
Abstract
This study aimed at investigating whether providing feedback on physical activity (PA) levels to patients with chronic obstructive pulmonary disease (COPD) is feasible and enhances daily PA during pulmonary rehabilitation (PR). Patients with COPD participated in a 12-week PR program. Daily PA was measured using activity monitors on weeks 1, 7, and 12, and feedback was given in the following weeks on the number of steps, time spent in sedentary, light, and moderate-to-vigorous intensity activities, and time spent standing, sitting, and lying. Compliance with PA monitoring was collected. Two focus groups were conducted to obtain patients’ perspectives on the use of activity monitors and on the feedback given. Differences in PA data were also assessed. Sixteen patients (65.63 ± 10.57 years; forced expiratory volume in one second (FEV1) 70.31 ± 22.74% predicted) completed the study. From those, only eleven participants used the activity monitors during all monitoring days. Participants identified several problems regarding the use of activity monitors and monitoring duration. Daily steps ( p = 0.026) and standing time ( p = 0.030) were improved from week 1 to week 7; however, the former declined from week 7 to week 12. Findings suggest that using feedback to improve PA during PR is feasible and results in improved daily steps and standing time on week 7. The subsequent decline suggests that additional strategies may be needed to stimulate/maintain PA improvements. Further research with more robust designs is needed to investigate the impact of feedback on patients’ daily PA.
Keywords
Introduction
Low levels of physical activity (PA) have been associated with increased health-care utilization and reduced survival in patients with chronic obstructive pulmonary disease (COPD). 1 Thus, improving PA levels has become one of the main goals of COPD research. 2,3
Pulmonary rehabilitation (PR) is an evidence-based intervention, which includes exercise training, education, and psychosocial support. 3 The exercise training component has been shown to improve exercise capacity and reduce dyspnea; 4 however, its effects in increasing PA levels are limited. 2 A recent study showed that although a 3-month PR program increased patients’ exercise capacity and quality of life, changes in daily PA were restricted to a marginal improvement in walking intensity. 5 The authors suggested that patients would likely require longer programs to increase their time spent actively. 5
Alternatively, PA levels may be enhanced by including behavior strategies in PR programs. 3 One strategy consists of increasing patients’ awareness of their actual PA levels. 6 In healthy adults, awareness of individual PA is a potential determinant of the intention to increase PA levels. 7 As patients with COPD tend to overestimate their PA levels, 8 making them aware of their actual levels may contribute to improve patients’ PA. For this purpose, activity monitors can be a valuable tool because they provide objective information about PA, which can then be delivered to the patient. However, the effective contribution of activity monitors to increase PA levels of patients with COPD is still unclear, with the few existing studies showing conflicting results. 9 –11 Differences in the devices used, PA monitoring protocols and interventions may explain, in part, these discrepancies, but patients’ compliance with PA monitoring and their experience with the activity monitors may have contributed as well. These aspects are key elements to ensure feasibility of interventions involving PA monitoring and feedback; however, they have been understudied in COPD research. 12 Before the widespread utilization of this technology on a larger scale, its feasibility should be investigated. Therefore, this study aimed to investigate whether providing feedback on PA levels to patients with COPD, using activity monitors, is feasible and enhances patients’ daily PA during PR.
Methods
Design
This was a feasibility study with a mixed methods design. The study received full approval from the Institutional Ethics Committee.
Participants
Patients with COPD were recruited in two primary care centers of the central region of Portugal (Aveiro). General practitioners informed eligible patients about the study and asked their willingness to participate. Inclusion criteria were (a) being 18 years old or older; (b) having a diagnosis of COPD according to the Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria; 4 and (c) presenting clinical stability for 1 month prior to the study (no hospital admissions or exacerbations). Patients were excluded if they (a) presented severe psychiatric, neurologic, or musculoskeletal conditions and/or unstable cardiovascular disease or (b) were engaged in regular exercise before the study. Patients who agreed to participate were contacted by the researchers. Detailed information about the study was provided and written informed consent was obtained before data collection.
