
Abstract
The use of different 6-min walk distance (6MWD) reference equations probably results in different predicted 6MWD reference values. We wished to investigate the impact of several 6MWD reference equations for adults in patients with chronic obstructive pulmonary disease (COPD) and factors accountable for different 6MWD% predicted values. Twenty-two 6MWD reference equations were applied to a data set of 2757 patients with COPD. The predicted 6MWD reference value of Troosters and colleagues was used as the point of reference. Four out of 21 remaining equations resulted in comparable 6MWD% predicted, 16 equations resulted in significantly higher 6MWD% predicted and 1 equation resulted in a significantly lower 6MWD% predicted. Similar differences in 6MWD% predicted were observed after stratification by sex. Body mass index and global initiative for chronic obstructive lung disease (GOLD) stage classification demonstrated varying results within and between the groups; 9 out of 21 equations resulted in comparable 6MWD% predicted in underweight patients but only 1 equation demonstrated comparable result in obese. Eight equations in GOLD I, whilst 5 out of 21 equations in GOLD IV resulted in comparable 6MWD% predicted. Existing 6MWD reference equations will give varying results. The choice of 6MWD reference equation should consider the consistency of 6-min walk test operating procedures and at least be specific for the country/region of origin.
Introduction
The 6-minute walk test (6MWT) can be used to assess functional exercise capacity, treatment efficacy and prognosis in chronic respiratory disease. 1 –4 New insights of chronic obstructive pulmonary disease (COPD) affliction, which include cardiac and peripheral muscle wasting effects, provide an additional value in the assessment of functional exercise capacity measured by the 6MWT. 5 The 6MWT elicit high but submaximal cardiorespiratory responses that mimic day life activities. 6 In some clinical situations, the 6-min walking distance (6MWD) may be a better index of actual patients’ ability to perform daily activities in comparison with the peak oxygen uptake. 7,8 The 6MWD has been indicated for the prediction of hospitalization and mortality in COPD 9 and has been also recognized for its predictive value to post-operative outcome in candidates for volume reduction surgery. 10
Multiple 6MWD reference equations 11 – 30 were derived to express the 6MWD as a percentage of these reference values (% predicted) (see Supplementary Table 1 for details). Adjusting the measured 6MWD for physiological variation using the percentage of walk predicted facilitates the interpretation of the walked 6MWD and helps to estimate the degree of exercise tolerance in patients. 31 Erroneous selection of a reference equation may result in misinterpretation of the levels of exercise capacity or improvements of physical performance after participation in pulmonary rehabilitation programmes. 30 The large number of published 6MWD reference equations and the fact that those equations are derived from healthy individuals with different clinical characteristics and do not consistently employ the same variables make the choice of 6MWD reference equation often vague.
Several demographic, anthropometric and physiological characteristics can determine the 6MWD in healthy individuals and in patients with COPD. 32 However, the strongest determinants that can independently affect the 6MWD in healthy adults seem to be the age, height, weight, sex and race and these characteristics have been proposed for clinical use. 15,18,26,33 Muscle strength, true leg length, symptoms of depression, health-related quality of life impairment and other factors such as the standardization of the 6MWT can influence the 6MWD. 11,34 –37 Therefore, it might be anticipated that the use of different 6MWD reference equations derived by several studies would result in different predicted 6MWD reference values.
Herein, we report a retrospective analysis in a large cohort of patients with COPD who were evaluated at CIRO+ between 1 January 2005 and 1 July 2013. 38 We assessed the impact of 22 existing 6MWD reference equations in patients with COPD and investigated the factors accountable for different predicted 6MWD reference values using data from 2757 patients with COPD. Furthermore, we wished to identify criteria for the choice of 6MWD reference equation in COPD patients.
Methods
A data set of patients with COPD
39
including demographic, anthropometric characteristics, lung function evaluation and 6MWT exercise outcomes was analysed. All patients performed two 6MWTs according to the American Thoracic Society guidelines,
7
including a practice walk.
40
The 6MWT with the highest 6MWD was used for further analyses.
