
Abstract
The objective of this study was to compare incremental shuttle walking test (ISWT) performance between South Asian and Caucasian British adults, identify predictors of ISWT distance and produce ethnicity-specific reference equations. Data from a mixed gender sample aged 40–75 years from Leicestershire, United Kingdom, were selected for analyses. Analysis of covariance determined differences in ISWT performance between South Asian and Caucasian British ethnic groups. Linear regressions identified predictors of ISWT distance, which determined the reference equations. In total, 144 participants took part in the study (79 South Asian (54 ± 8 years, 71% female) and 65 Caucasian British (58 ± 9 years, 74% female)). Distance walked for the ISWT was shorter for South Asian individuals compared with Caucasian British (451 ± 143 vs. 575 ± 180 m, p < 0.001). The ethnicity-specific reference equations for ISWT distance explained 33–50% of the variance (standard error of the estimate (SEE): 107–119 m) for South Asians and explained 14–58% of the variance (SEE: 121–169 m) for Caucasian British. Ethnicity univariately explained 12.9% of the variance in ISWT distance and was significantly associated with ISWT distance after controlling for age, gender, height, weight, dyspnoea and lung function (B = −70.37; 1 = Caucasian British, 2 = South Asian), uniquely explaining 3.7% of the variance. Predicted values for ISWT performance were lower in South Asian people than in Caucasian British. Ethnicity-specific reference equations should account for this.
Background
Exercise tests are commonly used in clinical practice for chronic disease management 1 and in research interventions targeting exercise capacity. 2 Field-based walking tests such as the incremental shuttle walking test (ISWT), 3 the endurance shuttle walking test 4 and the 6-minute walk test 5 are now commonplace outcome assessments for pulmonary and cardiac rehabilitation programmes. It is important to understand the factors that impact test performance to identify people with performance lower than predicted for their peer group. This may allow targeting of rehabilitation to groups with a specific deficit. Such information can be used to increase motivation and prescribe tailored workloads during rehabilitation. 6
To date, normative values for the ISWT have been provided on three continents: South America 7 ; Europe 6 and Asia. 8 Normative values are of great importance because they describe the natural history of clinical outcomes or conditions and help develop standards of care. 9 With societies around the world becoming increasingly ethnically diverse, a need to investigate differing populations has been advocated. 10 For example, reference standards produced for the 6-minute walk test across seven countries found large geographical variations in test performance despite following a standardised protocol. 11 To date, reference equations have been developed in ethnically homogenous populations. It is unknown whether ISWT performance differs between ethnic groups residing in the same region and what characteristics predict performance within healthy adults of a particular ethnicity. The present study was conducted in Leicestershire, United Kingdom, which has a large ethnic Indian population (4% in Leicestershire and 28% in Leicester city). 12
The aims of this study were to (i) investigate differences in ISWT performance between healthy Caucasian British and UK South Asians, (ii) identify predictors of ISWT performance and (iii) produce a reference equation accounting for South Asian ethnicity.
Materials and methods
Study participants
Data were obtained from the Physical Activity and Respiratory Health Study, a cross-sectional, observational study. 13 Participants attended a single study visit at the NIHR Leicester Biomedical Research Centre – Respiratory, Glenfield Hospital, Leicester, United Kingdom.
The inclusion criteria for the present study were ≥40 years of age, residing in Leicestershire and Rutland with no cognitive impairment. Inclusion criteria for the present study were as follows: no diagnosis of respiratory disease, normal airflow obstruction (forced expiratory volume in 1 second (FEV1)/forced vital capacity (FVC) ratio ≥ 0.70), being a never smoker (<100 cigarettes in their life), minimal functional limitations (modified Medical Research Council (mMRC) dyspnoea grade < 2) and the completion of two ISWTs. Healthy participants who selected themselves as Caucasian British or South Asian were included for this analysis. The sample consisted of both first- and second-generation South Asian participants. All participants gave their written informed consent, and all procedures were approved by the National Research Ethics Service Committee East Midlands Nottingham-2.
