
Abstract
The objective of this study is to review available functional status measures (FSMs) validated for use in the chronic obstructive pulmonary disease (COPD) population and categorizing the measures by their commonalities to formulate a framework that supports clinicians in the selection and application of FSMs. A literature review identifying valid and reliable measures of functional status for people with COPD was undertaken. Measures were thematically analyzed and categorized to develop a framework for clinical application. A variety of measures of activity levels exist, with 35 included in this review. Thematic categorization identified five categories of measures: daily activity, impact, surrogate, performance-based, and disability-based measures. The vast variety of FSMs available for clinicians to apply with people who have COPD may be overwhelming, and selection must be thoughtfully based on the nature of the population being studied/evaluated, and aims of evaluation being conducted, not simply as a standard measure used at the institution. Psychometric testing is a critical feature to a strong instrument and issues of reliability, validity, and responsiveness need to be understood prior to measurement use. Contextual nature of measures such as language used and activities measured is also important. A categorical framework to support clinicians in the selection and application of FSMs has been presented in this article.
Introduction
Functional status measures (FSMs) are instruments generally used to evaluate the impact of a person’s health condition on their ability to perform activities. These measures have also been referred to as activity (or functional status) measures, questionnaires, instruments, or tools. FSMs were initially developed to describe an individual’s participation in activities of daily living; however, functional status is sometimes more broadly used as a term for the evaluation of other types of function such as social, psychological, physiologic, and emotional. This article will use the term FSM as it relates to the direct or indirect measurement of activity by patients with chronic obstructive pulmonary disease (COPD).
Why measure activities? FSMs can provide detailed information on what individuals do, providing a window into the daily life of patients. The development of FSMs in the 1950s and 1960s focused on grading disability or the degree to which patients required assistance in the long-term residential care setting. However, since this time, expansion of the application of FSMs, such as for patients with chronic disease, has allowed clinicians to use FSMs to describe progress secondary to the disease, or in response to therapy.
In the past 30 years, there has been a great deal of interest in quantifying the degree of activity limitation for patients with COPD. During this time, activity monitors were introduced to measure activity levels as purportedly, a more reliable method due to their objective nature, as opposed to the subjective nature of FSMs. However, activity monitors have limitations in measuring small changes in daily life and patterns of activities in patients. 1 Compared to FSMs, activity monitors have the disadvantages of expense, limitation in detecting steps in those with slow walking speed, evaluation of predominantly lower extremity movement, and failure in some instances to provide information specific to what activity is being performed, 2 for example, making a bed versus washing the dishes. More recently, attempts have been made to evaluate patients with both types of measures, resulting in complimentary information being gathered. 1
Numerous FSMs exist, most developed for purposes of measuring activities in patients other than COPD. Many have the potential to be applied in the COPD population after the measure has undergone appropriate psychometric testing. For example, the Nottingham Extended Activities of Daily Living Scale 3 was developed in the 1980s for use with stroke patients, and has now been validated for use in the COPD population. 4 This transferability of FSMs between patient population groups has led to a vast array of measures being available to clinicians, with a potential for confusion over which measure is the most appropriate for specific scenario use. Observing patterns of uniqueness of measures led the authors of this article to consider categorizing FSMs to support clinicians in decision-making. Providing a categorical framework of FSMs for the pulmonary community would be beneficial for greater clarity in the selection and informed application of these measures.
The purpose of this article is to review available FSMs that have been validated for use in the COPD population and categorizing the measures by their commonalities. Characteristics and unique qualities of the instruments will be highlighted, and a framework for selection of a measure will be presented to support the appropriate application of the measures for both clinicians and researchers. The features presented will include ease of use (reflected in time to administer, scoring, etc.), time frame, psychometric properties (e.g. validity, reliability, responsiveness), and minimal clinically important difference (MCID).
Methods
Establishing the FSM categories was completed in three phases. First, FSMs were identified that were commonly used in COPD patients through a literature search of PubMed and Google Scholar. Three recent systematic reviews of FSMs were identified, published in 2014 and 2016 5 –7 and FSMs presented in these systematic reviews obtained. A reference list check of all papers included in the review was also completed to source all FSMs for use with COPD patients. Measures that were included in the synthesis had to meet the following criteria:
Validated for use with the COPD population.
Documented beginning psychometric properties of the measure, reporting on validity and reliability.
Published in English.
Full-text articles published in peer review publications.
Tools publicly available to review.
