
Abstract
Chronic obstructive pulmonary disease (COPD) patients often experience lower limb muscle dysfunction and wasting. Exercise-based training has potential to improve muscle function and mass, but literature on this topic is extensive and heterogeneous including numerous interventions and outcome measures. This review uses a detailed systematic approach to investigate the effect of this wide range of exercise-based interventions on muscle function and mass. PUBMED and PEDro databases were searched. In all, 70 studies (n = 2504 COPD patients) that implemented an exercise-based intervention and reported muscle strength, endurance, or mass in clinically stable COPD patients were critically appraised. Aerobic and/or resistance training, high-intensity interval training, electrical or magnetic muscle stimulation, whole-body vibration, and water-based training were investigated. Muscle strength increased in 78%, muscle endurance in 92%, and muscle mass in 88% of the cases where that specific outcome was measured. Despite large heterogeneity in exercise-based interventions and outcome measures used, most exercise-based trials showed improvements in muscle strength, endurance, and mass in COPD patients. Which intervention(s) is (are) best for which subgroup of patients remains currently unknown. Furthermore, this literature review identifies gaps in the current knowledge and generates recommendations for future research to enhance our knowledge on exercise-based interventions in COPD patients.
Introduction
Chronic obstructive pulmonary disease (COPD) is a lung disease characterized by persistent airflow limitation. 1 Nevertheless, many patients with COPD also commonly experience systemic features, such as impaired lower limb muscle function and muscle wasting. 2 Cross-sectional research has reported that quadriceps strength is reduced by 20–30% in patients with COPD. 2 This observed decrease in strength is proportional to the decrease in muscle mass in the majority of patients with COPD, suggesting the onset of disuse-related muscle atrophy instead of myopathy-related muscle atrophy. 3 In line with this reasoning, patients with COPD generally are less physically active compared to healthy peers, 4,5 which is directly related to lower limb muscle dysfunction. 6 A decreased quadriceps endurance has also been established in COPD but is more variable across studies because of differences in test procedures. 2 This lower limb muscle dysfunction clearly contributes to the observed exercise intolerance and exercise-induced symptoms of dyspnea and fatigue in patients with COPD. 7 Moreover, lower limb muscle dysfunction has been associated with a worse health status, more hospitalizations, and worse survival. 2
In turn, exercise-based interventions have the potential to reverse or at least stabilize lower limb muscular changes in patients with COPD. 2,8 Exercise-based pulmonary rehabilitation programs are a cornerstone of the comprehensive care of patients with COPD. 9 Indeed, international guidelines state that exercise training is the best available nonpharmacological therapy to improve lower limb muscle function and muscle mass in these patients. 9,10 The comprehensive American Thoracic Society/European Respiratory Society (ATS/ERS) statement provides only a short overview of the effects of exercise-based therapies on muscle function and muscle mass in patients with COPD, 2 whereas actually the literature about this topic is extensive and heterogeneous including numerous interventions and outcome measures. A critically appraised and detailed overview of the impact of this wide range of exercise-based therapies on lower limb muscle function and muscle mass in patients with COPD is presented in this narrative review.
Methods
Inclusion and exclusion criteria
The included studies investigated the effects of any exercise training intervention on lower limb muscle strength, endurance, and mass in clinically stable patients with COPD. Studies investigating the muscle response to a single exercise test or a single exercise session were excluded. Studies that specifically investigated the effect of an additional intervention on top of exercise training were also excluded. The selected studies needed to include original data, but there were no restrictions regarding study design or muscle strength, endurance, and mass assessment used. Only studies published in English were included.
Search methods
Electronic databases PUBMED and PEDro were searched for articles published from inception until March 7, 2016. In PUBMED, the following search strategy was used: COPD AND (exercise OR exercise training OR rehabilitation OR pulmonary rehabilitation OR physical activity OR aerobic training OR endurance training OR resistance training OR strength training OR cycling OR walking OR neuromuscular electrical stimulation OR NMES OR magnetic stimulation). The search strategy was adapted to “COPD” alone when searching in PEDro to identify all relevant articles. Corresponding authors were contacted to provide full texts when not accessible via electronic databases. Reference screening of available reviews in the same field of research was also performed to expand the search for eligible articles.
Selection of studies
Two reviewers (JDB and CB) performed the study screening based on the listed inclusion and exclusion criteria. In the first phase, both reviewers conducted a part of the title screening in a conservative manner, excluding only titles that undoubtedly did not fulfill the criteria. Next, both reviewers screened all remaining abstracts independently. Results were compared, discrepancies between reviewers were discussed, and a consensus-based decision was taken. Finally, full-text screening was performed in a similar way.
Data extraction
Information on sample size, study design (for studies comparing COPD with other disease states, only the data from patients with COPD is shown and the design described as single group pre post-test), baseline forced expiratory volume at first second (FEV1), age, exercise training parameters (frequency, intensity, modality, session and program duration), assessment modality, and relevant outcome measures of muscle strength, muscle endurance, and muscle mass were extracted from the articles. Mean relative change (percentages of baseline) between pre- and postmeasurements were extracted. If mean relative change (expressed as percentage of baseline) was not available, pre- and postvalues were used to manually calculate mean relative change as percentage of baseline: ([post – pre]/pre x 100). All extracted data are presented in Tables 2–7 (according to training modality) and Figures 1 –7. For Figure 4, a weighted mean relative change (percentage of baseline) was calculated per study as followed:

Assessment of methodological quality of RCTs and non-randomized controlled trials based on the PEDro scoring system. Studies are ranked alphabetically.

Aerobic training.

ns: not significant; RCT: randomized controlled trial; FEV1: forced expired volume in 1 second; MVC: maximum voluntary contraction; BIA: bioelectrical impedance analysis; Wpeak/max: peak/maximal workload.
aMeasured via strain-gauge system.
bMeasured via computerized dynamometer (e.g. Biodex).
cBetween groups difference based on post training values.
Resistance training.

ns: not significant; RCT: randomized controlled trial; RM: repetition maximum; FEV1: forced expired volume in 1 second; RPE: rate of perceived exertion; MVC: maximum voluntary contraction; CSA: cross-sectional area; MRI: magnetic resonance imaging; DEXA: dual energy x-ray absorptiometry.
aMeasured via strain-gauge system.
bMeasured via computerized dynamometer, for example, Biodex.
cMeasured via hand-held dynamometer.
dBetween groups difference based on post training value.
eOnly absolute values available.