41
During the 6MWTs, transcutaneous oxyhaemoglobin saturation (SpO2%) and heart rate (HR) were measured using a pulse oximeter (Nonin 2500; Nonin Medical Inc., Plymouth, Massachusetts, USA). The predicted maximum HR (HRmax, %) was derived from the formula
The 6MWD% Troosters et al. 26 was used as a point of reference. These reference values were used in CIRO+ since the last decade, as these reference values were derived from a Belgian sample of healthy elderly subjects with a mean 6MWD of 622 ± 75 m, which is comparable to the mean 6MWD of Dutch healthy elderly subjects. 43 All available 6MWD reference equations were applied with the exception of the alternative equation of Dourado et al., 24 which required handgrip strength measurement not available in our data set. All statistical analyses were carried out using SigmaPlot Version 11 and Statistical Package for the Social Sciences Version 19.0. Data are presented as mean (±SD) or proportion, as appropriate. For parametric data, comparisons were made using a two-tailed unpaired t-test. The 6MWD% predicted by Troosters et al. 26 was compared with the other reference values using Dunnett’s multiple comparisons test. A priori, a two-sided level of significance was set at p value of <0.05.
Results
A total of 22 reference equations were applied to a data set of 2757 patients with COPD (age range: 38–92 years). Reference equations encompassed race/ethnic differences and variety of technical aspects that can determine the 6MWD (see Supplementary Figure 1 and Table 2). The clinical features of patients are summarized in Table 1. In brief, patients generally had moderate to very severe COPD and an impaired lung diffusion capacity for carbon monoxide (DLCO). Men were slightly older compared with women and had more impaired Tiffeneau index and lower total lung capacity, whilst