
Abstract
We described physical activity measures and hourly patterns in patients with chronic obstructive pulmonary disease (COPD) after stratification for generic and COPD-specific characteristics and, based on multiple physical activity measures, we identified clusters of patients. In total, 1001 patients with COPD (65% men; age, 67 years; forced expiratory volume in the first second [FEV1], 49% predicted) were studied cross-sectionally. Demographics, anthropometrics, lung function and clinical data were assessed. Daily physical activity measures and hourly patterns were analysed based on data from a multisensor armband. Principal component analysis (PCA) and cluster analysis were applied to physical activity measures to identify clusters. Age, body mass index (BMI), dyspnoea grade and ADO index (including age, dyspnoea and airflow obstruction) were associated with physical activity measures and hourly patterns. Five clusters were identified based on three PCA components, which accounted for 60% of variance of the data. Importantly, couch potatoes (i.e. the most inactive cluster) were characterised by higher BMI, lower FEV1, worse dyspnoea and higher ADO index compared to other clusters (p < 0.05 for all). Daily physical activity measures and hourly patterns are heterogeneous in COPD. Clusters of patients were identified solely based on physical activity data. These findings may be useful to develop interventions aiming to promote physical activity in COPD.
Keywords
Introduction
Physical activity levels in patients with chronic obstructive pulmonary disease (COPD) are mostly presented as a total amount or as an average of multiple measurement days. 1 –6 Nevertheless, physical activity is a multidimensional construct that should be described by relevant constructs and measures. 7 A more detailed approach to physical activity data analysis could provide complementary information about the physical activity behaviour of patients with COPD.
Studies in different patient populations show that a more detailed analysis of physical activity can be achieved by plotting physical activity hourly patterns 7 –9 and by applying cluster analysis to physical activity measures. 8,10,11 Physical activity hourly patterns provide a graphic representation of the temporal trends of physical activity intensities over the course of a day 7 –9 and they can provide useful information. Rochester et al., 12 for example, observed a delayed morning start and a reduced peak of activity in patients with Parkinson’s disease. Cluster analysis, 13 in turn, can be useful to identify subgroups of subjects with distinct physical activity characteristics. In middle-aged Chinese adults, Lee et al. 8 were able to identify two clusters of subjects, one more active than the other. Male subjects in the least active cluster had higher body fat percentage and older age than those in the active group. These detailed analyses could then lead to new insights regarding subgroups of patients with COPD with specific physical activity patterns, which may be used in further investigations and intervention strategies. 6,14 –16 Indeed, for specific groups of patients, greater and/or more sustainable results may be achieved if the focus shifts from an increase in moderate-to-vigorous activities towards a reduction in sedentary time. 17 –20
Therefore, the main contributions provided by this work are to describe physical activity measures and physical activity hourly patterns in patients with COPD after stratification for generic and COPD-specific characteristics and to identify clusters of patients with COPD based on physical activity measures.
Materials and methods
Detailed methods and supplementary results are available in the supplementary material.
Study design and participants
This is a pooled analysis of historical, cross-sectional and objectively assessed physical activity data from 10 countries (i.e. United Kingdom, Ireland, the Netherlands, Germany, Switzerland, Italy, Spain, the United States, Brazil and Australia). Published and/or unpublished physical activity data from previous studies as assessed by the SenseWear Armband or SenseWear Mini Armband activity monitors (both from BodyMedia Inc., Pittsburgh, PA, USA) were considered for analysis. A detailed description of the sources of the data included in the current analysis – including study registration number, study type, main publications, sites of recruitment, period of data collection and number of subjects included – is provided in Supplementary e-Table 1. Ethics board approval was obtained from the local ethics committees/institutional review boards and written informed consent was provided by the participants. Subjects were included if they had COPD with a post-bronchodilator-forced expiratory volume in the first 1 second (FEV1)/forced vital capacity ratio <0.70, 21 clinical stability at the time of physical activity assessment and complete data for age, sex, body mass index (BMI) and daily physical activity measures.