Combined aerobic and resistance training.

ns: not significant; RCT: randomized controlled trial; RM: repetition maximum; FEV1: forced expired volume in 1 second; FFM: fat free mass; ISWT; incremental shuttle walk test; MVC: maximum voluntary contraction; Wpeak/max: peak/maximal workload; 6MWT: 6-minute walking test; MRI: magnetic resonance imaging; AT/VT: anaerobic/ventilatory threshold; CSA: cross-sectional area; RPE: rate of perceived exertion.
aMeasured via strain-gauge system.
bMeasured via computerized dynamometer, for example, Biodex.
cMeasured via hand-held dynamometer.
dMeasured via pushing against force platform.
eBetween group difference based on post training value.
fOnly absolute values available.
gData not reported.
Neuromuscular electrical stimulation and magnetic stimulation training.
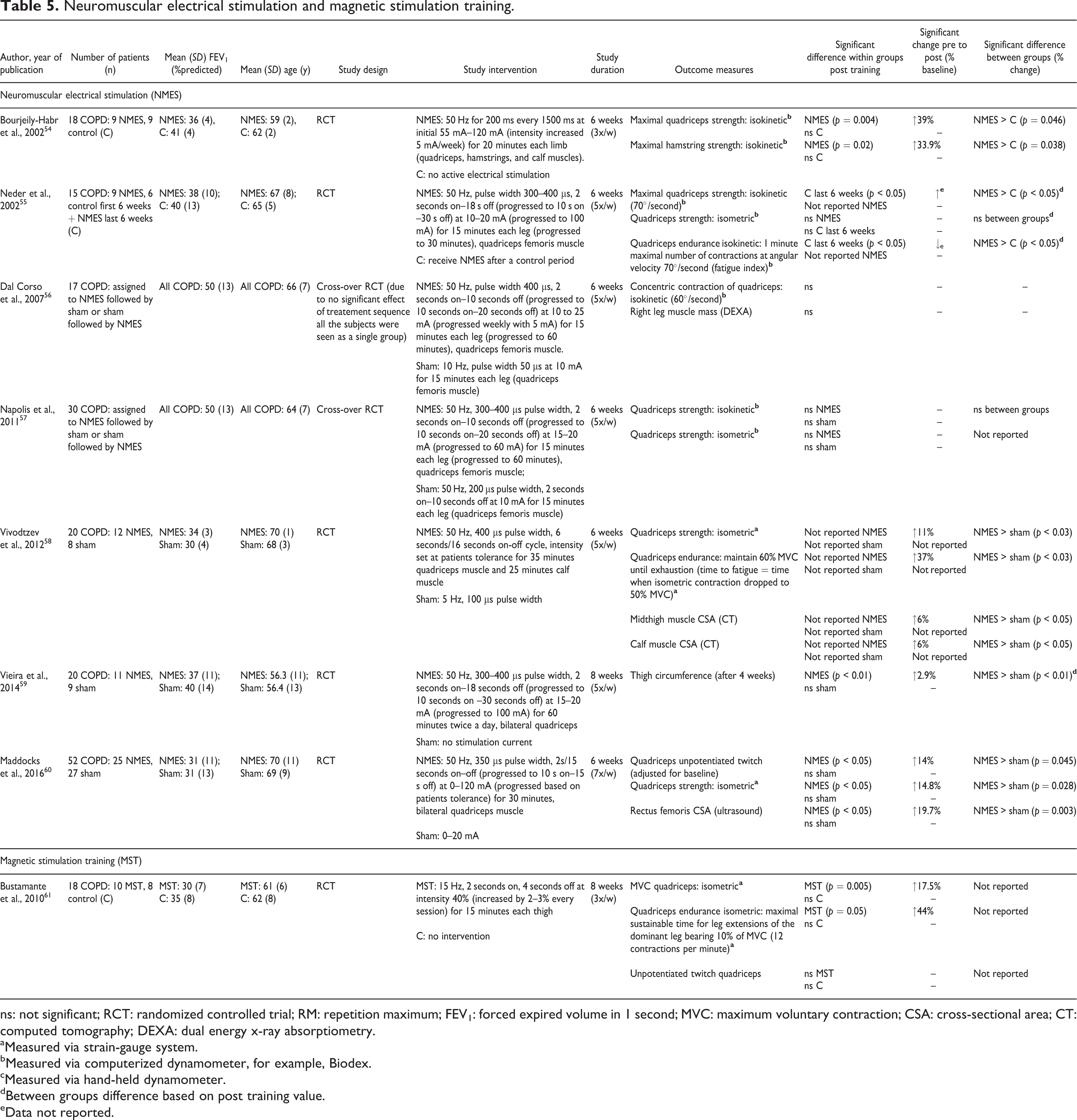
ns: not significant; RCT: randomized controlled trial; RM: repetition maximum; FEV1: forced expired volume in 1 second; MVC: maximum voluntary contraction; CSA: cross-sectional area; CT: computed tomography; DEXA: dual energy x-ray absorptiometry.
aMeasured via strain-gauge system.
bMeasured via computerized dynamometer, for example, Biodex.
cMeasured via hand-held dynamometer.
dBetween groups difference based on post training value.
eData not reported.
Other training modalities.

ns: not significant; RCT: randomized controlled trial; RM: repetition maximum; FEV1: forced expired volume in 1 second; MRI: magnetic resonance imaging; HR: heart rate.
aMeasured via strain-gauge system.
bMeasured via computerized dynamometer, for example, Biodex.
cMeasured via hand-held dynamometer.
dIncremental knee-extension protocol.
eBetween groups difference based on post training value.
Comparing studies.

ns: not significant; RCT: randomized controlled trial; RM: repetition maximum; FEV1: forced expired volume in 1 second; pt: points improvement on manual muscle testing scale 0–5; RPE: rate of perceived exertion; MET: metabolic equivalent; HF/LF NMES: high/low frequency neuromuscular electrical stimulation; MCSA: muscle cross-sectional area; CT: computed tomography; Wpeak/max: peak/maximal workload; 6MWT: 6-minute walking test; HRR: heart rate reserve; HR: heart rate; MMT : manual muscle testing.
aMeasured via strain-gauge system.
bMeasured via computerized dynamometer, for example, Biodex.
cMeasured via hand-held dynamometer.
dBetween groups difference based on post training value.
eOnly absolute values available.

Study flowchart from identification of articles to final inclusion (based on the Prisma flowchart template). IC: inclusion criteria; NMES: neuromuscular electrical stimulation; MST: magnetic stimulation training.