women had worse DLCO%. On average, the functional exercise capacity was profoundly limited: 422 ± 124 m, which equals 68 ± 18% of the reference values of Troosters et al. 26 (Table 1). Four out of 21 remaining equations resulted in comparable 6MWD% predicted; 16 equations resulted in significantly higher 6MWD% predicted (all p < 0.05); and 1 equation resulted in a significantly lower 6MWD% predicted (p < 0.001) (Figure 1). Similar discrepancies in the 6MWD% predicted among the equations were observed in patients stratified by sex (Figure 2).
Anthropometric and clinical characteristics of patients with COPD.a
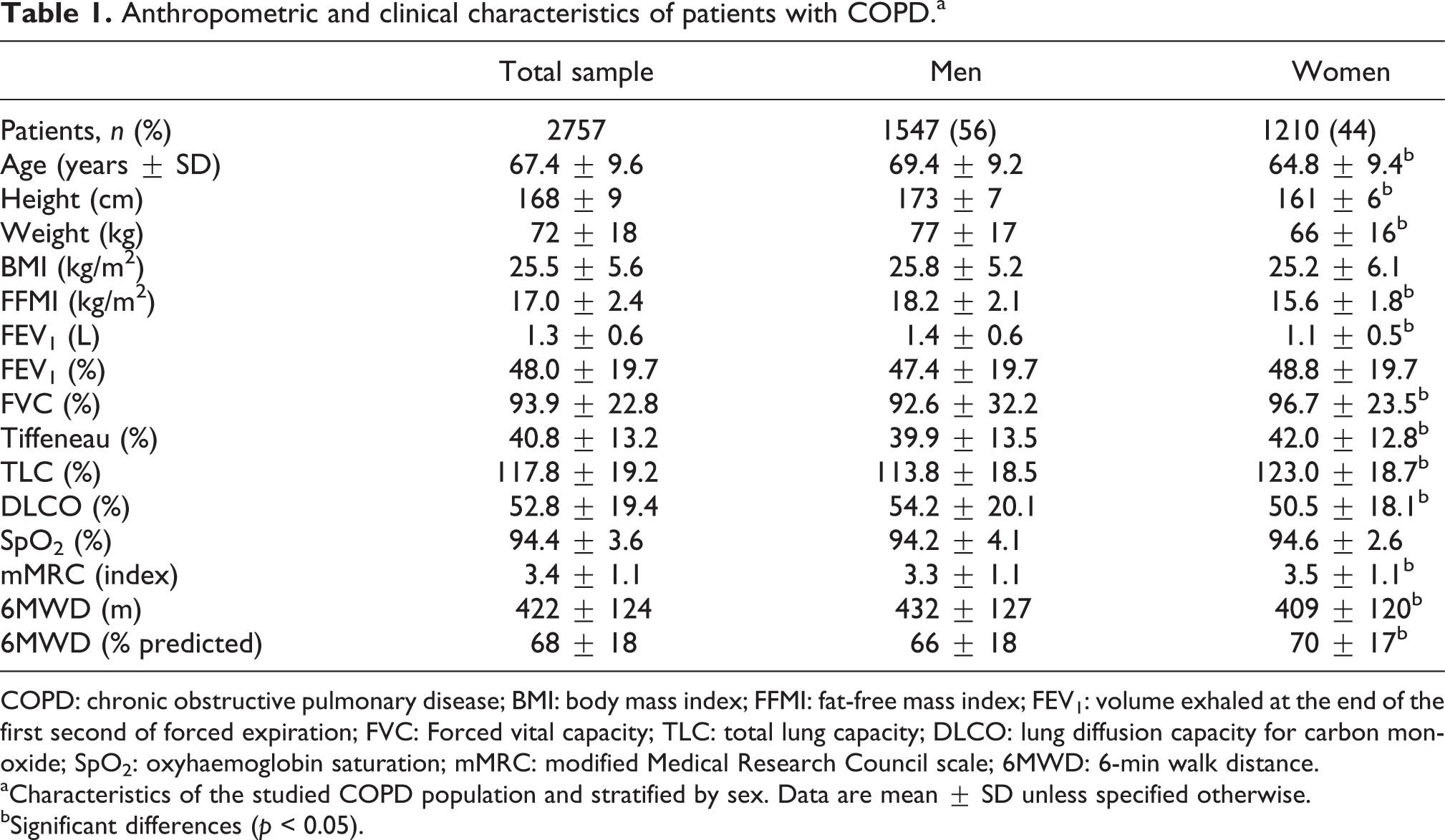
COPD: chronic obstructive pulmonary disease; BMI: body mass index; FFMI: fat-free mass index; FEV1: volume exhaled at the end of the first second of forced expiration; FVC: Forced vital capacity; TLC: total lung capacity; DLCO: lung diffusion capacity for carbon monoxide; SpO2: oxyhaemoglobin saturation; mMRC: modified Medical Research Council scale; 6MWD: 6-min walk distance.
aCharacteristics of the studied COPD population and stratified by sex. Data are mean ± SD unless specified otherwise.
bSignificant differences (p < 0.05).

The frequency distribution of estimated 6MWD applying the existing equation of healthy individuals to patients with COPD, demonstrated large variation. The numbers on the right are mean values per equation. 6MWD: 6-min walk distance; COPD: chronic obstructive pulmonary disease.
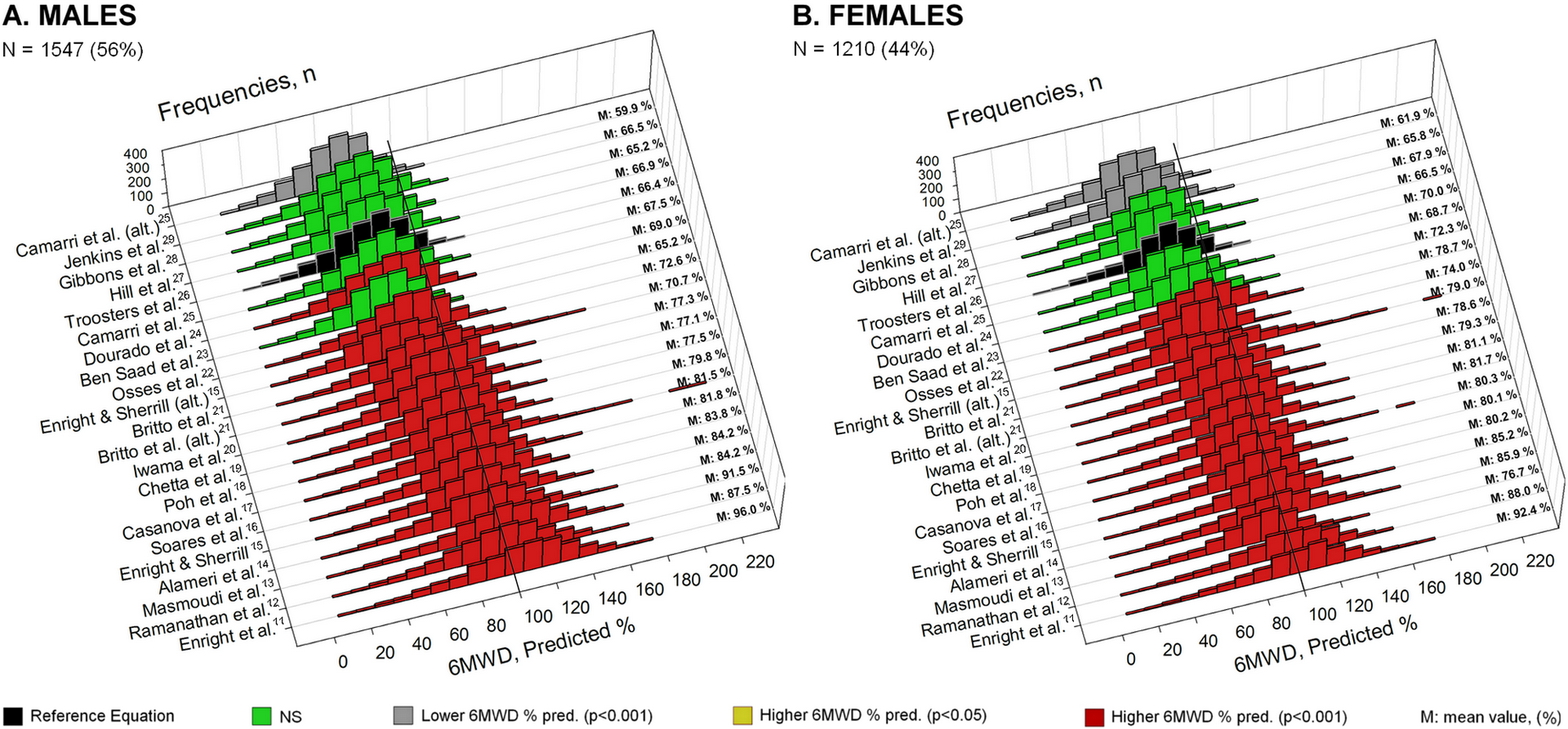
The frequency distribution of estimated 6MWD, applying reference equations of healthy individuals to patients with COPD, demonstrated similar impact after stratification by sex. The numbers on the right are mean values per equation. 6MWD: 6-min walk distance; COPD: chronic obstructive pulmonary disease.
