
Abstract
We evaluated whether a chronic obstructive pulmonary disease (COPD) assessment test (CAT) with adjusted weights for the CAT items could better predict future respiratory-related hospitalizations than the original CAT. Two focus groups (respiratory nurses and physicians) generated two adjusted CAT algorithms. Two multivariate logistic regression models for infrequent (≤1/year) versus frequent (>1/year) future respiratory-related hospitalizations were defined: one with the adjusted CAT score that correlated best with future hospitalizations and one with the original CAT score. Patient characteristics related to future hospitalizations (p ≤ 0.2) were also entered. Eighty-two COPD patients were included. The CAT algorithm derived from the nurse focus group was a borderline significant predictor of hospitalization risk (odds ratio (OR): 1.07; 95% confidence interval (CI): 1.00–1.14; p = 0.050) in a model that also included hospitalization frequency in the previous year (OR: 3.98; 95% CI: 1.30–12.16; p = 0.016) and anticholinergic risk score (OR: 3.08; 95% CI: 0.87–10.89; p = 0.081). Presence of ischemic heart disease and/or heart failure appeared ‘protective’ (OR: 0.17; 95% CI: 0.05–0.62; p = 0.007). The original CAT score was not significantly associated with hospitalization risk. In conclusion, as a predictor of respiratory-related hospitalizations, an adjusted CAT score was marginally significant (although the original CAT score was not). ‘Previous respiratory-related hospitalizations’ was the strongest factor in this equation.
Keywords
Introduction
Chronic obstructive pulmonary disease (COPD) is a common cause of disability, hospitalization and mortality. 1,2 COPD exacerbations are common and contribute to disease progression, 3 hospital admissions and death among patients with COPD. 4
The current Global Initiative for Chronic Obstructive Lung Disease (GOLD) Strategy recommends categorizing patients’ risk of adverse outcomes by evaluating not only the degree of airflow limitation but also the past exacerbation frequency and the current level of symptoms. 5 This combined COPD assessment is based on patient-centred outcomes that can be assessed by validated measurements. However, performing spirometry is not always feasible, especially in primary care settings. 6,7
Health status is reported to be at least as important as spirometry in predicting risk of exacerbations, hospitalizations and death. 8 The COPD assessment test (CAT) is one of the tools recommended by the GOLD Strategy for evaluating overall health status and documenting symptoms in patients with COPD. 9 The well-validated CAT contains eight items, which cover common symptoms in patients with COPD, each scored on a 5-point Likert scale. 9 A higher summed final score indicates worse health status. The CAT score correlates well with the St. George’s Respiratory Questionnaire 10,11 and is responsive to pulmonary rehabilitation and recovery from COPD exacerbations. 12,13
Clinicians in our hospital raised the question whether the CAT score could also have predictive value in clinic-based assessment of COPD patients. Literature showed that slightly higher baseline CAT scores were found in patients who were admitted to the hospital 1 year after completing the CAT 14 and in patients having moderate to severe COPD exacerbations during 6 months of follow-up. 15 The CAT may therefore also have predictive value in clinic-based assessment in COPD patients. 14,15
Currently, all CAT items are given the same weight when calculating the overall CAT score. Literature suggests, however, that some items might be more strongly related to outcomes of disease severity than others. Patients with COPD having chronic mucus hypersecretion are, for example, at significantly higher risk of COPD exacerbations, 16,17 a common cause of hospitalizations in patients with COPD. 4,5 The items cough and phlegm could therefore be expected to be of more importance in predicting respiratory-related events than other items.
In this study, we have investigated whether applying different weights to the individual CAT items might strengthen associations between CAT scores and respiratory-related hospitalizations in COPD patients. We first developed and then applied several algorithms to calculate adjusted CAT scores. These algorithms were developed using qualitative analysis of local experts’ opinions and then used to determine a predictive model for future respiratory-related hospitalizations. We hypothesized that an adjusted CAT algorithm in which the individual CAT items have different weights would be a stronger predictor of future respiratory-related hospitalizations in patients with COPD than the original CAT score.
Material and methods
Several algorithms were determined for calculating adjusted CAT scores using focus group data. Subsequently, retrospective analyses were performed of outpatient data from the departments of respiratory medicine of the Repatriation General Hospital and the Flinders Medical Centre, both within the Southern Adelaide Local Health Network.