Intervention
The intervention was conducted between April and July and consisted of a 12-week PR program with exercise training (three times per week, 60 minutes/session) and psychoeducation (once per week, 90 minutes), along with the provision of feedback on PA levels to participants. Exercise training sessions included the following: A warm-up period (5–10 minutes) with range-of-motion, stretching, low-intensity aerobic exercises, and breathing techniques. Endurance training (20-minute walking) at 60–80% of the 6-minute walk test (6MWT) average speed,
13
with intensity adjusted to patient’s levels of fatigue/dyspnea (4–6 in the Modified Borg Scale).
3
Strength training (15 minutes), including seven exercises (two sets, 10 repetitions/set) of the major muscle groups of the upper and lower limbs, at 50–85% of the 10 repetition maximum (10-RM).
14
Progression was based on the two-for-two rule.
15
Balance training (5 minutes) with static and dynamic exercises organized in progressive levels of difficulty.
16
A cool-down period (10 minutes) similar to the warm-up period.
The psychoeducation component included educational and supportive modules regarding information on COPD; breathing and energy conservation techniques; adoption of healthy lifestyles (exercise, nutrition, and sleep habits); emotion management strategies; and community resources.
PA was monitored during the first (W1), seventh (W7), and 12th (W12) weeks of the PR program using the activity monitors GT3X+ (ActiGraph, Pensacola, Florida, USA), and feedback to participants was given in the following weeks. As these devices did not provide automatic feedback to participants, researchers analyzed the information collected and summarized it. Feedback was given by one of the health professionals conducting the PR program and lasted 15–20 minutes. Feedback of W1 and W7 was given at the end of the exercise training session of the following week (W2 and W8, respectively); feedback of W12 was given in the week following program completion. Each participant received written (graphical) and verbal information about (a) time spent standing, sitting, and lying on each day of the week and (b) a weekly average of the number of daily steps and of time engaged in sedentary, light, and moderate-to-vigorous intensity activities. On W1, participants were instructed to maintain their routine to establish a baseline of their activity levels and received verbal and written instructions on how to use the device. While receiving feedback of W1, participants were informed about the recommended values of PA for healthy people (≥150 minutes/week or ≥30 minutes/day of moderate intensity activities, ≥75 minutes/week or ≥20 minutes/day of vigorous intensity activities or a combination of both, performed continuously or accumulated in bouts of at least 10 minutes; 7000–10,000 steps/day). 17 Although feedback was given in group, each participant received individualized recommendations to improve or maintain his/her PA levels regarding the time spent in moderate-to-vigorous intensity activities and number of steps per day, based on the results of the previous week. Participants also received general recommendations to improve daily PA and a leaflet with exercises similar to those of the exercise training component. Feedback of W7 and W12 was similar to W1.
Data collection
Participants’ characteristics
Sociodemographic data were collected before the intervention to characterize the sample. Lung function was assessed with a portable spirometer (MicroLab 3500, CareFusion, Kent, Dan Diego, California, USA) according to the guidelines. 18 All participants took their usual prescribed medications before performing the lung function test. COPD grade and severity (ranging from group A (low risk, less symptoms) to group D (high risk, more symptoms)) were determined in accordance with the GOLD criteria. 4 Patients’ breathlessness was measured using the Modified Medical Research Council Dyspnea Scale. 19 Exercise capacity was assessed with the maximal distance walked on the 6MWT. 13 Two tests were performed according to the American Thoracic Society guidelines. 20 The best performance was reported and related to the reference values. 21
Feasibility measures
Patients’ compliance with the use of activity monitors (number of days wearing the device, time per day) and reasons for noncompliance were collected. In the week following the intervention, two focus groups were conducted in Portuguese to evaluate patients’ perspectives on the use of activity monitors and feedback given. Each focus group lasted approximately 30 minutes and was audio recorded for further transcription and analysis.
