
Abstract
The purpose of this study was to investigate whether there is evidence that individuals with severe idiopathic pulmonary fibrosis (IPF) have cognitive deficits when compared to individuals with healthy lungs. Participants completed five neuropsychological tests: Trail Making Test (TMT) A and B, Stroop Color Word Test (1, 2, 3), Hopkins Verbal Learning Test, Boston Naming Test, and Grooved Pegboard Test, additionally, the short form-36 and Beck Depression Index. Twelve participants (7 male, mean age 69.3, 9.4 years) comprised the severe IPF group defined by a diffusion capacity for carbon monoxide (DLCO) <30%. Thirty-four patients (22 male, mean age 63.2, 9.6 years) comprised the mild-to-moderate group with a DLCO >30%. Participating spouses (n = 15, 4 male) served as the control group and had a mean age of 66.0, 10.8 years. Controlling for gender and age, the severe group had a significantly longer mean TMT B time (69.4, 135.9 seconds) than the mild group and the control group (86.7 seconds vs 83.2 seconds; p = 0.004 and 0.008 respectively), suggesting inferior performance on tasks requiring speed divided attention. In addition, the severe group had a significantly lower number of correctly identified colors in the Stroop 3 test (22.4 vs 30.6 vs 38.6; p < 0.001), suggesting slower processing speeds when requiring suppression of a familiar response. Participants with severe IPF had worse cognitive function than mild IPF or control subjects. Further research is needed to explain these findings and to develop interventions tailored to address these deficits.
Cognitive function in IPF
Idiopathic pulmonary fibrosis (IPF) is a terminal illness characterized by progressive fibrosis of the lung parenchyma and worsening ventilatory restriction. The disease course is relentless, ultimately escalating to respiratory failure and death. 1 –4 It is estimated that, in the United States, IPF affects between 13,000 and 200,000 individuals and results in 50,000 deaths/year. 5 The median age at diagnosis is 63 years, and the median survival is less than 3 years from diagnosis. 6 The diagnosis of IPF is based upon combined clinical, radiologic, and pathologic criteria as defined by the American Thoracic Society (ATS). 7 Early clinical manifestations of IPF include dyspnea and cough with minimal to no sputum production.
Until recently, no single or combined agent had been found beneficial for the treatment of IPF. In May 2014, the results of two separate pharmaceutical studies were published to show that pharmaceutical agents nintedanib and pirfenidone slow the progression of the disease compared to placebo. Although promising, the resulting decline in disease progression is minimal and neither agent is without adverse effects. 8,9 Therefore, the current management of IPF focuses on symptom relief, pulmonary rehabilitation, treatment of comorbidities, and lung transplantation.
There is very little information about the impact of this disease on cognitive function. From anecdotal clinical experience at a tertiary referral center, patients with severe IPF appear to have a difficult time grasping and recalling certain concepts pertaining to their illness and/or plan of care.
Although neurocognitive decline has not exclusively been studied in IPF, it has been shown in other similar illness such as chronic obstructive pulmonary disease (COPD) and heart failure. 10,11 Changes in cognitive function can manifest in areas such as memory, concentration, learning, and visual–motor response speeds. 10 Cognitive decline may further decrease the quality of life of patients and families and is associated with mood disturbances, functional limitations, and increased health-care expenditures. 10,11 This phenomenon poses a clinical challenge as these patients may require closer management and increased resource utilization in between clinic visits. In addition, it can hinder patient comprehension of information given by clinicians and negatively impact patients’s compliance with recommended therapies and self-care.
