
Abstract
Asthma is the most common chronic medical condition affecting pregnancy. Optimizing asthma management in pregnancy is paramount for the well-being of both the mother and the baby. The primary objectives of this study were to assess patient’s knowledge about asthma, the level of asthma care, and fetal and maternal outcomes among pregnant asthmatic women in this wealthy country with tremendous improvement in maternal and fetal health care. The secondary objective was to identify barriers to asthma control. This was a cross-sectional, face-to-face, prospective study of 80 pregnant women with physician-diagnosed asthma. About 56% of patients reported worsening of their asthma control during pregnancy, of which 52.3% felt this worsening in the third trimester. About 65% of patients had uncontrolled asthma during their pregnancy, and inhaler technique was incorrect in 64.4%. Only 38% of patients knew the difference between controller and reliever asthma medications, 12.7% of patients had received written asthma action plan, 17% had a spirometry done in the previous 5 years, and 3.8% had peak expiratory flow meter at home. The main reasons for uncontrolled asthma were lack of knowledge about right asthma medications in 30% and fear of side effects of inhaled corticosteroids in 19% of patients. No financial reason was reported. Significant associations between total number of pregnancies, poor perception of asthma medications, asthma exacerbation during delivery and poor asthma control were observed. Preeclampsia and congenital anomalies occurred at higher rates than previously reported among general population in this country. The tremendous improvements in maternal health care and socioeconomic status do not seem to be a barrier to the globally recognized poor asthma care in pregnancy. Important strategies are much needed.
Background
Asthma is the most common chronic medical condition affecting pregnancy, occurring in 4–12% of pregnant women, and its prevalence appears to be continuing to increase. 1,2 Several previous studies have examined the effects of maternal asthma during pregnancy on a number of maternal and fetal outcomes. Such studies have clearly demonstrated that inadequate asthma control poses a greater threat for the mother and the fetus, including perinatal death, intrauterine growth retardation, preeclampsia, premature delivery, and low birth weight. 3 –6 The mechanisms for the effect of uncontrolled asthma on low birth weight and other fetal complications are unknown but may include a direct effect of fetal hypoxia on growth, changes in fetal growth via reduced uteroplacental blood flow or other alterations in placental function. 7,8 Optimal asthma control during pregnancy is therefore of paramount importance for protecting both the mother and the fetus. Despite the multiple reasons contributing to poor asthma control in general, a major contributor to asthma exacerbations and poor asthma control during pregnancy is the lack of appropriate treatment with inhaled corticosteroids (ICS) or their withdrawal during pregnancy due to unjustified or exaggerated fear of their side effects on the fetus. 7,9 ICS are the drug of choice for asthmatic women during pregnancy. The safety of ICS and their efficacy in controlling asthma in pregnancy have been demonstrated in multiple studies, indicating that these drugs can be used comfortably during pregnancy. 10,11 This fact has been further augmented by a meta-analysis that investigated the safety of different forms of ICS during pregnancy and did not find increase in the risk of major malformations, preterm delivery, low birth weight or pregnancy-induced hypertension from using these medications. 12 Following such strong level of evidence in the literature, the available international guidelines have emphasized the importance of continuing asthma medications (particularly preventer therapy such as ICS) during pregnancy as the risk of harm to the fetus from severe or chronically undertreated asthma outweighs any small risk from these medications used to control asthma. 13,14 Nevertheless, despite the wide availability of these clear guidelines, the poor management of asthma during pregnancy and the unjustified fear of use of ICS by both physicians and patients have been reported in many developed and developing countries. The reasons for such a huge discrepancy between the management of asthma recommended by evidence-based guidelines and that observed in clinical practice are poorly understood. 15 In a pre-piloted Australian survey of 842 general practitioners involved in shared maternity care at six maternity hospitals, a quarter of the respondents stated that they would stop or decrease patients’ ICS doses during pregnancy, even when their asthma was well controlled on these medications. In addition, 12.1% of respondents were not sure how to manage deteriorating asthma during pregnancy. Almost half the respondents reported encountering medication nonadherence during pregnancy. 16 Over a 6-year period in the United States, asthma medications were used by 63% of pregnant women with asthma. Only around a quarter of these women were using ICS. 2,17 Qatar is an oil and gas-rich country, and its gross domestic product (GDP) per capita is among the highest in the world with high health expenditure. 18 The country is currently witnessing a robust reform in its health care system aiming at achieving a world-class, patient-centered health care system by 2030. Tremendous improvements in maternal and child health care over the last two decades have been made and its current maternal, perinatal and neonatal mortality, and morbidity rates are comparable to the developed world. 19,20 Nevertheless, we have shown in a recent study that the very high GDP per capita in Qatar and the high health expenditure per capita do not seem to have led to better asthma care and control. 21 The main objectives of the current study were to assess patients’ level of education about asthma in pregnancy, the level of asthma care during pregnancy, and the maternal and fetal outcomes of pregnancy in asthmatic patients. The secondary objectives were to assess the barriers to asthma control during pregnancy in this rich country and the associations between asthma control and different variables.