Assessments
Demographics, anthropometrics, lung function and clinical data were assessed. In order to investigate their association with physical activity measures and hourly patterns, these outcomes were stratified according to the established criteria or according to the median value (i.e. above or below the median). The SenseWear Armband or SenseWear Mini Armband activity monitors, which use multisensory data in combination with pattern recognition algorithms to reliably estimate energy expenditure (EE) and metabolic equivalents of task (METs), 22 were used to assess physical activity. 23 –26 SenseWear Professional software versions 6.1 and 7.0 were used for data analysis. METs data are divided into activity intensity levels using the thresholds proposed by the American College of Sports Medicine; 27 very light intensity, <2.0 METs; light intensity, 2.0 to 2.9 METs; and moderate-to-vigorous intensity, ≥3.0 METs.
Subjects with a minimum of four recorded days (two weekdays + Saturday + Sunday), 1 with the device being used for ≥22 h·day−1,28 were included in the analyses. Only recordings during waking hours of weekdays were considered for the main analysis, since physical activity measures during the weekend are known to be different. 1 The physical activity measures represent the average of all valid weekdays. Weekend days were used only for the presentation of daily physical activity hourly patterns. All values represent absolute values.
Cluster analysis
Cluster analysis was used to identify subgroups of patients with distinct physical activity profiles. First, minute-by-minute EE and METs data were stratified according to different criteria (and the combination of them): intensity (e.g. very light, light or moderate-to-vigorous intensity), duration (e.g. bouts of activity; a bout was defined as a predefined minimum period of consecutive minutes (e.g. 10 min) in the same intensity), period of the day (e.g. before or after midday), frequency (e.g. number of bouts per day) and quantity (e.g. absolute numbers or percentage of total). These stratifications led to 180 distinct variables referred to as features (Supplementary e-Table 2). Data regarding steps-per-day were not included in the current analysis as this outcome is subject to inaccuracy unless the subject walks at higher speeds. 29 Second, principal component analysis (PCA) was used to compress the information contained in the high-dimensional feature set (180 dimensions) to a lower subspace (3 dimensions) that is both convenient for data visualisation and able to account for the desired variance of the data (set to 60%). The features were initially standardised using z-scores. All 180 features contributed to each principal component, but some contributed more than others. The most relevant features in each component are presented. Third, a k-means clustering algorithm with automatic selection of the number of clusters was applied to the three principal components to separate the subjects into groups with distinct characteristics. The algorithm selects the number of clusters in a way that the corresponding clustering results are the most stable under small perturbations of the input data set. 13 The normalised mean over pairwise clustering distances was used as instability measure. 13 Feature extraction, PCA and cluster analysis were performed using Matlab R2012b (Mathworks Inc., Natick, MA, USA).
Statistical analyses
Continuous variables were expressed as median (interquartile range), as most variables showed non-normal distribution. Categorical variables were expressed as absolute and/or relative frequency. Mann–Whitney U test or Kruskal–Wallis test (post hoc Dunn; significant if p < 0.05) was used for comparing continuous variables, while the χ 2 test was used for categorical variables. The influence of seasons on daily physical activity measures was minimal (Supplementary e-Table 3) and therefore this was not taken into consideration throughout the analyses. Spearman coefficient was used to investigate correlations, when appropriate. The area under each hourly pattern, named as the area under the curve (AUC), was calculated and presented with its 95% confidence intervals to quantitatively represent time-varying averages of the hourly patterns. A p value of <0.01 was considered significant and all statistical analyses were performed using SPSS 17.0 (SPSS, Chicago, IL, USA) or GraphPad Prism 5 (GraphPad Software, La Jolla, CA, USA).
Results
General characteristics, physical activity measures and hourly patterns of 1001 patients with COPD
In total, 1001 patients with COPD were analysed (Table 1). The majority of patients were men, had a normal-to-overweight BMI, moderate-to-severe degree of airflow limitation and only a small proportion used long-term oxygen therapy (LTOT). Regarding the assessment of physical activity levels, the median number of valid days analysed per patient was 6 (6–6), resulting in a total of 6074 valid physical activity days, of which 4049 (67%) were weekdays. The daily total time was smallest and the daily total EE was lowest in moderate-to-vigorous intensity (Table 1). Higher EE was observed during summer for very light and light intensities, but this did not translate into more time in these intensities (Supplementary e-Table 3). Characteristics per country can be found in Supplementary e-Table 4.
