
Abstract
While there are both ethical and practical imperatives to address health inequity issues related to chronic disease management for persons with social complexity, existing programs often do not appropriately address the needs of these individuals. This leads to low levels of participation in programs, suboptimal chronic disease management, and higher health-care utilization. The aims of this project were to describe the challenges related to availability, accessibility, and acceptability faced by socially complex patients with Chronic Obstructive Pulmonary Disease (COPD) who were eligible, but declined enrollment in a traditional Chronic Disease Management Program (CDMP). Using a qualitative descriptive study approach informed by a health equity lens, interviews with participants, managers, and a focus group with providers were used to gather data addressing the above aims. Qualitative data were analyzed using Braun and Clarke’s theoretical thematic analysis approach. The ability of participants to manage chronic disease was profoundly influenced by contextual and personal factors, such as poverty, disability, personal attitudes and beliefs (including shame, mistrust, and hopelessness), and barriers inherent in the organization of the health-care system. The existing chronic disease management program did not adequately address the most critical needs of socially complex patients. Challenges with accessibility and acceptability of chronic disease management and health services played important roles in the ways these socially complex participants managed their chronic illness. The individualistic approach to self-management of chronic illness inherent in conventional CDMP can be poorly aligned with the needs, capacity, and circumstances of many socially complex patients. Innovative models of care that promote incremental and guided approaches to enhancing health and improving self-efficacy need further development and evaluation.
Keywords
Introduction
Chronic Disease Management Programs (CDMPs) have been successful in empowering many individuals living with chronic illnesses, such as Chronic Obstructive Pulmonary Disease (COPD), to assume greater influence over their health and achieve improved health outcomes. 1 –3 These programs help patients make lifestyle changes, monitor symptoms, and adhere to treatment to prevent disease progression and reduce potential health complications by enhancing patient activation (the ability and confidence to manage his or her own health and health care). 4 Higher levels of patient activation have been associated with better treatment adherence and health outcomes. 5 –9
Not everyone who is eligible to participate in a CDMP, however, elects to participate and the characteristics of patients mostly likely to benefit from CDMPs are still being investigated. 10 Males, 11 indigenous people, 11 non-English speaking persons, 11 patients with low levels of readiness for self-management, 12 –14 and older persons 15 have been reported to be less likely to participate in CDMP programs. Cortis et al. 16 noted that persons with the greatest health needs are often the least likely to make use of any type of health service. Participation of populations described as “hard to reach” 17 or “unengaged non-users of service” 18 may be affected by a host of factors including low socioeconomic status and financial concerns, 4,10,16 low literacy levels, language barriers and cultural differences in values, 18 previous negative experiences with the health-care system, 18 fear of the unknown and authority, feelings of hopelessness or “not being ready,” perceptions of services as irrelevant, communication difficulties, limited access to information, attitudes toward help-seeking, fear, and misconceptions about services. 16,19 Social norms and expectations, social disorganization, and limited social capital can also limit engagement in those considered most vulnerable. 18,20
Any one of the above factors can restrict the capacity of patients to assume the proactive stance that Cramm and Nieboer 21 propose as a requirement for successful outcomes in CDMPs. Concerns that some CDMPs might serve to actually increase health inequities among certain groups of people with chronic illness have been raised. 22 –24 Although some CDMP programs in Canada have begun to offer programs that address the needs of patients considered “hard to engage,” the majority of existing programs lack the capacity to make the often major changes that are required. 25
The overall aims of this project were to describe the challenges related to availability, accessibility, and acceptability faced by socially complex patients with COPD who were eligible, but declined enrollment in a traditional CDMP, through the perspectives of the patients themselves, and through the clinical CDMP staff and a newly dedicated community-based case manager who promoted the CDMP in this population.
Setting and intervention
Within the Saskatoon Health Region (Canada, population approximately 336,000 people), the LiveWell Chronic Disease Management Program offers the Stanford-based COPD CDMP as one of the three component pillars. 26,27 The program consists of individual follow-up, evidence-informed optimization of management, exercise reconditioning and pulmonary rehabilitation, support and education and is delivered by specialty-certified nurse clinicians and educators in collaboration with physician directors and other interprofessional members of the health-care team (Figure 1).

CDM elements.
In Saskatoon, however, people experiencing personal, social, and economic disadvantage represent a significant number of individuals who could benefit from the COPD CDMP, but often decline participation. Quality improvement work within the health region identified that persons not enrolled in CDMP programs had higher levels of health-care utilization than those who received these supports.