Materials and methods
Study design
This was a cross-sectional prospective study of 80 pregnant women with physician-diagnosed asthma. The study was approved by the Institutional Review Board of Hamad Medical Corporation (Doha, Qatar; IRB No. 13245/13). The study was conducted from January 2014 to December 2016. Inclusion criteria included randomly selected pregnant women with physician-diagnosed asthma who attended women’s hospital and Hamad General Hospital (the largest tertiary hospital) in Qatar during the study period. The study settings included Hamad General Hospital outpatient medical and respiratory clinics and outpatient and inpatient settings of women’s hospital. All study subjects were presented verbally and in writing with detailed information about the study and its objectives. None of the patients who were invited to participate declined yielding a 100% participation rate.
Methods
Data collection
Participants who provided informed consent were interviewed face-to-face by one of the authors of this report for an average of 30 minutes using a written questionnaire. The questionnaire assessed five asthma and pregnancy-related items. The first item included current and previous pregnancy data and the effects of pregnancy on asthma, asthma history, symptoms, and associated medical conditions (that might worsen asthma control). The second item included questions on the level of asthma control and the level of asthma care during pregnancy including details of asthma medication prescribing pattern and use during pregnancy. The third item assessed the patient’s knowledge about asthma in pregnancy. The fourth item assessed the barriers to asthma control during pregnancy. The fifth item was completed during the follow-up interview and assessed the maternal and fetal outcomes during and after pregnancy.
Follow-up of participants
Following the initial interview mentioned above, participants were interviewed again at 6 months postpartum to assess details of asthma course and maternal and fetal outcomes of pregnancy. To confirm accuracy of information provided by participants at this time and minimize recall bias, electronic health records were also reviewed.
Assessment of asthma control
We used the Asthma Control Test (ACT) to assess the level of asthma control in the study subjects. The ACT has been previously validated during pregnancy and demonstrated good internal consistency and was responsive to changes in asthma course. Significant associations between asthma control during pregnancy by the Global Initiative for Asthma (GINA) classification and ACT has also been demonstrated. 22 –24 The ACT scores range from 5 (poor control of asthma) to 25 (complete control of asthma). An ACT score >19 indicates controlled asthma. 24
Assessment of inhaler technique
Patients were requested to demonstrate their inhaler technique to the interviewer using their own inhalers. For metered-dose inhalers, the following five steps were used to determine the correct use of inhaler 25 : (1) removing cap and shaking the inhaler, (2) breathing out gently before using the inhaler, (3) putting the mouthpiece in the mouth, (4) pressing the canister down at the start of inspiration and continuing to inhale slowly and deeply, and (5) performing a breath-hold for at least 10 seconds. For dry powder inhalers, patients were assessed for their performance of the following steps: (1) breathing out gently before using the inhaler, (2) placing the inhaler in the mouth and creating an adequate seal with the lips, (3) deep inhalation of the powder, and (4) removing the inhaler from the mouth and performing a breath-hold for 10 seconds. Incorrect use was defined as the failure to perform at least one of these steps.