General characteristics and daily physical activity measures of patients with COPD (n = 1001).a
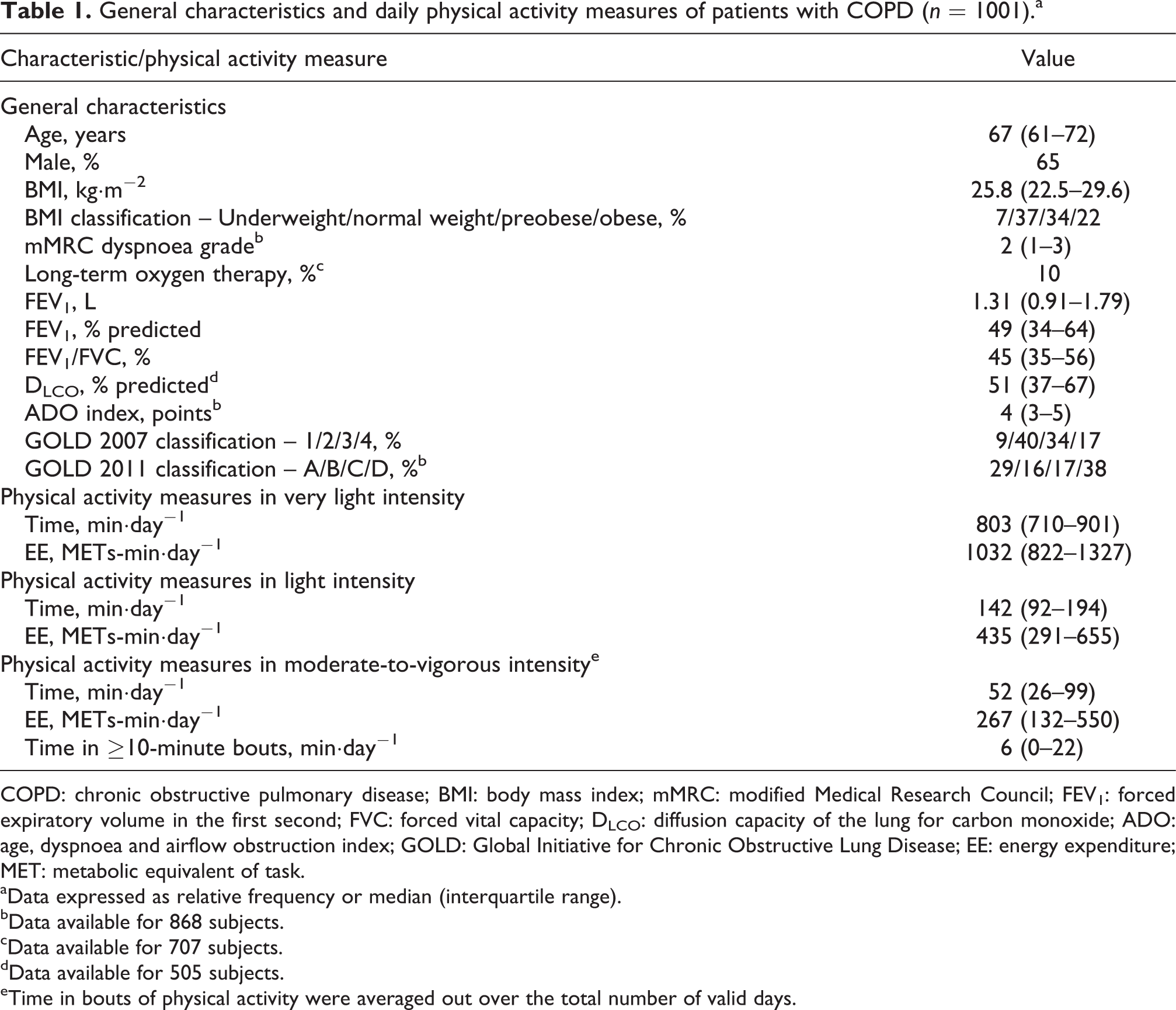
COPD: chronic obstructive pulmonary disease; BMI: body mass index; mMRC: modified Medical Research Council; FEV1: forced expiratory volume in the first second; FVC: forced vital capacity; DLCO: diffusion capacity of the lung for carbon monoxide; ADO: age, dyspnoea and airflow obstruction index; GOLD: Global Initiative for Chronic Obstructive Lung Disease; EE: energy expenditure; MET: metabolic equivalent of task.
aData expressed as relative frequency or median (interquartile range).
bData available for 868 subjects.
cData available for 707 subjects.
dData available for 505 subjects.
eTime in bouts of physical activity were averaged out over the total number of valid days.