To address this significant gap, the Health Region piloted a short-term (6 months) social work Case Manager position into the current CDMP program to allow for the collection of critical data about socially complex nonparticipants and to provide the opportunity to test novel approaches to engaging this group. Case management refers to a collaborative approach directed at meeting patient and family needs for care 28,29 and has shown promise as a means to improve outcomes and reduce health-care costs for frequent users of health services. 30 –34
Patients eligible for the LiveWell CDMP Program with complex social needs but who declined participation were referred by the Nurse Clinicians for follow-up by the Case Manager. The Case Manager actively established relationships with these patients through home visits, identifying needs, barriers and gaps, facilitating access to both health and social resources and benefits and providing ongoing education and support.
Conceptual model
The Framework for Conceptualizing Equity in Health Care 35 served as the organizing model for study design and analysis. This socioecological model proposes that equity in health care is affected by the key factors of culture, income, housing, gender, language, and (dis)ability. Equity is the result of the intersection of availability, accessibility, and acceptability. The model was modified by the authors to reflect the influence of personal attitudes and beliefs (Figure 2).
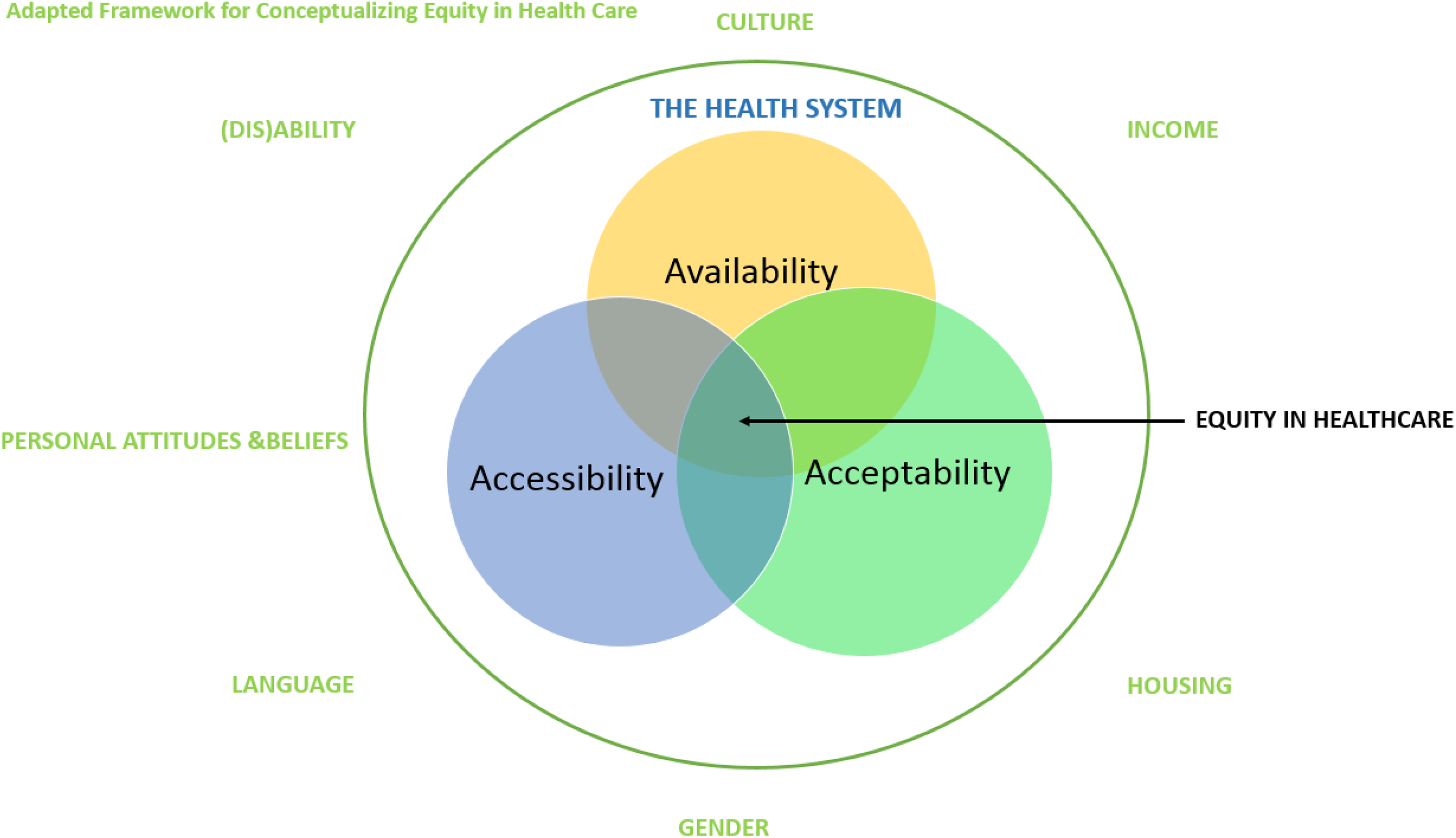
Modified framework for conceptualizing equity in health care.