Physical activity
Daily PA was assessed using the activity monitors GT3X+ (already validated in COPD population) 22,23 on W1, W7, and W12 of the PR program. Participants were instructed to wear the device for seven consecutive days during waking hours (except when bathing or swimming) and informed about its correct positioning, that is, at the waist on an elastic belt at the anterior axillary line of the right hip. Data were then downloaded using Actilife version 6.7.2 (ActiGraph, Pensacola, Florida, USA). Since 5 or more days of measurement are required to reliably assess PA in COPD, 24 patients with less than 5 days in one of the time points were excluded from PA analysis. A valid day was defined as at least 8 hours of wearing time. 25 Daily PA was calculated using the algorithms incorporated in the software and included (a) number of steps; (b) time spent in sedentary, light, and moderate-to-vigorous intensity activities; and (c) time spent standing, sitting, and lying. Cut points for PA intensity were defined as sedentary (0–99 counts per minute (CPM)), light (100–1951 CPM), and moderate-to-vigorous intensity activities (1952–∞ CPM). 26 Since an increase in exercise capacity might facilitate increases in PA, 27 the 6MWT was also performed in the week following program completion to assess intervention-related differences.
Data analysis
Participants’ characteristics
Descriptive statistics were used to characterize the sample. Baseline measurements of completers and dropouts were compared using independent t tests for normally distributed data, Mann–Whitney U tests for ordinal/non-normally distributed data, and χ2 tests for categorical data. The normality of data was investigated with the Shapiro–Wilk test. A similar analysis was conducted to compare baseline measurements of patients with complete and incomplete PA assessment (i.e. patients with seven PA monitoring days vs. those without seven monitoring days).
Feasibility measures
The number of monitoring days missed by patients and wearing time were calculated, and reasons for noncompliance were analyzed. Focus group analyses were conducted by two independent researchers using the procedures suggested by Ulin, 28 namely (a) reading and rereading the transcripts; (b) identifying possible themes; (c) displaying the information relevant to each theme; (d) reducing the information to its essential points; and (e) identifying its core meaning. Any disagreements were resolved by consensus.
Physical activity
Differences in PA data among the three time points were assessed using a repeated measures analysis of variance (ANOVA), and pairwise comparisons were performed whenever statistical significance ( p < 0.05) was reached. Effect sizes (ES) were computed using the eta squared (η 2), interpreted as 0.01 (small effect), 0.06 (medium effect), and 0.14 (large effect). 29 Observed power was also calculated. A paired t test was used to assess differences in the 6-minute walking distance (6MWD) of participants before and after the intervention. Analyses were conducted using SPSS version 20.0 (IBM Corp., Armonk, New York, USA).
Results
Participants
Twenty patients entered the study. However, four were lost due to non-COPD health-related problems (n = 2), changes in work schedule (n = 1), and no reasons given (n = 1). Sixteen participants completed the intervention. Their baseline characteristics are presented in Table 1. There were no significant differences between completers and dropouts ( p > 0.05).
Participants’ characteristics (n = 16)a.

BMI: body mass index; FEV1: forced expiratory volume in one second; GOLD: Global Initiative for Chronic Obstructive Lung Disease; mMRC: Modified Medical Research Council Dyspnea Scale; 6MWD: 6-minute walking distance.
aThe results are shown as mean ± SD, n (%), or median [25th percentile–75th percentile].
Feasibility measures
Eleven participants (68.8%) used the activity monitors during all monitoring days. Five participants missed 1 day (n = 1, 6.3%), 2 days (n = 1, 6.3%), or ≥3 days (n = 3, 18.8%) of PA monitoring in at least one of the time points. Various reasons were cited, namely, the monitor was uncomfortable to wear in specific situations (n = 1, 6.3%); failure to attend the last week of the program due to work-related issues (n = 1, 6.3%); and forgetfulness (n = 3, 18.8%). No significant differences were found in the baseline characteristics of participants who had complete and incomplete PA assessments ( p > 0.05). Daily wearing time was similar over the weeks (W1 = 14.04 ± 0.68 hours; W7 = 13.85 ± 1.92 hours; W12 = 13.40 ± 1.81 hours, p = 0.348).
Five participants (of 16 who completed the study) did not attend the focus groups due to work-related issues (n = 2), schedule constraints (n = 2), and no reasons given (n = 1). Focus group analyses revealed that while five participants (45.5%) reported no difficulties in using the activity monitors, six participants (54.5%) felt that the device was uncomfortable due to its placement and the pressure exerted by the elastic belt: It caused some pressure and sometimes the elastic belt felt like scratching (…) It was placed in a region where there is not much fat, there is mostly bone. [P1] I used the monitor underneath the clothes and, when I started to sweat, it felt like burning…. [P2]
Suggestions to improve its use consisted of changing the elastic belt for another with a softer material (n = 4, 36.4%) and changing the placement (e.g. attached to the thigh, chest, or arm; n = 4, 36.4%) or the dimensions of the device, making it more flattened (n = 2, 18.2%).
