up or other interventions may reduce readmissions. Influenza vaccine, maintenance bronchodilators and/or inhaled corticosteroids, and pulmonary function tests were underused, and these standards of care should be provided to improve care.
Introduction
Chronic obstructive pulmonary disease (COPD) exacerbations have adverse effects on both health care systems and patients. They are associated with faster declines in lung function, poorer health status, and increased morbidity, mortality, and health care costs. About 50% of exacerbations are due to respiratory infections; the other half are secondary to heart failure, environmental pollution, or unknown etiologies. 1 Although patients may have similar disease severity, environmental exposures, comorbidities, and treatment, they often have different rates of exacerbations and hospitalizations. Consequently, additional factors must affect these rates. Recent studies suggest that continuity with the patient’s primary care physician or pulmonologist after an acute hospitalization, early postdischarge care, telephone support, and pulmonary rehabilitation can reduce COPD early rehospitalization rates. 2,3 Other studies have analyzed the standard of care for COPD patients and found that only half of the eligible patients received influenza vaccine and pneumococcal vaccines and that only 46% of hospitalized COPD patients received long-acting bronchodilators and/or inhaled corticosteroids when discharged. 4 These deficiencies could contribute to more frequent COPD exacerbations and hospitalizations. We have reviewed readmission rates in our patients to identify factors associated with early rehospitalization and to identify strategies to reduce COPD early rehospitalizations.
Methods
We retrospectively reviewed COPD patients admitted to University Medical Center (UMC) in Lubbock, Texas, USA, between 1 October 2010 and 31 March 2011. The medical record numbers were available from UMC case management that collected information on the Centers for Medicare and Medicaid Services (CMS) performance measure for the 30-day readmission rate for patients with COPD. From electronic medical records and case management resources, we collected baseline characteristics (age, sex, past medical history of coronary artery disease and atrial fibrillation, and current smoking history), postdischarge follow-up interval, disposition type, telephone support, forced expiratory volume in 1 s (%FEV1) from pulmonary function tests done within the past 5 years to determine COPD severity, long-acting bronchodilator and/or inhaled corticosteroid administration, congestive heart failure defined by echocardiogram done within the past 5 years, acute infection defined by leukocyte count on admission, antibiotics use, pulmonary rehabilitation, influenza vaccine, length of stay, intubation, β-blocker use, chest X-ray results, serum brain natriuretic peptide (BNP) levels, corticosteroid administration, and highest blood glucose level during hospital stay. We followed this group of patients for early rehospitalization within 30 days after discharge.
The baseline characteristics, COPD early rehospitalization rate and standard of care, using influenza vaccine, and long-acting bronchodilator and/or inhaled corticosteroid administration as the indicators, were analyzed using simple descriptive statistics. Pearson chi-square, Fischer’s exact tests, and independent sample T tests were used to compare the difference between the early rehospitalization group and the nonearly rehospitalization group. We then used logistic regression analysis to analyze which factors affected the early rehospitalization rate. We selected factors from the univariate analysis that had a p value of less than 0.2 to analyze the multivariate logistic regression analysis. All analyses were performed using SPSS Windows version 15.0. The Texas Tech University Health Sciences Center Lubbock/Odessa Institutional Review Board approved the study protocol.
Results
We identified 81 patients admitted to UMC due to COPD exacerbations between 1 October 2010 and 31 March 2011. There were 103 admissions with 14 early rehospitalizations (13.6%) defined as rehospitalizations within 30 days after discharge. The age of the patients ranged from 50 to 98 years, with an average of 73.9 years. Forty-three patients were female (53.1%). Twenty-four patients (29.6%) had a history of coronary artery disease. Thirty-six patients (44.4%) had pulmonary function tests done within the past 5 years. Based on the Global initiative for chronic Obstructive Lung Disease criteria, of the 36 patients, 1 patient (2.8%) had mild, 7 patients (19.4%) had moderate, 20 patients (55.6%) had severe, and 8 patients (22.2%) had very severe COPD. Fifty-five patients (67.9%) had echocardiograms for review. Eight patients (13.8%) had a left ventricular ejection fraction <55%, 50 patients (91.3%) had diastolic dysfunction, 14 patients (29.8%) had normal pulmonary artery pressure (PAP) of less than 30 mm Hg, 12 patients (25.5%) had mild pulmonary artery hypertension (PAH) (PAP 30–40 mm Hg), 13 patients (27.7%) had moderate PAH (PAP 41–50 mm Hg), 8 patients (17%) had severe PAH (PAP more than 50 mm Hg), and 11 patients (20.4%) had cor pulmonale (based on right ventricular enlargement; Table 1).