Incremental shuttle walk test
The ISWT is a symptom-limited test of exercise capacity requiring participants to walk up and down a 10-m course 3 supervised and instructed by a trained technician during the full assessments. Walking speed was externally paced using pre-recorded bleep signals. Walking pace for the test began at 0.5 m/s and increased by 0.17 m/s at the end of each minute (indicated by a triple bleep). The ISWT was terminated if participants reported symptoms (e.g. muscle pain or breathlessness), were unable to maintain the necessary pace, or completed the test (12 minutes, 1020 m). Participants were not permitted to run. The ISWT was repeated by the same operator following recovery with the best distance achieved used for analysis. Before the second ISWT, oxygen saturation and heart rate (Pulse Oximeter CMS50F; Contec, Qinhuangdao, China) were checked to ensure return to baseline. Rate of perceived exertion (RPE, 6–20), perceived dyspnoea (Borg breathlessness scale, 0–10) and heart rate were recorded immediately upon completion of the ISWT by the operator. Maximum predicted heart rate was calculated as 220 minus age in years. 14 No participants were taking β-blockers or other medications impacting heart rate.
Anthropometrics and body composition
Height, weight, body mass index (BMI) and waist circumference (average of two measures) were taken. Percentage body fat (% body fat; Tanita MC 780 MA, Tanita corporation, Tokyo, Japan) was measured using bioimpedence.
Respiratory health
Participants completed forced spirometry tests (MicroLab MK8 spirometer) conducted according to British Thoracic Society standards. 15 Lung function was examined using forced spirometry (ML3500 MicroLab MK8) with the best result from at least three valid efforts for absolute FEV1/FVC ratio carried forward. Self-reported breathlessness was obtained using the mMRC dyspnoea scale 16 with 0 equating to “Not troubled by breathlessness except on strenuous exercise” and 1 equating to “Shortness of breath when hurrying on the level or walking up a slight hill.”
Physical function
Quadriceps maximal voluntary contraction (QMVC) test was conducted requiring participants to sit in a purpose-built chair with an inextensible strap connecting the ankle of their dominant leg to a strain gauge (PR1 force transducer; HURLabs, Finland). Participants’ knees were flexed to 90°, and the strain gauge and couplings were aligned to ensure an isometric contraction. 17 Participants performed three sustained maximal isometric quadriceps contractions with 30- to 60-second rest between efforts.
Grip strength was assessed using a hand-held dynamometer (Takei analogue dynamometer, Takei scientific instruments co., Ltd, Niigata, Japan) for both dominant and non-dominant hands with three measures on each hand. Participants were asked to squeeze the dynamometer with as much force as possible, with their elbow extended down by their side. 18
Statistical analyses
Data were analysed using SPSS 23.0 for Windows (SPSS Inc., Chicago, Illinois, USA) with α set at 0.05. Independent t-tests and analysis of covariance (controlling for age and gender) were conducted to compare ethnic groups. χ 2 test was used to compare categorical data between ethnic groups. Enter linear regressions were performed to examine the relationship between variables and ISWT distance and to develop reference equations. Biethnic and ethnicity-specific reference equations were developed. Five regression models were generated to account for the availability of variables in routinely collected data: model 1 (most practicable): age and gender, model 2: with the addition of height and weight, model 3: with the addition of self-reported dyspnoea, model 4: with the addition of lung function and model 5 (least practicable): with the addition of body composition and physical function. All models were checked for linear relationship, absence of multicollinearity (variance inflation factor < 10 and tolerance > 0.10), 19,20 homoscedasticity and a normal distribution of residuals. Explained variance (R 2) and SEE were provided for all models.
Results
Participant characteristics
Sample characteristics are presented in Table 1. South Asians were younger, shorter, weighed less, had lower spirometry outputs and had lower physical function values than Caucasian British. After adjusting for age and gender, South Asians were also found to have a greater body fat percentage.
