
Abstract
Many people with chronic obstructive pulmonary disease (COPD) undertake pulmonary rehabilitation more than once. This study examined patient experiences and health professional perspectives regarding repeating pulmonary rehabilitation. Participants were 14 patients with COPD and 15 health professionals. Patients had undertaken pulmonary rehabilitation at a tertiary hospital; health professionals were doctors, physiotherapists, and nurses. Semi-structured interviews were conducted, and data were analyzed using thematic analysis. Patients described improved fitness and better breathing after repeating pulmonary rehabilitation; however, some also reported that repeating required confronting their disease progression. Improved confidence and motivation were an important outcome of repeating. Although most participants had attended community-based exercise classes, they valued the greater intensity of exercise and closer supervision that came with repeating pulmonary rehabilitation. Health professionals reported referring patients to repeat pulmonary rehabilitation if they had worsening functional capacity, an exacerbation, or hospitalization. There was no agreement regarding the optimal time for repeating and many would only re-refer if the patient demonstrated motivation to attend. In conclusion, patients with COPD reported many symptomatic benefits from repeating pulmonary rehabilitation and gained confidence from a supervised program. There was no agreement between health professionals regarding the optimal time to repeat pulmonary rehabilitation.
Introduction
The benefits of pulmonary rehabilitation for people with chronic obstructive pulmonary disease (COPD) have been well-documented. 1 Pulmonary rehabilitation is an episodic intervention, with intense periods of supervision followed by unsupervised exercise training and a reliance on self-management. 2 Many people with COPD undertake pulmonary rehabilitation more than once, with a retrospective study suggesting that 20% will repeat within the first 2 years after program completion. 3 The reasons for repeating pulmonary rehabilitation have not been examined. A small number of studies suggest that repeating is pulmonary rehabilitation beneficial; however, due to the limited number of participants in these studies, it is not clear whether the benefits are as great as for the first program. 4 –8 Previous studies examined repeating pulmonary rehabilitation after a time period of 6 months, 12 months, and 2 years, 7,8 with one study randomizing patients into a modified 3-week program after an exacerbation within 12 months of their initial pulmonary rehabilitation program. 5 None of these time points are clearly superior and the ideal timing for repeating pulmonary rehabilitation has not been defined. Guidelines for pulmonary rehabilitation suggest that patients could repeat pulmonary rehabilitation after 1 year, but this is based on expert opinion, and the authors acknowledge that timing may be influenced by the aim of re-referral. 9 Little is known as to why health professionals re-refer patients to pulmonary rehabilitation or patient experiences of repeating the program.
The aim of this study was to better understand health professionals’ reasoning for referring people with COPD to repeat pulmonary rehabilitation and to appreciate the experiences of repeating pulmonary rehabilitation for people with COPD. This information may assist in identifying the role of repeat pulmonary rehabilitation programs and the optimal time to re-refer.
