
Abstract
Chronic obstructive pulmonary disease (COPD) is a leading cause of death, morbidity, and health-care spending. The Halifax, Nova Scotia-based INSPIRED COPD Outreach Program™ has proved highly beneficial for patients and the health-care system. With direct investment of <$1-million CAD, a pan-Canadian quality improvement collaborative (QIC) supported the spread of INSPIRED to 19 teams in the 10 Canadian provinces contingent upon participation in evaluation. The collaborative evaluation followed a mixed-methods summative approach relying on collated quantitative data, team documents, and surveys sent to core members of the 19 teams. Survey questions included a series of multiple-choice responses, Likert scale ratings, and open-ended questions. The qualitative evaluation entailed key informant interviews and focus groups undertaken between February and April 2016 post-collaborative. Teams reported that the year-long QIC helped bring focus to a needed, though often overlooked area of improvement, facilitating innovation spread. They report examples of new work practices as well as unanticipated cultural change (given the short QIC time frame). Most teams gained new skills in quality improvement (QI) and evidence-based medicine, showing progress in their ability to measure and implement COPD care improvements. Teams felt networking with other teams across the country toward a common solution as well as learning from a team of clinical innovators and evidence-based innovation were critical to their success. Factors affecting sustainability included local leadership support, involvement of frontline clinicians, and sharing milestones to motivate continued QI. The INSPIRED QIC enabled teams across Canada to adapt and implement a new COPD care model for high users of health-care with rapid improvements to work practices, cultural change, and skill sets, and at relatively low cost.
Introduction
Recent professional society consensus statements, clinical practice guidelines, reviews and research related to COPD promote more holistic, collaborative, and integrated care. 1 –6 Patients with advanced stages of COPD are among the highest users of hospital-based care. 7,8 They endure a long trajectory of diminishing quality of life, escalating frequency of hospitalization, and ongoing unmet needs 9 –11 that warrant changes to current care models and health-care practices.
Quality improvement collaboratives (QICs) address provider practices by supporting health-care teams to apply evidence-based medicine (EBM) and quality improvement to implement change. 12 –14 Through QICs, collaborating teams of frontline clinicians can learn how to change practice, thereby improving outcomes, ultimately improving service use and costs. The Institute for Healthcare Improvement (IHI) in the United States has a long tradition of supporting QIC initiatives. 15 In Canada, where provincial-based health-care funding models and geography pose challenges to national initiatives, experience with and outcomes of QICs are more limited.
A federal advisory panel on health-care innovation alluded to these challenges when concluding, “many excellent ideas or inventions are never translated into saleable or scalable innovations.” 16 “Such ideas often remain isolated due to the absence of ‘winning conditions’ within and across health systems for facilitating innovation uptake and spread.” 16 The same report highlighted the INSPIRED COPD Outreach Program™ (hereafter referred to as INSPIRED), as a spread-worthy innovation.
INSPIRED was implemented in Halifax in 2010 as a novel, evidence-based, and facility-to-community clinical initiative. It was designed to reverse the revolving door patient experience for those with advanced chronic obstructive pulmonary disease (COPD) by improving care transitions, self-management, and engagement in advance care planning (ACP). Patients consented to a series of home visits (usually four) with education and support provided initially by a certified respiratory educator with follow-up visits from a spiritual care practitioner. Patients were then followed monthly (×3) by telephone.
Enrollment criteria were as follows: confirmed or pending diagnosis of COPD (spirometry), community dwelling in Halifax Regional Municipality, willing to be enrolled AND at least one criterion that defines advanced disease and increased mortality risk (from Medical Research Council (MRC)) 4 or 5 dyspnea, at least one admission in 12 months prior to index admission, an ICU/IMCU admission in previous 12 months, chronic respiratory failure (PaCO2 > 45), or clinical signs of right heart failure. INSPIRED was designated as a leading practice by Accreditation Canada in 2014. We have described development and components, 17 earlier positive outcomes for patients (enhanced confidence in symptom management and willingness to discuss care goals/ACP) 18,19 and for the health-care system (substantial cost aversion based on marked reductions in facility reliance for enrolled patients completing all program components and surviving for at least 6 months). 19,20
Building on local success and recognizing the widespread nature of the underlying problems INSPIRED addresses, the Canadian Foundation for Healthcare Improvement (CFHI)—an independent, nonprofit organization—delivered a pan-Canadian quality improvement INSPIRED collaborative with (arms-length) funding from industry (Boehringer Ingelheim Canada Ltd., BI). 21 Nineteen teams were supported through 2014 to 2015 in adapting and adopting an INSPIRED approach to care. We planned for and described this approach in a pre-implementation phase in a previous publication 21 (in which we also provide information on elements of the original INSPIRED program that patients found helpful). We expand upon this here, with details of team experiences and changes in practice consequential to participation within the collaborative.
