
Abstract
In a primary care setting, our aim was to investigate characteristics of patients classified as having chronic obstructive pulmonary disease (COPD) and currently being prescribed inhaled corticosteroids (ICSs). The electronic patient record system in each participating general practice was searched for patients coded as COPD (ICPC, Second Edition code R95) and treated with ICS (ACT code R03AK and R03BA, that is, ICS in combination with a long-acting β2-agonist) or ICS as monotherapy. Data, if available, on demographics, smoking habits, spirometry, COPD medication, symptom score, blood eosinophils, co-morbidity and exacerbation history were retrieved from the medical records for all identified cases. Of all patients registered in the 138 participating general practices, 12.560 (3%) were coded as COPD, of whom 32% were prescribed ICS. The final study sample comprised 2.289 COPD patients currently prescribed ICS (98% also prescribed long-acting β2-agonist), with 24% being coded as both COPD and asthma. Post-bronchodilator spirometry was available in 79% (mean forced expiratory volume in 1 second 60% pred (standard deviation (SD) 23.3)), symptom severity score in 53% (mean Medical Research Council score 2.7 (SD 1.1)) and 56% of the COPD patients had had no exacerbation in the previous year (and 45% not within the 2 previous years). Blood eosinophils were measured in 67% of the patients. Information on severity of airflow limitation was missing in 15% of the patients, and the combined information on symptom severity and exacerbation history was missing in in 46%. Most of the patients (74%) were managed only by their general practitioner. Although only one-third of the COPD patients were prescribed ICSs, our findings from this study of a large cohort of patients prescribed ICSs for COPD in general practice suggest that more detailed assessment of diagnosis and disease characteristics is likely to improve the risk–benefit ratio of maintenance therapy with ICSs in COPD patients managed in primary care.
Introduction
Chronic obstructive pulmonary disease (COPD) is the fourth leading cause of mortality world-wide 1,2 and is associated with substantial burden for both the individual patient and society. 3,4 The aim of maintenance inhaled therapy for COPD, including treatment with inhaled corticosteroids (ICSs), is to relieve symptoms, reduce risk of exacerbations and improve long-term outcome. 2,5 –7 Previous guidelines, or strategy documents, from the Global Initiative for Chronic Obstructive Pulmonary Disease (GOLD) proposed ICS for COPD patients at increased risk of recurrent exacerbations. However, the positioning of ICS in the management of COPD has been much debated recently based on findings in clinical trials published within the last few years. 8 –10 In line with this, in the strategy paper from GOLD since 2017, ICS is proposed as an add-on maintenance treatment for COPD patients, who despite treatment with long-acting bronchodilators, that is, long-acting β2-agonists (LABA) and anti-muscarinic antagonists (LAMA), still have exacerbations. 11
With increasing awareness of the potential side effects associated with ICS treatment in COPD patients including a possible increased risk of pneumonia, osteoporosis and diabetes, there has been an increased focus on identifying COPD patients with a favourable risk–benefit ratio for treatment with ICS. 11 –17
A large sample of patients with COPD from primary care in Denmark recruited in two previous surveys 1 year apart was examined with regards to enhancement of adherence to COPD guidelines. 18,19 By educating GPs and the general practice staff in the year between the two surveys, improvements were observed in the recording of forced expiratory volume in 1 second (FEV1), FEV1/forced vital capacity (FVC) ratio, smoking status and Medical Research Council (MRC) score. 18,19 In addition, the general practitioners more often provided advice on smoking cessation, physical activity and diet and were more likely to refer patients for pulmonary rehabilitation after the educational sessions. 18 Interestingly, a decline in the use of ICS to patients with mild COPD was observed between the two surveys. 18,19 In the first survey, 40% of patients were in monotherapy ICS, and in the second survey, 18% of patients were in monotherapy ICS, suggesting that relatively simple interventions in general practice may improve adherence to current guidelines. In an analysis of a large database comprising information on severity of disease, treatment with bronchodilators, MRC and COPD assessment test (CAT) score gathered through questionnaires and electronic patient records by Price et al. revealed that prescription of maintenance therapy for COPD was not according to guidelines, as some symptomatic patients received no treatment, and among those on maintenance therapy, the majority received ICS irrespective of severity of airflow limitation, concomitant asthma and exacerbation history. 20
A more recent study by Chalmers et al. found that two-thirds of COPD GOLD A and B patients prescribed maintenance therapy within 3 months of diagnosis were prescribed ICS-containing treatment. 21 Trends over time revealed a decline in initial ICS prescriptions, but it still accounted for 47% of initial prescriptions in 2015.