Study design
Providing CAT algorithms
Weightings for individual CAT items were derived from qualitative analysis of focus group discussions with health professionals. One focus group was conducted with respiratory nurses and another with advanced respiratory trainees and respiratory physicians together. All participants provided signed informed consent prior to participating in a single focus group.
At the start of each focus group, the demographic and descriptive characteristics of participants and information regarding their current CAT usage were collected. Before and after the focus group discussion, all participants were asked to write down the three CAT items that they thought were most important and another three they considered least important in relation to respiratory-related hospitalizations.
During the focus group discussions, all CAT items were discussed and participants were asked if they thought the items were more important or less important in predicting the risk of respiratory-related hospitalizations and why. They were also asked to assign a weight difference between the most and least important items. Each focus group lasted approximately 1 hour. Investigator CAB was the moderator of the focus groups; investigators TWE and JMS were present to observe the discussion and to make notes. Each focus group discussion was audiotaped and later transcribed. After analysis, a summary of the focus group discussion and the adjusted item weightings were sent to the participants by e-mail.
Selection of patient data
Patient data were collected retrospectively by screening case notes and searching electronic patient databases between February and June 2014. Three hospital databases were screened for eligible patients: (a) patients in the Respiratory Integrated Care Service (RICS), a nurse practitioner led program directed towards intense case management of COPD patients with high rates of hospitalizations for COPD care; (b) patients receiving home oxygen therapy for their respiratory disease; and (c) patients visiting the outpatient clinic of a respiratory physician.
To be eligible for the current study, the patients had to meet the following criteria: (a) having a clinical diagnosis of COPD according to GOLD; 5 (b) having completed the CAT at least 6 months ago while being in a stable phase of their COPD; (c) having no other serious lung diseases; and (d) having no terminal diseases (death likely within 12 months).
Approval for this study was given by the Southern Adelaide Clinical Human Research Ethics Committee (approval no. 553.13).
Sample size
Based on expert opinion, we assumed that approximately 40% of the eligible patients (who had advanced disease) would be frequently hospitalized in the year after completing the CAT (defined as >1 hospitalization per year) because of respiratory problems. Assuming that a maximum of three characteristics would be included in the final multivariate model, a patient sample of approximately 80 was calculated to be sufficient to determine the multivariate model.
Outcomes
The primary outcome for the multivariate analyses was defined as the number of respiratory-related hospitalizations in 12 months after completion of the CAT.
Prior to the start of the study, literature was explored to define which patient variables needed to be considered for multivariate analyses because of their association with respiratory-related events (i.e. exacerbations, hospitalizations and/or death; Figure 1).
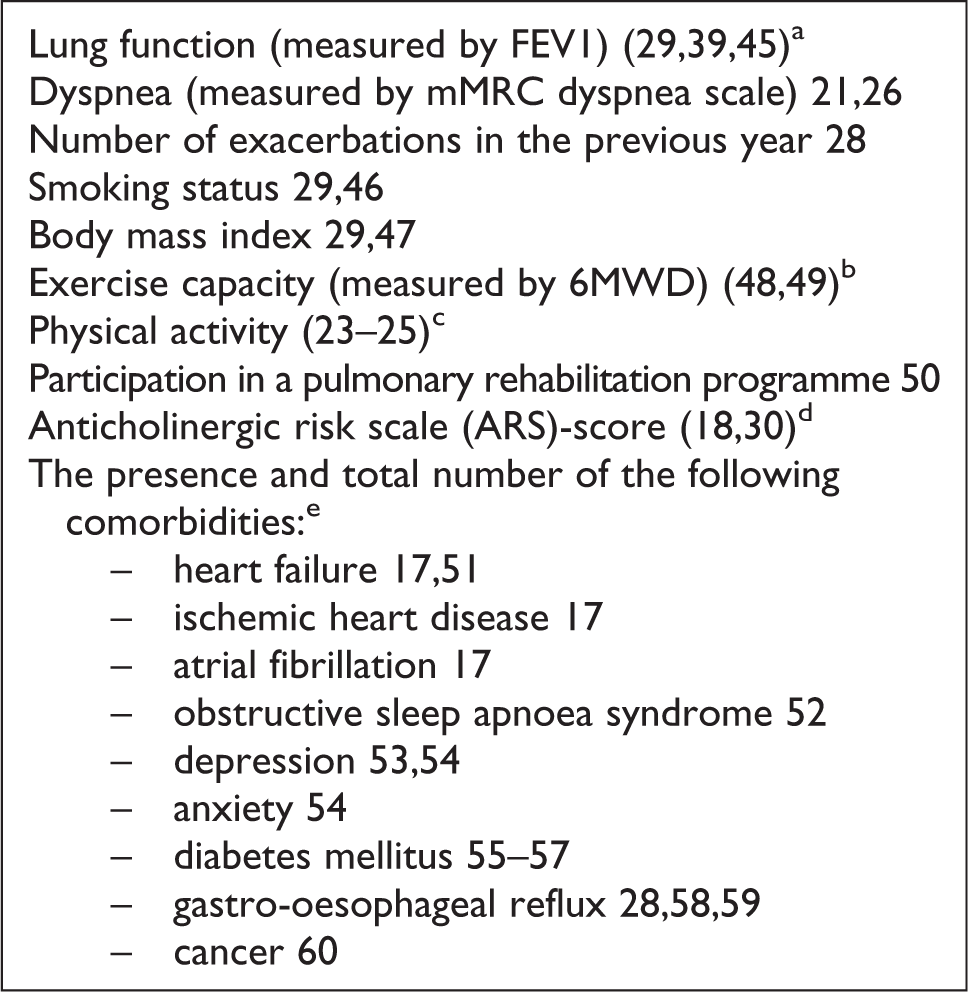