Within the context of the INSPIRED approaches to COPD care QIC, our aim was to understand and highlight components of the QIC that we believe underpin a successful spread innovation that addresses the burgeoning needs of patients and families living and dying with COPD. 9 –11
Methods
The INSPIRED QIC supported and provided start-up funds for 19 teams from more than 78 organizations (across acute, primary, and home care) from every province in Canada. Nineteen of 31 applications were selected on the basis of a merit review process involving two reviewers, subsequent group discussion as part of a chaired review panel and a scoring system (akin to a research review process). Teams were mandated to comprise at a minimum: a certified respiratory educator, a measurement/quality improvement specialist, a physician lead, and a social worker or spiritual care practitioner. 22 Applications were rated according to clarity of plans to understand local context of COPD (admissions, emergency department (ED) visits), gain institutional support, plus ability to collect and measure data prior to and during the implementation of their projects (see Table 1A for details).
The INSPIRED QIC provided teams with enhanced support beyond the typical components of QICs (Table 1A). 12 During a one-year period of instruction, CFHI offered teams 24 webinars (∼46 hours of instruction), one in-person workshop, regional roundtables (four in total—one per Western and Atlantic Canada, Ontario and Quebec), and numerous teleconferences within and across teams. The curriculum framework developed by CFHI, built on the IHI improvement model and the “doing the right thing right” framework, which focuses on evidence-based medicine (doing the right thing) in combination with quality improvement (doing it right) to inform practice change. 23 –25
Teams also received seed funding of $50,000 CAD each to support the human resource needs associated with implementing and evaluating INSPIRED interventions. Several teams opted to receive additional logistical support (e.g. project management or networking/dissemination support) from the collaborative partner, BI.
Potential INSPIRED models of care were acute-dominant, as opposed to community dominant (e.g. home or community-based programming). Teams reported alignment with the following care models during the post-collaborative workshop (Figure 1):

Team-reported models of care. A: Alberta Health Services Edmonton Zone; B: Centre intégrés de santé et de services sociaux de la Montérégie-Est; C: Centre intégré de santé et de services sociaux du Bas-Saint-Laurent; D: Bruyère Continuing Care; E: Central Health; F: The Ottawa Hospital; G: University Health Network; H: London Health Sciences Centre; I: Horizon Health Network; J: Nova Scotia Health Authority (South Shore Health); K: Providence Healthcare; L: Health PEI; M: Joseph Brant Hospital; N: Hôpital du Sacré-Coeur de Montréal; O: Hamilton Health Sciences; P: Institut universitaire de cardiologie et de pneumologie de Québec; Q: Winnipeg Regional Health Authority; R: Saskatoon Health Region; S: Grey Bruce Health Services.
Specialist outreach (push): The hospital extends its reach into patients’ homes and out into the community and drives the initiative.
Acute with community care partnerships (including public–private partnerships): A hospital-driven model, but with distinct roles for community providers (public or private).
Community driven (pull): Model which is home/community care-led, considered a “destination home” approach, pulling in the services patients need at home.
Integrated specialist expertise into primary care: A model led by primary health care with truly integrated specialist expertise (often referred to as the chronic care model (CCM) 26 or the “patient-centered medical home model.” 27
Nine teams indicated selection of two models or a combination thereof (Figure 1). Two teams indicated they were “other” categories—for example, a transdisciplinary model of care and a continuing care model, respectively.