In a large cohort of patients with COPD managed in primary care, our aim was to explore clinical characteristics of patients currently prescribed ICSs.
Material and methods
The aim was to identify patients coded with a diagnosis of COPD in general practice, and thereafter enrol COPD patients currently being prescribed ICS. In order to be eligible for the study, the GP had to fulfil the following criteria: (1) One of the following Electronic Patient Journal (EPJ) systems: XMO, Clinea, WinPLC, Ganglion or Novax, and (2) diagnostic coding of COPD patients for a minimum of 3 years. Written information about the study as well as the invitation to participate was distributed to all interested GPs by the sponsor’s local representative (during the period 15th August to end of October 2017).
The participating GPs were guided to perform uniform searches in their designated EPJ system for the International Classification of Primary Care, Second Edition (ICPC-2) code R95 to identify patients with COPD. Identified COPD patients (ICPC-2 code R95) currently being prescribed corticosteroids were then identified through the ATC code R03AK (adrenergics in combination with corticosteroids) and R03BA (corticosteroids for inhalation). Search methodology was provided by the respective EPJ system houses. Search lists were manually confirmed by participating GPs. Among patients fulfilling the criteria for inclusion in the study, 20 patients were selected at random per clinic, if less than 20 patients were identified, data were registered for all patients.
All available information on demographics, clinical characteristics, comorbidities, level of blood eosinophils, annual audits and respiratory specialist visits, prescribed COPD medication, hospital admissions for COPD, duration of COPD, smoking status and previous COPD exacerbations were retrieved from the GPs medical records for each individual patient included in the study. The information was anonymized and entered directly into a secured database. Each patient registered in the database was assigned a project ID number. The participating GPs kept record of project IDs, names and the unique civil registration number (in Danish called the CPR number).
The present study was a non-drug, non-interventional study, and approval from the scientific ethical committee and the Danish Medicines Agency were, therefore, not mandatory. However, they were given all relevant study information, and the study was approved by the Danish Data Protection Agency.
Assessment of COPD severity
According to current guidelines, the severity of COPD was assessed on the basis of severity of symptoms, degree of lung function impairment and exacerbation history, provided the information was available from the GPs medical records.
Degree of dyspnoea and impact of symptoms was assessed by the MRC scale 22 and/or the CAT. Severity of lung function impairment was assessed by spirometry and, according to the classifications provided by GOLD, the patients were classified as either GOLD 1 (FEV1 ≥ 80% predicted), GOLD 2 (FEV1 ≥ 50% and < 80% predicted), GOLD 3 (FEV1 ≥ 30% and < 50% predicted) or GOLD 4 (FEV1 < 30% predicted). 11
Patients were also classified into four groups, that is A, B, C and D, following the GOLD 2017 group classification based on COPD symptoms (more symptoms MRC-scale score ≥2, and/or CAT score ≥10), spirometry classification and the number of exacerbations (high risk, two or more exacerbations the previous year or one hospitalization for COPD exacerbation).
Data analysis
Statistical analyses were performed using IBM SPSS version 25 (IBM Corporation, Armonk, New York, USA). Based on the measurements, the mean values together with one SD from the mean was calculated. The original data will be available upon request from the senior author (CSU).
Results
A total of 12,560 (3%) of 416,233 registered patients from the 138 participating general practices were coded with a diagnosis of COPD, of whom 3985 were currently prescribed ICS and, therefore, eligible for the present study. Of the eligible patients, 2594 entered the database, with the final cohort comprising 2289 patients (57.4% of the eligible patients), as 304 patients (11.8%) did not fulfil the inclusion criteria (a diagnosis of COPD and currently prescribed ICS) at the time of data collection; further details are given in Table 1 and Figure 1. Characteristics of the included COPD patients are given in Tables 1 and 2. The GPs had coded 23.6% of the patients as having both COPD and asthma.