Methods
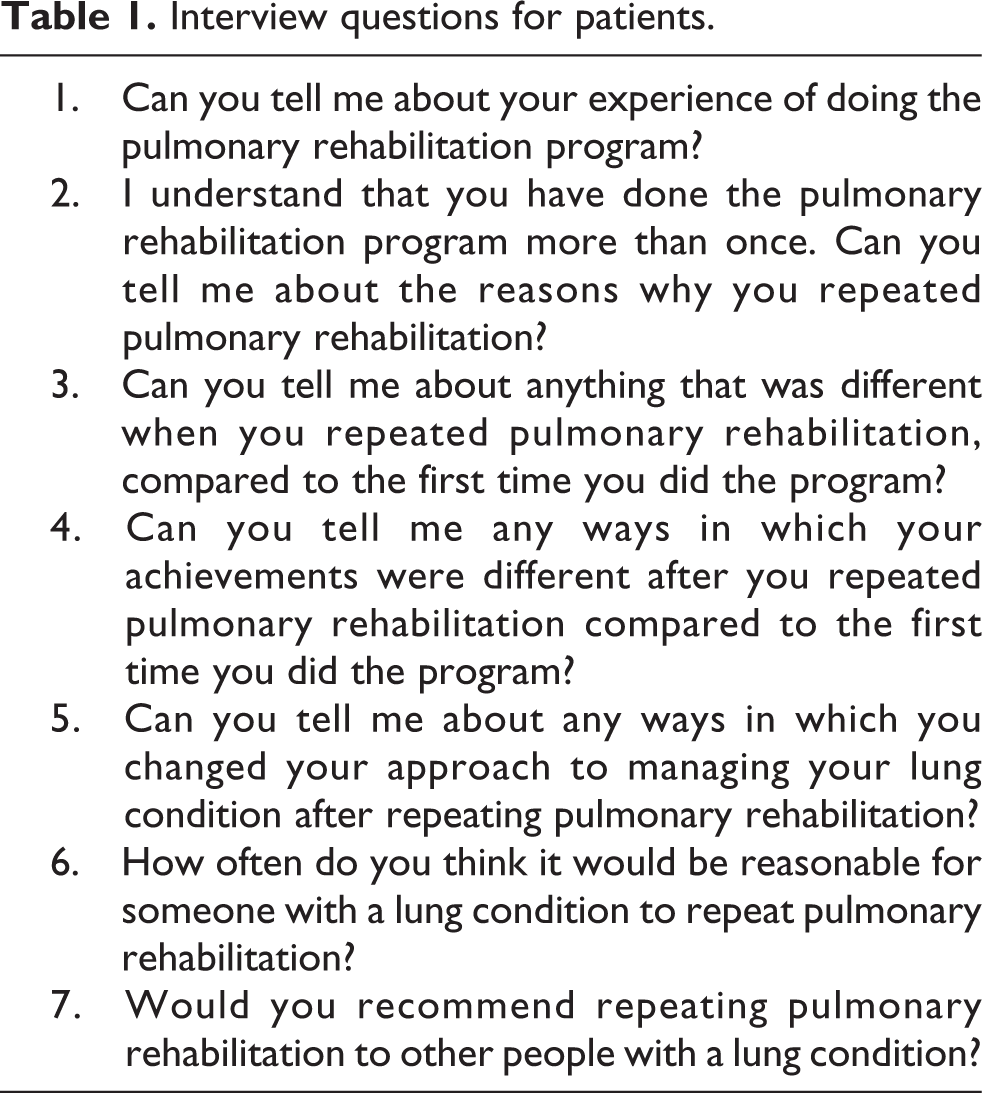
This qualitative study used semi-structured interviews with open-ended questions. Participants had a diagnosis of COPD confirmed on spirometry and had undertaken an outpatient pulmonary rehabilitation program at a tertiary hospital at least twice within the previous 18 months. They were identified from a database of patients who had undertaken pulmonary rehabilitation. Potential participants were sent a letter inviting them to contact the investigators if they were interested in taking part. Information gathered from the medical history included age, gender, comorbidities, spirometry, confirmation of participation in pulmonary rehabilitation, and outcomes of pulmonary rehabilitation including 6-minute walk distance (6MWD) before and after the programs. We also recruited health professionals caring for people with COPD at two teaching hospitals, one an inner metropolitan hospital and one in the outer metropolitan region. Health professionals were respiratory physicians, advanced medical trainees, physiotherapists, or nurses who had referred people with COPD to pulmonary rehabilitation. They were identified from staff lists at the participating hospitals and were invited to participate by e-mail. Participant interviews were conducted over the telephone or in person, according to the participant’s preference and were audio recorded for accuracy. Telephone interviews were chosen to minimize the barriers to participation for people with COPD, who may find it difficult to travel to the center for a face-to-face interview due to disabling symptoms. A series of open-ended questions were developed based on a review of the literature and the experience of the investigators (Tables 1 and 2). Interviews were conducted by one of the investigators (SS) who has a background in nursing and health services management. The study was approved by the Human Research Ethics Committees of Alfred Health, Peninsula Health, and La Trobe University, and informed consent was obtained from all participants.
Interview questions for patients.
Interview questions for health professionals.