Evaluation
The mixed-methods summative evaluation relied on post-collaborative team final reports, survey, key informant team/focus group interviews, and self-rating exercises: Final reports: (19 reports collected in October to November 2015) focused on team improvement aims, results, impacts (related to care delivery, culture and patient, family, and provider stories of change), and sustainability. Survey: (19 teams, 54 respondents, with a mean of 2.8 respondents/team and carried out in November to December 2015) focused on team skills and competencies gained, new work practices implemented, sustainability, spread, and experience in the collaborative. Each question was analyzed and descriptive statistics generated based on the number of respondents per question (in anticipation of some incomplete surveys). Key informant team/focus group interviews: Invitations to participate were sent to 19 teams in January to February 2016 and focused on successes, challenges, and lessons related to innovation adaption to local context, plans for sustainability, spread and scale-up, and value of collaborative participation. Thirteen teams (n = 38 participants) participated (February to April 2016) in either a key informant team interview (n = 8 teams, n = 31 participants) or focus group (n = 5 teams, n = 7 participants). Two evaluators were present and took notes for all interviews, which were audio-recorded. Self-rating exercises: (invitations to participate were extended to 19 teams in April 2016) focused on prepost team measurement capacity (five-point scale), adapted (though not validated) from a scale developed by IHI, which CFHI used to understand team-reported performance measurement capacity, see Figure 2. The rating exercise was carried out between April and June 2016 with 14 teams as part of an April 2016 postcollaborative workshop (teams subsequently validated their results in May to June 2016); and an additional four teams via email (between May and June 2016). One team did not respond and was ranked by CFHI based on knowledge adequate to undertake that ranking.

Pre and post-collaborative measurement capacity (n = 19). A: Alberta Health Services Edmonton Zone; B: Centre intégrés de santé et de services sociaux de la Montérégie-Est; C: Centre intégré de santé et de services sociaux du Bas-Saint-Laurent; D: Bruyère Continuing Care; E: Central Health; F: The Ottawa Hospital; G: University Health Network; H: London Health Sciences Centre; I: Horizon Health Network; J: Nova Scotia Health Authority (South Shore Health); K: Providence Healthcare; L: Health PEI; M: Joseph Brant Hospital; N: Hôpital du Sacré-Coeur de Montréal; O: Hamilton Health Sciences; P: Institut universitaire de cardiologie et de pneumologie de Québec; Q: Winnipeg Regional Health Authority; R: Saskatoon Health Region; S: Grey Bruce Health Services.
A modified thematic analysis was employed for all qualitative components, whereby all materials (report or survey responses, interviewer notes) were read by three evaluators (a lead researcher, (SS), working with two research assistants) to generate overall themes from the data, followed by a process of open coding, which then informed development of overarching themes. To ensure consistency, the evaluators met frequently, including with CFHI staff (JV, CA) to discuss and clarify emerging themes and findings. Where possible, illustrative verbatim quotes were extracted. CFHI worked with teams throughout the collaborative to establish ethical parameters to govern data sharing for continuous quality improvement and public communication of results. These parameters were part of the CFHI-team memoranda of understanding. As a QI initiative, formal research ethics board (REB) approval was neither required nor sought by CFHI; however, some teams sought local REB approval.
Results
Collectively, the 19 teams have reached more than 1000 patients. Preliminary results (to be reported in detail later) suggest similar outcomes to the Halifax-based programs patients and families consistently report greater self-confidence in symptom management, returns to daily activities, and enjoyment of enhanced functional status. 28 Similar to outcomes in Halifax, teams have also reported substantially fewer ED visits and hospitalizations (40–80%) among those enrolled. 29
We present results relating to delivery of the collaborative under four subheadings: (i) the most significant achievements, cultural changes, and new work practices, (ii) team skills acquisition and improvement capability, (iii) the collaborative approach—the components of the INSPIRED QIC and related team feedback, and (iv) sustainability.
Most significant achievements, cultural change, and new work practices
Teams shared their top achievements placing greatest emphasis on the role the INSPIRED QIC played in increasing awareness of COPD (8 teams—refer to legend—A, C, E, G, H, J, K, and M); identifying gaps in transitions and working to eliminate them in partnership with community services and resources (8 teams: A, D, F, H, J, K, R, and Q); and improving consistency and coordination of COPD management (6 teams: D, F, G, H, M, and O). Many teams noted that the focus on INSPIRED helped to drive efficiency in and spread of health system improvement; in particular, teams indicated that participating in a pan-Canadian collaborative helped to raise the profile and immediacy of a needed area of innovation, while providing the structure and support to adopt new practices (Box 1).