Definition of asthma worsening or exacerbation
We used the internationally accepted definition of asthma worsening or exacerbation as events characterized by a change from the patient’s previous status (including symptoms or lung function) sufficient to require change in the treatment. 26
Quality assurance
Prior to starting the study, all physicians involved in conducting interviews with patients received training sessions on how to conduct the interview, asthma guidelines (GINA), ACT and the correct use of inhalers.
Statistical analysis
Qualitative and quantitative data were expressed as frequency with percentage and mean ± standard deviation with median and range. Descriptive statistics were used to summarize demographic and all other clinical characteristics of the participants. Associations between at least two qualitative or categorical variables were assessed using the chi-square (χ 2) test. For small cell frequencies, the χ 2 test with a continuity correction factor or the Fisher’s exact test was applied. Pictorial representations of the key results were made using appropriate statistical graphs. A two-sided p value <0.05 was considered statistically significant. All statistical analyses were performed using SPSS 22.0 (SPSS, Inc., Chicago, Illinois, USA).
Results
Characteristics of the disease and study population
Table 1 lists the characteristics of asthma in the study population. The mean age of patients was 31.6 ± 6.2 years and the mean age at diagnosis of asthma was 13.3 ± 11.1 years. During the initial interview, 75.9% of patients were in their third trimester of pregnancy, 17.7% were in the second trimester, and 6.3% were in the first trimester. Around 56% of patients reported worsening of asthma during pregnancy, 18% reported improvement, while 27% felt no difference compared with the prepregnancy state. In women whose asthma worsened during pregnancy, 52.3% reported the worsening in the third trimester, 22.7% in the second trimester, and 25% in the first trimester.
Patient and disease characteristics.

GERD: gastroesophageal reflux disease
Patient’s level of knowledge and education regarding asthma in pregnancy
Incorrect inhaler technique was observed in 64.4% of patients and 62% misunderstood the role of reliever and controller medications in asthma management. Although 78.5% of patients thought that asthma might affect the fetus, around 44% did not know what effects it could pose on the fetus. Around 39% of patients thought that ICS carry more risks to the fetus than asthma (Table 2).