The purpose of this study was to investigate whether there is evidence to suggest that individuals with severe IPF have cognitive deficits. The correlation between the extent of cognitive impairment and disease severity or oxygen dependence in advanced COPD has been well documented across multiple studies. 11 It has been found that cerebral perfusion in COPD patients is significantly altered, with more abnormalities seen in participants requiring supplemental oxygen therapy. A correlation may be seen between the brain perfusion scans and neurocognitive test results, suggesting that decreased perfusion may be responsible for the decline in verbal memory, delayed recall, and ability to pay attention. 12 Such results imply that as COPD progresses, it may bring about, or even increase abnormalities in cognitive function. If this trajectory is also true in IPF, health-care professionals caring for these individuals should be conscious of their increased risk for cognitive deficits and plan accordingly to manage their care.
Methods
This study was a prospective, cross-sectional, descriptive study. After obtaining approval from the institutional review board at the University of Minnesota, United States, patients with an IPF diagnosis were identified from the University of Minnesota Health’s interstitial lung disease program clinical database and were approached to determine interest in participating. Each consecutive patient with IPF who presented for a clinic visit (either new or as a follow-up) was asked to participate in the study. For patients who agreed to participate, their spouses were also asked to participate to make up a control group that would be demographically matched to the IPF participants.
Inclusion criteria for the IPF groups included a well-documented diagnosis of IPF per the 2000 ATS guidelines. 13 Exclusion criteria for all groups included a history of brain trauma, including a history of cerebral vascular accident or recent concussion (in the past year); known diagnosis of a neurologic condition that affects cognition; participant’s native language was not English (study materials are not available in foreign languages); and/or the participant was color-blind, as the Stoop Color Word Test’s (SCWT) results would be affected by this condition. To better reflect individuals living with IPF, participants were not excluded based on comorbidities known to affect oxygenation such as pulmonary hypertension and/or sleep apnea.
After participants consented, baseline demographic and clinical data including 6-minute walk distance (6MWD), spirometry, diffusion capacity for carbon monoxide (DLCO), echocardiogram, and computed tomography scan imaging were obtained. Eligible participants were asked to complete the following previously validated cognitive function tests: Trail Making Test (TMT) A and B, the SWCT, the Hopkins Verbal Learning Test–Revised (HVLT-R), the Boston Naming Test (BNT), the Grooved Pegboard, and the Health-Related Quality of Life Short form-36 (HRQOL SF-36) questionnaire. The Beck Depression Index-II was used to assess depression because it has been associated with both subjective complaints of cognitive dysfunction and decreased performance on objective neuropsychological testing.14 Testing was performed in a quiet area, free from outside disturbances. Participants completed all testing in approximately 1 hour. Two study personnel supervised the test: one administered the tests and the other was keeping time.
Participants were stratified based on the % of predicted DLCO. This decision was based in part on the clinical observation that at the University of Minnesota Health, IPF patients had a greater level of variance in their DLCO than in their forced vital capacity (FVC). Additionally, there is evidence to suggest that using the DLCO as an indicator was more likely to correspond with supplemental oxygen requirements. 15 Therefore, study subjects were a priori stratified into three groups based upon the DLCO enrollment criteria of several clinical trials that were recruiting participants at that time: control (no evidence of IPF or known condition that affects cognitive function), mild-to-moderate IPF (DLCO >30%), and severe IPF (DLCO < 30%). The primary outcome was the trail making exercise part B to detect a difference of 1 SD in mean test scores between the severe IPF patients and the controls using two-sample t-test, with a sample size of 27 per group yielding a power of 0.910. Since there are multiple comparisons in this protocol, the type 1 error α was set up to be 0.025 in the above-mentioned power analysis.
TMT A and B
Test takers must draw pencil lines to connect, in numerical order, 25 encircled numbers randomly arranged on a page (part A) and 25 encircled numbers and letters in alternating order (part B). These tests measure speed for attention, sequencing, mental fexibility, and visual search and motor function. 16 Scoring is expressed in terms of time, in seconds, required for the completion of the test, up to a maximum of 5 minutes.