COPD patient characteristics associated with respiratory-related events (exacerbations/hospitalizations/death) and collected for all included patients. COPD: chronic obstructive pulmonary disease; FEV1: forced expiratory volume; mMRC: modified Medical Research Council dyspnoea scale; 6MWD: 6-minute walk distance. aThe window for valid lung function tests was defined as 6 months before and 6 months after completion of the CAT; if a lung function was not available in this window, it was defined as a missing. bNot tested in univariate analysis because of the high number of missing variables. cNot collected because in most medical records physical activity level was not clearly documented. dThe anticholinergic risk scale (ARS) 18 estimates the risk of anticholinergic adverse effects of a drug (0: limited or no risk and 3: very strong risk). The ARS of the individual prescribed drugs were added up to provide the ARS score. The ARS score 19 was adjusted according to Rudolph et al. 18 by adding the inhaled agents tiotropium and ipratropium to the original ARS score. eThe medical history of each patient was reviewed to determine their co-morbidities.
Analyses
Focus groups
Immediately after each focus group, a first CAT algorithm was made by the three investigators present (CAB, TWE and JMS). Subsequently, two of the investigators (TWE and JMS) independently provided a second algorithm for each focus group using audio recordings and/or the written focus group reports. The final algorithms were then determined by all three investigators (CAB, TWE and JMS) taking into account those previously defined (n = 3) for each focus group and the data regarding the three most and least important items as marked by the participants at the end of each focus group.
Weightings of the individual CAT items were assigned a value higher than one where a majority of focus group participants considered an item as ‘more important’ and lower than one if the majority considered it ‘less important’.
Models
For patients with follow-up data of less than 12 months, hospitalization rate was adjusted by using the following calculation: (12/number of months of follow-up) × number of hospitalizations during follow-up. Death was scored as a substitute for hospitalization for these patients. The number of hospitalizations was dichotomized: ≤1 per year or >1 per year.
Data were presented as mean and standard deviation (SD) for normally distributed continuous variables, median and interquartile range (IQR) for non-normal distributed continuous variables, and as a number and percentages for categorical variables.
The original and adjusted CAT algorithms were applied to raw CAT data to calculate original and adjusted CAT scores. Univariate associations with the respiratory-related hospitalization frequency were then tested for these CAT scores and for the relevant patient characteristics using Student t-tests, Wilcoxon’s rank sum tests, χ 2 tests, Fisher’s exact tests and Pearson/Spearman rank correlation tests, as appropriate. The adjusted CAT algorithm that exhibited the highest correlation with the frequency of respiratory-related hospitalizations as well as patients’ characteristics with a significance at or below p = 0.2 were then entered in a multivariate logistic regression analysis (bottom-up procedure). In case of multicollinearity, the variable that was most relevant to the research purpose was included. A second multivariate logistic regression analysis was performed in which the original CAT score was entered together with the patients’ characteristics that were entered in the first multivariate model. The statistical analysis was performed with IBM SPSS statistics version 20.