Data analysis
Recordings were transcribed verbatim. Two researchers independently analyzed the data using deductive thematic analysis. 10 Line-by-line iterative thematic analysis took place with the development of descriptive codes to represent the data. Open coding commenced during the data collection and was used to compile a hierarchical coding scheme. Axial coding was then used to refine themes and understand the relationship of themes to subthemes. Finally, selective coding was used to understand the relationship between them. Discussion of themes took place until consensus was reached between the researchers. A third researcher provided peer debriefing. Additional strategies used to enhance the trustworthiness of data analysis were researcher memos, constant comparison to compare codes with newly transcribed data, diagramming to describe the relationship between themes, and documentation of theme naming. Quotations extracted from the transcripts provide supportive data. Data were analyzed separately for health professionals and patients. Data collection continued until saturation was reached in each group. 11
Results
Patient themes
Of the 29 eligible patients who were sent a letter of invitation, 14 patients were interviewed. Participants with COPD were aged 45–90 years and 50% were male. The majority had undertaken pulmonary rehabilitation more than twice (range 2–5 programs). Demographic characteristics are presented in Table 3. On average, interviews lasted 22 minutes. Data saturation was evident after 12 interviews. Themes that emerged from the interviews are listed in Table 4.
Demographics of patients.
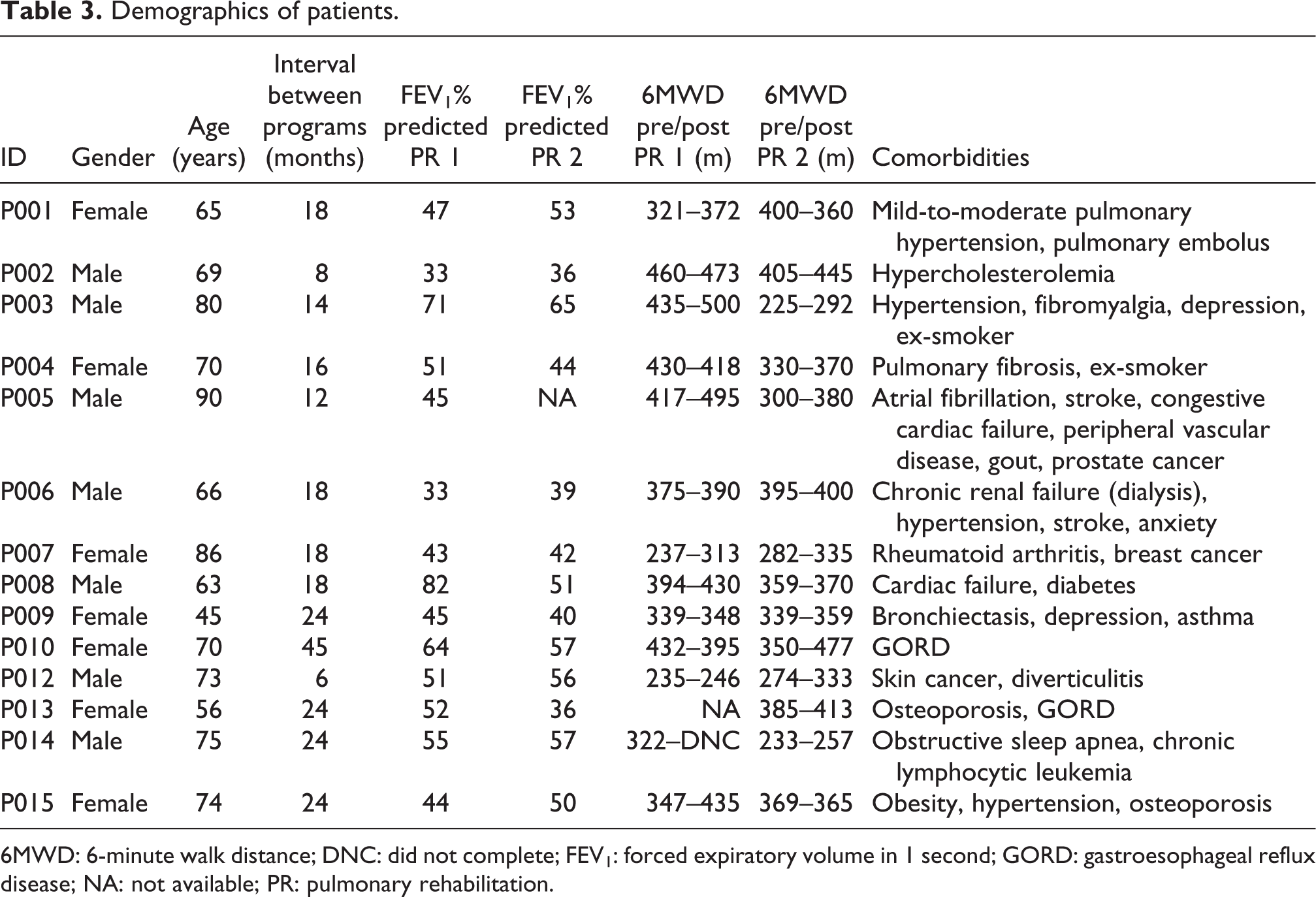
6MWD: 6-minute walk distance; DNC: did not complete; FEV1: forced expiratory volume in 1 second; GORD: gastroesophageal reflux disease; NA: not available; PR: pulmonary rehabilitation.
Themes from patient interviews.

Participants with COPD were all extremely positive about the benefits of pulmonary rehabilitation for their health. Some reported benefits included improved fitness, better breathing, greater confidence in their ability to undertake activities of daily living, weight loss, and increased motivation: P013: It’s a positive message that you are actually getting…I find physically and mentally the rehabilitation program is excellent.
External drivers to repeat pulmonary rehabilitation
Patients reported a variety of reasons for repeating pulmonary rehabilitation, most relating to external drivers rather than a personal motivation: P008: Yes I got sick and went back to hospital and I was referred back to do the program again because I was having problems with my mobility and my breathing capacity. P003: It was the lung specialist…probably because there has been some change in my condition. P003: …it may not be possible to restore the level of fitness that was there before, but to recoup some of the lost level of fitness due to my not having participated.