Demographics of the patients with COPD (n = 2289) identified in general practice currently being prescribed ICSs.
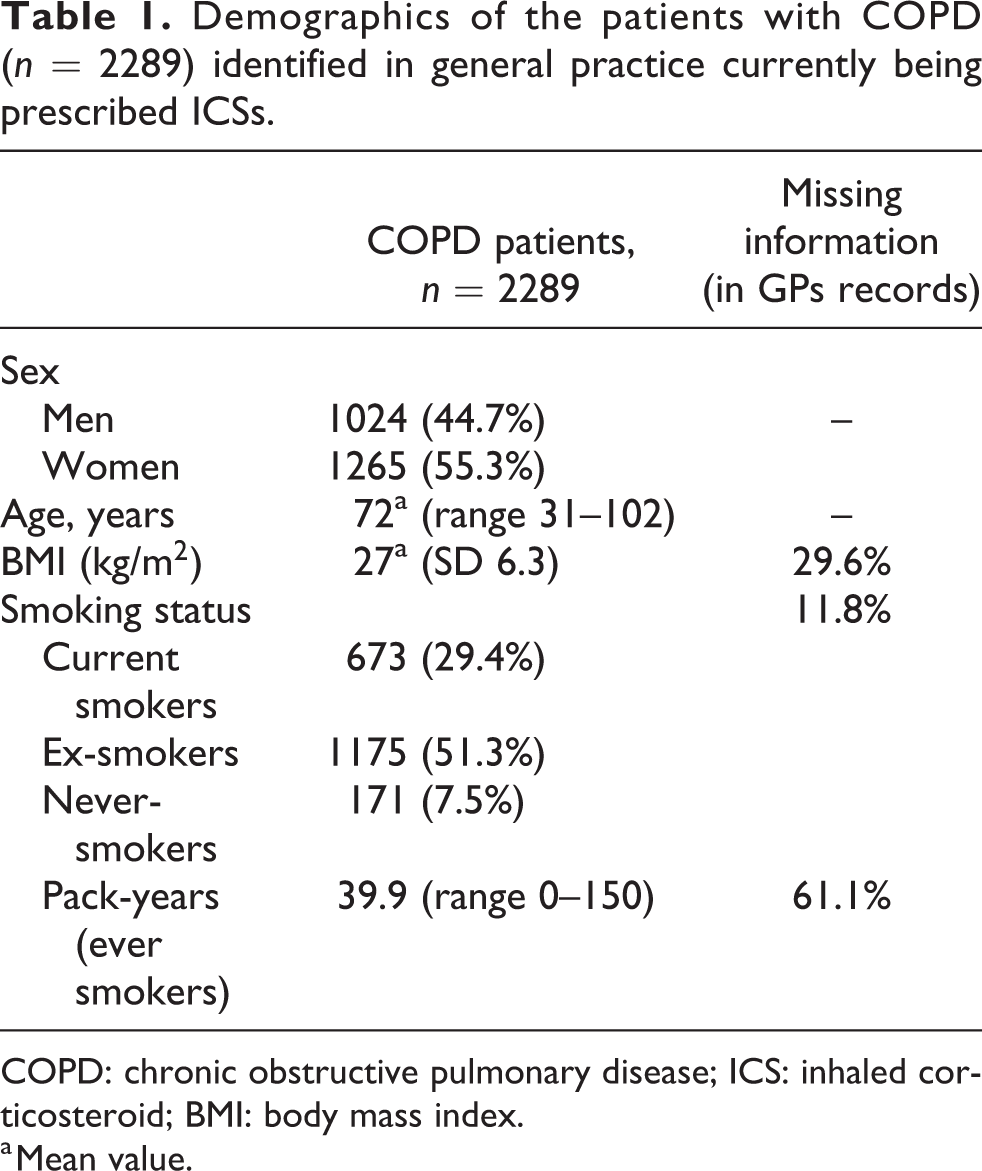
COPD: chronic obstructive pulmonary disease; ICS: inhaled corticosteroid; BMI: body mass index.
a Mean value.