Stratification for generic and COPD-specific characteristics
In general, patients of older age, female sex, LTOT users, lower diffusion capacity of the lung for carbon monoxide (DLCO), higher modified Medical Research Council (mMRC) dyspnoea grade, higher BMI, higher ADO index (including age, dyspnoea, and airflow obstruction), higher Global Initiative for Chronic Obstructive Lung Disease (GOLD) grade and patients from GOLD group D spent the smallest daily total time and lowest daily total EE in moderate-to-vigorous intensity (Supplementary e-Tables 5–13). Daily physical activity hourly patterns after stratification for the abovementioned characteristics are presented in Figure 1 and Supplementary e-Figure 1, showing a significant influence of age, BMI, mMRC dyspnoea grades and ADO index scores, as there was little or no overlap between the 95% confidence intervals of the hourly patterns. The AUC values for these parameters varied between 0.25 and 0.36 (Supplementary e-Table 14). The influence of GOLD grades or GOLD groups on these patterns was small. Moreover, only weak associations existed between FEV1 (% predicted) and the time in activities of very light, light and moderate-to-vigorous intensities (e-Figure 2).

Daily physical activity hourly patterns of the patients with chronic obstructive pulmonary disease after stratification for (a) and (b) – modified Medical Research Council (mMRC) grades, data available for 868 subjects only; (c) and (d) – body mass index (BMI) classification; (e) and (f) – Global Initiative for Chronic Obstructive Lung Disease (GOLD) grades (1 to 4); and (g) and (h) – GOLD groups (a to d). (a), (c), (e) and (g) represent weekdays, while (b), (d), (f) and (h) represent weekend days. Data pooled per hour as mean (95% confidence intervals).
Cluster analysis of daily physical activity measures
The PCA identified three components, which accounted for 60% of the total variance of the data (first component, 34%; second component, 17%; third component, 9%). The most relevant features of each component were: first component, daily time in ≥2-min and ≥10-min bouts of very light intensity; second component, total daily EE in moderate-to-vigorous intensity and daily EE in ≥2-min and ≥10-min bouts of moderate-to-vigorous intensity; third component, daily EE in very light intensity after midday, total daily EE in very light intensity and daily EE in ≥2-min bouts of very light intensity after midday.
Cluster analysis performed on the three principal components identified five distinct clusters (Figure 2; see e-Video for a three-dimensional video of Figure 2). Table 2 presents the characteristics and physical activity measures of these groups, which were named based on the time spent on each physical activity intensity, as previously. 30 Couch potatoes (n = 216, 22%) were characterised by higher BMI, more dyspnoea, higher ADO index, more time in very light intensity and less time in light and moderate-to-vigorous intensities compared to other clusters. Similar to couch potatoes, highly sedentary (n = 415, 41%) spent more time in very light intensity and less time in moderate-to-vigorous intensity than other clusters. Sedentary movers (n = 184, 18%) spent more time in light intensity and less time in moderate-to-vigorous intensity than sedentary exercisers (n = 165, 17%) and busy bees (n = 21, 2%), while sedentary exercisers in turn spent more time in light intensity compared to busy bees. Busy bees were characterised by less time in very light intensity and more time in moderate-to-vigorous intensity compared to other clusters. Figure 3 presents the daily time in activities of different intensities by the clusters, highlighting the mixed arrangements of physical activity. Figure 4 presents the daily physical activity hourly patterns of the clusters. In all clusters, the peak of intensity during the day occurred before midday, and in general weekdays and weekend days presented a similar pattern, especially in more inactive clusters. Hourly patterns after synchronisation of the waking up moment are presented in Supplementary e-Figure 3. Moreover, increasing AUC values were found from couch potatoes to busy bees (Supplementary e-Table 14).