A) Pie chart depicting an overview of muscle strength measures used across the 70 included studies. B) Pie chart depicting an overview of used isometric strength assessment modalities. MMT: manual muscle testing; uptwitch: unpotentiated twitch; ptwitch: potentiated twitch.

A) Pie chart depicting an overview of muscle endurance measures used across the 70 included studies. B) Pie chart depicting an overview of muscle mass assessment modalities across the 70 included studies. MRI: magnetic resonance imaging; DEXA: dual energy x-ray absorptiometry; BIA: bioelectrical impedance analysis; CT: computed tomography.
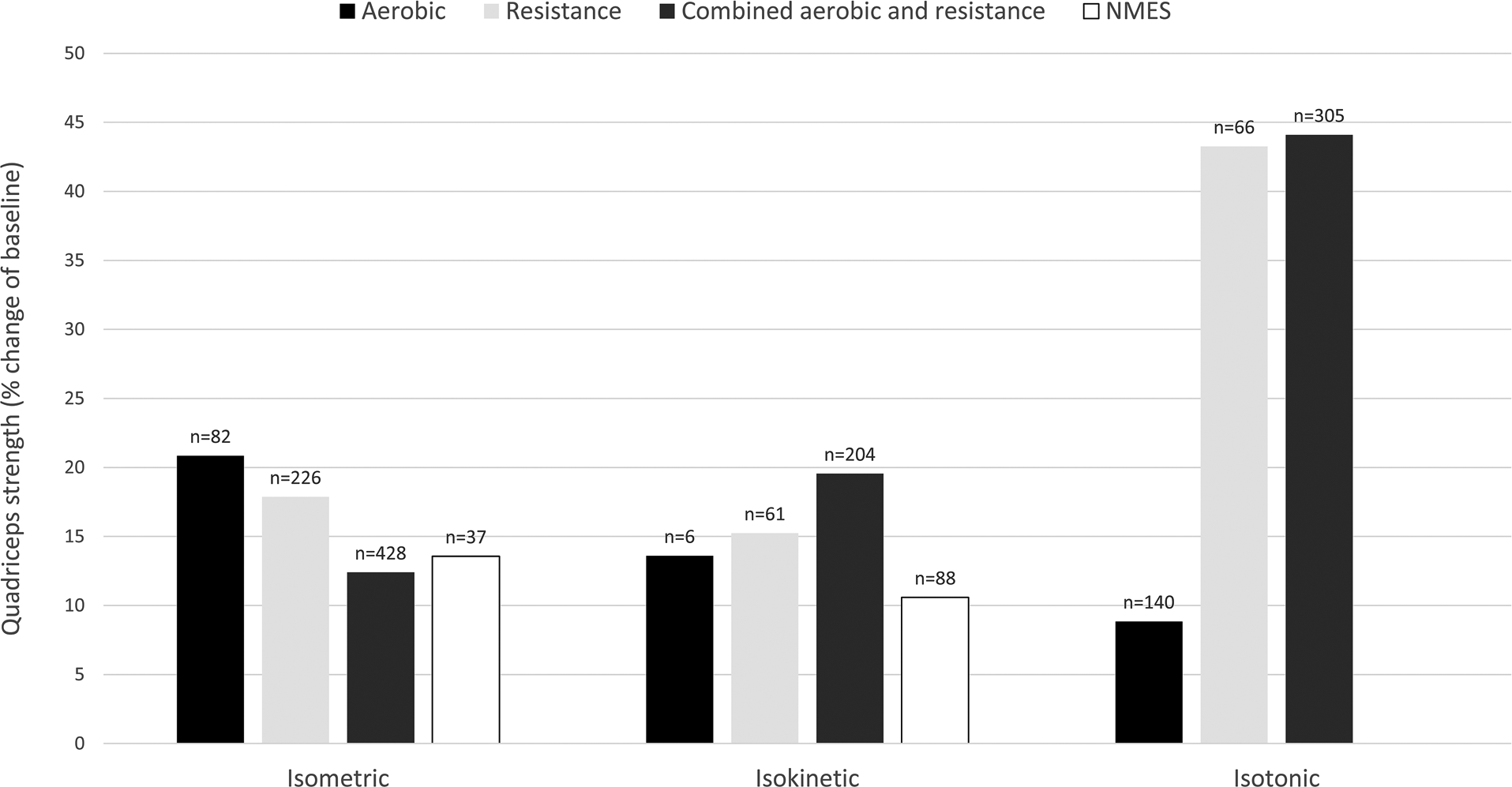
Effect of aerobic, resistance, combined aerobic and resistance training and NMES on various measures of quadriceps strength in patients with COPD expressed as weighted means of relative change (percentage of baseline). Values on top of the bars are the number of patients with COPD. NMES: neuromuscular electrical stimulation.