Patient’s level of knowledge and education regarding asthma in pregnancy.
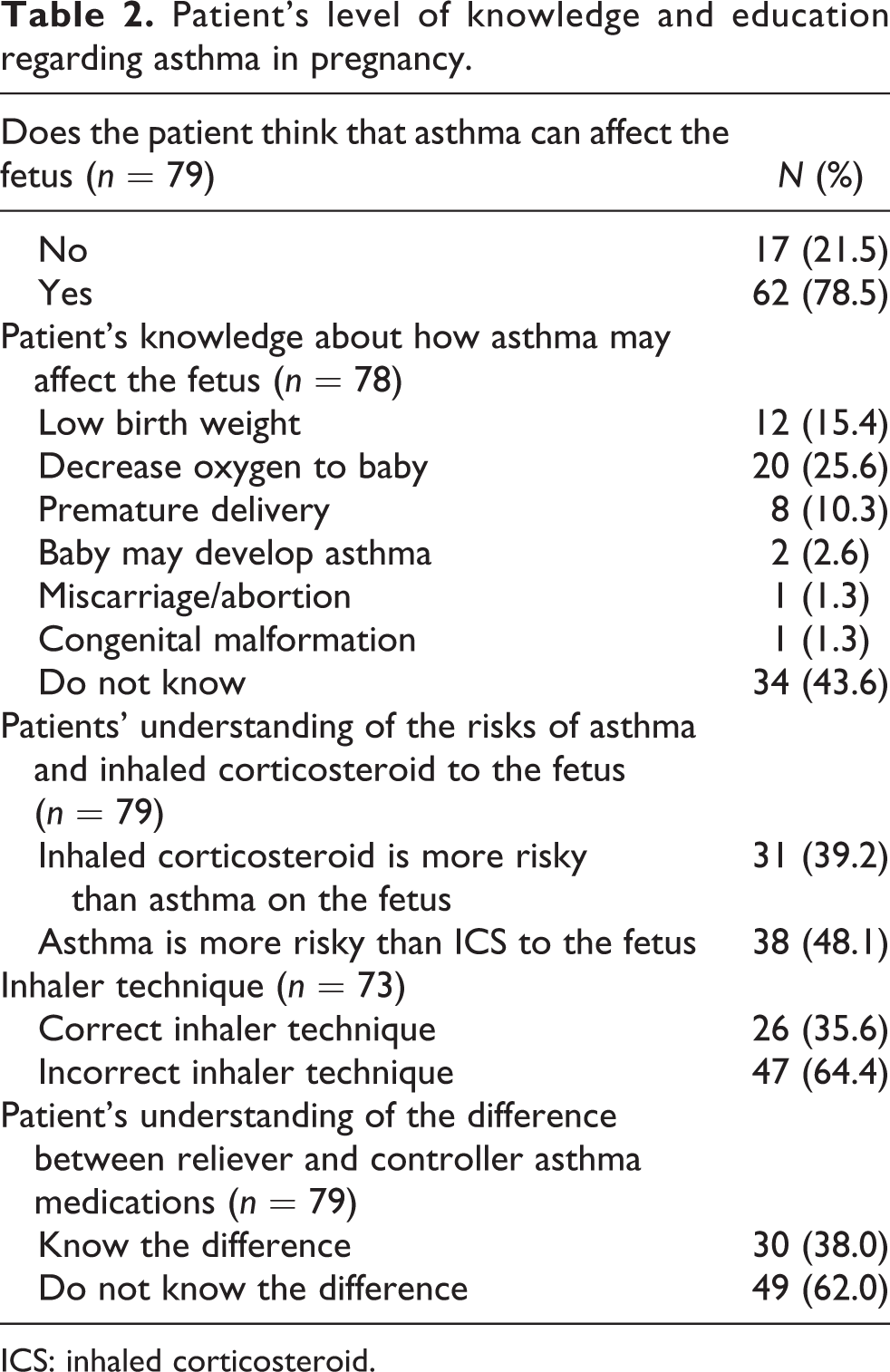
ICS: inhaled corticosteroid.
Asthma care practice during pregnancy
Based on ACT scores, around 65% of patients had uncontrolled asthma at the time of interview. Despite ICS were considered indicated in 68.4% of patients according to GINA guidelines stepwise approach, only 52% were actually receiving these medications suggesting suboptimal use of ICS. Patients reported the reasons for suboptimal ICS use as the fear of ICS’ side effects in 51.4% and failure of prescribing them by caring doctor in 48.6% of cases. Around 48% of patients had at least one emergency department (ED) visit, 36.7% had at least one hospital admission, and 33% had at least one unscheduled doctor visit for asthma reason during their current pregnancies. Only 3.8% of patients had peak expiratory flow (PEF) meter to monitor their asthma at home, 12.7% had received a written asthma action plan (AAP) and 17% had their spirometry done in the past 5 years (Table 3).
Asthma care practice during pregnancy.

ACT: Asthma Control Test; ICS: inhaled corticosteroids; ED: emergency department; GINA: Global Initiative for Asthma; PEF: peak expiratory flow; AAP: asthma action plan.
Maternal and fetal outcomes in pregnant asthmatic patients
The median length of hospital stay during and after delivery was 4 days. Around 42% of patients developed asthma exacerbation in the peripartum period and during delivery. The incidence of preeclampsia/eclampsia, low birth weight, congenital anomalies, miscarriage and preterm labor were 9.2%, 5.6%, 5.6%, 3.1%, and 1.5%, respectively. Furthermore, 8.5% of the infants developed asthma-like symptoms in the form of wheezy chest and breathlessness. The rate of cesarean section was 55.4% (Table 4).
Maternal and fetal outcomes in pregnant asthmatic patients.

Barriers to asthma control
Around 30%, 18.6%, and 21% of patients with uncontrolled asthma during pregnancy reported that lack of knowledge about the right asthma medications, fear of ICS side effects, and lack of regular follow-up, respectively, as the main reasons for their poorly controlled asthma. Furthermore, 9.3% reported the main reason as wrong perception of their asthma as mild one and a further 9.3% blamed their doctors for not prescribing the right asthma medication. Financial reasons have not been reported by any of the patients (Table 5).