Discrepancies between 6MWD expressed as % predicted of the reference values of Troosters et al. and the 6MWD expressed as % predicted using the remaining reference equations were also observed after stratification by body mass index (BMI) and the degree of airflow limitation as given by global initiative for chronic obstructive lung disease (GOLD) stages within all groups of patients. Furthermore, differences in the number of 6MWD predicted values with clinically important discrepancies were noticed between the BMI and between the GOLD stages groups. Patients with underweight BMI compared those with obese BMI and patients in GOLD stage I compared those in GOLD stage IV had a smaller number of discrepant 6MWD% predicted values (Figures 3 and 4).

The frequency distribution of estimated 6MWD, applying reference equations of healthy individuals to patients with COPD, demonstrated less differences in patients with underweight BMI compared with those with normal range or higher BMI. The numbers on the right are mean values per equation. 6MWD: 6-min walk distance; COPD: chronic obstructive pulmonary disease; BMI: body mass index.
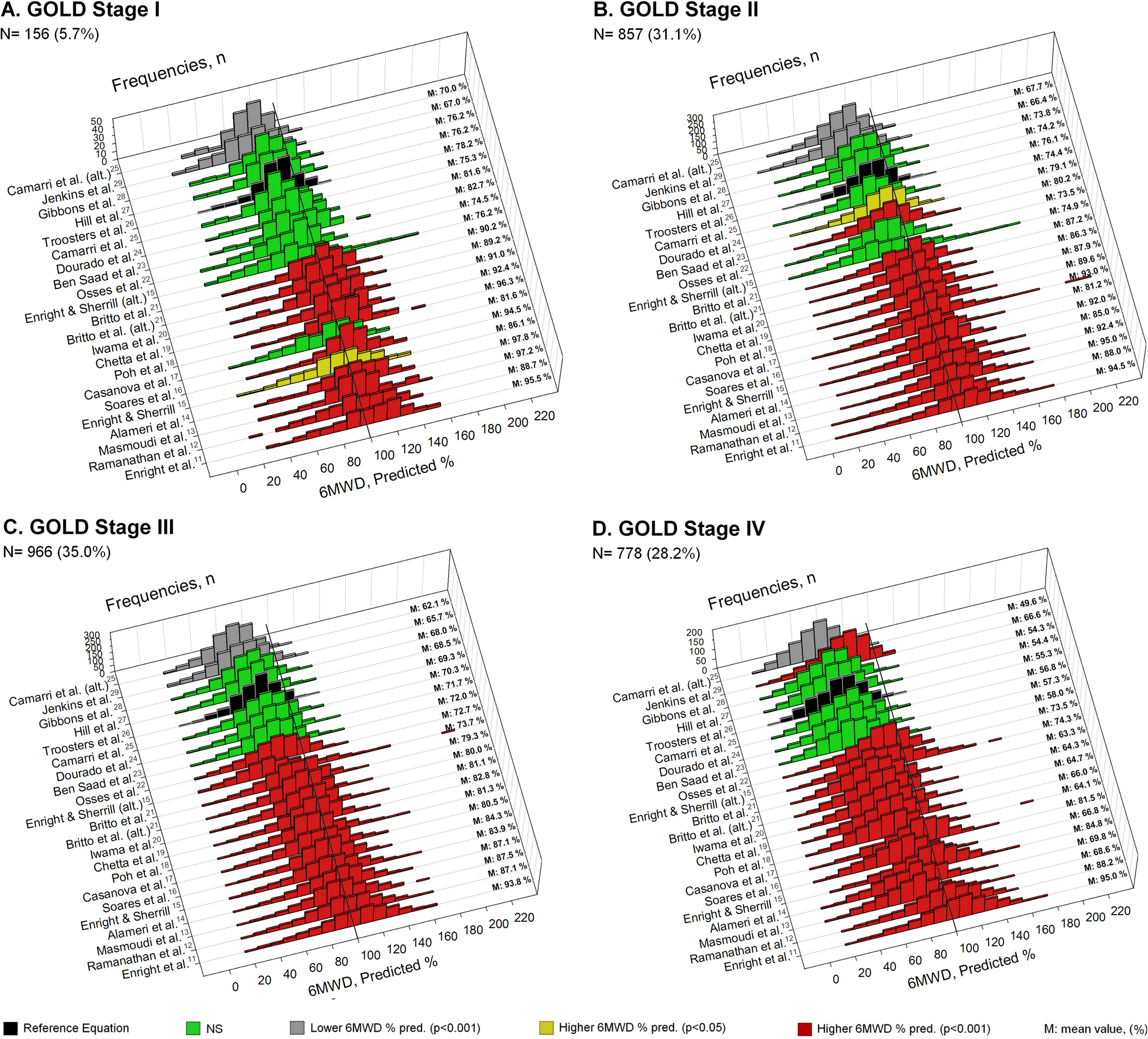
The frequency distribution of estimated 6MWD, applying the reference equations of healthy individuals to patients with COPD, demonstrated less differences in GOLD stage I across the progress of disease severity. The numbers on the right are mean values per equation. 6MWD: 6-min walk distance; COPD: chronic obstructive pulmonary disease; GOLD: global initiative for chronic obstructive lung disease.
Discussion