Diversity of experiences when repeating pulmonary rehabilitation
Some participants found no differences between the first and second rehabilitation programs. Others said it was easier the second time, primarily because they knew what to expect and were more confident. Another group of participants reported that repeating pulmonary rehabilitation meant confronting the deterioration in their health since the previous program, revealing a decline in their physical capacity. As a result, these participants had lowered their expectations of what they could achieve after repeating pulmonary rehabilitation: P014: I do notice a difference, they put me on oxygen now when I’m exercising, where as previously I wasn’t. P007: In myself I’m not as good as I used to be…I’ve gone downhill and I can’t expect to come back to where I was before unfortunately.
Other exercise programs are not the same as pulmonary rehabilitation
Many participants commented on the differences between the pulmonary rehabilitation program and other programs they had attended in the community. The differences included reduced frequency of community programs, lower intensity of exercise training, a smaller range of equipment, and less supervision: P008: I don’t think I get as much out of it (the community exercise program) but I’m doing it because I’m still struggling with my breathing. P012: …pulmonary rehab is specialised and it monitors you much more closely.
Benefits of repeating pulmonary rehabilitation are due to supervision
Nearly all of the participants discussed how much easier it was to maintain a meaningful exercise regimen when supervised. They were more motivated to exercise regularly, confident with being monitored during the sessions and found it a disciplined way of maintaining regular exercise: P006: Often I’d be at the pulmonary gym…I’d be on the treadmill thinking if I was at home I would have stopped now .…So it’s motivation to keep doing it. P008: …I find when I go walking if I have the dog it sort of gives me more purpose as well, it’s…easier to drag yourself out of the door.
Desire to undertake pulmonary rehabilitation more frequently than offered
Many participants wanted to undertake pulmonary rehabilitation more frequently than it had been offered to them, with some preferring continuous involvement: P012: I think you have to do it all the time…the only remedy for the condition is to have exercise and try to build up the lungs. P003: …I’m very conscious of the fact, there are (only) so many places available. I would not like to be taking the place of someone else whose needs are greater or equal to mine.