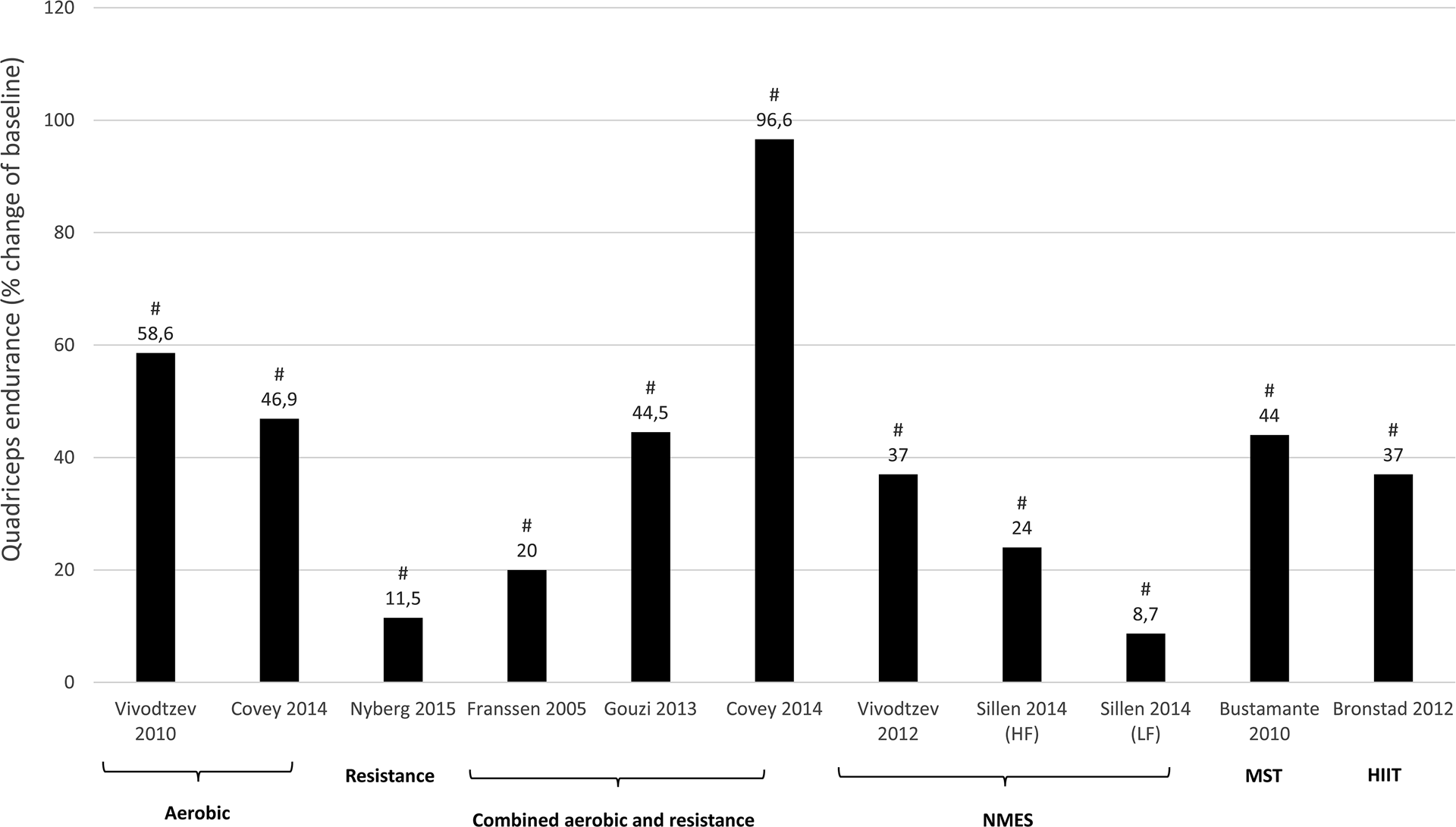
Effect of different exercise interventions on quadriceps endurance in patients with COPD expressed as mean of relative change (percentage of baseline). NMES: neuromuscular electrical stimulation; HF: high-frequency NMES; LF: low-frequency NMES; HIIT: high-intensity interval training. #Significant change from baseline (within group effect: P < 0.05).

Effect of different exercise interventions on muscle mass in patients with COPD expressed as mean of relative change (percentage of baseline). T: thigh; LL: lower-limb; Q: quadriceps; RF: rectus femoris; IT: individualized training; NIT: non-individualized training; NMES: neuromuscular electrical stimulation; HIIT: high-intensity interval training; DEXA: dual energy x-ray absorptiometry; MRI: magnetic resonance imaging; CT: computed tomography; BIA: bioelectrical impedance analysis. #Significant change from baseline (within group effect: P < 0.05).

Effect of different exercise interventions on isotonic quadriceps strength in patients with COPD expressed as mean of relative change (percentage of baseline). §Significantly different with aerobic training (P < 0.05 - between group effect).
(e.g. study 1, with x1 = mean relative change (percentage of baseline) and n1 = number of patients). Subsequently, an overall weighted mean per training modality and per outcome measure was calculated:

Quality assessment
Methodological quality of randomized controlled trials (RCT) or nonrandomized controlled trials were assessed (Table 1). The PEDro scale, based on the Delphi list and “expert consensus,” was used as a tool to assess the quality of the studies. 81,82 PEDro scores were obtained from the PEDro database. If a study was not found in the PEDro database, PEDro scores were calculated for that study by two reviewers (JDB and CB). Eleven quality criteria received a “yes” or “no” answer and were summed (criteria 1 is not used in the calculation) to a maximum score of 10 points. 82 Studies were considered of “good” to “excellent” quality when scoring ≥6 points on the PEDro scale. Studies scoring ≤5 points were defined as “low” to “fair” quality studies. 83 Studies using a single group design with or without a healthy control group following a similar intervention were not assessed.
Results
Search results
The study selection process is outlined in Figure 1. We identified 9933 articles with our search strategy. After title screening, 8843 articles were excluded, resulting in 1090 remaining articles for abstract screening. Reference screening of review papers delivered 10 more eligible articles. Finally, 162 full-text articles were screened, of which 92 articles were excluded. The remaining 70 articles (n = 2504 patients with COPD; n = 2124 exercise training, n = 380 control) were established as eligible to be used in our review.
Quality assessment
Pedro scores of RCTs and non-RCTs are given in Table 1. Of the 40 assessed studies, 17 studies scored between 6 and 8 points and are considered to be studies of “good” quality. In all, 23 studies scored ≤ 5 points, with 18 studies scoring 4 or 5 points (“fair” quality), and 5 studies ≤ 3 points which is considered “low” quality. The criteria of concealed allocation, blinding of assessors, adequate follow-up, and intention-to-treat analysis were often not fulfilled. One non-RCT was not assessed because of its retrospective nature. 65 The other 29 studies used a single group design with (n = 4) or without (n = 25) a healthy control group that followed a similar intervention (Table 1).
Results per outcome measure
Outcome measures
Muscle strength can be categorized into voluntary strength, that is, isometric, isokinetic, and isotonic strength, and involuntary strength. Isometric strength is defined as a static contraction without a change in muscle length. Isokinetic strength is determined as dynamic strength while maintaining a constant speed. Isotonic strength is defined as dynamic strength with maintaining constant force while changing the length of the muscle. Involuntary strength is assessed by electrically or magnetically stimulating a peripheral nerve, resulting in an unpotentiated twitch (rest) or potentiated twitch (performed seconds after a maximum voluntary contraction). An overview of muscle strength measures used across the 70 included studies is given in Figure 2 (A). Isometric strength measures were used most frequently (43%), followed by isotonic (28%), and isokinetic (21%) strength measures. Manual muscle testing and involuntary strength measures were rarely used. Isometric strength assessment modalities are depicted in Figure 2 (B) and were dominantly performed by strain gauge, followed by computerized dynamometer, handheld dynamometer, force plate, or an unknown device. Used measures of muscle endurance and assessment modalities of muscle mass varied strongly and are depicted in Figure 3.