Barriers to asthma control in patients with uncontrolled asthma.

Associations between level of asthma control and other variables
Significant associations were found between the level of asthma control and asthma exacerbation in the peripartum/delivery period (p = 0.001), patient’s knowledge about asthma medications (p = 0.019), total number of pregnancies (gravida) (p = 0.005), and postdelivery hospital stay (p = 0.047) (Table 6).
Associations between different variables and asthma control.

Discussion
A major finding of this study is the poor asthma control and increased health-care utilization due to asthma among pregnant women. We have demonstrated in a recent study the poor asthma control among asthmatic patients in this country in general. 21 Moreover, this finding concurs with prior evidence that suggests inadequate asthma control and asthma exacerbations during pregnancy as a worldwide problem affecting both developed and developing countries. In a recent study of 103 pregnant women with asthma from Brazil, only 44% fulfilled the criteria of controlled asthma using the GINA assessment tool. 27 A large population-based study of 4315 pregnant women with asthma examining asthma morbidity in the United States revealed that 12.7% of women received rescue corticosteroids during their pregnancies, 11.1% had asthma-related ED visits, and 6.3% of women were hospitalized. Moreover, racial differences were also observed with Black asthmatic women who were more likely to receive a course of rescue corticosteroids than Whites (14.6% vs. 11.9%), have an ED visit (16.7% vs. 8.7%), or be hospitalized for asthma (9.0% vs. 5.2%). 28 In a prospective study from Australia, up to 45% of pregnant women with asthma had moderate-to-severe exacerbations requiring medical intervention during pregnancy. 17,29
The finding that suboptimal use of asthma medications (particularly ICS) in this study is in agreement with other studies from other parts of the world, suggesting also a global nature of the problem. An American study that assessed the prevalence of asthma medication use during pregnancy between 2001 and 2007 revealed that asthma medications were used by 63% of patients and only a quarter of these women were using ICS. 2,17 Suboptimal use of asthma medications during pregnancy have also been reported in Ireland, Korea, and Australia. 17,30 –32 Education in asthma self-management, which involves self-monitoring by either PEF or symptoms and proper medication use coupled with regular medical review and a written AAP improves health outcomes for adults with asthma. 33 Murphy et al. reported poor asthma self-management skills and knowledge among pregnant women, regardless of the severity of their asthma. Overall, 40% of patients were nonadherent with ICS medication, less than 50% had optimal inhaler technique, and 42% had inadequate knowledge about their prescribed medications. PEF monitoring was performed only by 3% of patients and only 15% had a written AAP. 34 After implementing an asthma education program in antenatal clinic, there were significant improvements in all aspects of asthma self-management with improvement in severe asthma symptoms and reliever medication use.
Interesting findings in the current study are related to the course of asthma during pregnancy. Over half of the patients reported worsening of asthma symptoms during pregnancy. The conventional wisdom is that asthma tends to follow the “rule of thirds” among pregnant women, with one-third of the patients experiencing an improvement of symptoms, one-third a deterioration of symptoms, and one-third no change in symptoms. 35 Nevertheless, more recent reports have challenged this quote and linked the asthma course during pregnancy to the initial severity of asthma. Among the pregnant women diagnosed with mild asthma, there is an 8% risk of deterioration resulting in exacerbation compared to a 47% and 65% risk of deterioration resulting in exacerbation in women diagnosed with moderate or severe asthma, respectively. 36 –38
In contrast to the findings from previous studies that reported asthma worsening to happen mostly during the second trimester with improvement during labor, 39 the current study revealed that asthma worsening happened more frequently in the third trimester and significant exacerbations were observed during labor. As mentioned earlier, asthma course during pregnancy tends to vary based on asthma severity. Gluck et al., in a more recent systematic review, concluded that second and third trimesters are the most likely time for asthma worsening with a peak in the sixth month. Moreover, 10–20% of asthmatics tend to develop symptoms during delivery. 40
As it was anticipated, as a consequence of the wealth of the country, none of the participants in the current study reported financial reasons for poor asthma control. The finding of significant association between the level of asthma control and the total number of pregnancies (number of gravida) in this study is very fascinating. To the best of our knowledge, this association has rarely been addressed in previous studies, and further studies needed to confirm it. Unlike asthma control in general population in this country, we did not find statistically significant association between asthma control and the type of physician practice (specialist vs. nonspecialist) in pregnant women. 21
Compared to previous studies that have estimated the incidence of different maternal, neonatal, and perinatal outcomes in general pregnant population in Qatar, the incidence of low birth weight in asthmatic pregnant women in the current study was less than that in the general population (5.6% vs. 8.3–9.5%). 19,20 However, the incidence of preeclampsia/eclampsia and major congenital malformations/birth defects were more than that of general population (9.2% vs. 0.31/1000 and 5.6% vs. 1.67%, respectively). 41,42 Furthermore, three of the four congenital anomalies and five of the six preeclampsia cases observed in this study occurred in mothers with poorly controlled asthma at the time of interview. The prevalence of gestational diabetes in Qatar is 16.3%. 43 Hence, the high prevalence of gestational diabetes observed in the current study participants is not surprising.
