
Abstract
The objectives of our study were to (i) compare, in chronic obstructive pulmonary disease (COPD) patients, acute responses to continuous training at high intensity (CTHI), continuous training at ventilatory threshold (CTVT) and interval training (IT); (ii) examine associations between acute responses and 12-week adherence; and (iii) investigate whether the relationship between acute responses and adherence is mediated/moderated by affect/vigour. Thirty-five COPD patients (forced expiratory volume in 1 second = 60.2 ± 15.8% predicted), underwent baseline assessments, were randomly assigned to CTHI, CTVT or IT, were monitored throughout about before training, and underwent 12 weeks of exercise training during which adherence was tracked. Compared with CTHI, CTVT was associated with lower respiratory exchange ratio, heart rate and respiratory rate (RR), while IT induced higher
Introduction
Exercise training is a key component to successful pulmonary rehabilitation (PR). 1 Current PR guidelines advocate continuous training at high intensity (CTHI) for patients with chronic obstructive pulmonary disease (COPD). 1,2 However, one issue with the use of CTHI is the associated low adherence rates. 3 Alternative approaches, including continuous training at ventilatory threshold (CTVT) and interval training (IT), have therefore been proposed as more tolerable and likely associated with better subsequent adherence. 1,4 –6
Acute response to different exercise training protocols has been examined in COPD from physiological and symptomatic perspectives. Compared to CTHI, IT has been associated with less physiological strain (lower oxygen uptake
In healthy individuals, evidence suggests that exercise intensity is negatively related to adherence. 7,8 This relationship is thought to be driven by affect, especially during the initial phase of an exercise program. 2,9 Affect can be defined as the degree of pleasure/displeasure one experiences during exercise; it includes dimensions of positive and negative affect as well as high and low vigour (i.e., one’s level of alertness). 10 The general conception is that lower exercise intensities are more enjoyable, leading to better adherence. 11 During exercise, affect has been negatively related to physiological responses of metabolic strain. 11,12 Detailed studies have further suggested that affect improves or remains stable when intensities are below or at the ventilatory threshold, 9,13 –15 and worsens above the ventilatory threshold. 9,13 –18 Accordingly, we hypothesized that affect would remain stable or improve during CTVT and, possibly as well, during IT because of the regular recovery periods; in contrast, it would worsen during CTHI, which continuously submits patients to intensities above the ventilatory threshold. We further hypothesized, that CTHI would be associated with lower adherence than CTVT and IT, and that this link would be mediated by affect/vigour.
The study objectives were to (i) compare, in COPD, the acute physiological, symptomatic and affective responses to CTHI, CTVT and IT; (ii) examine the association between acute responses and adherence to a 12-week exercise training program and (iii) investigate whether the relationship between acute responses and adherence was mediated/moderated by affect/vigour.
Methods
Study design and procedure
The present study followed a prospective parallel-group design. Eligible subjects completed baseline evaluations, were randomly assigned to CTHI, CTVT or IT, were monitored throughout an entire exercise training bout, and underwent 12 weeks of training, three times/week, according to assigned protocol (see online supplement). This study was approved by the institutional ethics committee and informed consent was obtained.
Subjects
Subjects were recruited at l’Hôpital du Sacré-Coeur de Montréal according to the following criteria: Inclusion: (1) COPD diagnosis; (2) age ≥40 years; (3) smoking history ≥10 American pack-years; (4) post-bronchodilation forced expiratory volume in 1 second (FEV1) <80% of predicted normal value; and (5) FEV1 to forced vital capacity ratio <0.7. Exclusion: (1) exacerbation of respiratory symptoms ≤4 weeks; (2) contraindication to exercise testing 19 ; (3) active condition other than COPD that can influence exercise tolerance; (4) resting or exercising supplemental oxygen; (5) participation in PR program ≤1 year; (6) current participation in an exercise training program of similar or greater dose than protocols under study 20 ; and (7) inability to complete baseline evaluations or achieve a ventilatory threshold on incremental cycling test.
Baseline assessments
Expiratory flow rates, lung volumes and lung diffusion capacity were measured according to recommended techniques. 21 Values were compared with predicted normal values from the European Community for Coal and Steel/European Respiratory Society. 22 A symptom-limited incremental cycling test was performed to rule out the presence of cardiovascular co-morbidities and to assess wattage (W) at peak effort (highest W maintained at ≥50 revolutions/minute for ≥30 seconds) and at the ventilatory threshold (determined using V-slope method 23 ) for subsequent determination of exercise training intensity (see online supplement). 24
A constant-load cycling exercise test was performed at baseline and repeated post 12 week training to measure change in exercise tolerance. The outcome was endurance time, defined as duration of pedalling at 80% of W peak (see online supplement). Evaluators were blinded to subjects’ intervention group assignment.