Participant characteristics stratified by ethnic group.a
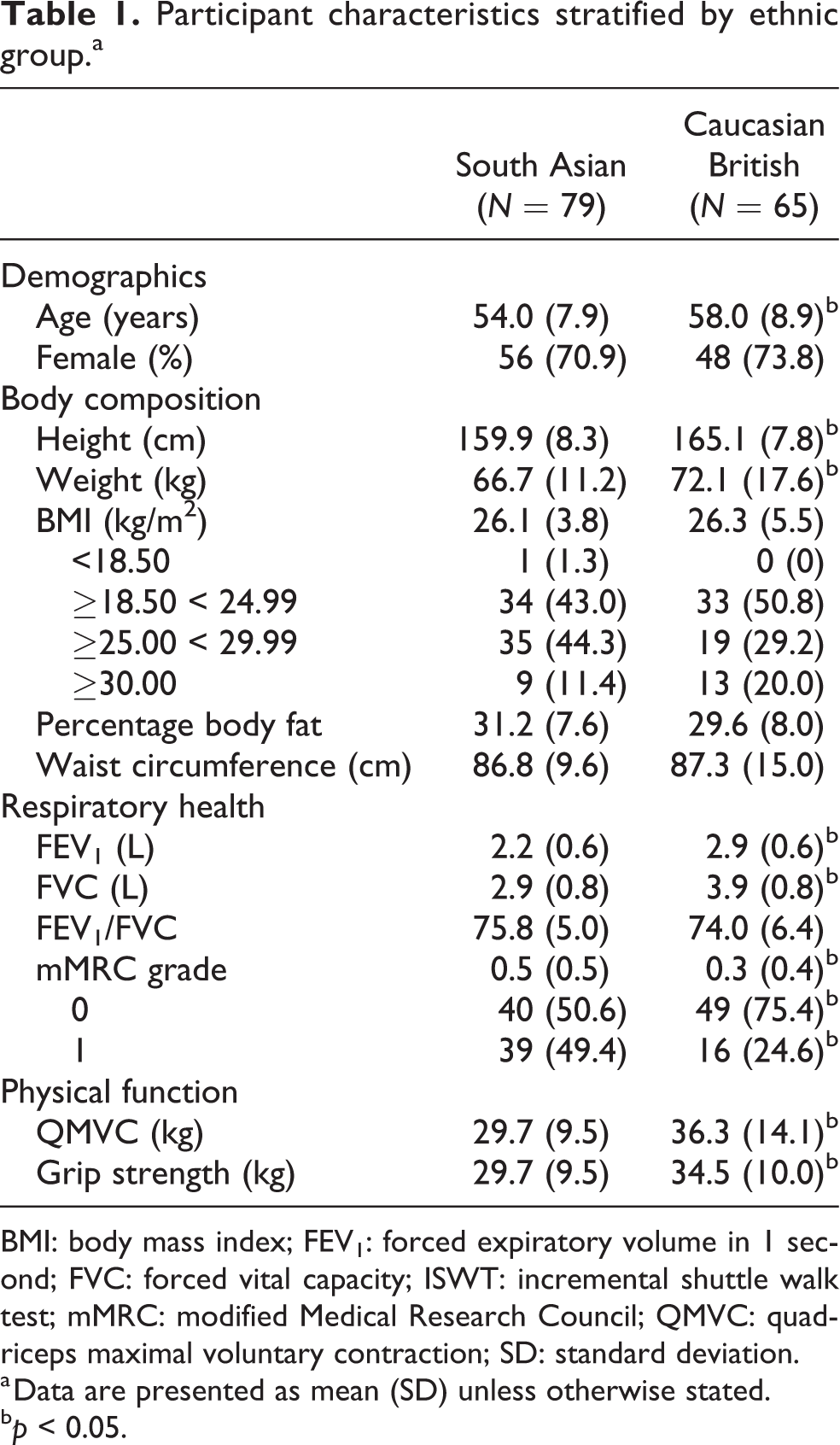
BMI: body mass index; FEV1: forced expiratory volume in 1 second; FVC: forced vital capacity; ISWT: incremental shuttle walk test; mMRC: modified Medical Research Council; QMVC: quadriceps maximal voluntary contraction; SD: standard deviation.
a Data are presented as mean (SD) unless otherwise stated.
b p < 0.05.
ISWT performance between ethnicities
A comparison of ISWT performance between South Asians and Caucasian British is presented in Table 2. South Asian adults achieved shorter ISWT distances (e.g. best ISWT distance 451 ± 143 vs. 575 ± 180 m, p < 0.001). South Asians had lower resting oxygen saturation, reached a lower percentage of maximum heart rate and reported a lower RPE and Borg for both tests. Differences in ISWT performance remained significant after controlling for age and gender.
Incremental shuttle walk test performance stratified by ethnic group.a

ISWT: incremental shuttle walk test; RPE: rate of perceived exertion; SD: standard deviation.
a Data are presented as mean (SD).
b p < 0.05.
For South Asians, 66 (83.5%) walked a greater distance on the second ISWT, six (7.6%) on the first ISWT and seven (8.9%) performing equally on both tests. For Caucasian British, 43 (66.2%) walked a greater distance on the second ISWT, 11 (16.9%) on the first ISWT and 11 (16.9%) performing equally on both tests.