“INSPIRED gave us a proven model to follow, which could be adapted to meet regional needs, but ensured significant time and resources did not have to be used for program development” (Central Health). “Prior to [the INSPIRED collaborative], the focused examination of clients with advanced COPD living in the community would have been years in the making” (Alberta Health Services). “The memorandum of understanding signed with our partners (CFHI and BI) and the accountability requirements [of the collaborative] helped ensure the project remained a priority for our organization” (Centre intégrés de santé et de services sociaux de la Montérégie-Est). “Participating in the collaborative provided the needed focus and profile to greatly accelerate the regional work on COPD…The national profile has helped to elevate the work within the region and with senior leaders. Reporting to CFHI created an urgency and sense of accountability to an external body. This pressure has helped the initiative to continuously drive forward” (Winnipeg Regional Health Authority).
While INSPIRED addressed a targeted (disease-specific) area of improvement, 17 of the 19 teams cited at least one example of how their participation in the collaborative led to organizational cultural changes (Table 1). Examples varied but generally included one or more of the following qualifying statements of culture change: INSPIRED helped to create a new standard of care for patients living with advanced COPD and their families; INSPIRED enhanced care integration across the facility-to-community divide, bridging relationships between providers across the care continuum; and INSPIRED created a heightened awareness of the impact of COPD on health system use and the opportunity for efficiency gains that impact the health system (Table 1).
Examples of team-reported organizational culture change (within final reports).

INSPIRED: INSPIRED COPD Outreach Program™; COPD: chronic obstructive pulmonary disease; MRC: Medical Research Council; RN: registered nurse.
Regarding implementation of new work practices, 30/41 (73%) respondents agreed the new (INSPIRED) practices became the “standard way to work” (Table 2). A similar number of respondents (31/41, 71%) reported “leadership acknowledges continued improvement is a key strategic priority for the organization.” The area receiving the greatest support (36/42, 86%) was “tools and educational resources on COPD management are available to staff.” Six months postcollaborative (in April 2016), all but three teams reported they were continuing to enroll patients, with 15 teams confirming they were sustaining their INSPIRED improvements and one having never enrolled patients.
Team-reported effects of new organizational work practices (reported postcollaborative, final survey).
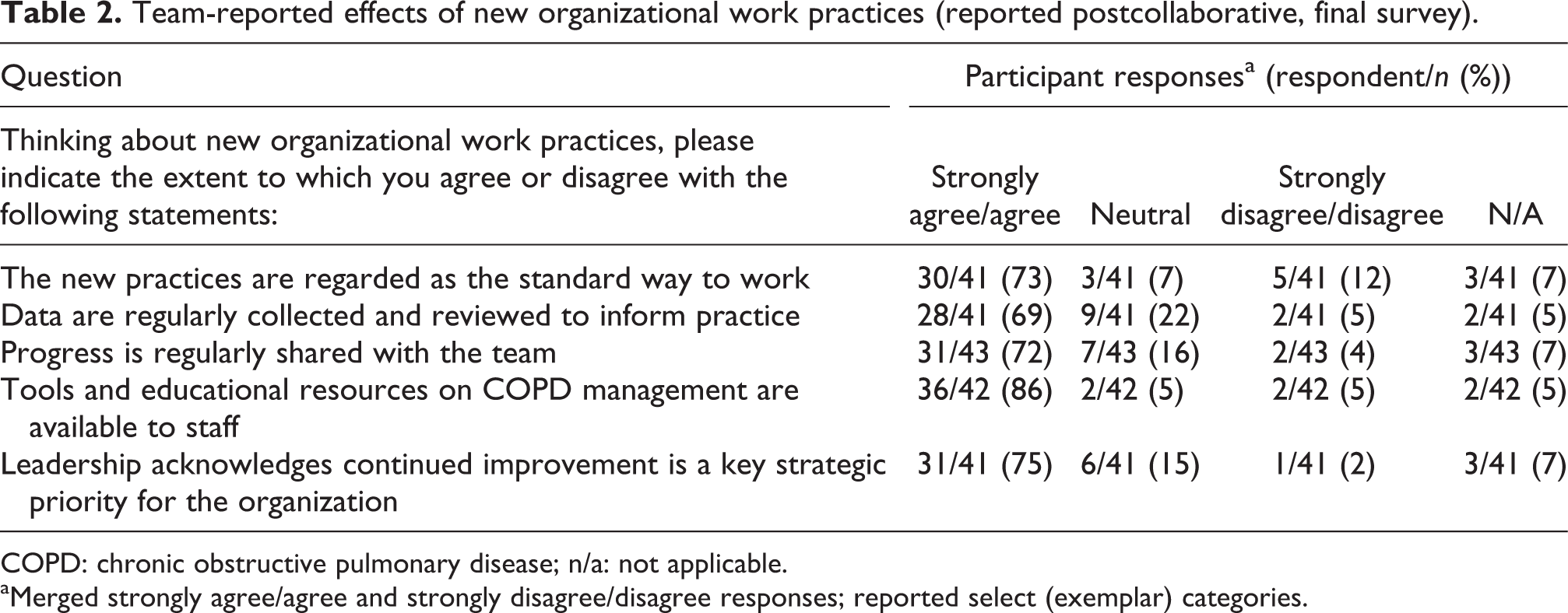
COPD: chronic obstructive pulmonary disease; n/a: not applicable.