General characteristics and daily physical activity measures of clusters of patients with COPD.a

COPD: chronic obstructive pulmonary disease; BMI: body mass index; mMRC: modified Medical Research Council; ADO: age, dyspnoea and airflow obstruction index; GOLD: Global Initiative for Chronic Obstructive Lung Disease; EE: energy expenditure; MET: metabolic equivalent of task; FEV1: forced expiratory volume in the first second.
aData expressed as absolute/relative frequency, or median (interquartile range).
b p < 0.05 vs. couch potatoes.
c p < 0.05 vs. highly sedentary.
dData available for 198 subjects in couch potatoes, 367 subjects in highly sedentary, 159 subjects in sedentary movers, 126 subjects in sedentary exercisers and 18 subjects in busy bees.
e p < 0.05 vs. sedentary movers.
f p < 0.05 vs. sedentary exercisers.

The five clusters identified. (a) Graph in three dimensions presenting the three principal component analysis (PCA) components; (b) graph in two dimensions presenting the first and second components; (c) graph in two dimensions presenting the first and third components; and (d) graph in two dimensions presenting the second and third components. Details about the relationship between components and clusters can be found in the supplementary material.

Daily time in activities of very light intensity (a), light intensity (b) and moderate-to-vigorous intensity (c) by clusters of patients with chronic obstructive pulmonary disease. Data are presented as median (interquartile range).
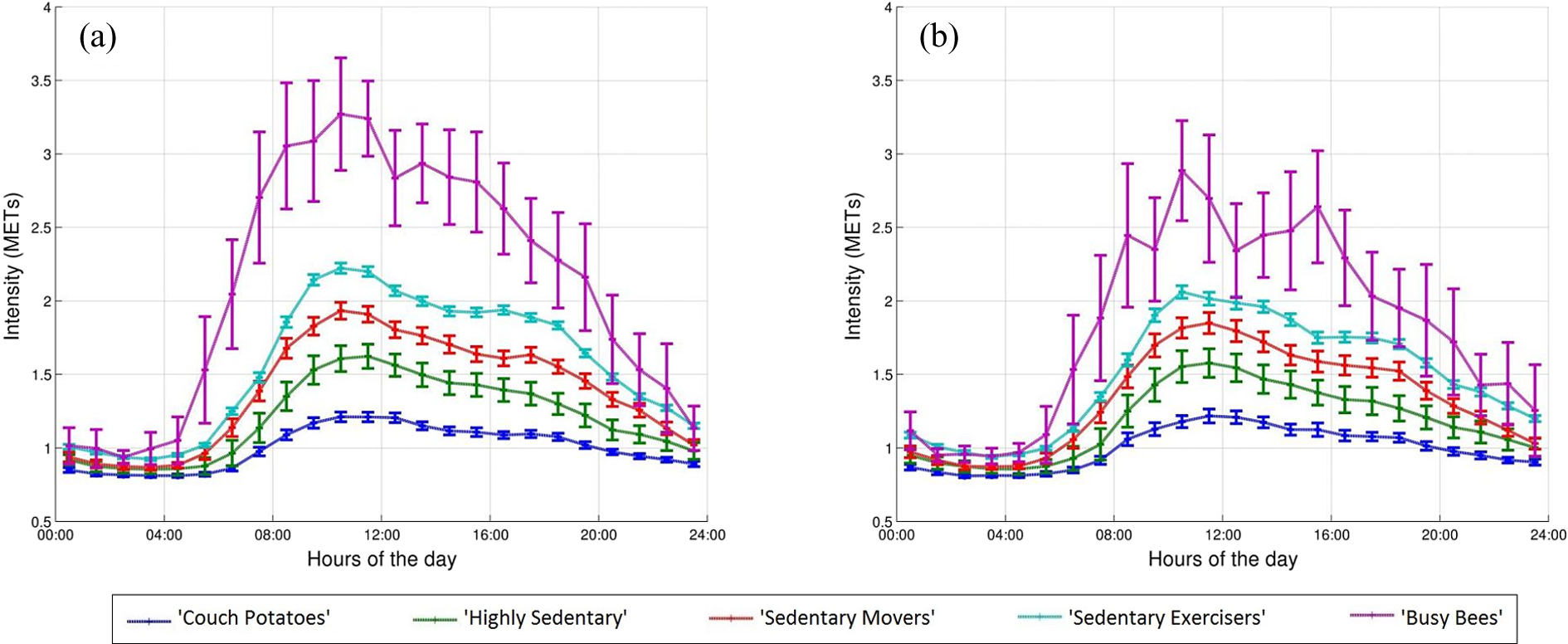
Daily physical activity hourly pattern of clusters of patients with chronic obstructive pulmonary disease during weekdays (a) and weekend days (b). Data pooled per hour as mean (95% confidence intervals).