Stroop Color Word Test
The SWCT measures information processing speed, selective attention, cognitive flexibility, and executive function in terms of an individual’s ability to suppress habitual response in favor of an unusual response. 17 There are three components to the Stroop test, all requiring individuals to correctly identify as many objects as possible within the time limit of 45 seconds. The first exercise requires participants to read the names of colors printed in black ink. The second exercise requires participants to name colors printed in the form of “XXXX” in red, yellow, or blue ink. The last, and most difficult, exercise contains the same words and colors as the previous two exercises, only now, participants are asked to name the color of the ink, and not read the word (for example, if the word GREEN was printed in red ink, participants would have to say “red” to answer correctly).
Hopkins Verbal Learning Test–Revised
The HVLT-R consists of a 12-item word list, made up of four words from each of three well-known semantic categories. In this case, the categories were animals, precious gems, and housing. A total recall score and a learning index are calculated. After 20 minutes, delayed recall of the word list is tested. Next, there is a yes/no recognition component from a list of 24 words, 12 authentic and 12 distracters. A discrimination index is calculated by substracting the false positives from the true positives. This test serves as a brief assessment of verbal recall and recognition. 18
Boston Naming Test
Object naming is frequently used to identify specific cognitive deficits related to accessibility of lexical and semantic information. 19 The BNT consists of 60 line drawings of items arranged from more recognizable (such as a pencil) to less recognizable (such as a protactor).
Grooved Pegboard
The Grooved Pegboard assesses motor tasks by evaluating eye–hand coordination and motor speed. Successful completion of the Grooved Pegboard requires sensory–motor integration and motor processing. 20 Beginning with the dominant hand, participants are timed, in seconds, as they rotate and place pegs into position on the board. The test is then repeated with the nondominant hand.
Short form-36
HRQOL is an integral component for measuring the impact and progression of chronic diseases. The SF-36 is a generic, multipurpose health status questionnaire designed to measure functioning and well-being along eight scales, each representing a different dimension of health. The eight dimensions include physical functioning, role physical, bodily pain, general health, vitality, social functioning, role emotional, and mental health. 21 Lower scores on the SF-36 are indicative of poorer HRQOL.
Beck Depression Inventory-II
The Beck Depression Inventory-II (BDI-II) is a widely used self-reporting measure of the intensity of depressive symptomatology consisting of 21 items. Higher scores are indicative of greater symptoms of depression. The rationale for including this test was derived from the results of previous studies, which found inverse associations between depressive symptoms and cognitive function. 22
Statistics
For categorical variables, Fisher’s exact test was used to examine whether the frequency distribution is different between groups with the respective p values being presented. For continuous variables, two-sample t-tests (to compare two groups for total 6MWD in feet, DLCO, and FVC) or analysis of variance (ANOVA) F-tests (to compare three groups for the other continuous variables) were performed to evaluate whether the means were different from each other. When comparing three groups, an overall p value from ANOVA F-test was presented. If the overall p value was ≤0.05, multiple comparisons were performed with Tukey–Kramer adjustment for the p values in order to assess which means differ from other means. The adjusted p values ≤0.05 are presented in Tables 1 and 2. All analyses were performed using SAS 9.1.3 (Carey, North Carolina, USA). Two-sided t-tests with p ≤ 0.05 denote statistical significance.
Demographics.a

aValues listed for age are means with the range in parentheses. The rest of the values represent the number of participants.
Data collection took place between November 2009 and April 2011. Of a total of 48 eligible IPF patients, 46 consented to participate. The two who declined participation did so due to lack of time. Of the 46 consented patients, 12 participants made up the severe IPF group (26%), of whom 7 were men (see Table 1 for demographics and Table 2 for comorbidities). Thirty-four participants (74%) made up the mild-to-moderate IPF group, of whom 22 were men. Fifteen family members (four were men) agreed to participate as the control group, thus age not was statistically different among the groups. All participants were Caucasian and long-term residents of the Midwest. Although the original intent was to keep enrolling until each group had at least 27 participants, recruitment and data collection were closed in April 2011 due to decreased participant enrollment.