Health professionals
Fifteen health professionals were interviewed, from a total of 25 e-mail invitations sent. Participants comprised seven doctors, six physiotherapists, and two nurses. Two doctors were in their final year of specialist physician training and the remainder had between 5 and 18 years of experience as a respiratory physician. Physiotherapists and nurses had between 2 and 25 years of experience in delivering respiratory services, including two physiotherapists who led pulmonary rehabilitation programs. All had made referrals to pulmonary rehabilitation for patients with COPD. On average, interviews lasted 14 minutes. Data saturation was evident after 14 interviews. Themes are listed in Table 5.
Themes from health professional interviews.
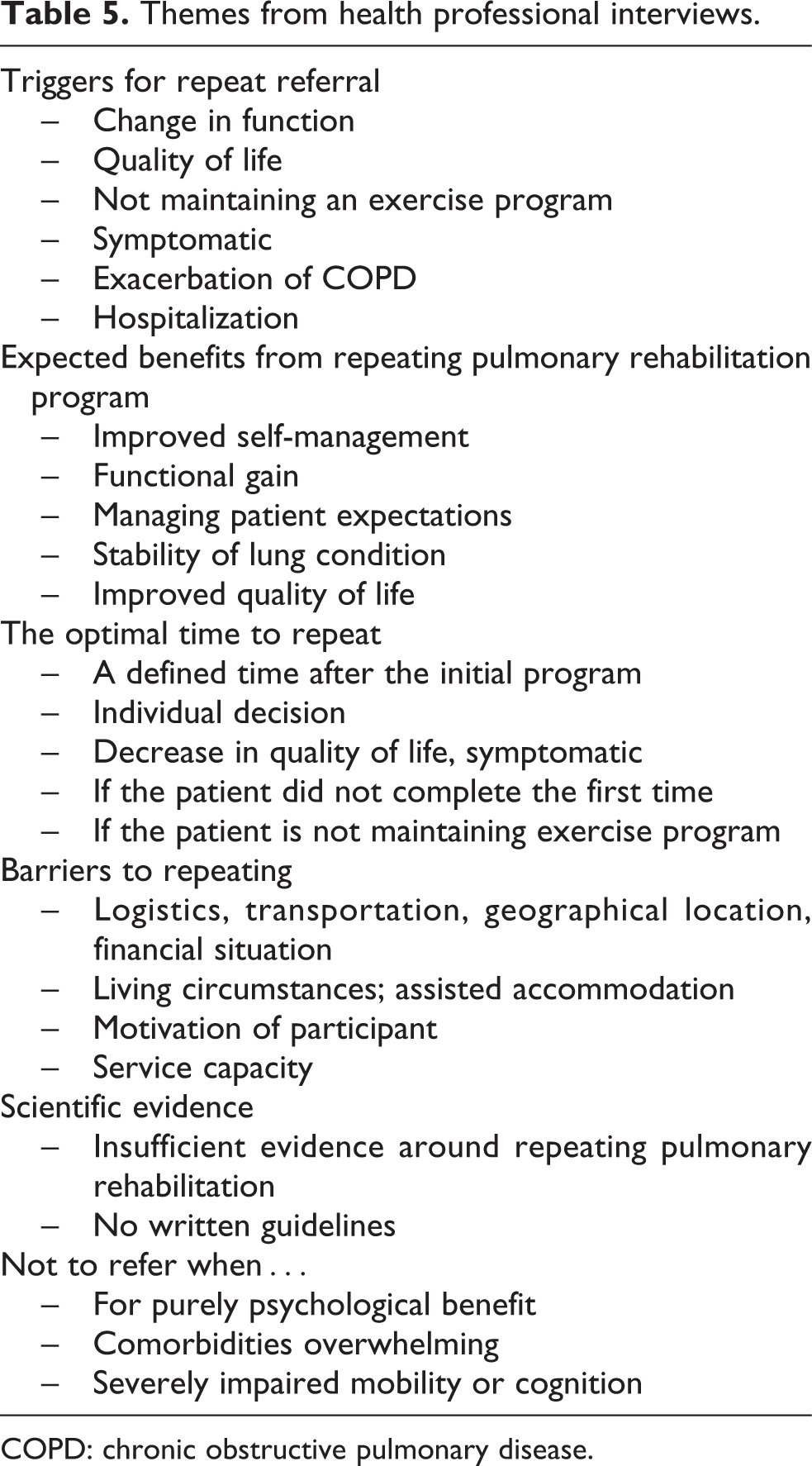
COPD: chronic obstructive pulmonary disease.