aMerged strongly agree/agree and strongly disagree/disagree responses; reported select (exemplar) categories.
Skills acquisition (improvement capability)
Teams reported a number of gained QI skills, for example, 35/46 respondents (76%) indicated they became better able to “design innovative solutions (e.g. suite of COPD interventions, effective team-based care, etc.)”, and the majority reported they became better equipped to develop benchmarks/targets for improvement (33/46, 76%), develop tools and processes to lead change in health-care improvement (33/46, 76%), and communicate improvement goals and outcomes to motivate staff to get and stay involved (32/45, 71%) (Table 3). When it came to teams’ abilities to assess, design, implement, and evaluate local INSPIRED innovations, all but one team reached implementation. The level of evaluation data collected and analyzed varied considerably across teams. An overview of the INSPIRED interventions and associated measurement framework that teams were asked to implement is available as a change package. 30
Team-reported skills acquisition (reported postcollaborative, final team survey).

INSPIRED: INSPIRED COPD Outreach Program™; COPD: chronic obstructive pulmonary disease.
aMerged strongly agree/agree and strongly disagree/agree responses; reported select (exemplar) categories.
The INSPIRED QIC helped to develop capacity of teams to measure and undertake quality improvement. On measurement, teams self-ranked their capacity pre and post-collaborative (Figure 2). Teams gained measurement capacity with an average jump of 2.7 (from an average pre-collaborative score of 1.3 to an average post-collaborative score of 4.1) on the five-point scale.
Collaborative approach
The emphasis that INSPIRED puts on collaboration between health-care professionals helped teams develop pathways for patients living with COPD during the facility-to-community transition. For example, the majority of respondents (38/46, 85%) reported the collaborative equipped them to be “better able to develop and coordinate partnerships with community and allied healthcare support services” (Table 3) as well as shift care from hospital to home. Teams reported, for example, The value of the program is bringing silos together…We work for a hospital but are trying to provide care outside of the hospital—because that’s what patients require (The Ottawa Hospital). [We are] starting to engage other elements of community who work with patients—primary care nurses, interprofessional providers and hospital-to-home teams for people with high ED readmissions and looking at what these pieces look like and how to integrate our current work with these groups (Winnipeg Regional Health Authority). The collaborative provided an opportunity for development and testing of an innovative partnership model between the hospital and community-based partners to ensure that the right care is delivered in the right place at the right time (Hamilton Health Sciences).