Instruments were excluded if they were not found to have been used in COPD patients, were never tested or used beyond the initial development after 5 years or more, have not been used for measurement with the COPD population for a decade or more, or where the scoring system changed too frequently to reliably report the psychometric properties. Papers considered for inclusion were reviewed by the two authors, and consensus reached on inclusion by discussion.
The second phase was to complete a subsequent search of PubMed and Google Scholar to obtain copies of the measures and the literature reporting on the psychometric properties of all FSMs identified for inclusion. The psychometric properties of the FSMs were then extracted from the papers by one author. While psychometric properties often receive less attention, inadequate testing of measures may result in failure to obtain the desired information about the patient/study, or provide false or misleading conclusions. Responsiveness of the instrument measuring the activity for impact of COPD or following treatment (e.g. pulmonary rehabilitation) was also recorded. The MCID of the measure was noted; however, as this information was not always available, papers were not excluded if MCID had not been determined.
Descriptive analysis of the components of the measures was then undertaken by one of the authors, grouping papers based on the purpose of the FSM, number of activities evaluated, how the activities were evaluated, how the FSM was administered, and whether it was tested and used in COPD patients. Finally, the instruments were thematically organized according to concepts. Initially, information on the types of activities measured, the number of activities evaluated, time taken to complete the entire measure, total number of items (questions) in the measure, time frame for administering, psychometric measurement properties (as previously described), and process of completing the measure, including scoring and whether nominal, ordinal, or interval scores, were extracted from the papers. The purpose of the FSM was the primary driver in developing the themes.
Results
A total of 61 FSMs were identified, with 35 included in this review and thematic analysis. A list of all FSMs reported for use with COPD patients are provided in Table 1, noting rationale for those excluded. The main reasons for exclusion were, they had either not been tested in the COPD population or testing was limited to the initial instrument development.
List of FSMs considered for inclusion with reasons for exclusion.
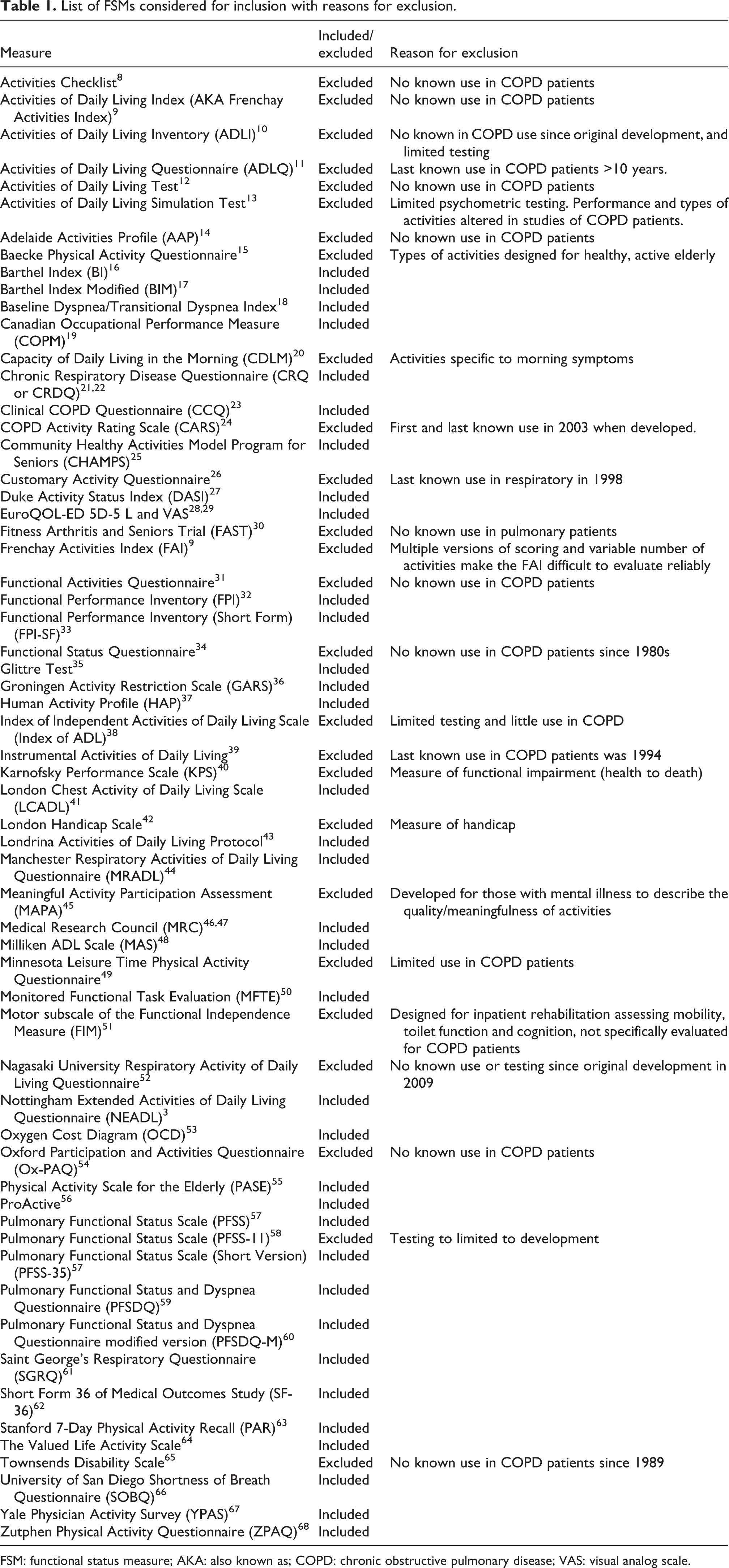
FSM: functional status measure; AKA: also known as; COPD: chronic obstructive pulmonary disease; VAS: visual analog scale.