Results
Patient characteristics
There were 82 patients included in the study, 54% (n = 44) from the ‘home oxygen database’, 35% (n = 29) from the ‘Respiratory Integrated Care Service database’, and 11% (n = 9) from the respiratory physician clinic list. The total original CAT score (oxygen database: 17.1 (SD: 5.8); RICS database: 20.7 (SD: 8.6); respiratory physician clinic list: 22.4 (SD: 7.3)) and the number of people with frequent (>1) previous hospitalizations (oxygen database: 16%; RICS database: 86%; respiratory physician clinic list: 11%) were significantly different between the three databases (p < 0.05). Follow-up time for 13 patients was less than 12 months, while the median follow-up time was 12 months (IQR: 12–12). Eight deaths occurred in the period between completion of the CAT and data collection. The baseline characteristics of the patients are shown in Table 1.
Baseline characteristics of included patients stratified by frequency of hospitalizations.a

SD: standard deviation; IQR: interquartile range; n: number of patients; FEV1: forced expiratory volume in 1 second (litres); FEV1%: percentage of predicted FEV1; FVC: forced vital capacity (litres); GOLD: Global Initiative for Chronic Obstructive Lung Disease; ARS: anticholinergic risk scale; RICS: Respiratory Integrated Care Service; BMI: body mass index; mMRC: modified Medical Research Council dyspnoea scale; CAT: COPD assessment test.
aIQR is reported as 25th–75th percentile.
b p-Value of univariate associations between patient characteristics and future hospitalization frequency (infrequent (≤1/year) vs. frequent (>1/year)).
cVariable considered to be eligible in the multivariate logistic regression model based on p-value ≤0.200.
d p-Value of dichotomized variable: GOLD stage: I–III vs. IV (reason: low number of patients with GOLD stages I and II); mMRC score: 0, 1 and 2 vs. 3 and 4 (reason: low number of patients that scored 0 or 1); number of hospitalizations in prior year: ≤1 hospitalizations per year vs. >1 hospitalizations per year; ARS-score: 0–2 vs. ≥3.
eVariables ‘heart failure’ and ‘ischemic heart disease’ combined because of strong correlations between variables.
fThe ARS score 19 was adjusted according to Rudolph et al. 18 by adding the inhaled agents tiotropium and ipratropium to the original ARS score.
1–9Patients with valid measures (n (% of total included patients)): 182(100), 246(56); 361(74); 468(83); 581(99); 676(93); 767(82); 877(94); 958(71).
Development of CAT algorithms
Five female nurses with a mean age of 41 years (SD: 11.1) and a mean working experience in the respiratory field of 9 years (SD: 5.6) participated in focus group 1. Three of them used the CAT regularly (at least once per week), one of them used it sometimes, and one participant had used it regularly in the past. Quotes from this focus group discussion and participants’ rankings of the importance of the different CAT items in relation to respiratory-related hospitalizations are given in Table 2.
Quotes of the focus group with respiratory nurses and their ‘importance’ rankings of the different CAT items in relation to respiratory-related hospitalizations.