When asked to report on the benefits of participating in the INSPIRED QIC, teams described the benefits of networking with other teams through face-to-face meetings. Learning from a team of clinical innovators from Halifax INSPIRED firsthand was also highly regarded. Teams also reported the seed funding provided by CFHI was beneficial, with teams indicating they had put this money to good use, most often to hire (or free up the time of) a project lead or COPD educator. Teams noted they would have benefitted from more face-to-face time (including early on in the collaborative) to brainstorm ideas and help collaboratively troubleshoot areas of change management/implementation, engagement (patient, provider, and leadership), and evaluation. In addition, time allocation for the webinars was an issue. Webinars—though helpful for bringing the teams together for engagement with faculty and CFHI staff—required more time than was anticipated or planned for.
Sustainability
Teams identified six factors as contributing to the success and sustainability of their INSPIRED programs: (1) leadership acknowledgement and buy in, (2) alignment with organizational priorities, (3) engagement and leadership from the clinical front line, (4) access to tools and educational resources on COPD management, (5) sharing of milestones to motivate the team doing the work, and (6) recognition in a new standard of practice and care as results validate the approach. The dominant cited barriers to sustaining INSPIRED included (1) a lack of continuous resourcing, (2) competing demands on staff time, and (3) difficulties associated with providing comprehensive care for patients with complex needs. At the time of writing, we are aware that plans to scale up and spread an INSPIRED-like approach to COPD care are already underway in several provinces and under consideration in others.
Discussion
As part of the evaluation of the INSPIRED Approaches to COPD Care collaborative, teams reported substantial changes in local attitudes to and delivery of care for patients with COPD that are consistent with the Triple Aim, long espoused by the IHI, namely “better care, better outcomes, better value.” 31 Teams reported that the QIC helped bring focus to a needed, though often overlooked area of improvement, facilitating innovation spread. They reported examples of new work practices as well as cultural change (Tables 1 to 3), which was unanticipated within the short time frame of the QIC. The majority of teams gained new skills in QI and EBM, showing progress in their ability to measure and implement COPD care improvements (Figure 2). Teams felt networking with other teams across the country toward a common solution as well as learning from a team of clinical innovators and evidence-based innovation were critical to their success.
The uptake of new practices in the light of new evidence often takes several years in medicine. Physicians in particular are often resistant to innovation.
32
An influential white paper on spreading health-care improvement summarized the key ingredient in spreading innovation: A key factor in closing the gap between best practice and common practice is the ability of health care providers and their organizations to rapidly spread innovations and new ideas. Pockets of excellence exist in our health care systems, but knowledge of these better ideas and practices often remains isolated and unknown to others…too often these improvements remain unknown and unused by others within the organization.
15
Financial implications
The achievements and improvements to COPD care made at team level within the 10 provinces came at a relatively low direct investment of less than $1-million CAD (19× $50,000). Based on a 2016 independent return on investment analysis, if INSPIRED reached <1% of people living with COPD in Canada, it would result in 68,500 fewer ED visits; 44,100 fewer hospitalizations; and 400,000 fewer bed days in the next 5 years, averting ∼$688 million in costs. 38 Translated into bed utilization, and were these beds to be made available to others, several thousand patients would gain earlier access for acute illnesses and/or be removed from surgical waiting lists each year.
With these considerations, several health systems/provinces are currently exploring opportunities for scale up and spread of an INSPIRED program. Moving from spread of an intervention (one jurisdiction adapts and adopts a practice to their context)—to scale up (a jurisdiction aims to reach all patients who stand to benefit from a given practice) undoubtedly requires further support. At the heart of transformative health system change are clinicians who work in partnership with patients and their families, toward testing and applying best practices and undertaking quality improvement to achieve it.
Limitations
We accept that the experiences of and lessons learned through this collaborative may not be generalizable to all jurisdictions in Canada or elsewhere. The INSPIRED program was designed for patients with advanced COPD and so the approach within the collaboration may not apply to those with mild to moderate disease. Nevertheless, with similar attention to detail and as expertise in delivery and evaluation of QICs grow, we anticipate improvements to COPD care across Canada and beyond. In addition, the approach to COPD within the collaborative lends itself to more generic chronic illness care models.