Categories of measures
Five themes of measures were identified: daily activities, impact, surrogate, indirect performance-based, and disability-based measures. These themes formed five categories of measures.
Measures that looked at participation in a variety of activities were labeled Activity Measures. These measures evaluated the ability of the patient to engage in numerous activities often assessing domains of self-care, home management, ambulation, and participation in social and recreational activities.
Activities that were associated with symptoms were labeled Impact Measures. These measures evaluated how symptoms (primarily dyspnea and/or fatigue) affected the person’s ability to participate in activities. A measure that is classically used to measure dyspnea is the Medical Research Council (MRC) Scale 46,47 ; however, because this scale focuses on the effect of dyspnea on walking limitations, it could also be considered an Activity Measure. Additionally, one could argue that the MRC reflects disability because like the Disability Measures, the MRC categorizes patients as ambulatory or housebound.
Where activities were subscales or domains of health status questionnaires, such as the physical function subscale of the Medical Outcomes Study/SF-36, 69 these measures were labeled Surrogate Measures of activities. These subscales are often used as substitutes to establish concurrent validity of Activity Measures; however, the activities in these Surrogate Measures sometimes included evaluation of emotional function making them not purely FSMs. The domains of these health status measures comprise part of a total score that reflects overall health status or health-related quality of life. Where feasible, the psychometric properties of the individual domains/subscales were reported.
Indirect Performance-Based Measures as a category describes measures used to evaluate the individual’s potential to engage in activities by observation of typical body motions. There are limited numbers of these measures but their contribution to understanding patients’ limitations in activities made them candidates as FSMs.
Disability-Based Measures either observe and rate an activity or have the individual self-report their level of independence with activities. These instruments were initially designed for patients in long-term care settings such as nursing homes or those limited in activity due to stroke or orthopedic surgery.
Figure 1 provides a pictorial illustration of how these categories address functional status. For example, the Activity Category measures “do you do it (the activity listed)?” In relation to activities, the Disability Category asks, “can you do it?” and so on.

An illustration of the five categories of functional status measures.
Of the measures identified, 17 instruments were deemed to fit in the category of Activity, 5 Impact, 5 Surrogate, 3 Performance-based, and 5 Disability-based measures. It was noted that some measures could be considered overlapping with other categories. For example, FSMs among the Impact Measures were a reflection of both an individual’s participation in activities (Activity Measure) and symptoms with the activity (Impact). However, because these measures ask what activities individuals have reduced or no longer perform because of dyspnea (e.g. Oxygen Cost Diagram, MRC, etc.), they were also candidates for being considered Activity Measures. Where there was overlap, these measures are noted in the comment column of each table (Tables 1 to 5), and explicitly presented for each FSM in Table 6. For example, the MRC is an Impact measure, but overlaps with both the Activity and Disability measures.
Description and psychometric properties of daily activity measures.

MCID: minimal clinically important difference; SA: self-administered; RA: rater-administered; NA: not available; ICC: intra class coefficient; METS: metabolic equivalent units; COPD: chronic obstructive pulmonary disease; TS: total score; act: activities; dysp: dyspnea; PR: pulmonary rehabilitation; VO2: oxygen consumption; PF: physical function; EE: energy expenditure; Accel: accelerometer.
* Overlap with another category.
Description and psychometric properties of impact measures.

MCID: minimal clinically important difference; SA: self-administered; RA: rater-administered; ICC: intra class coefficient; PR: pulmonary rehabilitation; NA: not available; Ped: pedometer.