Availability refers to whether services are provided within a community, while accessibility denotes the extent to which the health system is designed to meet the needs of health system users, in conjunction with the level of openness to the participation of underserved groups in the planning and evaluation of those services. 36 Literacy, language, gender, ethnicity, and geography are recognized to impact on the accessibility of health services. 37 Acceptability refers to the extent that services are provided in a way that meets the needs of distinct cultural, linguistic, ethnic, and social groups and incorporates culturally competent services and culturally safe spaces. 35
Methods
Our qualitative descriptive study used face-to-face, semi-structured interviews to elicit patient, Manager, Case Manager, and Nurse Clinician perspectives on the barriers to participating in a CDMP. Patients with a medically confirmed diagnosis of COPD who were referred to the CDMP, but who declined to participate, were recruited for participation in the case management program by the LiveWell Nurse Clinicians using a standard recruitment script. Patient interview questions were pilot-tested with one patient to comment on the flow and nature of the items. Patients were interviewed in their home or another location of their choice. A male research assistant Master’s student in Public Health was trained in interviewing and interacting with vulnerable persons. All qualitative data were digitally recorded and professionally transcribed.
Transcripts were entered into NVivo v. 10 and coded by the research assistant and DG, a doctorally prepared nurse with extensive clinical experience in chronic disease management, but who was not associated with the CDMP. Theory-driven thematic analysis was used, where initial coding involved a parallel, formative process of code-making and synthesis using a priori theoretical knowledge. 38 Use of NVivo allowed us to merge data across the participant groups. Data that did not correspond to the theoretical categories of the model were extracted and reviewed by the team to determine if there was sufficient evidence of patterns across subjects to constitute data-driven themes.
Ethical approval was granted by the University of Saskatchewan Behavioral Research Ethics Committee (Beh-REB #15-231). Patient and manager interviews were conducted by the research assistant, and DG conducted the clinician focus group. Signed informed consent was obtained from all participants.
Results
Profile of program participants
Thirty-seven patients received services from the Case Manager over the 6-month period from April to September 2015, primarily following a referral from the LiveWell Nurse Clinicians. Half of the patients were male (51.4%) with a median age of 53 (range 28–78). Table 1 describes key demographic characteristics.
Demographic characteristics of participants (n = 37).

Of the 37 patients, 9 agreed to be interviewed, but 5 of these were lost to follow-up (moved or unable to locate), leaving 4 patients who were interviewed. Interviews with participants (P; n = 4), managers (M; n = 2) and the social work Case Manager (CM; n = 1), and a focus group with nurses clinicians (NC; n = 5), as well as narratives of client stories constructed by the CDMP team, provided in-depth data.
Contextual and personal influences on CDMP participation
Poverty
The poverty experienced by patient participants had a profound influence on their capacity to participate in the CDMP. The majority of those who declined CDMP services, and all participants who completed the interviews, resided in areas considered both materially and socially deprived, based on an assignment by the Saskatoon Public Health Observatory. Figure 3 is a geographic information system (GIS) map of the 30 participants for whom postal codes were available (remainder had no fixed address). This illustrates the concentration of participants in Quintile 5, considered the most deprived quintile in the region.

Residence of participants by total deprivation quintile.