Comorbidities.a

CVA: cerebral vascular accident.
aValues listed represent the number of participants that identified the listed condition as part of their health history.
Individuals with severe disease had shorter 6MWD, walking on average 500 feet less than patients in the mild-to-moderate group (<0.0001) and were more likely to require supplemental oxygen therapy (0.01; see Table 3 for pulmonary function test values).
Pulmonary function tests.a
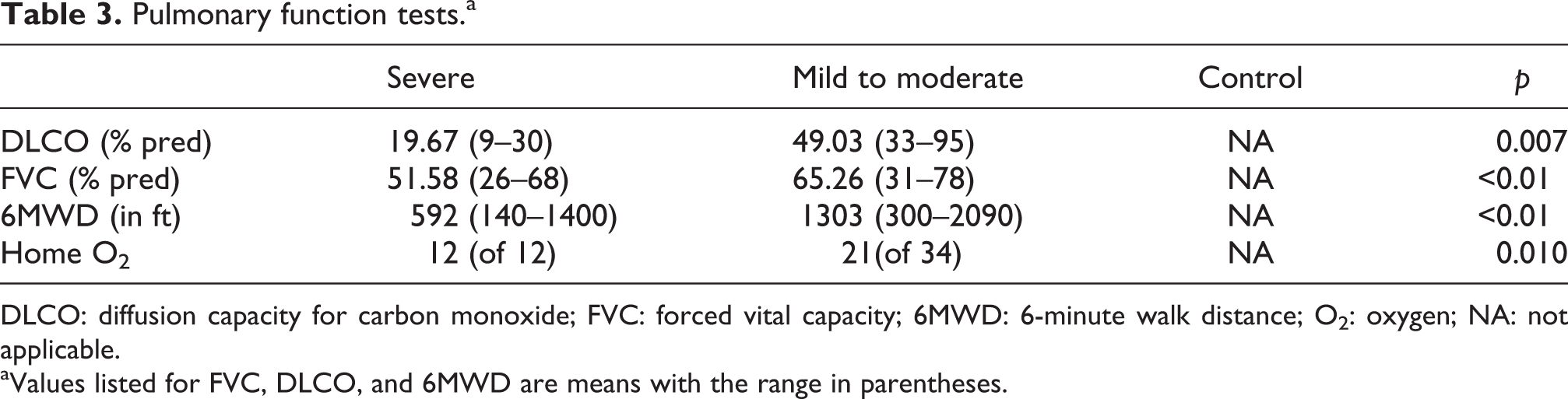
DLCO: diffusion capacity for carbon monoxide; FVC: forced vital capacity; 6MWD: 6-minute walk distance; O2: oxygen; NA: not applicable.
aValues listed for FVC, DLCO, and 6MWD are means with the range in parentheses.
The severe IPF group had a significantly higher mean TMT B time (135.9 seconds, SD = 69.4) than the mild-to-moderate IPF group or the control group (86.7 seconds [34.8] vs. 83.2 seconds [35.4]; p value 0.004 and 0.008; see Table 4 for cognitive function test results). After adjusting for gender and age, differences were still significant (p values 0.017 and 0.019, respectively). Participants with severe IPF performed more poorly on the cognitive function tests than those with mild-to-moderate IPF and the control group. The most significant differences were on measures of speed divided attention (TMT B), processing speeds requiring suppression of a familiar response (Stroop 3), psychomotor speeds (Grooved Pegboard—both hands), and to a lesser extent, confrontation naming (BNT). In all cases, the findings were consistent with the severe IPF patients performing worse than the mild-to-moderate group and the control group.
Results of cognitive function tests, SF-36, and BDI-II.

IPF: idiopathic pulmonary fibrosis; TMT: Trail Making Test; HVLT, DR: Hopkins Verbal Learning Test, delayed recall; BNT: Boston Naming Test; SF-36: short form 36; BDI-II: Beck Depression Index II.
aDominant hand.
bNondominant hand.