Baseline characteristics of 81 patients admitted with COPD exacerbations

FEV1: forced expiratory volume in 1 s.
For all admissions, there were five intubations (5.1%; Table 2). Most patients were treated with antibiotics (81.8%) and corticosteroids (87.9%). The average length of stay was 4.9 days (1–16 days). Laboratory data on admission revealed unilateral pulmonary infiltrates in 14.1% of patients, abnormal white blood cell counts (<4.0 × 103/μl or >12.0 × 103/μl) in 25.8%, and a proBNP >900 pg/ml in 23.2%. Four patients (3.9%) died during hospitalization. Most patients (63.6%) were discharged to home; the others went home with home health care (11.1%) or to an inpatient facility (25.3%). Thirty-six patients (32.3%) did not have long-acting bronchodilators and/or inhaled corticosteroids prescribed on discharge. Thirty-eight patients (38.4%) had prior influenza vaccination. Sixty-six (71%) received follow-up calls with a median follow-up interval of 14 days.
Comparison of patients with COPD exacerbations according to early rehospitalization status

BNP: brain natriuretic peptide; COPD: chronic obstructive pulmonary disease; FEV1: forced expiratory volume in 1 s; HHC: home health care; PAH: pulmonary artery hypertension; WBC: white blood cell.
When comparing COPD patients classified according to early rehospitalization or no early rehospitalization, there were no statistically significant differences in age, sex, echocardiographic findings, COPD severity, use of β-blockers, antibiotics, long-acting bronchodilator and/or inhaled corticosteroids, systemic corticosteroids, white blood cells, blood glucose, proBNP, current smoking status, intubation, length of stay, follow-up call, follow-up duration, and discharge type (home, home with home health, or to an inpatient rehab, and skilled nursing or nursing home). The early rehospitalization group had a higher percentage of influenza vaccination (Table 2).
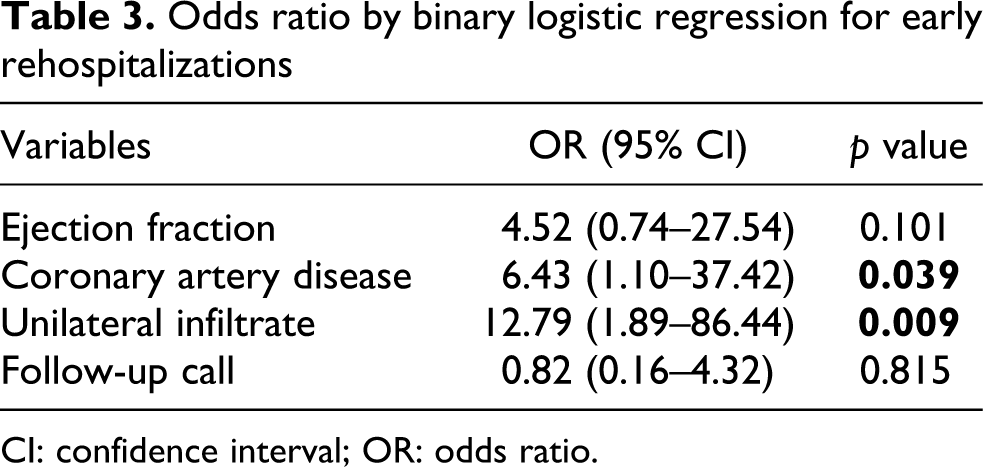
Binary logistic regression analysis showed that a history of coronary artery disease (odds ratio (OR) 6.43, 95% confidence interval (CI) 1.1–37.4) and the presence of unilateral pulmonary infiltrates on admission (OR 12.79, 95% CI 1.9–86.4) significantly increased the odds of early rehospitalization (Table 3).
Odds ratio by binary logistic regression for early rehospitalizations
CI: confidence interval; OR: odds ratio.
Discussion
The Jencks study of Medicare fee-for-service beneficiary claims data from 2003 to 2004 reported that the 30-day readmission rate for COPD was 22.6%. 5 The most frequent reasons were COPD, pneumonia, heart failure, and pulmonary edema. Chen et al. analyzed 65,497 COPD admissions in Hong Kong in 2006 and 2007; these included 15,882 unplanned readmissions (24.2%) within 30 days after discharge. 6 These patients with readmissions were more often men receiving public assistance living in a nursing home. There was no association with comorbidity. In our study, the early rehospitalization rate for COPD was 13.6% which is lower than the above 2 studies. This lower rate may reflect different patient populations, different patient management strategies, and/or better transition of care processes. We do know that our hospital made additional efforts to provide better transition of care to outpatient clinics, made more follow-up calls, and tried to organize follow-up within 30 days postdischarge, and these efforts could potentially explain this lower rate of early rehospitalization in our patients. 2,3 More details with case-by-case analysis about posthospitalization events and the indications for readmission might identify the opportunities for intervention.