Conclusion
The CFHI has, at relatively low cost, enabled teams across Canada to adapt and implement a local evidence-based and patient-centered innovation for the care of patients with advanced COPD with improvements to work practices as well as cultural change. Most teams gained new skills in QI and EBM, showing progress in their ability to measure and to implement improvements to COPD care within a time frame of less than 2 years. By describing the anatomy of a successful collaborative, we hope to illuminate a path that other organizations may follow to support the creation and rollout of new care models. New models are essential components of strategies to drive restructuring of health-care systems that have for too long failed to respond to demographic changes and the needs of patients who live with chronic illness. 6
Footnotes
Author’s note
The views expressed herein do not represent those of the Government of Canada. JV is and CA was employed by CFHI; GR and SS are consultants working with CFHI.
Acknowledgments
The authors thank Maureen O’Neil OC (President) and Stephen Samis (Vice-President) of the CFHI as well as the faculty for their support for the implementation and delivery of the INSPIRED COPD collaborative and the teams who accepted this call to action to join the collaborative. The authors also thank Meghan Rossiter, Kirby Kirvan, and Catherine Giroux of CFHI as well as Dylan Brennan of Western University for their dedication to the successful delivery of the multiple components of the collaborative and/or its evaluation. The authors acknowledge Catherine Simpson PhD for her review of an earlier draft of this manuscript. The authors gratefully acknowledge the leadership of BICL for their arms-length funding and in-kind support.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The INSPIRED Approaches to COPD Care collaborative was hosted by the Canadian Foundation for Healthcare Improvement (CFHI) with arms-length funding from Boehringer Ingelheim Canada Ltd. (BI). CFHI is a not-for-profit organization funded by the Government of Canada.
Appendix 1
Description of the most common structural and process-oriented components* of QICs (reported by Nadeem et al. 2013) 12 as compared to the INSPIRED QIC model (2014–2015).

| Component | Description | INSPIRED QIC model |
|---|---|---|
| Overall QIC structure | 12 months on average | 12 months with prework and postcollaborative support for ongoing evaluation and dissemination |
| In-person learning sessions led by expert faculty for multidisciplinary teams | In-person learning session (midpoint workshop) led by expert faculty coaches for multidisciplinary teams, regional roundtables hosted in four regions involving existing and new stakeholders to support sustainability and scale-up planning, and in-person learning session (postcollaborative workshop) led by expert faculty for multidisciplinary teams | |
| Team-led quality improvement projects | 19 team-led improvement teams | |
| All in-person learning sessions and most phone meetings involved multiple sites | All in-person and webinar learning sessions and most teleconferences involved multiple sites. Webinar sessions included all team calls (9), team progress reporting (4), measurement calls (5) with recordings archived for on demand use, and optional affinity (or theme) calls (6). Teams received on demand coaching via teleconference. | |
| Governance | All content independently designed and delivered by CFHI faculty and staff (via monthly teleconferences and face-to-face meetings); industry sponsor (BI) partner provided financial support to CFHI, in turn providing financial support to teams ($50,000 per team). BI also provided in kind support to teams (e.g. project management support, business development support, etc.)—only for those teams that requested. CFHI-BI met regularly (via monthly teleconferences and face-to-face meetings) to exchange information about the collaborative and teams. | |
| Multidisciplinary QI teams* | Most involve such teams, but with limited detail as to team roles (e.g. direct care providers or management-level staff; representing different roles within an organizational hierarchy) | Teams comprised of direct care providers and middle managers, with an assigned team lead or co-lead, measurement lead, physician champion, clinical and administrative leads, and COPD educator. Executive level sign off was required. |
| Selection criteria | Pan-Canadian cohort of teams from across ten provinces: Quebec (4), Ontario (7), British Columbia (1), Saskatchewan (1), Manitoba (1), Alberta (1), Prince Edward Island (1), Nova Scotia (1), New Brunswick (1), Newfoundland, and Labrador (1) | |
| Call for application issued for expressions of commitment (applications) outlining organizational structure and readiness (including relevant QI experience and ties across facility-to-community settings), budget, team composition, population characteristics, and health-care use associated with COPD. Each application was evaluated by two reviewers (including CFHI staff, INSPIRED faculty, and guest reviewers with expertise in QI and/or respirology) and ranked on a five-point scale as part of a chaired Merit Review Panel. Applicants receiving a review grade at or above four were offered participation in the collaborative. | ||