Consort diagram showing the patient selection procedure.
Symptom score and lung function in patients with COPD (n = 2289) identified in general practice currently prescribed ICSs.
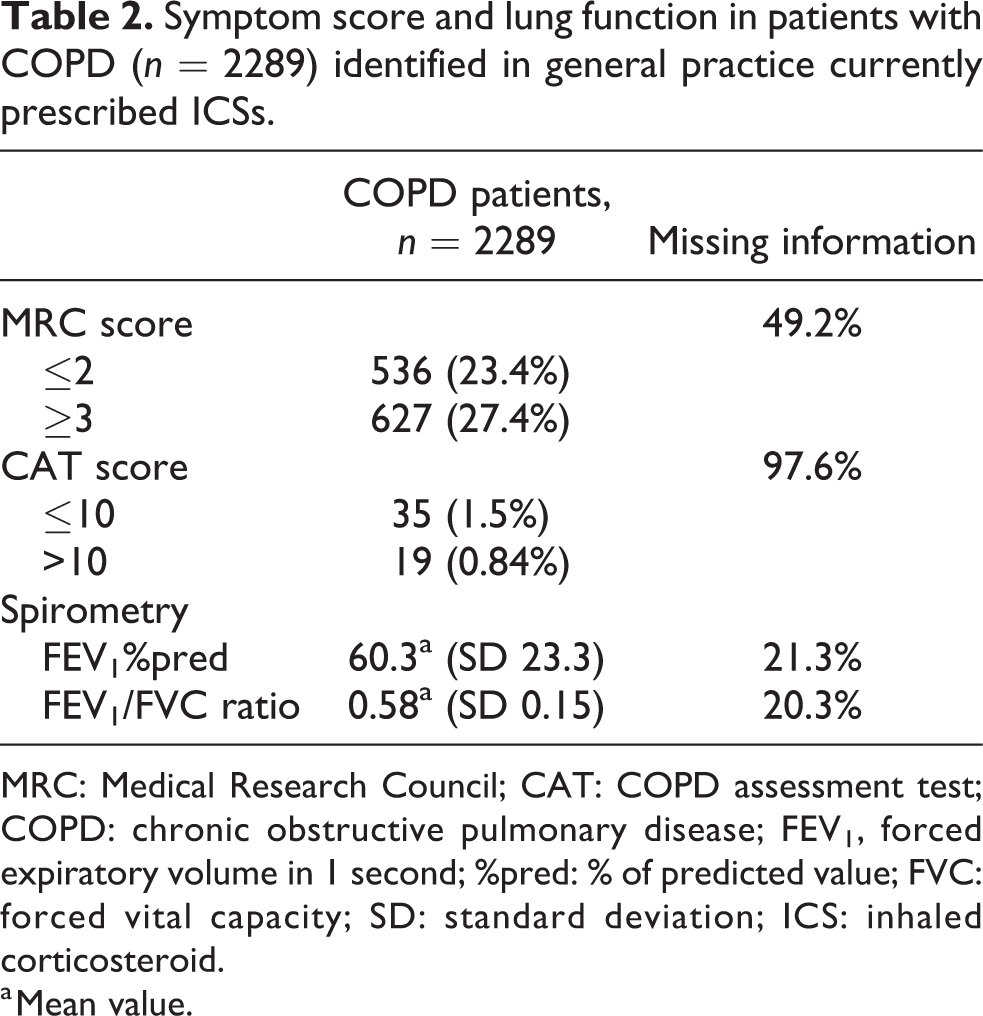
MRC: Medical Research Council; CAT: COPD assessment test; COPD: chronic obstructive pulmonary disease; FEV1, forced expiratory volume in 1 second; %pred: % of predicted value; FVC: forced vital capacity; SD: standard deviation; ICS: inhaled corticosteroid.
a Mean value.
Assessment of severity of symptoms
The CAT score was not widely used among the participating GPs as only 54 patients (0.9% the enrolled patients) had a registered CAT score (mean score 16.5), whereas 1163 patients had a registered MRC score (mean score 2.7) (Table 2).