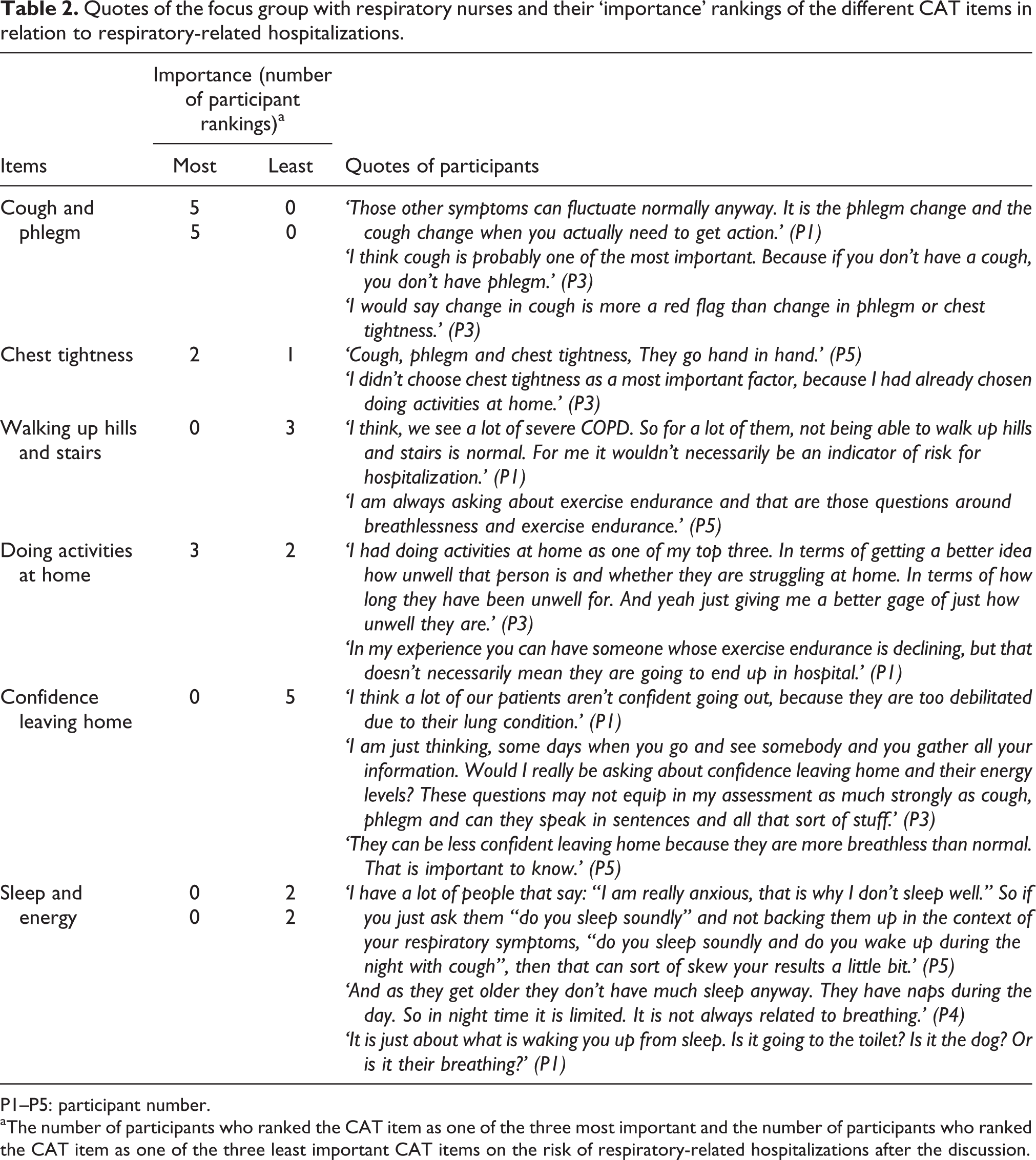
P1–P5: participant number.
aThe number of participants who ranked the CAT item as one of the three most important and the number of participants who ranked the CAT item as one of the three least important CAT items on the risk of respiratory-related hospitalizations after the discussion.
In focus group 2, four respiratory physicians (three male) and two respiratory advanced trainees (both female) participated. They had a mean age of 41 years (SD: 13.1) and a mean working experience in the respiratory field of 17 years (SD: 15.7). None of the participants used the CAT regularly, but all were aware of the content of the CAT. Quotes from this focus group and participants’ rankings of the importance of the different CAT items in relation to respiratory-related hospitalizations are given in Table 3.
Quotes of the focus group with respiratory physicians/advanced trainees and their ‘importance’ rankings of the different CAT items in relation to respiratory-related hospitalizations.

P6–P11: participant number.
aThe number of participants who ranked the CAT item as one of the three most important and the number of participants who ranked the CAT item as one of the three least important CAT items on the risk of respiratory-related hospitalizations after the discussion.
The final weights for the two adjusted CAT algorithms are listed in Table 4.
Derived algorithms of CAT scoring and the predictive value on respiratory-related hospitalizations.

CAT: COPD assessment test; SD: standard deviation.
a p-value of univariate associations between (adjusted) CAT scores and future hospitalization frequency (infrequent (≤1/year) versus frequent (>1/year)).