Discussion
The present study provides detailed analyses of objectively measured physical activity in a multinational sample of 1001 patients with COPD. The principal findings show that daily physical activity measures and hourly patterns vary considerably after stratification for generic and COPD-specific characteristics and that patients with COPD can be clustered based on daily physical activity measures, with five clusters being identified, each with distinct physical activity measures and hourly patterns.
Daily physical activity measures and physical activity hourly patterns in COPD
Our results clearly show that physical activity is a heterogeneous characteristic in patients with COPD, corroborating previous findings. 31,32 Distinct levels of physical activity were found after stratification for age (< or ≥67 years), sex (male or female), BMI (underweight to obese), mMRC dyspnoea grade (0 to 4), LTOT (yes or no), DLCO (< or ≥51% predicted), ADO index (< or ≥4 points), GOLD grades (1 to 4) and GOLD groups (A to D) (Supplementary e-Tables 5–13). Interestingly, comparable time in very light and moderate-to-vigorous intensities was found between GOLD groups A and C, and between GOLD groups B and D (e-Table 13). This suggests that symptoms of dyspnoea, which discriminates between groups A/C and B/D, are better associated with physical activity measures than the degree of airflow limitation, which discriminates between groups A/B and C/D. Demeyer et al. 33 also investigated physical activity levels in patients with COPD after classification into GOLD groups. Our findings are in broad agreement with theirs. When using the mMRC scale to classify patients into GOLD groups, as done in our study, these authors found similar number of steps per day between GOLD groups A and C, and between GOLD groups B and D. 33 In our study, despite the significant influence of GOLD groups on physical activity measures, only little or no influence could be observed on physical activity hourly patterns. Few studies have investigated hourly patterns in COPD. In the study by Hecht et al., 9 the authors observed that the highest activity level occurred during the late morning and early afternoon hours, which is corroborated by our findings. Together with our findings, this suggests that hourly patterns have the potential to complement the information provided by summary values.
Clusters of patients with COPD based on daily physical activity measures
The present study is the first to apply cluster analysis using objectively assessed physical activity measures only to a large and diverse sample of patients with COPD. Indeed, five clusters were identified, each with distinct physical activity measures and hourly patterns. One very active cluster (busy bees) and one very inactive cluster (couch potatoes) were identified, but clusters in intermediate categories were also observed.
Only a few studies have used objectively measured physical activity data solely to cluster subjects. In 10-to-12-year-old children, De Bourdeaudhuij et al. 34 were able to identify a cluster with a mixed arrangement of physical activity (i.e. less time in moderate-to-vigorous intensity + less sedentary time). In our study, we also found a cluster with resembling characteristics (i.e. sedentary exercisers), confirming that activities of moderate-to-vigorous intensity and sedentary activities are not two sides of one continuum. 34 Based on the amount of time in moderate-to-vigorous physical activity, sedentary exercisers could be considered physically active. 27 Nonetheless, these patients spent over 11 h in very light intensity (i.e. sedentary behaviour), which can have negative health consequences as previous studies have shown the detrimental effects of prolonged periods of sedentary behaviour on health outcomes. 35,36
The characteristics of the clusters identified in our study can provide important insights on how to plan physical activity/exercise regimens for patients with COPD. For instance, couch potatoes were characterised by worse airflow limitation and more debilitating symptoms compared to other clusters. Previous studies have shown that some interventions might be particularly useful in patients with these characteristics. For example, interval training has been shown to result in lower symptom scores and fewer unintended breaks while reproducing the effects of endurance continuous training. 37 This type of training uses short bouts of high-intensity exercise interspersed regularly with periods of rest or lower intensity exercise. Another modality that is particularly useful in more symptomatic patients is transcutaneous neuromuscular electrical stimulation, 38 but new modalities are emerging such as downhill walking. 39 Moreover, based on their characteristics couch potatoes may benefit the most from pulmonary rehabilitation. 40