Of the enrolled COPD patients included in the study, 79.7% had information on spirometry in their medical records and the mean FEV1/FVC was 0.58 (SD 0.15) (Table 2).
The enrolled patients classified according to the degree of airflow limitation, that is FEV1% predicted, severity of symptoms and exacerbation history according to GOLD I to IV and A to D are given in Figure 2.

Classification of enrolled subjects with COPD on ICS therapy (n = 2289) according to GOLD. (a) Upper panel based on symptom severity and exacerbation history (as recorded in the GPs medical records) and (b) lower panel according to degree of airflow limitation. COPD: chronic obstructive pulmonary disease; GOLD: Global Initiative for Chronic Obstructive Pulmonary Disease; ICS: inhaled corticosteroid.
Exacerbation history and concomitant therapy
More than half the patients (55.7%) had had no exacerbation of COPD treated with prednisolone and/or antibiotics within the last year, and 44.9% had not had an exacerbation within the last two years (Figure 3).

Hospital admissions for exacerbations, rescue courses of oral corticosteroids and antibiotics for exacerbations in COPD patients (n = 2289) currently prescribed ICSs (n = 0 exacerbations, n = 1 exacerbation and n > 1 exacerbations). COPD: chronic obstructive pulmonary disease; ICS: inhaled corticosteroid.
Most of the COPD patients were also on LABA therapy (98.2%), whereas 57.3% were on LAMA therapy. Most of the patients (74.4%) were managed only by their GP.
Comorbidities
The most common co-morbidity was cardiovascular disease (29.4%), followed by osteoporosis (18.9%) and 23.5% of the enrolled patients were also classified by the GP as having asthma (Table 3).
Presence of co-morbiditiesa in COPD patients (n = 2289) currently prescribed ICSs managed in primary care.
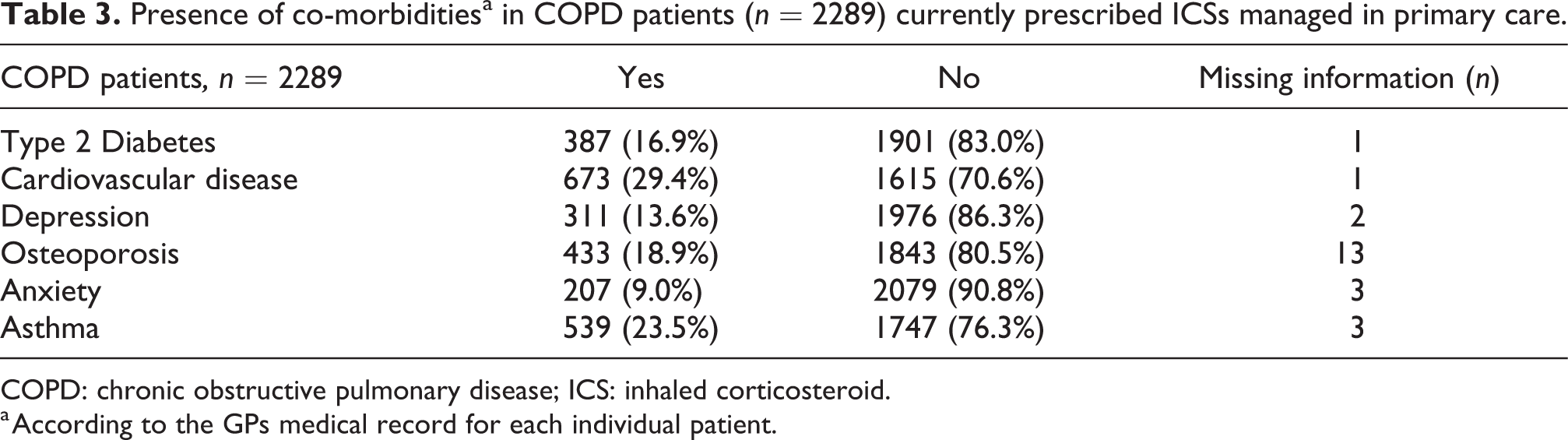
COPD: chronic obstructive pulmonary disease; ICS: inhaled corticosteroid.
a According to the GPs medical record for each individual patient.