The predictive value of the CAT algorithms in multivariate models
The results of the univariate analyses are given in Tables 1 and 4. In the first multivariate regression model for respiratory-related hospitalization risk (Table 5), the adjusted CAT score based on weightings developed from focus group 1 (respiratory nurses) showed borderline significance controlling for other variables with univariate significance p = 0.2 or below. Patients with frequent hospitalizations (>1) in the year prior to completing the CAT had an almost four times higher risk of having frequent hospitalizations (>1) in the follow-up year. Patients with ischemic heart disease and/or heart failure had a significantly decreased risk of having frequent respiratory-related hospitalizations in the following year and the anticholinergic risk scale (ARS) score (≥3) was positively related to respiratory-related hospital admissions in the following year. The adjusted CAT score contributed to the best fitted model (difference of −2 log-likelihood: 4.134 (p < 0.05)). This model explained 36.4% of the variance. The modified Medical Research Council dyspnoea scale was not entered in the model because of the significant correlation with the adjusted CAT score (p = 0.04). The GOLD stage was not included in the model because of the high number of missing spirometry values.
Logistic multivariate regression model for respiratory-related hospitalizations (≤1/year vs. >1/year).a

CAT: COPD assessment test; OR: odds ratio; 95% CI: 95% confidence interval.
aModel based on 76 patients with valid measurements. Explained variance: 36.4%; −2 log-likelihood: 75.534.
In the second multivariate regression model (Table 6), the original CAT score was not significantly related to the frequency of respiratory-related hospitalizations and did not contribute to the best fitted model (difference of −2 log-likelihood: 3.50 (0.10 > p > 0.05)).
Logistic multivariate regression model for respiratory-related hospitalizations (≤1/year vs. >1/year).a

CAT: COPD assessment test; OR: odds ratio; 95% CI: 95% confidence interval.
aModel based on 76 patients with valid measurements. Explained variance: 35.5%; −2 log-likelihood: 76.168.
Discussion
Using a combination of qualitative (focus groups) and quantitative analyses, this study found that using adjusted weights for CAT items provided a better predictor of the frequency of respiratory-related hospitalizations in patients with COPD than using unadjusted CAT scores. The adjusted CAT algorithm that was based on information received from a focus group with respiratory specialist nurses correlated best with future respiratory-related hospitalizations.
In the adjusted CAT algorithm that correlated highest with future respiratory-related hospitalizations, cough and phlegm received the highest weightings, in line with published studies showing cough 20 and chronic mucus hypersecretion were strong predictors for COPD exacerbations and death. 8,16,17,20 –22 Other items allocated a weight higher than one in this algorithm were ‘chest tightness’ and ‘doing activities at home’. We were unable to find literature reports indicating an association between chest tightness and hospitalizations in patients with COPD. Several studies have however confirmed that physical activity is associated with exacerbations and hospital admissions. 23 –25 Results of our univariate analyses and literature both indicate an association between dyspnoea and hospitalizations in COPD patients. 26 Allocating a higher weighting to the CAT item ‘breathlessness walking up hills and stairs’ (which covers dyspnoea) may therefore also improve the predictive value of the adjusted CAT score further. In our study, however, this item was not adjusted because it was not rated by the focus group participants as more important than other items.
The CAT was developed to assess the impact of symptoms on the life of individual patients with COPD. 9,10 The CAT summary score was found to correlate well with the St. George’s Respiratory Questionnaire, a standard test of respiratory-related health-related quality of life and health status. 10,11 Responsiveness to pulmonary rehabilitation has been demonstrated and a high CAT score appeared to be associated with future hospitalizations. 14,15,27 The CAT therefore has a range of advantages, one of which may be to predict risk of future hospitalizations. We did, however, not find a significant relationship between the original CAT score and future hospitalizations in this sample of patients with severe COPD. Whereas the adjusted CAT score showed only a borderline significant relationship with future respiratory-related hospitalizations, the variable nonetheless contributed to the best fitted model in the prediction of respiratory-related hospitalizations in our study. Because the odds ratio was low, though, the clinical relevance of the adjusted CAT score alone as a predictor of the risk of respiratory-related hospitalizations needs to be considered carefully. The adjusted CAT score might be more helpful in assessing the hospitalization risk in COPD patients when combined with other factors that assess hospitalization risk. Combining the adjusted CAT score, for example, with the simple measure of ‘number of hospitalizations in the year before assessment’, 28,29 may help the health care professional to generate quickly a reliable indication of the patients’ risk of hospitalizations and thereby to make better management decisions. This approach is in line with the GOLD 2016 Strategy 5 encouraging multidimensional patient assessment that addresses an individual’s symptoms and/or health status, their severity of airflow limitation and exacerbation history to stratify their risk of adverse outcomes. However, large prospective validation is necessary to evaluate whether the adjusted CAT adds any value beyond using the strong predictor ‘prior hospitalizations’ alone when assessing hospitalization risk. Likewise, it would be of further interest to evaluate the validity of the adjusted CAT for measuring health status (as well as the original CAT 9 ) in a wider range of COPD severities, to give a better indication of the usefulness of the adjusted CAT alone for the assessment of COPD patients.