Regarding data collection, six participants (54.5%) mentioned that there were too many days of monitoring. The optimal duration for using the device would be 3 days (n = 4, 36.4%): Sometimes it was even unnoticed, but at the end of the third, fourth, and fifth days, it started to [bother me]…I would choose to use it only for 3 days, because this was the time that it did not really bother…[P3]
The feedback given to participants made them more conscious about their PA levels, as they found that it reflected the reality (n = 8, 72.7%). Six participants (54.5%) reported that they had improved their active time because they were wearing the devices: Using the device made me walk more! [P4] I tried to get out of the car when I could to avoid being seated for so long. [P3]
Three participants (27.3%) referred that giving daily feedback (instead of a weekly average) would be important to allow comparisons between the activities performed on a given day and the results reported by the device: We should use it during the day and download [the information] at the end of it. We would try to improve, ‘On this day I didn’t do anything… It was Tuesday… On Tuesday, I have no chance to improve…’ or ‘I will try to improve! [P5]
Physical activity
Table 2 presents daily PA levels of patients in the three time points. Significant differences with a large effect were found for number of daily steps ( p = 0.026, η 2 = 0.306). Participants increased their steps from W1 to W7 ( p = 0.050), followed by a decrease on W12 ( p = 0.048). The mean time spent in moderate-to-vigorous intensity activities was above 30 minutes/day in the three time points; however, no significant differences were found ( p = 0.167). No changes were observed in time spent in light intensity and sedentary activities ( p = 0.685 and p = 0.673).
Daily physical activity levels of participants on weeks 1, 7, and 12 of the intervention (n = 13).a
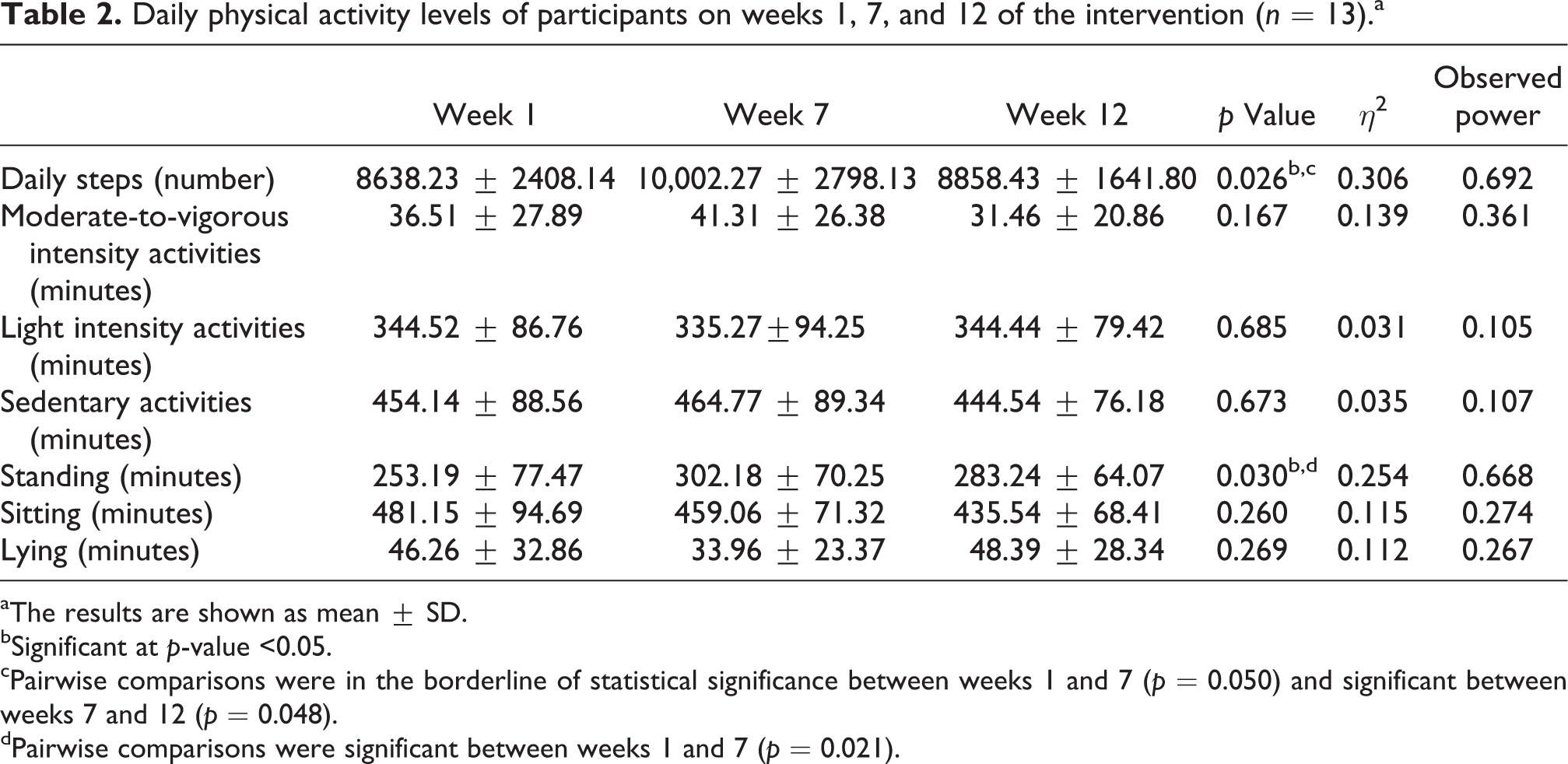
aThe results are shown as mean ± SD.
bSignificant at p-value <0.05.
cPairwise comparisons were in the borderline of statistical significance between weeks 1 and 7 (p = 0.050) and significant between weeks 7 and 12 (p = 0.048).
dPairwise comparisons were significant between weeks 1 and 7 (p = 0.021).