Couch potatoes as well as highly sedentary were characterised by considerable amounts of time in very light physical activity (i.e., sedentary behaviour) and little time in moderate-to-vigorous physical activity. These clusters would probably benefit from an intervention focusing not only on increasing the time in moderate-to-vigorous physical activity but also on reducing the time in sedentary behaviour. Potential ways to increase physical activity in COPD have been explored in a recent systematic review. 16 Although some intervention characteristics seemed to associate with greater improvements, such as interventions focusing specifically on increasing physical activity and longer pulmonary rehabilitation programmes, 16 to date there is little evidence that relevant and sustainable changes in physical activity are achievable in patients with COPD, especially physical activity in moderate-to-vigorous intensity. 20 Some patients might find it difficult to increase the time in moderate-to-vigorous physical activity, which suggests that it might be more realistic for these patients to increase the time in light activities. 17,19 In fact, there is emerging literature in other populations suggesting that health benefits can be achieved by decreasing time in sedentary behaviour and increasing the participation in light intensity physical activities. 41 –43 In patients with COPD, low-intensity exercises were able to improve health-related quality of life and functional status. 44 Moreover, a recent study demonstrated that greater quantity of low-intensity physical activity associates with a reduced risk of COPD hospitalisation. 18
Sedentary movers and sedentary exercisers spent a considerable amount of time in moderate-to-vigorous intensity (i.e. 68 and 166 min, respectively), which is in agreement with the recommended by physical activity guidelines. 27 Nonetheless, these patients also spent important amounts of time in very light intensity (i.e. 706 and 675 min, respectively). Indeed, the daily amount of time spent in very light intensity (i.e. sedentary behaviour) by these groups is more than what other studies have considered as harmful (i.e. 7 h). 35,36 Sedentary behaviour has been the focus of recent literature in COPD. 20,45 Sedentary behaviour is defined as any waking behaviour characterised by an EE ≤1.5 METs while in a sitting or reclining posture (e.g. watching television). 46 Epidemiological data in non-COPD populations have shown that engaging in moderate-to-vigorous intensity physical activity is not enough to fully protect against the detrimental consequences of prolonged periods of sedentary behaviour. 47,48 This suggests that researchers and clinicians should also aim to reduce sedentary behaviour. Interventions focusing on sedentary behaviour in patients with COPD are scarce. Nevertheless, studies on other populations have shown promising results. In the ‘Stand Up For Your Health’ study, 49 a brief intervention based on goal setting and behavioural self-monitoring was shown to be feasible and able to reduce sedentary time and increase physical activity in Australian older adults. In the ‘TView’ study, 50 a 3-week programme using an electronic television lock-out system led to reductions in TV viewing time (a sedentary behaviour) of almost 3 h per day in overweight and obese adults. Strategies based on the use of technology might also provide beneficial results, such as pads to measure sitting time. 51
Busy bees were characterised by very high levels of moderate-to-vigorous physical activity. Not surprisingly, this group was formed by a very small number of patients (i.e. 21 patients, 2% of the whole sample). Busy bees would probably benefit from strategies to maintain their very high physical activity levels. Home-based exercise training combined with monthly phone calls was able to maintain the gains in exercise capacity and health-related quality of life after a short pulmonary rehabilitation programme in patients with moderate COPD. 52 Strategies that can be easily incorporated into daily life, such as leisure walking, can produce more sustainable results. A randomised controlled trial including a 3-month programme of outdoor Nordic walking in patients with COPD resulted in significant improvements in exercise capacity and physical activity. 53 These improvements were sustained at 6 and 9 months after the initial intervention. 53
Strengths and methodological considerations
We have analysed a large and diverse sample of patients with COPD with objectively assessed physical activity data. This allowed detailed analyses of daily physical activity, even identifying clusters of patients with COPD with distinct physical activity measures, a novelty within the COPD literature. Physical activity hourly patterns were also investigated for the first time in a large-scale study in COPD, representing another important advance. All these analyses were only possible due to the use of objective methods to assess physical activity.