| In-person sessions* | Three sessions of two days each on average | One two-day in-person (midpoint) workshop held in Vancouver, BC; four one-day regional roundtables held in Western and Atlantic Canada, Ontario, and Quebec (teams participated in one each); and one one-day (postcollaborative) workshop held in Halifax, NS. |
| Foster team planning and cross-site sharing of experiences, for example, through site presentations, breakout sessions, and storyboards | Foster team planning and cross-site sharing of experiences, for example, through site presentations, breakout sessions, and storyboards | |
| Site visits/grand rounds to requested sites (Alberta Health Services, Hamilton Health Sciences, Grey Bruce Health Services, The Ottawa Hospital, Joseph Brant Hospital, and Health PEI). Four celebratory receptions held in Halifax, Toronto, Vancouver, and Burlington | ||
| Content of in-person sessions | Didactic training in a particular care process or practice (e.g. the CCM) and training in quality improvement techniques (e.g. Plan-Do-Study-Act or PDSA cycles). | Curriculum designed to provide teams with content related to EBM for COPD management (e.g. ACP, self-management support, action planning, etc.) and quality improvement (e.g. PDSA cycles, measurement and evaluation, etc.) |
| PDSA cycles* | Most report using PDSAs, but offer little detail as to sites’ experiences during PDSA cycles, how PDSAs were integrated into improvement efforts, or how ongoing data collection informed the QI process. | Faculty delivered content on and encouraged teams to make use of PDSA cycles Combination of EBM and quality improvement methodologies |
| Team calls | Monthly team calls | Monthly all team webinars, one series of 1:1 calls with each team, and coaching calls with select faculty by request of teams |
| Cross-site participation on calls | Cross-site participation on affinity calls | |
| Email or web support | Web-based or email support sometimes offered, but little information as to the extent to which QIC participants relied on this support | Online learning platform for teams; Extranet for faculty, Extranet for industry partner, email support, Microsoft Outlook meeting holds, and CFHI designated a main point of contact for teams |
| QI processes* | Most incorporate ongoing data collection (e.g. performance indicators, ongoing reporting on target outcomes) | Measurement and data collection plans developed to support tracking of core measures (related to QI domains: patient- and family-centeredness, coordination and efficiency) and unique measures (related to appropriateness/effectiveness). Teams adapted the plans to local context, for example, amending standard operating definitions, collection details, and so on as needed |
| In some cases, faculty provide site feedback and received external support for data synthesis and feedback | Two faculty reviewed team measurement plans and provided written feedback. Faculty and staff also provided teams with written and verbal feedback on measurement plans, improvement charters, and portfolio of services worksheets | |
| Teams completed postwebinar surveys for continuous quality improvement and to assess their skills acquisition and other implementation factors | ||
| Organizational involvement | Some report organizational leadership involvement, but not clear if leaders are members of the QI team or engaged via other means | Organizational leadership required to provide executive sign off |
| Few examples of QIC penetration into the broader organization, for example, training of non-QIC team members by either QIC faculty or local QIC members | Sites visits and receptions allowed for introduction of QIC to broader organization and leadership; CFHI-BI support to teams to participate in various conferences (e.g. Canadian Respiratory Conference, National Health Leadership Conference, and so on) to disseminate learnings | |
| Pre-QIC involvement | Few examples of “prework” activities, for example, use of an “expert panel,” a group that finds targets for improvement and plans the collaborative; for example, requiring formal commitments, application or “readiness” criteria | Various prework activity: |
| • Optional informational webinar | ||
| • Required submission of an expression of commitment | ||
| • Required development of an improvement or project charter | ||
| • Required development of a memorandum of understanding between CFHI and each team’s organization |
QIC: quality improvement collaborative; INSPIRED: INSPIRED COPD Outreach Program™; CFHI: the Canadian Foundation for Healthcare Improvement; BI: Boehringer Ingelheim Canada Ltd.; COPD: chronic obstructive pulmonary disease; CCM: chronic care model; PDSA: Plan-Do-Study-Act; EBM: evidence-based medicine; ACP: advance care planning. “*” indicates Most common QIC components (as per Nadeem et al 2013); indicates alignment; indicates additional feature added by CFHI.
{kind=link}