Discussion
The results of this study suggest that IPF participants with severe disease have worse cognitive function than those with mild-to-moderate disease and controls. They are also more likely to have poorer HRQOL (Figure 1) and symptoms of depression (Figure 2). These findings support the original hypothesis that individuals with severe IPF have poorer cognitive function.
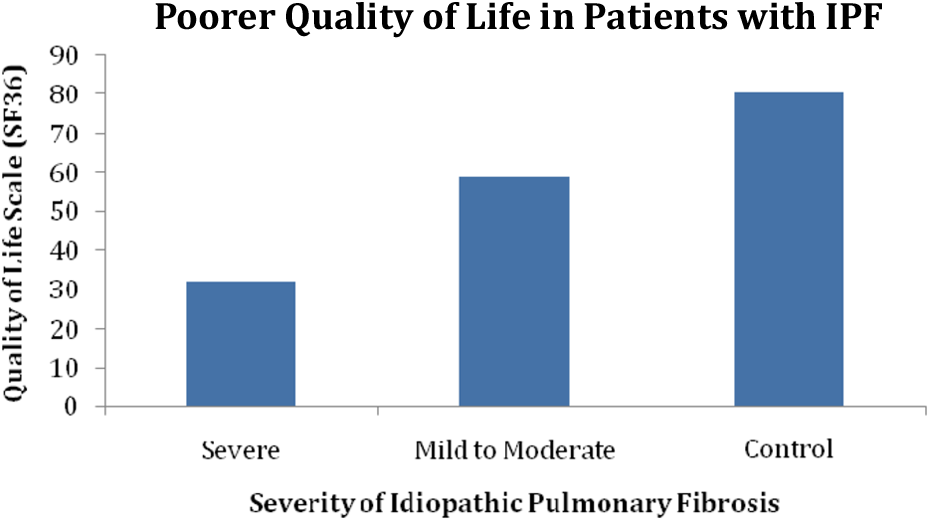
Participants with severe IPF scored lower on the SF-36 HRQOL questionnaire.

Despite lower HRQOL scores, DBI-II depression scores among participants with severe IPF were not suggestive of clinically meaningful depression.
These findings also support what has previously been shown that individuals with IPF suffer from worse HRQOL. 6 HRQOL is especially important in this patient population, given the lack of treatment options, poor mortality, and rapid progression of the disease.
Acknowledging that individuals with severe IPF may have worse cognitive function may help identify them as at risk for poorer self-care, the natural decision-making process of maintenance, monitoring, and management. In patients with heart failure, better self-care has been shown to increase HRQOL and self-reported health status, with neuropsychological decline being associated with poorer self-care and decreased compliance with treatment recommendations. 23 For example, individuals suffering from impaired processing speeds and executive function may have altered symptom perception and delayed treatment-seeking behaviors, while those who have impaired memory may have difficulty in learning and remembering therapeutic regimes. 24 Thus, finding ways to tailor illness management intervention to aid in their self-care practices may help increase their HRQOL.