Patient participants described that they usually prioritized dealing with their everyday living concerns over health issues until they became seriously ill. This, in turn, affected their ability to address everyday concerns because they were too ill and created further problems with their health: I got so many things on my plate…I was worried about my COPD, then I got my cancer diagnosis. Social services…held back $500 bucks a month for the past four months. . I’ve been in here [the hospital] at the turn of the month and every month I’ve had to pay a $50 dollar penalty for late [apartment rental] fee. So the illness is costing me money that I truly, truly don’t have. (P2)
One of the root causes of missed appointments with health-care providers was the lack of financial resources interfering with patients’ ability to connect with health-care providers, particularly where telephones were not available or transportation to health-care appointments could not be afforded or arranged. It also affected patients’ ability to adhere to the basic tenets of managing their illnesses such as accessing prescribed medications and adequate nutrition. A manager noted the interaction between poverty and outcomes: The patient didn’t have the money to fill that prescription…Then one thing leads to another and then it escalates and pretty soon they’re in the hospital for something different and only a piece of that gets addressed…so it soon becomes very chronic.
(Dis)ability
Just over one third (37.8%) of clients presented with three or more problems, typically physical health (including medication management) in combination with social and/or mental health problems (housing, emotional/mental health well-being, friendships/social relationships, stressful life events/trauma, substance use and problem gambling, daily living skills). Twenty-one patients identified personal goals in their interactions with the Case Manager. The most common goals related to locating or improving housing (9–42.9%), dealing with substance use (6–28.6%), financial concerns (5–23.9%), and family concerns (5–23.9%). Other goals related to improving physical and mental health, strengthening social networks, getting to appointments, transportation, accessing community supports, legal issues such as obtaining parole, and learning to read.
Low levels of general and health literacy were major barriers for a number of patient participants in attempting to manage their chronic illnesses even in the presence of health care. “I didn’t know how to talk to social workers. Like I thought they were all above me and everything and they controlled my life. I was scared of them” (C01). Patients did not always recognize the signs of chronic disease or worsening symptoms and thus did not seek treatment until these conditions were well-advanced: “They end up coming in with complications like an amputated toe and some of them don’t even find out they have diabetes until then” (NC).
Personal attitudes and beliefs
At a personal level, feelings of shame about health conditions or their living circumstances further isolated and made it more challenging for providers to care for participants: “[This group of patients] really hate to admit that they do not have the funds to afford their supplies…like their inhalers or their diabetes medications. Or they don’t have food…The conditions where they live…They’re embarrassed” (NC). One participant chose not to fully disclose all of her health conditions to the Case Manager: “I didn’t tell [Case Manager] at first that I had Hep C and HIV. My daughter did because I was ashamed of it” (P3).
Lack of trust in other people posed an important barrier to establishing the interpersonal connections needed for patients with complex social needs to engage in the CDMP. Fear of their condition, or of what the CDMP program might entail, resulted in avoidance. Some participants described their hopelessness about the possibility of improving their health and their overall circumstances. “You don’t feel so pessimistic, or down, or dare I say, sometimes suicidal; sometimes I think about that. You know because what’s to look forward to nothing, you know just…grief” (P4). Hopelessness was recognized as a key barrier to engaging socially complex persons in the CDMP by health-care providers.
Good health was valued when their basic social needs were addressed. A number of patient participants found the motivation to improve their own health because others were relying on them. “If I’m not healthy and don’t take care of myself, I can’t take care of others…They look up to me so I’ve got to be healthy for my granddaughter” (P2).
Participants often demonstrated resourcefulness when they had means to improve their health and social isolation. In speaking about trying to deal with his need for social contact, one patient participant said: “I’m too much time by myself and I get very unproductive…whereas, if I’m better if I’m responsible to someone else - this is why I got a cat” (P1). Unfortunately, this strategy couldn’t be managed long term because of the participant’s frequent hospitalizations: “With this stuff going on now, I could go home to find a rigid cat. So I had to give the cat away” (P1).
Health system influences on participation in CDMP
Availability
Availability refers to the extent to which the health system is designed to meet the needs of health system users, in conjunction with the level of openness to the participation of underserved groups in the planning and evaluation of those services. There was agreement from both patient participants and health-care providers that the existing CDMP program did not address the most critical self-identified needs of socially complex patients and thus, was of relatively low interest to them: Patients have to see the value of the service that you’re suggesting that they get involved in. And that value has to match what their needs are. And so if they can’t connect that what you have to offer…then they’re much less likely to become involved. (M)
Accessibility
Accessibility to CDMP programs and providers was a major concern. The expectation that patients living with social complexity would travel to providers was repeatedly noted as a barrier to participation in the CDMP: “People are not always prepared to come to us. They would prefer to build that relationship first…we need to go to them” (M). Particularly for patients living with COPD, traveling to appointments with CDMP providers was a challenge: These are people who can’t leave their house because they are so short of breath even the bus stop is too far. And so how can we expect somebody to make an appointment who can’t catch a bus…they’re booking off almost an entire day to get through to get to that appointment and back (CM).