Results per outcome measure
All studies wherein percentage change from baseline was available or where percentage change from baseline was calculated by the reviewers are presented per outcome measure in Figures 4 –7. Weighted means for changes from baseline for isometric, isokinetic, and isotonic strength are depicted for aerobic, resistance, combined aerobic and resistance training, and neuromuscular electrical stimulation (NMES) in Figure 4. Overall, isometric quadriceps strength increased with 15%, isokinetic quadriceps strength with 17%, and isotonic lower limb strength with 34% (Figure 4). Quadriceps endurance improved with 8.7–96.6% (Figure 5) and quadriceps muscle mass with 4.2–12.1% (Figure 6). Comparisons in isotonic lower limb strength between aerobic, resistance and combined aerobic, and resistance training are presented in Figure 7.
Results per training modality
Different exercise training modalities were used to investigate the effect of exercise-based therapy on muscle function and muscle mass (Figure 1). A detailed overview is given in the following sections. More information on the characteristics of the different studies grouped per training modality are given in Tables 2–7.
Aerobic training (Table 2)
Muscle strength
Isometric strength: Four studies showed an increase of 10–21% in isometric quadriceps strength after training.
11,12,14,15
In contrast, one study reported no significant change in isometric quadriceps strength.
16
Significant between-group differences in the change in isometric quadriceps strength were reported in favor of the training group compared to the nonexercising COPD control group.
15
Isokinetic strength: One study measured isokinetic quadriceps strength which increased with 13.6% after training in patients.
13
Isotonic strength: Isotonic hamstring muscle strength was measured by 1RM leg curl and increased with 50% after training, while in the COPD control group no significant change was reported.
17
The difference between groups was however not significant.
17
Involuntary strength: Involuntary contraction of the quadriceps muscle produced by magnetic stimulation of the nervus femoralis and measured as potentiated and unpotentiated twitch showed a significant increase of 8.8% and 9.7% after training, respectively.
12
In contrast, another study reported a nonsignificant increase in potentiated twitch after training.
14
Muscle endurance
Isometric endurance: A study showed a nonsignificant increase in isometric knee extension endurance, measured as holding an isometric contraction at 50% of maximum until exhaustion.
11
Isokinetic endurance: An increase of 58.6% in quadriceps muscle endurance, measured as dynamic repeated leg extension with weights corresponding to 30% MVC until exhaustion, was reported in one study. This change was significantly greater compared to the nonexercising control group.
15
Muscle mass
Resistance training (Table 3)
Muscle strength
Isometric strength: Six studies showed a significant increase of 13.2–25.4% in isometric quadriceps strength after resistance training.
17,18,20,23
–25,27
Two studies also reported a significant difference in isometric quadriceps strength between training group and control group in favor of training.
20,22
One study, however, did not report a significant increase in isometric quadriceps muscle strength after training.
26
Two studies measured isometric hamstrings muscle strength, all showing a significant increase of 11.4–19.0%.
27,26
Isometric hip abductor strength was not significantly different after training between the training group and the control group
22
. The study of Ramos et al. did not report a significant difference in isometric strength of knee flexors and knee extensors between 8 weeks of conventional resistance training and elastic tube resistance training.
27
Isokinetic strength: Three studies showed a significant increase of 8.0–25.2% in isokinetic peak torque (Nm) after training.
24,20,28
One study, however, reported no significant increase in isokinetic peak torque.
80
Significant between-group differences in isokinetic peak torque were in favor of training compared to control in two studies.
20,28
In one study, however, no significant difference between training and control group was reported in isokinetic peak torque.
19
Isotonic strength: Isotonic quadriceps strength measured by 1RM leg press showed an increase of 16.0–27.1% after training.
18,21
Between group differences were also significant in favor of training compared to control.
18,21
A 5RM leg press was also measured in one study and increased with 34.5% after training, which was significantly different compared to control.
20
A 1RM leg extension increased with 44% after resistance training in patients with COPD, which was significantly different compared to control in favor of training.
18
Muscle endurance
Isokinetic endurance: Isokinetic total work during 30 consecutive knee extension repetitions was significantly increased with 11.5%, which was significantly different with controls.
28
Another study reported a significant increase of 320 J in isokinetic total work during 60 seconds of knee extension repetitions in patients with COPD after training which was also significantly different with controls.
19
Isotonic endurance: Isotonic muscle endurance of the lower limbs with external loading increased with 25 repetitions performed in 30 seconds in the training group compared to the control group.
80
Muscle mass
One study reported a significant 4.2% increase in cross-sectional area (CSA) of the quadriceps, measured by magnetic resonance imaging (MRI), which was not different compared to nonexercising COPD controls. 20 Two other studies measured thigh lean mass with dual-energy x-ray absorptiometriy (DEXA) and reported a 5.7–7.3% increase after resistance training. 24,25 Menon et al. also measured an increase of 21.8% in m. rectus femoris CSA and 12.1% in quadriceps thickness via ultrasound after training. 25
Combined aerobic and resistance training (Table 4)
Muscle strength
Isometric strength—A significant increase of 7.0–32.0% in isometric quadriceps strength after training was reported in seven studies,
34,35,37,38,42,44,49
with one study only stating significant improvement without showing data.
45
Two studies reported no significant change in isometric quadriceps strength after training.
30,40
Three studies reported significant differences between the training and the control group in favor of training,
37,29,46
while one other study reported no significant difference between training and control group.
39
Nonsignificant differences were also reported between sarcopenic and nonsarcopenic patients,
50
between patients with or without contractile muscle fatigue,
44
between trained patients with COPD and trained healthy controls,
45
and between hypoxemic and normoxemic patients.
49
Isokinetic strength: Five studies measured isokinetic quadriceps strength after training showing a 8.3–30% increase in peak torque.
31
–33,36,41
One study also measured isokinetic hamstring strength of the right and the left leg which increased with 20.2% and 42.1%, respectively.
32
Isotonic strength: One study measured isotonic strength as 1RM after training, showing a 33.9% increase in leg extension 1RM after high-intensity training which was significantly different with low-intensity training.
43
No significant change was established after low-intensity training.
43
Four studies measured isotonic quadriceps strength via 10RM, with three studies showing a 63.4–96.9% increase in 10RM leg extension,
48,51,52
while another study reported a 71.0% increase in 10RM weightlifting after training.
53
A 15RM leg press was measured in one study, with a mean change of 16 kg reported after training, which was significantly different with controls whom did not show a significant change.