*Indicate the instrument overlapped with another category.
Description and psychometric properties of subscales of surrogate measures.*

COPD: chronic obstructive pulmonary disease; MCID: minimal clinically important difference; SA: self-administered; RA: rater-administered; ICC: intra class coefficient; PR: pulmonary rehabilitation; act: activities; dysp: dyspnea; VAS: visual analog scale; CI: confidence interval; NA: not available; TS: total score; ILD: interstitial lung disease; PCS: physical component score; PF: physical function
* Overlap with another category. The domains representing activity levels (e.g. dyspnea, physical function) were reported: CRQ: dyspnea; CCQ: functional state; SGRQ: activity; SF36: physical function scales.
Description and psychometric properties of protocol/performance-based measures.

MCID: minimal clinically important difference; NA: not available; COPD: chronic obstructive pulmonary disease; ICC: intra class coefficient; RA: rater-administered.
Description and psychometric properties of disability-based measures.

MCID: minimal clinically important difference; SA: self-administered; RA: rater-administered; TS: total score; NA: not available; COPD: chronic obstructive pulmonary disease; ICC: intra class coefficient.
Listing of FSMs by categories and identifying categories with which they overlap(X).

FSM: functional status measure. Shaded columns indicate the activities within the respective categories.
a Refer to Table 1 for abbreviations of FSMs.
Design and psychometric properties of the FSMs
Tables 1 to 5 summarize the characteristics of each measure, presenting measures by each of the aforementioned categories. The number of activities evaluated is reported for each measure (specifically the number of unique activities addressed in each measure). Those measures with more activities often allow a better understanding of the breadth of activities affecting the patient. The fewer the activities, the less time to complete, especially with dichotomous (Yes/No) answers. However, Yes/No responses may provide limited information. For example, brevity may sacrifice information on the frequency, the difficulty or the need for assistance with the activity or if the activity is no longer performed due to a respiratory problem. It was noted that in selected FSMs, if the patient did not perform the activity, they are asked to estimate their performance if they could engage in the activity. No studies are known to evaluate the consequences of this type of estimate on the validity of the data.
The types of activities evaluated are diverse across all measures. The user should consider if the activities of the FSM satisfy their needs for understanding their population. For example, activities designed for a younger or healthier older population (e.g. playing soccer, cycling, etc.) are less relevant to patients who are impaired from their respiratory problem or other comorbidity such as poor balance. Activities that may be more gender-specific may result in missing data (e.g. cooking, washing laundry, mowing the lawn, etc.), because these activities may not be undertaken equally among genders. The type of scoring is important, since some responses are dichotomous, or on a 0–10 scale, while others ask for the frequency and time spent in the activity. Generally, the more complex the scoring (e.g. weighted or reversed scoring), the more time-consuming scoring becomes, unless a computerized program is readily available.
Most measures reviewed were self-reports; however, some categories had predominantly observer/assessor ratings. This was true for the Performance-based measures. The time to take/administer the instruments were often under 10 minutes (range 1–20 minutes). Instruments varied in the time frame in which the activity was performed ranging from current to past 3 months. Time frame is a consideration if an intervention requires more time to take effect than identified in the FSM. Of note, the psychometrics of the instrument may be changed if a user randomly selects a time frame or does not utilize the entire measure (e.g. only administers one domain of an FSM) other than specified by the developer.
Discussion
This review of the literature has identified a diverse range of measures available to the clinician evaluating functional status for people with COPD. This diversity likely reflects the numerous reasons why functional status is measured for people with COPD in the clinical and research objectives. Considering the diversity of measures available for use, selection must be thoughtful based on the nature of the population being studied, and evaluation being conducted, not simply used because it is a standard at the institution. The options are varied and may be overwhelming. Through categorizing the FSMs and providing a summary of design and psychometric properties of the measures, this article aims to guide clinicians and researchers alike in the selection of the most appropriate measure for their situation.