Univariate analysis of factors influencing ISWT performance
Table 3 provides univariate associations for ISWT distance. Ethnicity (being South Asian) was negatively associated with ISWT distance. Height, FEV1, FVC, QMVC and grip strength were positively associated and % body fat and mMRC were negatively associated with ISWT distance across ethnicities and for the whole sample. Gender (being male) was significantly positively associated with ISWT distance for the whole sample, and South Asians and age was significantly negatively associated for both ethnic groups.
Univariate predictors of incremental shuttle walk test distance for the whole sample, South Asians and Caucasian British.

FEV1: forced expiratory volume in 1 second; FVC: forced vital capacity; mMRC: modified Medical Research Council; QMVC: quadriceps maximal voluntary contraction.
a Ethnicity (1 = Caucasian British; 2 = South Asian).
b Gender (0 = female; 1 = male).
Bold signifies p < 0.05.
Ethnicity as an independent predictor of ISWT distance
Table 4 provides whole sample (biethnic) prediction equations for ISWT distance. Ethnicity (being South Asian) was associated with ISWT distance after controlling for age, gender, height, weight, mMRC and FEV1 (models 1–4). Ethnicity was no longer significantly associated with ISWT in model 5 (additionally controlling for % body fat, grip strength and QMVC). Ethnicity uniquely explained 20.4%, 16.5%, 13.6% and 3.7% for models 1–4, respectively.
Multivariate regression models to examine the independent association of ethnicity with incremental shuttle walk test distance.

FEV1: forced expiratory volume in 1 second; mMRC: modified Medical Research Council; QMVC: quadriceps maximal voluntary contraction; SEE, standard error of the estimate.
a Gender (0 = female; 1 = male).
Ethnicity-specific reference equations
South Asian– and Caucasian British–specific reference equations for ISWT distance are shown in Table 5. For South Asians, model 1 (age and gender) explained 32.8% of the variance, rising by 7.8% with the addition of height, weight, mMRC and FEV1 (model 4). Model 5 (addition of % body fat, grip strength and QMVC) was able to account for 50.4% of the variance. For Caucasian British, model 1 explained a smaller proportion of the variance compared with South Asians (14.4%). The addition of height and weight (model 2) provided 27.1% of additional explained variance. Model 5 accounted for 57.6% of variance in ISWT distance.
Multivariate regression models to predict incremental shuttle walk test distance, stratified by ethnic group.
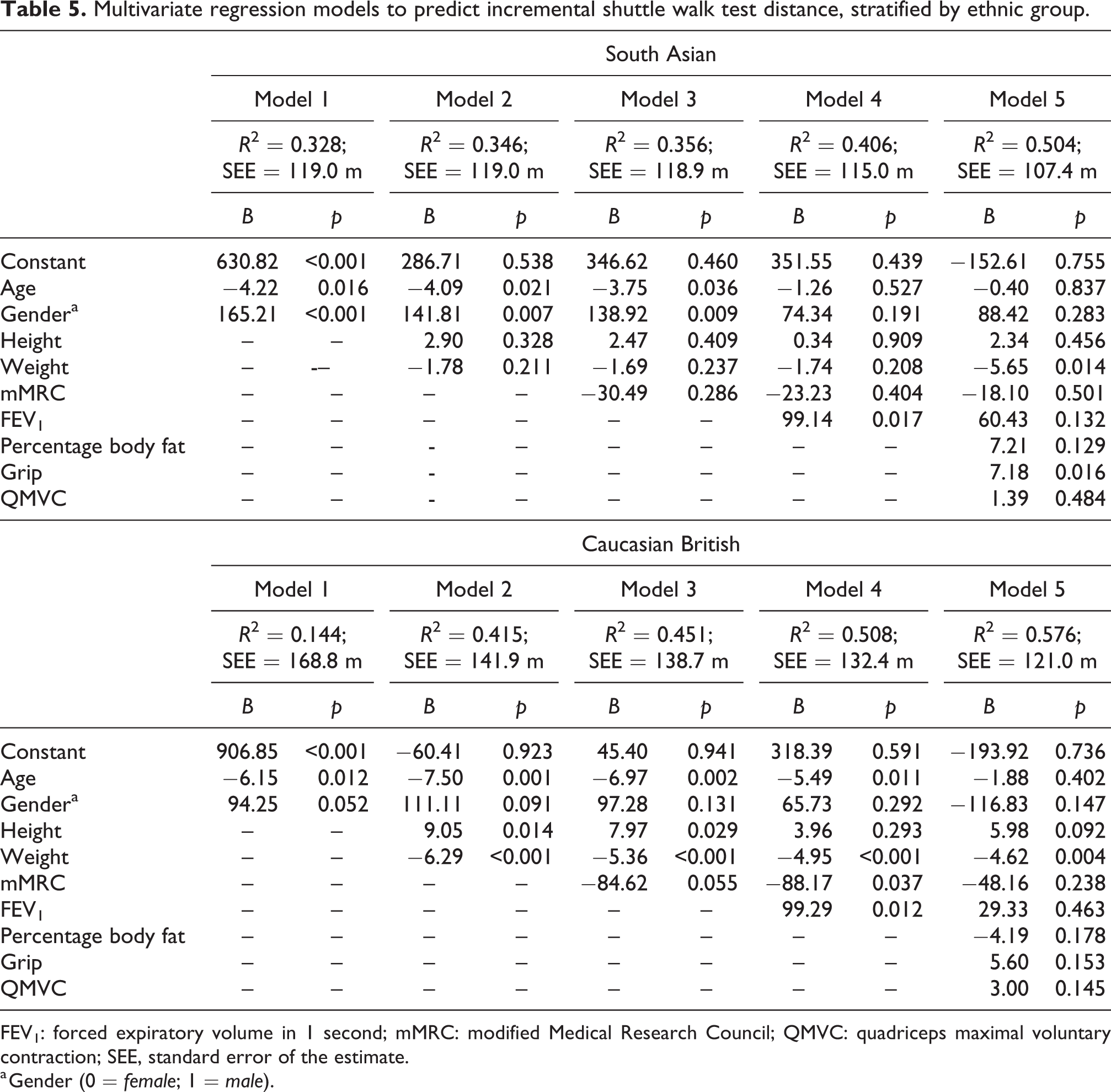