Exercise training protocols
Exercise training was performed on cycle ergometers at the hospital’s cardiopulmonary rehabilitation centre. Training included a 10-minute warm-up (5 minutes unloaded and 5 minutes at progressively increasing load), an intensity phase at subjects’ respective target intensity and duration and 5-minute cool-down. The intensity phase for CTHI consisted of 25 minutes of pedalling at the HR reached at 80% of W peak on the incremental test. For CTVT, the target intensity was the HR reached at the ventilatory threshold, while IT consisted of 30-second intervals at the HR reached at 100% W peak interspersed with 30-second intervals of unloaded pedalling. Session duration for CTVT and IT was adjusted for each subject using metabolic equations 25 to equal total amount of work performed to 25 minutes of CTHI. Subjects were instructed to train within ±5 beats/minute of the target HR identified. Two trained exercise physiologists supervised sessions; instructions and feedback were standardized.
Acute response to exercise training
Acute response to training was measured during an entire bout in the beginning phase of the PR program (−1 to +2 weeks of start). Physiological measurements (
Affective measurements were completed at various time points. The PANAS was administered at rest, 100% of exercise time and 30 minutes post-exercise, whereas the GVA was completed at rest, 0%, 50% and 100% of exercise time, and 30 minutes post-exercise. The PANAS, developed by Watson, Clark and Tellegen, 10 is a brief and easy self-administered questionnaire. The final outcome is obtained in two separate scores: one for positive affect and the other for negative affect. More specifically, this questionnaire consists of 20 questions related to affect, 10 dealing with positive affect responses (interested, excited, strong, enthusiastic, proud, alert, inspired, determined, attentive and active), and 10 dealing with negative affect responses (distressed, upset, guilty, scared, hostile, irritable, ashamed, nervous, jittery and afraid). 10 Scores range from 10 to 50 for each affective response. Various time frames have been used for the PANAS 10 ; the chosen time frame for the present study was “in the present moment”. Its structure is consistent with the two-dimensional circumflex model and has been shown to have excellent reliability 28 and validity. 10 In addition, it has been shown to be highly internally consistent and largely uncorrelated. 10
The GVA is composed of eight visual analogue scales, four related to global affect and four related to global vigour. Each score is entered into an equation revealing a global affect and vigour score ranging from 0 to 100. Visual analogue scales have an extensive history in the measurement of mood 29,30 and have been shown to be highly reliable and valid in assessing both global affect and global vigour. 27,31 This scale is a simple and frequently used measure that has been included in several studies to assess a wide range of subjective phenomena such as dyspnoea, pain, fatigue and sleep loss among others. 27
Adherence to exercise training program
Adherence was defined as percentage of time spent within the target HR range throughout the 12-week program and was measured for attended sessions using continuous data tracking technology (Bike Excite Med 700, Technogym, Italy; T31 transmitter, Polar, Finland; CardioMemory, Technogym, Italy). A detailed description of this methodology has been published. 32 Since subjects undergoing IT were expected to spend 50% of their time in their target HR range (during high intervals), adherence to the target training intensity was obtained by multiplying time spent within the target HR range by two up to a maximum of 100%.
Statistical analyses
Baseline measurements were compared between groups using one-way analyses of variance (ANOVA). Acute physiological and symptomatic changes to exercise were analysed with a series of repeated-measures mixed models. To assess acute effects of exercise protocols on PANAS (positive and negative affect) and GVA (global affect and vigour) responses, four repeated-measures general linear models were conducted. Mean adherence to the target training intensity for the intervention protocols was compared using Levene’s test (see online supplement). Adherence data lost from technical difficulties were replaced by bringing the last value forward. Double data extraction was performed on adherence data. Change in exercise tolerance from baseline to week 12 was compared between groups with a repeated-measures ANOVA. To assess the intensity–adherence relationship, associations between a priori selected acute measures (W,
Results
Subjects
Baseline characteristics are presented in Table 1. Thirty-five subjects completed the acute bout. The sample was predominantly composed of female (60%), overweight (66%) participants with, on average, moderate airflow obstruction corresponding to GOLD stage II COPD. 36 No significant between-group differences were found in baseline characteristics.
Baseline characteristics of the study groups.a

CTHI: continuous training at high intensity; CTVT: continuous training at ventilatory threshold; IT: interval training; BMI: body mass index; FEV1: forced expiratory volume in 1 second; FVC: forced vital capacity; TLC: total lung capacity; FRC: functional residual capacity; RV: residual volume; DLCO: lung diffusion capacity for carbon monoxide.
aValues presented are mean ± SD.