The QAKCOP study is the first comprehensive study to address asthma knowledge, care, and outcome in pregnant women in this wealthy country. In this study, patient’s interview was conducted face-to-face by trained physicians, with good background knowledge of asthma and asthma guidelines, who were not responsible for asthma care of the participants. This has permitted direct observation of inhaler technique by the interviewing physician as well as accurate judgment of controller medication indication and use based on the current asthma guidelines.
Limitations of the study
A major limitation of this study, besides the relatively small number of participants, is the reliance on physician diagnosis of asthma because of the underuse of spirometry in this country. Reliance on prior physician’s diagnosis of asthma could result in an impure asthma cohort. 21 Furthermore, asthma control in the current study was based on a single assessment via ACT rather than an average of multiple assessments. A patient’s level of asthma control may vary over relatively short or long time intervals in response to allergens or infectious agents or in response to treatment. Although ACT is used to assess asthma control over a 4-week period, clinical asthma control is ideally assessed on multiple occasions. 26 Previous studies have reported a reversion to preconception bronchial hyperresponsiveness occurring 1 month after delivery. 39 In the follow-up part of the current study, we inquired about asthma symptoms and exacerbations during delivery and in the short peripartum period, but, unfortunately, we did not inquire about asthma symptoms beyond that period. The rate of some and fetal outcomes in this study should be interpreted with caution due to the lack of control group of non-asthmatic pregnant women. Despite the high prevalence of asthma among children in Qatar (19.8%), 44 the current study was not intended to measure asthma prevalence among pregnant women, as another study with the objective of estimating the prevalence of this disease in adults (including pregnant women) is ongoing in the country.
Conclusions
The current study has shed a light on the critical shortage in asthma care and patient’s perception of asthma and asthma medications during pregnancy even in the absence of economic reasons. Asthma care and management during pregnancy did not seem to coincide with tremendous improvements in maternal and child health care in this wealthy country. The results of this study also highlighted the urgent need for clinicians and health care policy makers to focus on maintaining asthma control during pregnancy. Important strategies such as early referral of asthmatic pregnant women for asthma management and follow-up, the introduction of specialized asthma in pregnancy clinics that encompass a multidisciplinary model of care for asthmatic pregnant patients, and the introduction of asthma education and self-management skills prepregnancy could potentially improve maternal asthma outcomes. 33,45,46 More frequent follow-up of such patients, preferably every 1–2 weeks initially, to ensure asthma control is achieved is also recommended. 47
Footnotes
Acknowledgements
The authors are indebted to Dr Tasleem Raza, Dr Abbas Al-Abbas, Dr Hassan Mobayed, and Dr Hisham Abdul-Sattar from Pulmonary Section, Hamad General Hospital, for their valuable support during the preparation of this manuscript. WHI, FR, MA, ASB, LIA, AMEA, MMD, IYA, MUK, TSI, and AAI were responsible for conception and design, provision of study materials/patients, collection and assembly of data, data analysis and interpretation, manuscript writing, and final approval of the manuscript. Administrative support was provided by WHI, FR, and MA.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.