Even though a majority of the existing 6MWD reference equations included similar characteristics, such as sex, age, height, weight or BMI, clear differences were found when applying the existing 6MWD reference equations to a data set of 2757 patients with COPD (Figure 1). The best choice for the predicted 6MWD reference values probably depends on the country/region of origin of the healthy subjects that were used to develop the 6MWD reference equation. For example, the 6MWD reference equation of Poh et al. 18 resulted in a mean 6MWD of 81% predicted. This suggests that applying Asian-derived 6MWD% predicted values to Dutch patients with COPD may result in an overestimation of their true functional capacity. As pointed out by authors, one possible explanation for this discrepancy is the differences in body stature between Asians and Caucasian. Herein, it is worth noting that some countries and regions are very ethnically and racially diverse and reference values derived from mixed-race populations could be recommended. When we applied the reference equation of Enright et al., 11 which is derived from a mixed-race elderly group (aged: 77 ± 4years), true functional capacity of our patients seems to be overestimated compared with the rest of the reference values (Figure 1). We assume that it could be partly attributed both to their younger age and to racial differences.
Next to demographic characteristics, a different operating procedure of 6MWT can also affect on walking distance and modify the reference values. 4 For example, in the study of Troosters et al., 26 the length of the corridor of used reference equation was 50 m, which can be considered as a long corridor compared with 20 m corridor of Gibbons et al. 28 This fact can also result in overestimation of 6MWD% predicted relative to a number of other reference equations. Accordingly, our triangular track for the 6MWTs of our patients has the characteristics of a long corridor. Therefore, at CIRO+, the predicted reference values of Troosters et al. 26 are used, who studied healthy Belgians 50–85 years of age.