FEV1: forced expiratory volume in 1 second; mMRC: modified Medical Research Council; QMVC: quadriceps maximal voluntary contraction; SEE, standard error of the estimate.
a Gender (0 = female; 1 = male).
Physiological responses and ISWT distance
Percentage heart rate maximum (%HRmax), RPE and Borg may be indicative of the level of effort from participants. Therefore, the univariate relationship between these factors and ISWT distance was assessed. %HRmax (B = 3.38–3.61, p < 0.001), RPE (B = 25.22–28.71, p < 0.001) and Borg (B = 43.74–51.71, p < 0.001) were associated with ISWT distance for each ISWT test in the whole sample. %HRmax was associated with ISWT distance for South Asians (B = 4.95–5.36, p < 0.001), but not for Caucasian British. RPE was associated with ISWT distance for Caucasian British (B = 36.35–38.12, p < 0.001), but not for South Asians. Borg was associated with ISWT distance for the second test for Caucasian British and South Asian ethnic groups (B = 45.20, p < 0.001; and B = 41.34, p = 0.004, respectively), but only for Caucasian British for the first ISWT test (B = 53.25, p < 0.001).
Discussion
The present study found that predicted values for ISWT performance were lower in healthy South Asian individuals than in healthy Caucasian British individuals, with ethnicity shown to be significantly and independently associated with ISWT distance after controlling for confounders. These results support the need for ethnicity-specific reference equations for the ISWT in order to more accurately evaluate patient performance in clinical practice.
The independent contribution of ethnicity and shorter distance achieved by South Asians supports the need for individual assessment of the ISWT in relation to what would be expected for their ethnicity. Although South Asians have a lower prevalence of COPD in those aged ≥35 years compared with Caucasian British (1.3 vs. 4.4%) 21 ; evidence suggests that there is also disparity within COPD management and prognosis between ethnicities. 21 Despite reporting less severe symptomatic breathlessness, 21 South Asian individuals with COPD have been found to have higher rates of hospital admission 22 and are less often referred to pulmonary rehabilitation when compared with Caucasian British patients in the United Kingdom. 21 Providing feedback to patients on their exercise capacity using ethnicity-specific reference equations may help increase or maintain motivation during pulmonary rehabilitation as goal setting would be more suitably tailored. Moreover, highlighting the shorter ISWT distance walked by South Asian individuals may motivate more clinicians to refer these individuals with chronic respiratory disease to pulmonary rehabilitation.