37
Muscle endurance
Isokinetic endurance: Quadriceps fatigue as a proportional decline of isokinetic peak torques during 15 sequential voluntary maximal contractions at an angular velocity of 90°/second was measured and improved with 20% after training.
33
Isotonic endurance: A study measured an increase of 44.5% in time to exhaustion during dynamic contractions at 30% maximal voluntary contraction (MVC) at a rate of 10 movements per minute after training.
45
Muscle mass
Quadriceps CSA, measured via MRI, was reported to increase with 7% after combined aerobic and resistance training. 35 Another study compared CSA of m. rectus femoris, measured via ultrasound, between a nonindividualized low-intensity and individualized training group. Muscle mass improved significantly with 8.6% after individualized training but not after nonindividualized low-intensity training. Between group differences were however not significant. 47
Neuromuscular electrical stimulation and magnetic stimulation training (Table 5)
Muscle strength
Isometric strength: Two studies reported an 11–14.8% increase in isometric quadriceps strength after NMES,
58,60
which was significantly different between NMES and sham after 6 weeks in favor of NMES.
58,60
Two other studies did not report a significant increase after NMES,
55,57
with one study also reporting no significant differences between NMES and control after the training protocol.
55
Magnetic stimulation training (MST) increased isometric quadriceps strength with 17.5%.
61
Isokinetic strength: Peak torque increased and was significantly different with controls in favor of NMES after the training protocol,
55,54
wherein one study with 39.0%
54
while the other study did not report significant data.
55
Two studies did not report a significant increase after NMES
56,57
with also no significant difference between NMES and sham after the training protocol.
57
Hamstrings peak torque showed a 33.9% increase after NMES which was significantly different with controls in favor of NMES.
54
Involuntary strength: Unpotentiated twitch after NMES was reported to be significantly increased with 14% which was significantly different between NMES and sham after 6 weeks in favor of NMES after adjustment for baseline.
60
Unpotentiated twitch after MST showed no significant increase in both the intervention and the control group.
61
Muscle endurance
Isometric endurance: A NMES study measured time to exhaustion after an endurance test (isometric contraction at 60% MVC) and reported a 37% increase in time to exhaustion after NMES, which was significantly different with the control group
58
. After MST, quadriceps muscle endurance was increased with 44%. Muscle endurance was measured as time to exhaustion for isometric leg extensions at 10% MVC with 12 contractions per minute.
61
Isokinetic endurance: The fatigue index after a quadriceps muscle endurance isokinetic test (maximal number of contractions in 1 minute) was reported to be decreased which was significantly different between NMES and controls in favor of NMES.
55
Muscle mass
A 6% increase in mid-thigh and calf muscle mass was reported, which was significantly different between NMES and sham in favor of NMES, measured by computed tomography (CT). 58 In contrast, another study reported no increase in leg muscle mass, measured by DEXA, after NMES. 56 A third study measured thigh circumference and reported a significant 2.9% increase, which was significantly higher compared to the control group. 59 Another recent study measured rectus femoris CSA via ultrasound after NMES and reported a significant increase of 19.7%, which was significantly different between NMES and sham in favor of NMES. 60 (Table 6)
Other training modalities (Table 6)
High-intensity interval training
One study performed high-intensity interval knee-extensor training in patients with COPD (Table 6). Muscle endurance of the quadriceps, measured as peak work during an incremental knee-extensor protocol with 2 W increments every 3 minutes, increased with 37.0% after training. 62 Muscle mass, measured with MRI, did not increase significantly after HIIT of the knee extensors. 62
Whole-body vibration training
Two studies implemented whole-body vibration training (WBVT) as their training stimulus (Table 6) 63,64 . In one 6-week WBVT study, isokinetic strength of the quadriceps and hamstrings did not increase significantly after WBVT and was not significantly different between WBVT and control group after the intervention. 63 Another 12-week study implemented WBVT or resistance training. Only the resistance training group increased their isometric quadriceps strength significantly with 10.5%. However, no significant differences between WBVT and resistance training were established after the intervention (Table 6). 64
Water-based training
One study compared water-based with land-based pulmonary rehabilitation 65 (Table 6). Aerobic and resistance components of training were similar for both water and land-based training. The 6RM knee extension (92.7% and 68.0%) and 6RM hip flexion (85.8% and 82.7%) increased significantly after both water- and land-based training, respectively. Between group differences were not significant (Table 6). 65
Comparing aerobic, resistance and combined aerobic and resistance training (Table 7)
Aerobic versus resistance training
Isometric knee extension peak torque was compared after 12 weeks aerobic versus resistance training and increased significantly with 42% versus 20% respectively, which was significantly different between the two training modalities. 68 Isometric knee flexion force increased 28% versus 31%, respectively, 68 while isometric knee extension force only increased significantly (35%) after resistance training. 68
Aerobic versus combined aerobic and resistance training
Significant increases were found after combined aerobic and resistance training (20%) and aerobic training alone (7.8%) in isotonic quadriceps strength in favor of combined aerobic and resistance training. 66 In contrast, isotonic quadriceps strength did not increase significantly after aerobic training compared to a significant 9–36.5% increase after combined aerobic and resistance training in four other studies. 69 –71,76 A similar phenomenon was reported for isotonic hamstring strength. 69 One study, however, reported no significant increases in isotonic quadriceps strength after both aerobic and combined aerobic and resistance training. 72 Solely one study compared muscle mass between different training modalities and reported a significantly increased bilateral thigh MCSA, measured by CT, with 8% after combined aerobic and resistance training but not after aerobic training alone. 66 Between group differences were significant and in favor of combined aerobic and resistance training. 66
Aerobic versus resistance versus combined aerobic and resistance training
A study reported a significant increase of 20.5%, 52.8%, and 52.8% in isotonic quadriceps strength after both aerobic, resistance, and combined aerobic and resistance training, respectively. 67 Isotonic hamstring strength also showed significant increases after all three training modalities. 67 Significant between group differences identified a greater increase in quadriceps and hamstring strength after resistance training and combined aerobic and resistance training compared to aerobic training. 67 Similar significant between group differences were reported in the study of Vonbank et al., where the aerobic training group did not improve its isotonic quadriceps strength significantly. 74
Training modality sequence