All health professionals strongly supported the role of pulmonary rehabilitation in the management of COPD. The top reasons for referring patients with COPD for their first program were upon diagnosis of COPD, symptoms of COPD impacting on their life, functional decline, and acute exacerbation of their lung condition. C011D: If they have significant functional limitations and if they’re interested in and willing to participate in a pulmonary rehab program.
Triggers for referral to repeat pulmonary rehabilitation
Health professionals re-referred patients with COPD to pulmonary rehabilitation when there was a change in their functional status or exercise capacity: C001P: …if they (patients) are able to articulate…a change from what they were capable of doing in the past then that’s often a motivating factor for people to come again. C012D: …if they…have noticed a decrease in their exercise tolerance and they are not on a structured exercise program. C012D: …if they have been in hospital…and they have become deconditioned, I probably would (refer to repeat).
Benefits from repeating pulmonary rehabilitation
Reengagement in pulmonary rehabilitation aimed to improve functional capacity and promote self-management, through the educational element of the program and by interaction with program staff. C003P: …the education that’s involved with pulmonary rehab is quite priceless in terms of their self-management; keeping them out of hospital for longer is a big benefit. C006 N: I think they are having like tune-ups…I think it could prevent the referral becoming urgent…. C004P: …the whole point of pulmonary rehab is we improve self-management and self-care at home. We don’t want to then become their sort of crutch to lean on as well.
Magnitude and nature of benefits from repeating pulmonary rehabilitation
There were varied expectations from the health professionals as to the likely outcomes and magnitude of benefit from repeating pulmonary rehabilitation. C001P: …thinking about what benefit someone will get you’re obviously hopeful that it will be what they had in the past but you’re…mindful of the fact that it’s a deteriorating lung condition. C010D: …this is probably fanciful but I think they would be similar (to the initial program)…Well, maybe I hope they would be similar. C004P: …they say, I didn’t do as well this time as I did before. But that said, I think they are still grateful for coming. I think they know their rate of decline probably would be rapider if they hadn’t come.
Determining the optimal time to repeat pulmonary rehabilitation
There was no agreement among the health professionals, irrespective of their profession, as to the optimal time for repeating pulmonary rehabilitation. Opinions varied from after 6 months to a year, definitely not within the year, consider re-referring after 1 year, to an annual referral if the patient has not been in a program for 4–5 years. C009D: Completely without any classification I think of it as an annual thing. C007P: No, every patient, person is totally different. Totally individual choice of the patient.
Patients should only be referred for repeating pulmonary rehabilitation if they are motivated to attend
The majority of health professionals considered patient motivation as a guide to whether they would re-refer to pulmonary rehabilitation: C008P: …Unless they are motivated it is actually very unlikely personally that I will re-refer.
Practical barriers to repeating pulmonary rehabilitation
Health professionals were very aware of the barriers to repeating pulmonary rehabilitation, which included transportation, finances, disability limiting travel, cognitive capacity, and language barriers: C011D: …often I think they find leaving the house difficult in terms of the physical aspects of transport. If they don’t drive a car and public transport is difficult for them then they are often very reluctant….
Insufficient scientific evidence regarding the benefits of repeating pulmonary rehabilitation
All health professionals were aware of literature supporting the value of pulmonary rehabilitation, but only a handful had any knowledge of the few papers focusing on repeating the program.