Regarding body postures, differences were found for standing time ( p = 0.030, η 2 = 0.254). Specifically, improvements were observed between W1 and W7 ( p = 0.021), but not between W7 and W12 ( p = 0.130). No significant differences were found for time spent sitting ( p = 0.260) or lying ( p = 0.269).
Regarding exercise capacity, participants’ 6MWD was significantly increased after the intervention (466.50 ± 81.56 vs. 513.33 ± 86.18, p = 0.001).
Discussion
This study demonstrated that using feedback to improve PA during PR is feasible and increases the number of daily steps and standing time in the short term. Nevertheless, there are still some issues that should be further enhanced to stimulate and/or maintain PA improvements.
Overall, participants’ compliance was satisfactory, and they reported a positive experience regarding the use of activity monitors. Still, some participants reported problems related to usability issues (monitor placement and pressure exerted by the elastic belt) and duration of PA monitoring. To date, a small number of studies have specifically addressed these issues; however, this may have important implications for compliance with activity monitoring 30 and should be carefully considered when planning a study. In addition, some participants occasionally forgot to wear the activity monitor. To overcome this problem, future studies should implement strategies to improve patients’ compliance, as it has been recommended in the literature. 30
Participants reported that feedback made them more conscious about their PA levels, and PA improvements were related to wearing the devices. This suggests that the aim of including feedback in PR was achieved, that is, increasing patients’ awareness and motivating them to improve daily PA. Nevertheless, some participants mentioned that daily feedback would have facilitated comparisons between the activities performed on a given day and the results reported by the device. Activity monitors with an automatic daily feedback function may, therefore, be valuable to meet patients’ needs and expectations. Pedometers include this option, but their limited accuracy may prevent them from detecting PA changes in interventional studies. 2 Future advances in sensing technologies may offer opportunities to improve PA monitoring and feedback in COPD research.