Some methodological considerations need to be taken into account. First, selection and information biases might be present, as the data were collected separately as part of different studies. Second, the clusters identified in our study were not validated as we were not able to show whether they relate to relevant clinical outcomes, such as COPD-related hospitalisations and deaths due to the lack of follow-up assessments, or whether they could be replicated in another sample. Third, other characteristics that may influence physical activity levels in patients with COPD, such as comorbidities, 54 were not available.
To conclude, daily physical activity measures and hourly patterns in patients with COPD were found to vary considerably depending on the clinical characteristic. Moreover, five clusters of patients were identified, each with distinct physical activity measures and hourly patterns. The present data show that outcome measures need to be clearly delineated when evaluating interventions aiming to promote physical activity in patients with COPD.
Footnotes
Acknowledgement
The Australian-based authors would like to thank the Pulmonary Rehabilitation Departments at Royal Prince Alfred Hospital (particularly Lissa Spencer), Concord Repatriation General Hospital, Prince of Wales Hospital (particularly Renae McNamara), Manly Hospital, Hornsby-Kuring-Gai Hospital, Sir Charles Gairdner Hospital (particularly Nola Cecins and Michelle Melang) and Bentley Hospital for assisting with participant recruitment.
Author contribution
RM and GS have contributed equally to this work. OA, HW and MAS are joint senior authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: RM is supported by the National Council of Scientific and Technological Development (CNPq), Brazil (246704/2012-8). DB holds a Canada Research Chair, Canada. SSCK was funded by the Medical Research Council, UK. WD-CM was funded by the Medical Research Council, UK, and the National Institute for Health Research, UK. MSP was supported by an unrestricted research grant from Astra Zeneca. KCF is supported by the Coordination for the Improvement of Higher Education Personnel (CAPES), Brazil. SZ, DM, SD and JDL were supported by the following foundations: ‘Gottfried und Julia Bangerter-Rhyner-Stiftung’, ‘Freiwillige Akademische Gesellschaft Basel’ and ‘Forschungsfonds der Universität Basel’, Switzerland. DS was supported by GSK and by the Medical Research Council, UK (G0701628). FP is supported by CNPq, Brazil. PRE was supported by an NHMRC Research Fellowship, Australia (1042341). MIP’s contribution to this manuscript was funded by the NIHR Respiratory Biomedical Research Unit at the Royal Brompton and Harefield NHS Foundation Trust and Imperial College, UK. EFMW was supported by Point-One funding from AgentschapNL, Dutch Ministry of Economic affairs, the Netherlands. AWV was supported by ‘Stichting de Weijerhorst’ and Point-One funding from AgentschapNL, Dutch Ministry of Economic affairs, Netherlands. MAS was supported by Point-One funding from AgentschapNL, Dutch Ministry of Economic affairs, the Netherlands. Part of the data was sponsored by GlaxoSmithKline (data from the ECLIPSE cohort sub-study). Data from Ireland was supported by Beaumont Foundation, Ireland and SwordMedical Ltd, Ireland. The Australian sites were supported by a National Health and Medical Research Grant, Australia (grant no.: 570814). Part of the data collection in the UK (data from Leicester) was supported by the National Institute for Health Research (NIHR) Leicestershire, Northamptonshire and Rutland Collaboration for Leadership in Applied Health Research and Care and took place at University Hospitals of Leicester NHS Trust, UK, and by the NIHR Leicester Respiratory Biomedical Research Unit, UK. Data from the PAC-COPD study was funded by grants from the following Spanish institutions: Fondo de Investigación Sanitaria, Ministry of Health (FIS PI020541); Agència d’Avaluació de Tecnologia i Recerca Mèdiques, Catalonia Government (AATRM 035/20/02); Spanish Society of Pneumology and Thoracic Surgery (SEPAR 2002/137); Catalan Foundation of Pneumology (FUCAP 2003 Beca Marià Ravà); Red RESPIRA (RTIC C03/11); Red RCESP (RTIC C03/09), Fondo de Investigación Sanitaria (PI052486); Fondo de Investigación Sanitaria (PI052302); Fundació La Marató de TV3 (No. 041110); and DURSI (2005SGR00392); and by unrestricted educational grants from Novartis Farmacèutica and AstraZeneca Farmacéutica.
Supplemental material
Supplementary material is available for this article online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.