Methodological differences in the 6MWT, with track lengths ranging from 20 m to 50 m, the number of test repetitions ranging from 1 to 3, test-retest intervals from 30 min to 24 h and variable practices regarding the given test instructions (i.e. ‘walk at your own pace’ or ‘walk as far as you can’) and the encouragement, may partly account for the observed discrepancies in the 6MWD% predicted values. Sciurba et al. 44 demonstrated that the long compared with short corridors can increase the 6MWD as the number of turns is less and thus the physical effort is less. 44 In the study of Alameri et al., 14 healthy individuals reached a low average of HRmax (45% pred.) when instructed to walk at their own pace. 14 Moreover, the impact of a learning effect on the walking distance of 6MWT has been investigated in COPD. Steven et al. 45 performed three 6MWTs in 21 COPD patients on separate days and observed an average increase of 10% in the second test and an additional 3% increase in walking distance in the third test compared with first 6MWT. 45 Such factors are known to have an impact on the measured distance (see Supplementary Table 2).
The health status of the ‘healthy subjects’ may also have impacts on findings. For example, the study of Enright et al. 11 included participants with risk factors associated with cardiovascular disease with likely limitations in functional capacity probably resulting in an overestimation of the 6MWD% predicted when applied to individuals with COPD. The physical condition of the volunteers who participated at the several studies should be considered. The HR recorded at the end of the 6MWT can vary substantially in moderate and intense levels of effort in different studies. 15,25 These facts indicate that differences in characteristics of healthy population, 6MWT protocols and/or different levels of effort during the 6MWT can result in different 6MWD% predicted values.
On the other side, certain clinical characteristics of patients’ populations, where the equations are applied, can also be accountable for the discrepancies in the 6MWD% predicted values. After stratification for BMI and the degree of airflow limitation as given by GOLD stages, the number of discrepant 6MWD values varied between the groups of BMI and GOLD stages, respectively (Figures 3 and 4). Applying the 6MWD reference equations to underweight or GOLD stage I groups of patients leads to more consistent 6MWD% predicted values. Therefore, the choice of 6MWD reference equation in patients with those characteristics (underweight and/or GOLD stage I) may be of less importance. BMI and/or disease severity as given by GOLD stages are major determinants of exercise performance especially in individuals with higher BMI and/or worse COPD. The exclusion of these characteristics from reference equations could account for the discrepancies in 6MWD% predicted values and that can be more obvious in obese or patients with GOLD stage IV disease. This might explain the larger number of discrepant 6MWD% predicted values among the reference equations applied in the groups of obese and patients with GOLD stage IV disease compared with the groups of underweight patients with GOLD stage I disease (Figures 3 and 4). Recently, Capodaglio et al. 30 provided a reference equation specific for obese population and suggested that specific predicted reference values may have the advantage of providing a benchmark for functional capacity assessment and changes monitoring after pulmonary rehabilitation. 30
Further studies with large cohorts of volunteers in wide range of age would be necessary in order to create a 6MWD reference equation that will be highly representative and applicable to patients with COPD. Specifically, a population-based sample, a large number of healthy subjects in each decade of age, adequate exclusion criteria for poor health of ‘healthy subjects’ and methodological approach based on American Thoracic Society guidelines 7 should be considered for the creation of 6MWD reference equations. Anthropometric and demographic characteristics of healthy individuals recruited for the development of a reference equation should be ideally matched to the corresponding patients’ characteristics in which the equation is being applied. Additionally, the 6MWT operating procedures of studies formulated reference equations should be in line with those operating procedures followed by the population in which the reference equation is being applied. All of these criteria should be considered for the development and the choice of 6MWD reference equation that can provide an instant practical clinical information and interpretation for the levels of exercise capacity. In summary, existing 6MWD reference equations will give varying results in patients with COPD. The choice of 6MWD reference equations should consider the consistency of 6MWT operating procedures and at least be specific for the country/region of origin. This seems of less importance in underweight patients with mild COPD.
Footnotes
Authors’ contribution
VA contributed to data acquisition, data and statistical analysis, figures’ design and drafted the manuscript. AH, SS and MS contributed to the writing of the manuscript, critically reviewed the manuscript. FF, HP, AM and FS contributed to patients’ medical assessment, medical surveillance during exercise tests, critically reviewed the manuscript. IV and EW critically reviewed the manuscript. All authors read and approved the final manuscript.
Acknowledgement
VA obtained an ERS Long Term Research Fellowship (LTRF 63-2012).
Conflict of interest
The authors declare no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.