It is well known that major depressive disorder has been linked to impaired memory, trouble with tasks requiring concentration, and a general decrease in cognitive function. 22 Often it is impossible to differentiate if these cognitive abnormalities are related to actual neuropsychological impairment or by an event characterized by depression. 14
Closer examination of the BDI-II scores revealed that of the 12 participants in the severe IPF group, 1 participant obtained a score of 22, indicative of moderate depression, and 1 participant obtained a score of 29, indicative of severe depression. All other scores ranged within the minimal or mild symptoms of depression categories. While individuals with severe IPF suffered from both decreased cognitive function and increased symptoms of depression, the depression levels observed were below the threshold for clinical significance and would not require clinical intervention. Thus, it is unlikely that depression is a leading cause of decline in cognitive function. This finding supports what DeVries et al. had previously found in that while individuals with IPF may suffer from negative thoughts and feelings, they are not, in general, clinically depressed.3
All patients in the group with severe IPF had been prescribed supplemental oxygen therapy based on the ATS recommendation for IPF individuals with resting hypoxemia. 7 As expected, participants with mild-to-moderate disease required less supplemental oxygen, and of the 21 participants requiring supplemental oxygen therapy in the mild-to-moderate IPF group, some needed it only with exertion while others additionally required it at rest. Due to this wide range of supplemental oxygen requirements and the small number of participants, the impact of requiring supplemental oxygen on cognitive function was not analyzed, and statistical computations were limited to addressing the differences observed between the groups as stratified by % of predicted DLCO. Although it is known that hypoxemia will alter cognitive function, 25 it is not completely clear what level of oxygenation is needed for proper cognitive function. Another possible reason for the observed decline in cognition in this patient population may be related to an inadequacy of the clinical management of hypoxemia or nonadherence with recommended supplemental oxygen therapy.
The intent of this study was not to diagnose individuals with cognitive impairment. Although screening instruments are frequently used to quantify the degree of neuropsychological decline, cognitive impairment cannot be diagnosed by neuropsychological tools alone and requires clinical judgment. While referring patients for further assessment and/or treatment of neuropsychological changes may help provide patients and their loved ones with information and may identify a need for support, labeling individuals with a diagnosis of cognitive impairment may have psychological and psychosocial repercussions. Therefore, compared to those presenting in clinic complaining of symptoms such as impaired memory, individuals with cognitive impairment as identified by research criteria should be managed using a more conservative approach. 26
To date, there are no Food and Drug Administration-approved treatments for cognitive impairment. Studies exploring lifestyle modifications in individuals with mild cognitive impairment recommend participation in intellectual activities, physical activities, social connectedness, and adopting a “heart healthy” diet (rich in fruits, vegetables, and omega-3 fatty acids). 27
To better understand the implications of cognitive decline in IPF, further studies are needed to investigate how cognitive impairment affects mortality and disease progression. The strengths of this study lie in its clearly well-defined cohort of IPF patients, and the data obtained from multiple tests on each subject consistently demonstrating deficits across testing. These novel findings may further prove insightful in better understanding patient-related outcomes and how individuals respond to therapies. The major limitations of this study include the small sample size and its homogeneity and the unclear nature of subclinical depressive symptoms on cognition. The etiology of the observed neuropsychological impairment in this cohort of individuals with IPF remains unknown, and future studies are warranted to address this matter.
Despite its limitations, this study nevertheless suggests that patients with severe IPF have poorer cognitive function, greater symptoms of depression, and worse quality of life. How individuals with IPF perceive this diagnosis is beyond the scope of this study; however, it is likely that cognitive deficits may affect patients’ understanding of the disease process, treatment requirements, and ability to assume therapeutic self-care practices. 10 As patient-related outcomes are increasingly identified as markers of effective therapies, it is important to acknowledge that unrecognized cognitive dysfunction may influence these outcomes. These findings expand upon the current understanding of IPF and cognitive function and suggest the need for additional, larger cohort follow-up studies examining the mechanisms involved in cognitive function and the development of interventions tailored to address these deficits.
Footnotes
Disclaimer
The views expressed in this article do not communicate any official positions of the University of Minnesota or the Medical University of South Carolina.
Acknowledgments
The authors acknowledge The University of Minnesota Health Interstitial Lung Disease Clinic for supporting this project; Deborah D Roman, University of Minnesota Health, for assistance in planning this study; Jeffrey J Swigris, National Jewish Health, for input and recommendations during the development of this document; and J Alan Panelli, University of Minnesota Health, for administrative assistance.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study was provided by the University of Minnesota Health’s Interstitial Lung Disease Clinic’s Research and Education Fund.