Participants improved their daily steps and standing time from W1 to W7; however, the former declined from W7 to W12. Nevertheless, a large effect was observed, indicating a relevant change. These findings suggest that patients’ PA levels may already be increased on W7 of PR programs, if appropriate feedback is given. However, complementary strategies may be necessary to stimulate and/or maintain PA improvements, since a decline was observed on W12. In this study, a psychoeducation session focused on promoting exercise habits in participants was carried out on W6, which could have acted as an additional motivational tool to stimulate behavior change and, thus, improve participants’ PA on W7. Future research should explore the value of feedback and additional strategies (e.g. psychoeducation sessions about exercise habits) to stimulate patients’ behavior change into a more active lifestyle, as this is one of the current challenges in COPD research.
Strengths and limitations
The combination of quantitative and qualitative methods of data collection is a strength of the present study, as it enabled gathering the full experience of participants with the use of activity monitors and provided important information for the design of future technologies and interventions.
The small sample size and lack of control group were limitations of this study, which may have contributed to the insufficient power obtained in some comparisons. The absence of a control group may have acted as a confounding factor, since previous studies have shown that PR per se is able to promote increases in PA levels. 5 Further studies with more robust designs are needed to investigate the value of providing feedback on PA levels to patients with COPD during PR. In addition, patients’ PA levels were collected on specific weeks of the PR program, which may compromise the comparisons with previous studies. However, this was deemed necessary to enable the provision of feedback on PA levels to participants as part of the intervention.
Most participants were in mild and moderate COPD grades, which differ from other intervention studies with PA monitoring. 5,9,11 Nevertheless, recent literature has acknowledged that PA is already reduced in early COPD grades, 6,24 and PR is now considered a standard of care for all patients, including those at earlier grades. 3
The fact that feedback was only given on specific time points may have limited participants’ PA improvements. In addition, it was not possible to determine whether PA levels were already increased before W7. Future studies should explore the impact of more regular feedback and monitoring on patients’ daily PA. Furthermore, since patients were, on average, sufficiently active on W1 (i.e. above the internationally recommended target of 7000 steps per day), 17 future studies should explore whether patients who have a lower step performance at baseline are more motivated to change their daily steps during and after the intervention.
The mean time spent in moderate-to-vigorous intensity activities was above 30 minutes/day in the three time points, which could suggest that patients have met the international recommendations. 17 However, one recent study showed that the recommended time of moderate-to-vigorous intensity activities varies upon the selected PA analysis, that is, bouts versus non-bouts analysis. 31 In the study of Van Remoortel et al., 31 the commonly used bouts cut point of 30 minutes/day was associated with a non-bouts cut point of 80 minutes/day. Since this study did not conduct a bouts analysis, it is possible that patients did not reach the international PA target for moderate-to-vigorous intensity activities. Future studies using bouts and non-bouts analysis should be conducted in order to clarify whether patients with COPD meet the international recommendations.
Despite the limitations, results from this study suggest that feedback on PA levels can be used to support patients in achieving a more active lifestyle, by helping them to self-monitor their daily PA. The costs associated with the provision of feedback were relatively small and related to the purchase of activity monitors and the time needed by health professionals to deliver feedback to the participants (15–20 minutes). Therefore, this seems a feasible intervention to be implemented in various health-care settings. Furthermore, as lower PA levels have been related to increased health-care utilization, poorer quality of life, and reduced survival of patients with COPD, 32 –34 it is reasonable to believe that this type of intervention may lead to reduced COPD health-related costs. This should be investigated in future research.
Conclusions
Providing feedback on PA levels to patients with COPD is feasible and may enhance daily PA during PR. However, additional strategies might be necessary to stimulate patients’ behavior change to a more active lifestyle, as this is one of the current challenges in COPD research. Patients’ experiences on the use of activity monitors should also be assessed, as they provide valuable information to adjust PA technologies and interventions to the target population. Further research with more robust designs is needed to investigate the impact of feedback on patients’ daily PA.
Footnotes
Acknowledgments
The authors would like to acknowledge the patients who participated in this study. A special thanks to Cristina Jácome and Raquel Gabriel for their valuable contribution in the implementation of the PR program.
Conflict of interest
The authors declared no conflicts of interest.
Funding
This work was supported by the Portuguese Foundation for Science and Technology (grant number SFRH/BD/81328/2011).