The shorter distances walked by South Asian adults may not solely be due to physical characteristics. It has been suggested that factors such as cultural aspects relating to mood, attitude and motivation of participants may contribute to variances in field test performances. 11 With both ethnic groups reporting similar RPEs (11–12; “light”), South Asian individuals reached lower %HRmax and lower Borg scores compared with Caucasian British individuals, which suggests that cultural differences in effort perception may exist. Additionally, participants did not reach near maximum heart rates, indicating that thresholds for stopping the ISWT may be lower for South Asian adults compared with Caucasian British. Ethnic differences in gait velocity may partly account for these differences. For example, African Americans have been found to have 7.79 cm/s slower gait velocity than White Americans after accounting for factors such as age, BMI and pain levels. 23 However, neither South Asians nor Caucasian British performed truly maximal tests. This suggests that effort may be overestimated by adults independent of ethnicity. This is supported by Canning et al. 24 who found that adults were not able to match perceived and physiological walking/jogging intensities (light, moderate and vigorous effort) independent of gender, BMI and ethnicity (White versus non-White (including South Asians)).
Distances covered during the ISWT in the present UK sample were lower than that of other findings. 6,8 For both ethnic groups, greater coaching may have facilitated better performances, particularly for apparently healthy individuals who may not perceive a walking-based test to be maximal. Currently, the ISWT pre-recorded instructions are only available in English, so translators may be required to adequately explain the test to individuals who do not have English as their first language. It is unknown how %HRmax values compared against UK participants from the study by Harrson et al. 6 as this was not reported. However, %HRmax levels of the present study were similar to those observed in South American 7 and Indian 8 populations. Additionally, with 84% of South Asians achieving a greater distance on the second test (66% for Caucasian British), further improvement may have occurred with a third ISWT, a notion also highlighted by Probst et al. 25 Given not all participants had English as their first language, the additional challenges of instructing and motivating participants may have contributed to the lower %HRmax values. Additionally, interpretation of RPE and Borg scales may also have been impacted by language barriers.
The present study identified a range of factors univariately associated with ISWT performance, including body composition (e.g. BMI), dyspnoea (mMRC score), physical function (e.g. grip strength) and lung function (e.g. FEV1,). Despite this, only 50% (South Asian) and 58% (Caucasian British) of the variance was explained by these variables in the reference equation models. The prediction equations of Probst et al. 25 and Agarwal et al. 8 accounted for a greater proportion of the variance (71% and 68%, respectively) than those of the present study and Harrison et al. 6 (50.4%) despite only incorporating age and gender 8 and BMI 25 into the multivariate models. The use of the modified ISWT by Probst et al., 25 which adds three more levels (420 m) to the original ISWT, 3 may have eliminated the ceiling effect observed for participants who completed the test.
Limitations of the present study must be considered when interpreting the findings. It was not possible to differentiate between first- and second-generation South Asian individuals in the analyses. As individuals with different background ethnicities become increasingly integrated in UK society, it would be beneficial for future work to explore whether cultural assimilation and epigenetic factors that change over time will impact the role of ethnicity-specific reference equations through evolutionary convergence. Participants were encouraged, but not required, to wear flat shoes and light-weight, attire which may have influenced performance. As the ISWT was the last of a large battery of physical measures conducted, the ordering of measures and possible participant fatigue (both mental and physical) may have been limiting factors in overall ISWT performance.
Conclusion
The present study found that predicted values for ISWT performance were lower in South Asian adults than in Caucasian British; with ethnicity shown to be independently associated with ISWT distance. Cultural differences in effort perception may also exist. Prospective studies with larger sample sizes are required to further the development of ethnicity-specific reference equations in the context of evolutionary convergence. The array of influencing factors and range of explained variances from the present study and existing research suggest that deriving reference equations for the ISWT is challenging and may be influenced too much by the heterogeneity of sample characteristics, motivation and cultural norms. Ethnicity-specific reference equations are recommended for a more accurate evaluation of ISWT performance in clinical practice.
Footnotes
Authors' note
Ethnicity independently predicts ISWT performance in healthy UK adults.
Acknowledgements
The authors thank Theresa Harvey-Dunstan, Centre for Exercise and Rehabilitation Sciences, National Institute for Health Research (NIHR) Leicester Biomedical Research Centre - Respiratory, United Kingdom, for conducting ISWT training and assessing operator competency before the study commencement. The authors acknowledge support from the NIHR Leicester Biomedical Research Centre, which is a partnership between University Hospitals of Leicester National Health Service (NHS) Trust, Loughborough University and the University of Leicester, and also acknowledge support from the NIHR Collaboration for Leadership in Applied Health Research and Care – East Midlands and the Primary Care Research Network. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR, Loughborough University or the Department of Health.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by NHS England.