Discussion
The present study showed that one-third of patients classified as having COPD in general practice were on maintenance therapy with ICSs. Furthermore, more than two-thirds of the identified COPD patients had information on post-bronchodilator spirometry in their medical records, and 24% were classified as having both COPD and asthma. Our findings suggest that prescribing ICSs for COPD patients in general practice may be guided more closely to the clinical characteristics of the individual patient.
The Danish Health Data Agency (in Danish called ‘Sundhedsdatastyrelsen’) found that two-thirds of all COPD patients in Denmark received ICS in 2013, while prescribing ICS had dropped almost 10% 4 years later. 23 Simultaneously, a rise in the prescription rate of long-acting bronchodilators occurred from one-fifth to one-third. 23 Opposed to the findings of the Danish Health Data Agency, a recent study of a German COPD cohort found that two-thirds of patients in GOLD groups A and B were treated with ICS despite recommendations set by GOLD. 2,24 Furthermore, patients in GOLD groups C (18.9 to 21.9% of patients received LABA therapy without a LAMA) and D (9.2 to 12.2% of patients received LABA without a LAMA) were undertreated with long-acting bronchodilators and 3.6% to 6.8% of the patients in these groups received a LABA monotherapy, despite recommendations by GOLD. 2,24
In our study, we have shown that a proportion of the included COPD subjects (67.4%) have a moderate blood eosinophil count, while a previous study by Vedel-Krogh et al. found patients with an increased risk of exacerbations with a blood eosinophil count exceeding 0.34 × 109/L. 25 However, results may have been confounded by patients with undiagnosed asthma, because only pre-bronchodilator spirometry measurements were obtained from the included sample. Compared to the current study, more than two-thirds of the included patients had information on post-bronchodilator spirometry.
In the present study, we found that a substantial proportion of COPD patients prescribed ICS had no history of recorded exacerbations within the last 2 years, which suggests that ICS are overprescribed for COPD in primary care managed patients. However, although information was obtained related to frequency of registered exacerbations and hospital admissions for COPD in the past 2 years, it should be emphasized that ICS has been shown to reduce exacerbation rate in patients with COPD, and by that some patients may have lower exacerbation rate than previously due to benefit from ICS therapy. Some further limitations should be emphasized in the current study. Consultations and prescriptions in primary care may not be sufficient to validate an exacerbation and the records provided by the GPs for the current study may, therefore, have over- or underestimated exacerbation rate in the included COPD patients. On the other hand, the individual participating patients GP have direct access, when the patient is in the consultation room, to information on filled prescriptions (through the so-called ‘Fælles Medicinkort’). The included COPD patients had, overall, moderate to severe airflow limitation, which may be related to the relatively high age of the patients. 26 Another limitation was that EPJs did not, as may be expected, contain all relevant information on characteristics of the COPD patients, and, in line with this, we may have missed some important details because of missing information. However, by studying subgroups of COPD, we may reduce inconsistency for some endpoints, such as blood eosinophil count in future analyses. Lastly, the relatively frequent missing information on dyspnoea, lifetime tobacco exposure and blood eosinophils may limit our possibilities for more complex statistical analysis, but nevertheless, the present study provides important insight into the characteristics of COPD patients managed in primary care.
The present study investigated characteristics of patients with COPD prescribed ICS in primary care and showed that ICS seems to be prescribed for COPD across the whole spectrum of disease severity and clinical characteristics. Our findings, therefore, may indicate that management of COPD patients in general practice may be tailored more precisely to the characteristics of the individual patient, and by that, improve risk–benefit ratio, not least regarding treatment with ICSs.
Footnotes
Author contributions
OS, NG, TS, CJ and CSU contributed to the acquisition of the data. OS and CSU analysed the data and drafted the manuscript. All authors contributed to designing the study, interpreting the data, revising the manuscript and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors declare that they have received fee for drafting the manuscript (OS as part of his candidate thesis at the University of Copenhagen) and as members of the steering committee of the study (NG, TS, CJ and CSU) from Boehringer Ingelheim, Denmark. The authors declare that they have no other potential conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was sponsored by Boehringer Ingelheim Denmark A/S.