Influenza vaccines reduce serious illness and death by 50%, in COPD patients, long-acting bronchodilators are more effective and convenient than short-acting bronchodilators, and inhaled corticosteroids are appropriate for patients with severe to very severe COPD and repeated exacerbations. 7 However, in our study 32.3% of patients did not receive long-acting bronchodilators and/or inhaled corticosteroids on discharge, and only 38.4% of patients had prior influenza vaccination. We need to develop protocols to provide more influenza vaccine and long-acting bronchodilator and/or inhaled corticosteroids in hospitalized COPD patients before discharge. The percentage of prior influenza vaccination in our early rehospitalization group was significantly higher than the nonearly rehospitalization group. This is most likely explained by an ongoing effort to administer influenza vaccine to every hospitalized patient who had not been vaccinated that year, provided there was no contraindication. Consequently, patients requiring readmission possibly had a higher chance of recent vaccination. Alternatively, patients receiving vaccination represented the most chronically ill and frailest patients and had a higher chance of readmission. In addition, only 44.4% of our COPD patients had pulmonary function tests done during the last 5 years, according to the data available in our electronic medical record. We probably need to make more consistent use of this testing to confirm the diagnosis of COPD, to assess COPD severity, and to monitor disease progression. 6 Recent guidelines published in the Annals of Internal Medicine provide an excellent framework for the management of COPD patients. 8 In particular, these guidelines make recommendations for inhaled bronchodilator therapy, pulmonary rehabilitation, and oxygen therapy. Garcia-Aymerich and coworkers have demonstrated that an integrated care plan which includes comprehensive patient assessment, education on self-management, tailored care following international guidelines, and access to specialized nurses can prevent hospitalization for exacerbations of COPD. 9 In addition, higher levels of usual physical activity reduce the risk for rehospitalization. 10 Pulmonary rehabilitation can both increase and maintain better levels of fitness and potentially has a role in reducing readmissions.
Use of β-blocker did not affect the rate of COPD early rehospitalization in our study, and this result supports the earlier studies which demonstrated that many patients with emphysema and chronic bronchitis can use β-blockers with few adverse events. 11 –13 β-Blocker therapy has been associated with reduced mortality, possibly due to a protective effect in patients with coexisting cardiovascular disease. Our study suggests that ischemic heart disease represents an important comorbidity in COPD patients and was associated with an increased risk for readmission (OR 6.4). Chen et al. reported that cardiac comorbidity was frequent in COPD inpatients (26.3% of the patients had ischemic heart disease) and was associated with an increased risk for COPD readmissions in female patients. 14 These patients warrant additional attention to ensure proper management of coronary artery disease and close monitoring after discharge from the hospital.
COPD exacerbations with chest X-ray consistent with pneumonia are associated with worse outcomes, including inpatient mortality, 90-day mortality, and frequent readmissions. 15 –17 Our study also found that unilateral pulmonary infiltrates increased the risk of early rehospitalization with OR of 12.8. Providing complete courses of appropriate antibiotics and early outpatient follow-up for COPD and pneumonia might help decrease the rate of early rehospitalization in these patients.
Limitations
COPD exacerbations in our hospital were managed by different physicians. It is possible that patients with acute respiratory distress secondary to asthma, congestive heart failure, and/or pulmonary embolus were misdiagnosed as having a COPD exacerbation. In addition, we identified the medical records used for this review by discharge codes which reflect both the quality of information in records and the hospital reimbursement strategies. We used information collected retrospectively from medical records, and some information was not consistently available in the records. The small number of patients in our study may give us inadequate power to detect the differences in risk factors between the two groups and probably does not support a rigorous statistical analysis of our data. We consider the logistical regression analysis results most useful for hypothesis generation.
Conclusions
Our results did not identify striking differences between COPD patients with early readmission and COPD patients with no early readmission after an acute flare. Our results do suggest that a history of ischemic heart disease and unilateral pulmonary infiltrates increase the risk of hospital readmission. Reviewing these risk factors before hospital discharge will help identify high-risk patients for readmission. These patients might need earlier follow-up in an outpatient clinic or other interventions to prevent early readmission, and this possibility should be investigated in the future studies. Influenza vaccine, maintenance long-acting bronchodilators and/or inhaled corticosteroids, and pulmonary function tests were underused, and these standards of care should be implemented to improve the overall quality of care in these patients. However, we did have a low overall readmission rate (14%), and this supports previous studies which suggest that early follow-up after hospital discharge of COPD exacerbation (which was a hospital initiative during this period) can reduce hospital readmissions.
Footnotes
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.