Discussion
This study has shown that patients with COPD experienced a wide variety of benefits from repeating pulmonary rehabilitation, many of which they attributed to the motivation and confidence they gained from exercising under supervision. However, the experience of repeating pulmonary rehabilitation was confronting for some in whom it revealed a physical deterioration since their last program. Most would have liked to repeat pulmonary rehabilitation more often than it was offered; however, they were mindful that it was a scarce resource. There was no agreement among health professionals regarding the optimal time or frequency for repeating pulmonary rehabilitation, with triggers for repeat referral including a reduction in functional capacity, failure to engage in a regular exercise program, and recent exacerbation or hospitalization. Health professionals were unsure about the expected gains from repeating pulmonary rehabilitation but emphasized the importance of patient motivation in the decision to re-refer.
Consistent with the variation in outcomes seen in quantitative studies, 4 –8 patients reported a variety of outcomes from repeating pulmonary rehabilitation. Some felt they attained similar benefits to the initial program and some found they gained more from the repeat program as they knew what to expect. Unexpectedly, some patients said that repeating pulmonary rehabilitation required them to confront the deterioration in their health. This has not previously been documented and did not emerge in our interviews with health professionals. Health professionals who run pulmonary rehabilitation should be aware of this common experience which may affect motivation and ability to engage with repeat programs. The referring health professionals also had a variety of expectations for the outcomes of repeat pulmonary rehabilitation and acknowledged that there was limited science to inform them on this topic.
Many patients reported that they had engaged in other exercise programs after completing pulmonary rehabilitation but were dissatisfied with their experiences due to differences in program content, format, and supervision. Many saw the supervision offered in a pulmonary rehabilitation program as a unique feature, providing confidence and motivation. Pulmonary rehabilitation is an episodic intervention, with intense periods of supervision, followed by unsupervised exercise training or a maintenance program with lower intensity of supervision. One of the goals of pulmonary rehabilitation is for patients to acquire the necessary skills to actively manage in their own care, achieving a degree of independence from health professionals. 2 This includes the maintenance of a personal activity program. However, our data suggest that many participants felt unable to sustain this over time. Health professionals also confirmed this pattern, with failure to maintain an exercise program being a major reason for re-referral. Recent data suggest that improvements in daily physical activity following pulmonary rehabilitation may be marginal, despite significant gains in exercise capacity, 12 suggesting that improved physical fitness does not necessarily translate to adoption of healthy behaviors. Repeating pulmonary rehabilitation may have an important “booster” role for physical health, motivation, and self-management skills. The cost-effectiveness of an approach to COPD care which involves regularly repeating pulmonary rehabilitation has not been investigated to date.
There was no agreement among health professionals regarding the best time to repeat pulmonary rehabilitation. Previous studies have shown that the benefits of pulmonary rehabilitation decline over the first year following program completion, with exercise capacity declining more rapidly than health-related quality of life. 2,7 Measures such as 6MWD may provide a useful clue as to when a repeat program should be offered to an individual. While previous studies of repeating pulmonary rehabilitation have trialed a number of time points, 7,8 it does not appear that any one approach is superior. However, the conclusions that can be drawn from previous studies are limited by low numbers of participants and, in some cases, uncontrolled designs.
The strengths of this study lie in the rich data extracted from the interview process. Health professionals were able to express their clinical reasoning regarding re-referral to pulmonary rehabilitation. We only interviewed patients who had repeated and did not obtain information from people with COPD who had declined to repeat; this is a limitation as the perspectives of those who choose not to repeat are not included and our participants may have been more positive about the benefits of repeating. All health professionals were recruited from teaching hospitals and were supportive of referral for repeat pulmonary rehabilitation. It is possible that their views and experiences do not reflect those of health professionals in other settings.
In conclusion, people with COPD value the opportunity to repeat pulmonary rehabilitation and gain confidence from a supervised program. There is no agreement among health professionals regarding the optimal time for repeating. Given the importance placed on repeating pulmonary rehabilitation by both patients and health professionals, future studies could investigate models of COPD care that involve regularly repeating pulmonary rehabilitation, including the cost-effectiveness of such an approach.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.