Interestingly, the ARS score was related to respiratory-related hospitalizations in our COPD population, in line with a paper describing an association between the ARS score and all-cause hospital readmission in vulnerable patients of >65 years age. 30 Use of agents with anticholinergic effects is common in patients with greater multimorbidity, 31 and sensitivity to these effects is expected to be greater in older people. 32 Both are common features in patients with COPD. 33 Moreover, inhaled anticholinergic drugs are frequently prescribed for these patients. Further prospective studies are warranted to explore the relation between the anticholinergic risk score and risk of adverse outcomes in patients with COPD.
More evidence is also needed to explore the relationship between the presence of ischemic heart disease and/or heart failure and hospitalization risk in patients with COPD. The strong but unexpected negative correlation we found between these factors was in contrast with findings of previous studies. 17 However, in a COPD self-management study, it was found that patients who had comorbid cardiac disease were more likely to adhere to their action plan for treatment of their exacerbations. 34 They may be ready to initiate their treatment earlier and thereby avoid more severe COPD exacerbations for which hospitalization would be required. We cannot determine whether this was the case in our study population, but the strength of our finding also warrants further investigation.
In both of our focus groups and in literature, it was suggested that some CAT items are influenced by co-morbidities of patients with COPD, 35 leading to a higher total CAT score. Literature also shows that co-morbidities often lead to an increase of hospitalizations in patients with COPD. 17,36 More research about the influence of co-morbid conditions on the different CAT items and on respiratory-related hospitalizations is necessary and could be helpful to develop the best CAT algorithm for predicting respiratory-related hospitalizations.
The fact that the ‘Respiratory Integrated Care Service’ patients have accounted for a relatively high number of cases with frequent hospitalizations is not surprising because having a high hospitalization risk is a criterion for inclusion in this programme. Apart from the hospitalization frequency, we do however not have a clear explanation for the difference in CAT scores between the databases. Overall, our study results cannot be generalized to the whole COPD patient population, as most patients had GOLD stage III–IV and all received secondary healthcare. GOLD stage could not be included in the multivariate analyses because of the high number of missing spirometry values; it was however related to respiratory-related hospitalizations in the univariate analyses. This is in line with previously published studies data. 28,29,37 –39 Other variables not included in the analyses because of insufficient data are exercise capacity, physical activity and arterial oxygen saturation (PaO2), even though they were associated with respiratory-related events in previous studies. 23,25,40 –44 Using a prospective design in the future will allow collecting a more complete set of variables for analyses. In such a future study, it would be interesting to include the patient’s perspective (by e.g. including a patient focus group), because the CAT is developed as a patient-reported outcome. 9 Further, the generalizability of the results would increase by adding focus groups incorporating healthcare providers with different clinical experiences and from a variety of centres and countries. Finally, we acknowledge that it would have strengthened our conclusions if we had included a longer follow-up and a larger patient population.
Conclusion
The adjusted CAT score described in this article may help predict respiratory-related hospitalization risk in severe and very severe patients with COPD who receive secondary healthcare, especially in conjunction with prior hospitalizations. Further prospective studies are necessary to confirm this.
Footnotes
Author Note
Department to which the work should be attributed: Department of Respiratory Medicine, Repatriation General Hospital, Daws Road, Daw Park, South Australia 5041, Australia/Department of Respiratory Medicine, Flinders Medical Centre, Flinders Drive, Bedford Park 5042 South Australia, Australia.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: A potential conflict of interest associated with this publication is Peter Frith’s advisory work with GlaxoSmithKline Australia, and his being on the Board of Directors of GOLD. There are no other conflicts of interest associated with this publication.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.