Acceptability
The trust issues experienced by patient participants in their everyday lives were often exacerbated by experiences at the health-care system level. Previous negative experiences and perceptions impacted patients’ willingness to engage in the CDMP: “Before, I used to use [street drugs] and Emergency knew me from that, but they also knew that I quit. And they still treated me like I was a user” (P1). The power differential between providers and patients reinforced and augmented these patient participants’ sense of powerlessness. Patient participants had often had consistently dehumanizing experiences with health-care providers in the past that created long-standing mistrust: “When they [health care providers] found out I was HIV, they’d stick me in a corner and leave me there for hours and deal with other patients” (P4).
The judgmental and paternalistic approach that could be assumed by CDMP providers presented barriers to engaging people with complex needs: “[Patients] feel they are going to be scolded for not changing their lifestyle” (M). The key foundational ethos of self-efficacy underpinning traditional CDMP programs was reflected in providers’ decisions not to pursue contact in the absence of responses from prospective participants: “You phone ‘em once, you phone ‘em twice, you left a message, they didn’t call back; done. They don’t wanna participate. So we take that as a no and we never follow it up” (M). Even when patients did engage in CDMP programs, there was relatively little understanding on the part of some providers of factors limiting participation: “We have people who are living in poverty and trying to get their next meal, “How am I gonna eat?” And yet we write them off because they don’t show up for an appointment” (CM).
Discussion
Recognition of the need to address “upstream” factors that increase vulnerability (such as housing and poverty) before expending energy on disease self-management efforts 39,40 is not recognized or well incorporated in many conventional CDMP programs. According to Mills and Vanden, 39 the fundamental premise is that existing CDMP programs can work for all persons with chronic illnesses, whereas they assert that the dominant approaches to the CDMP actually best serve the needs of White, middle-class women. Key assumptions of CDMP programs often do not reflect the realities and capacities of people living with complex personal and social needs and can act to limit engagement with the health-care system in general, and CDMP programs in particular. Our findings support a report 41 noting the mismatch between the Stanford CDMP program and what is needed, and wanted, by vulnerable populations.
The issue, then, is how to draw the attention of funders and systems to the potential value inherent in personalizing services to the largely silent and politically invisible population of vulnerable persons living with chronic illnesses. The rising prevalence of chronic disease among the growing number of older population is estimated to result in significantly increased health-care costs in the near future. By 2020, chronic diseases are anticipated to be responsible for 73% of all deaths globally and account for 32% of the global burden of disease. 42 Given that CDMP originally developed as a response to the rising prevalence of chronic conditions, 40 the unprecedented pressures resulting from chronic diseases may afford new opportunities for innovation in the area of CDMP.
We don’t have to start from the beginning, as work has been done to address many of these important issues. Six community-informed and patient-centered practices to improve care for socially at-risk populations could be incorporated into CDMP programs to better serve those with socially complex needs. 43 These recommendations include (a) a commitment to health equity, (b) data and measurement to understand health risk factors and patterns of care, (c) comprehensive needs assessment, (d) collaborative partnerships across teams and service sectors, (e) care continuity, and (f) engaging patients in the design of individualized care.
Limitations
The challenges of conducting research involving “hidden” populations, such as those with social or economic disadvantage, are well-recognized. 44 This project engaged individuals experiencing precarious housing, necessitating frequent moves. The majority had neither a landline nor a cell phone, making them difficult to locate. While only four patients participated in the interviews, their voices provide important perspectives not frequently heard in the chronic disease literature.
Conclusions
The underlying assumptions of conventional CDMPs can be poorly aligned with the needs, capacity, and circumstances of many socially complex patients. Our findings illustrate specific barriers that exist both within and outside of the health-care system and suggest alternative approaches for improving the CDMP for socially complex patients. Innovative models of care that promote incremental and guided approaches to enhancing health and improving self-efficacy require implementation and evaluation.
Footnotes
Authors’ Note
Thilina Bandara is now affiliated with Alberta Health Services, Edmonton, Alberta, Canada.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Canadian Foundation for Healthcare Improvement.