One study investigated the sequence of training modalities and reported that 8 weeks of resistance training followed by 8 weeks of aerobic training increased the sum of 1RM of lower limb exercises with 26.7%. Comparable significant results were found after 8 weeks of combined aerobic and resistance training which increased the 1RM sum with 27.7%, while 8 weeks of aerobic training only increased the 1RM sum with 13.3%. 75 Isotonic muscle endurance, measured by repeated leg extensions at 60% of 1RM (12 repetitions per minute) until exhaustion, increased significantly after resistance training followed by aerobic training (+ 173.8%) but also after combined aerobic and resistance training (+96.6%) and after aerobic training (+46.9%). 75 Both resistance training followed by aerobic training and combined aerobic and resistance training increased muscle endurance significantly more compared to the aerobic training group. 75
Resistance training versus low-intensity training
Resistance training increased leg press and leg extension 1RM with 58.2% and 44.4% compared to no significant changes after low-intensity training. Resistance training combined with low-intensity training increased leg press and leg extension with 48.7% and 21.2%, respectively. 73 Between group differences established that adding resistance training significantly increases strength more compared to low-intensity training alone. 73
Comparing NMES with other training modalities (Table 7)
NMES versus aerobic training
Ten weeks of high-frequency NMES (HF-NMES) (50 Hz) versus 8 weeks of aerobic training (treadmill walking and cycling) in patients with severe COPD 78 increased the quadriceps manual muscle testing (MMT) score significantly in both groups with no significant differences between the groups. 78
NMES versus resistance training
Sillen et al. compared resistance training (4 sets of 8 reps leg extension and leg press at 70% of 1RM) to low-frequency NMES (LF-NMES) (15 Hz) and HF-NMES (75 Hz) 77 and reported significant increases in isokinetic quadriceps peak torque after HF-NMES (13.7%) and resistance training (8.3%). Isokinetic quadriceps peak torque was significantly different between HF-NMES and LF-NMES with the latter showing no significant changes. 77 Quadriceps endurance was measured as total work (J) during an isokinetic test, which increased significantly after HF-NMES (24.0%), LF-NMES, (8.7%) and resistance training (16.3%). Total work after HF-NMES was however significantly higher compared to total work after LF-NMES. 77
NMES as add-on intervention
One other study investigated the effect of adding HF-NMES (50 Hz) to a 10-week combined aerobic and resistance training program. 79 Quadriceps strength, measured with a 1RM test, significantly increased with 18.4% and 31.0% in the NMES group and the sham NMES group, respectively. No differences in quadriceps strength were reported between the addition of NMES or sham NMES to combined aerobic and resistance training in patients with COPD. 79
Discussion
This is the first review of the English-language, peer-reviewed literature that summarizes in detail the changes in lower limb muscle function and muscle mass after exercise-based training interventions in patients with clinically stable COPD. Despite the large heterogeneity in exercise training interventions and outcome measures used, most exercise-based trials showed improvements in lower limb muscle strength, muscle endurance, and muscle mass in patients with COPD, which proves again the utter importance of exercise training during pulmonary rehabilitation.
Methodological considerations
Generally, lower limb muscle function and mass improved in patients with COPD following the exercise-based interventions. Nevertheless, multiple methodological considerations need to be discussed.
Large variation in exercise-based interventions
In total, 70 articles were identified describing a variety of exercise-based interventions. Indeed, the impact of treadmill or outdoor walking, stationary cycling, resistance training, elastic tube training, HIIT, NMES, MST, WBVT, water-based training, or a combination thereof on lower limb muscle function and mass have all been assessed in patients with COPD. Which intervention(s) is (are) best for which subgroup of patients remains currently unknown. To date, only a limited number of studies that assessed effects of exercise-based interventions on muscle function/mass have specifically recruited patients with COPD based on the degree of lower limb muscle dysfunction/atrophy. 68,77 For example, resistance training and NMES are safe and very effective in COPD patients with severe dyspnea and lower limb muscle weakness at the start of the program. 84,85 The low burden on the impaired ventilatory system may be another reason to select NMES or resistance training to improve limb muscle function/mass in severely dyspneic COPD patients. 86,87 The purposes of resistance training and NMES also reach the acute care setting and both training modalities seem viable and effective in increasing muscle function and mass in unstable patients that are hospitalized due to a severe COPD exacerbation. 88 –94 This evokes physiotherapists to implement these exercise-based interventions during and after hospitalization to counteract muscle weakness and wasting.
If the aim is to increase lower limb muscle function/mass, resistance training may be a better training modality than aerobic training. 67,74 This fits with an important training principle: specificity, which means that both acute exercise responses and training adaptations are highly specific to the type of activity and to the volume and intensity of the exercise performed. 95 It is especially important when aiming to achieve a specific goal, for example, increased muscle strength. 95 Interestingly, increases in lower limb muscle function (Figures 4 and 5) and mass (Figure 6) also occurred after walking/cycling training in patients with COPD. 3,11 –15,17,67,68,73,75,78 These cross-over training effects have also been observed in healthy elderly 96,97 and patients with chronic heart failure. 98,99 It can be hypothesized that high-intensity (whole-body and local) aerobic exercises are sufficient to induce significant morphological (e.g. it can counteract skeletal muscle atrophy) and functional changes related to the force generating capacity of the skeletal muscles in healthy elderly subjects and in patients with COPD or congestive heart failure. Nevertheless, it should be noted that aerobic training combined with resistance training resulted in significantly greater improvements in skeletal muscle force and in muscle CSA of the mid-thigh compared to aerobic training alone in patients with COPD (Figure 7). 3,67,69,70,71,74,75 Thus, when patients with COPD are able to perform combined aerobic and resistance training, this may be the preferred choice of exercise training modality.
Another popular training modality in healthy adults, but still less used in patients with COPD is HIIT. Whole body HIIT (e.g. cycling) has been shown to improve muscle fiber proportion (type I and IIA increase, type IIB decrease), fiber size, and capillary to fiber ratio in lower limb muscle regardless of GOLD stage and presence/absence of cachexia. 8,100 –103 Local muscle HIIT induced improvements in quadriceps endurance, citrate synthase activity, and mitochondrial respiration capacity. 62 Muscle mass, however, did not increase after local muscle HIIT. 62 Measurements of muscle strength have not yet been performed in patients with COPD after HIIT. It seems likely that HIIT training will mostly affect the aerobic capacity, but in light of the cross-training effects on muscle strength seen after aerobic training it seems worth to investigate the effect of HIIT on muscle strength.