While measuring functional status is a complex construct, not all measures could be easily categorized into one theme. We found measures that overlap between categories. Further, some aspects of FSMs may not be considered “activity measures” by some. For example, the chronic respiratory disease questionnaire (CRQ) 22 dyspnea domain can be considered an “impact” measure, as this most closely measures function in the CRQ (see Surrogate category). On the other hand, the Saint George’s Respiratory Questionnaire (SGRQ), 61 also a health status measure, has an “activity” as well as a symptom domain. However, this domain queries about many symptoms, not only dyspnea with an activity. Arguably, the dyspnea domain of the CRQ could be an Impact-Based Measure because it asks patients to rate the severity of their dyspnea with each activity. However, because it is a subscale of the CRQ, we determined it best fit with other Surrogate Measures. On the other hand, the Medical Research Council Modified version (mMRC) with 5 grades (0–4) 46,172 has been used as both a measure of dyspnea and disability. 47,95 While more commonly known as a dyspnea measure, the mMRC evaluates the impact of dyspnea on activity levels (primarily walking) and therefore meets our criteria for an Impact-Based Measure. However, the mMRC could also arguably be justified as a disability measure because the grades provide a distinct indication of impairment, that is, activity limitation (breathlessness only with strenuous exercise) to severe limitation (too breathless to leave the home). In interpreting the categorization, clinicians and researchers therefore may select an FSM based on the overlap. This could be of particular use when more than one domain or construct is to be measured, saving patients time in completing only one tool instead of multiple. While the creation of this framework and categorization of FSMs has attempted to simplify selection of instruments, extensive consideration by clinicians and researchers alike is still needed prior to selection of an FSM to ensure that the most efficient and targeted tool is indeed selected.
Psychometric testing is a critical feature to a strong instrument and issues of reliability, validity, and responsiveness should have been demonstrated, and through this review a summary of these properties has been synthesized for clinicians to access. Where psychometric properties of an instrument are not available in the literature, further research should be completed prior to clinical application of the tool. The framework presented in this article provides information only on tools that have been assessed, and therefore, this article is intended as one of many resources for clinicians to draw on.
The available FSMs to date have predominantly been developed and evaluated in English language countries with European-based cultures, and this should be considered when selecting a measure. Some activities identified in the original development of the instruments may not be relevant for some countries/cultures/genders/age groups. For example, FSMs containing activities such as soccer, shoveling snow, and ice skating may not be relevant to certain areas of the world or to the elderly individual with moderate to severe disease. Further, some instruments used gender-specific terms or stereotypes to describe activities. This may result in significant missing data. In the development of an instrument, there should be virtually no missing data (i.e. the instrument must make allowances for activities never performed, unrelated to COPD). On the other hand, if a study finds missing data occurring, they should be vigilant for the reasons for lack of response. For culturally responsive and adaptable health-care practice, ethnocultural interpretation of the measures should be evaluated prior to selection for application, and research into application of the FSMs to broader diverse communities is needed.
In evaluation of reading level of FSMs included in this review, most instruments attempt to attain reading at the 5th or 6th grade reading level (although not always stated); however, the nature of terms used in health care (e.g. breathlessness) may result in higher than desirable reading levels and may impact the psychometric properties of the FSMs. Understanding the reading and health literacy of the population group should also be a factor in selecting an instrument. Health literacy is the level to which an individual has the capacity to obtain, process, and understand basic health information and health-care services available to make informed decisions on health-care management. 173 Low levels of health literacy are readily reported for people with COPD and are linked to poorer health outcomes. 174 –176 Cognitive capacity may also impact the ability to complete the FSM. The incidence of cognitive impairment for people with COPD is greater than the general population with structural brain abnormalities, such as decreased hippocampal volume, 177 increased deep or infratentorial microbleeds, 178 and white matter lesions, 179 being more frequently evident. When measuring functional status, should the patient’s reading, cognitive, and literacy level be below that required, this could significantly impact the psychometric properties of the tool and lead to inaccurate information and conclusions. Further, research in understanding the impact of reading or literacy levels on the psychometric properties of FSMs is warranted to ensure that the tools are valid and reliable across different cultural groups.
Conclusions
A diverse range of measures are available to the clinician and researcher looking to evaluate functional status for people with COPD. The establishment of the many FSMs is likely related to the numerous reasons for why functional status is measured for people with COPD. Considering the diversity of measures available for use, selection must be thoughtful based on the nature of the population being studied, and evaluation being conducted, not simply because it is a standard at the institution. Psychometric testing is a critical feature to a strong instrument and issues of reliability, validity, and responsiveness need to be understood prior to measurement use. Contextual nature of measures such as language used and activities measured is also important. One approach to categorizing FSMs was presented to include daily activities measures, impact measures, surrogate measures, indirect performance-based measures, and disability-based measures. A summary of design and psychometric properties of the measures was provided as a guide to clinicians and researchers in the selection of the most appropriate application of a measure.
Footnotes
Authors’ note
Portions of this article were presented at the International Conference of the American Thoracic Society, Washington, DC, USA, May 2017.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SL is developer of the PFSDQ and PFSDQ-M referred to in this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.