All studies reported a rather large variation in the muscle response to the various interventions. In light of this, in 17%, 8%, and 13% of cases where quadriceps strength, quadriceps endurance, and lower-limb mass, respectively, were measured, a nonsignificant increase compared to baseline values was reported. This suggests that not all patients may benefit to the same extent from a similar exercise-based intervention, and/or patients perform the exercise-based intervention to a different extent, which, in turn will give a different response in change in muscle function and muscle mass. This variation in response is also reported in healthy elderly. 104 A similar phenomenon is also seen in the combined aerobic and resistance training study of Jones et al., where sarcopenic patients increased significantly their quadriceps strength while nonsarcopenic patients did not. 50 It is however specifically striking for NMES interventions because NMES protocols did not differ greatly compared to the other NMES studies with significant results. Whether this is a variation in individual response to NMES dependent on disease severity or attributed to poor compliance to the treatment in the home setting remains to be elucidated. In general, for all exercise-based therapies, to date in-depth analyses of responders and nonresponders in muscle function/mass following an exercise-based intervention have not been performed in patients with COPD. Only then statements can be made about which underlying mechanisms (e.g. genetics, training intensity, training duration, disease severity, degree of sarcopenia, compliance, etc.) are responsible for this nonresponse.
Large variation in the methodology used to assess lower limb muscle function and mass
Lower limb muscle function can be assessed using various methodologies, using different outcomes. Some are effort dependent (isometric, isokinetic, and isotonic testing) and others are not (n. femoralis magnetic stimulation). Even within a specific muscle testing approach, for example, isokinetic muscle endurance testing, different protocols exist. Robles et al. also stipulate that standardization is necessary to acquire reliable and valid muscle function measures. 105 Indeed, to enable benchmarking between studies/centers and to perform a meta-analysis, standardization of the muscle testing methodology needs to take place. The Official ATS/ERS statement on limb muscle dysfunction in COPD proposes to use a strain gauge to measure isometric quadriceps peak torque. 2 Indeed this method is commonly used in the research setting, but whether and to what extent this method has been implemented in daily clinical practice remains currently unknown. Furthermore, without standardization of testing procedures, it is difficult to make conclusions about which increase in muscle function/mass is actually clinically relevant. To the authors’ knowledge, there is no minimal clinically important difference (MCID) developed for evaluating the relevance of muscle function/mass increments. 106
Envisioning Figure 4, the different muscle strength outcomes seem to respond differently to exercise training, with isotonic strength clearly being more responsive to the effects of exercise training in comparison with the other strength outcomes. This is in line with a study from Frontera et al., where knee extensor and flexor strength gains were 10 times greater measured via 1RM (isotonic) compared to Cybex (isokinetic), 107 and a recent meta-analysis in healthy elderly reporting that resistance training had large size effects on upper and lower limb 1RM (isotonic strength) while only medium size effects on lower-limb MVC (isometric strength). 108 The training principle of specificity most probably plays a large role in explaining this phenomenon. During resistance training sessions, patients perform their movements on the same device and in the same motor pattern as during the 1RM testing method, while this is not the case when other strength tests (i.e. computerized and/or handheld dynamometry) are performed. Thus, neural adaptations specific to the type of training are suggested to explain this phenomenon, resulting in more pronounced increases in strength when mimicking the training movements during strength test procedures. 109,110 Also, the strength–velocity relationship comes into play, suggesting that increases in slow contractions are gained after slow-velocity resistance training and increases in fast contractions after high-velocity exercise training. 111 Thus, velocity and characteristics of the movements during training are important factors to take into account when interpreting strength tests. 107
Recommendations for future research and practice
Several studies have implemented exercise training programs that focus on short-term efficacy. Still, the currently available evidence did not enable the development and validation of a clinical decision tree in setting up an exercise-based pulmonary rehabilitation program, including setting, training modality/modalities, intensity, frequency, and duration. Such a clinical decision tree, already in development for cardiovascular disease, 112 would support health-care professionals to choose the most optimal training approach, taking multiple outcome measures, the baseline characteristics of patients with COPD and their personal care needs into consideration. Interestingly, a reduced muscle function/mass can occur due to a variety of reasons. 2 Whether and to what extent exercise-based therapies can also reverse the impact of other underlying causes of muscle weakness/atrophy (i.e. low-grade systemic inflammation, oxidative stress, accelerated aging, smoking, endocrinological disturbances, etc.) remains to be determined but may partially explain the lack of response to exercise-based therapies in individual patients. Therefore, future research may also want to take these covariates into consideration.
Obviously, consensus needs to be reached among clinicians and researchers on how to assess muscle function and mass before and after an exercise-based intervention. At least, the chosen tests should be safe, reproducible, valid, and accurate. The clinical decision tree together with standardization of the methodology of muscle function and mass testing will reduce the heterogeneity in the future trial results. Indeed, this will also allow us to better understand which patients will respond poorly to our exercise-based treatments. In fact, exercise training also fails to have a positive response in all healthy subjects. 113 –116
Additionally, in those patients with a beneficial short-term response to exercise training, longitudinal effects need to be studied. Indeed, maintaining the benefits on a long-term basis seems difficult. 117 Only a few studies have shown that it is possible to maintain muscle function improvements after a long-term follow-up of 6–18 months in patients with COPD. 23,29,118 Therefore, focus should also be placed on educational interventions and behavior change. 9 The behavior change interventions may also enable the development of exercise maintenance strategies for patients to adopt a physically active and more healthy lifestyle. In addition to exercise training, nutritional support also needs to be taken into consideration to optimize maintenance or increments in muscle function and mass.
Methodologically, more research with a high level of evidence is required to address future research recommendations. After analyzing the study designs used in the included studies in this review, 40 (57%) of 70 studies were designed as (non)-randomized controlled trials, with only 17 studies providing “good” quality research. On the other hand, 29 (41%) of 70 identified studies used a single group design with (n = 5) or without (n = 24) a healthy control group that followed a similar intervention. The lack of trials with a nonexercising COPD control group might be due to the “unethical” aspect of denying patients access to a highly effective evidence-based intervention. A crossover of the initial nonexercising COPD control group after a waiting period might be a possible solution. Concerning sample size, 20 (29%) of the 70 studies used a small sample size (defined as n ≤ 10 per group). Hence, regarding future research, it seems advised to lift the current level of evidence by setting up more RCTs or crossover RCTs with large sample sizes.
Footnotes
Acknowledgements
We would like to thank all colleagues in the field of research that provided us with extra information about their included work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Bijzonder Onderzoeksfonds (BOF) of Hasselt University (15DOC12BOF).