Response to the symptom-limited incremental cycling test is presented in Table 2. Subjects had, as expected, reduced peak W, HR and
Responses to symptom-limited incremental cycling test for each group.a
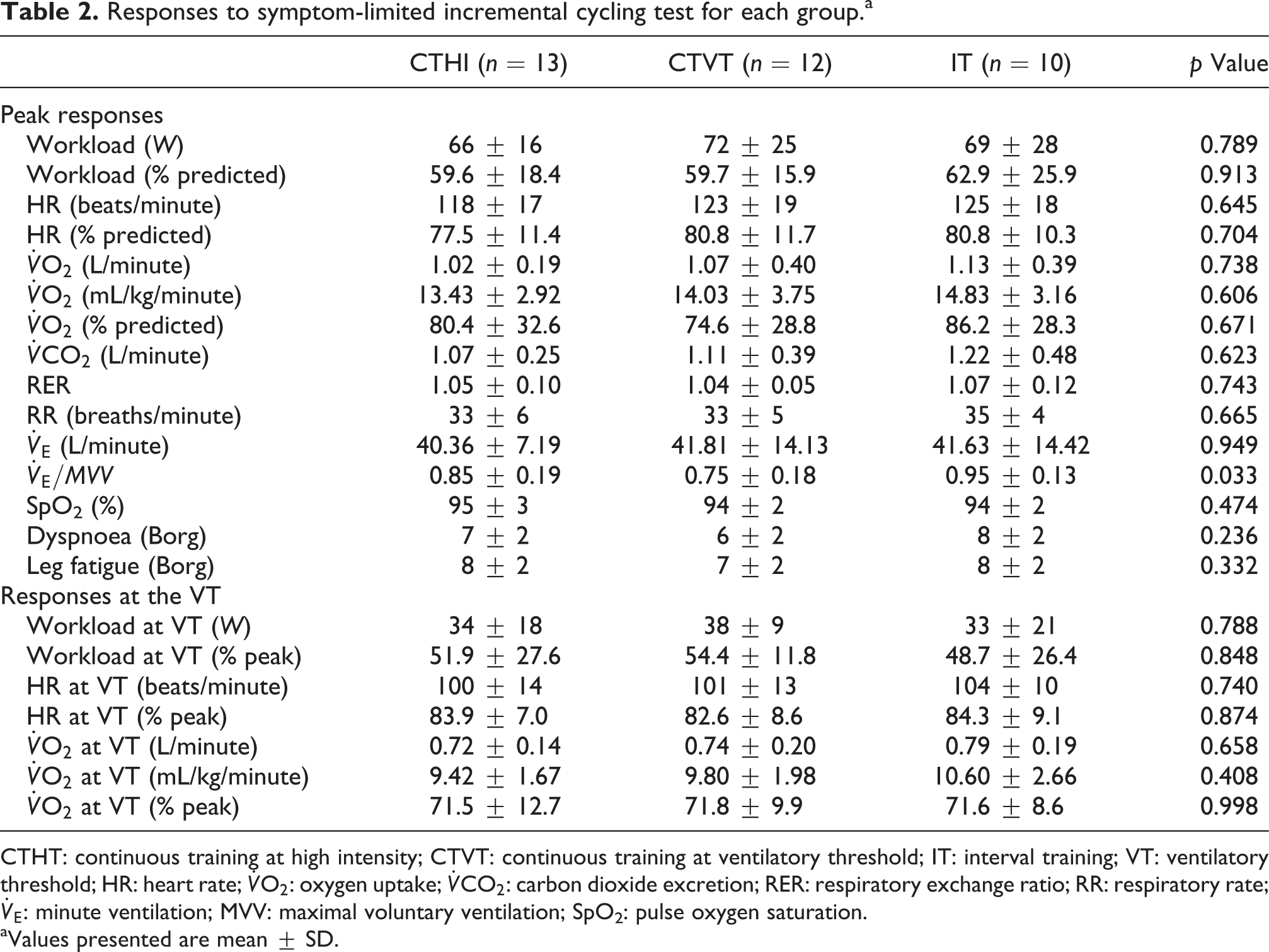
CTHT: continuous training at high intensity; CTVT: continuous training at ventilatory threshold; IT: interval training; VT: ventilatory threshold; HR: heart rate;
aValues presented are mean ± SD.
Acute responses to exercise training
Targeted exercise duration (excluding warm-up and cool-down) was 25.0 ± 0 minutes for CTHI, 30.7 ± 2.9 minutes for CTVT and 31.5 ± 1.2 minutes for IT. Everyone, except one subject from CTHI, was able to achieve the target exercise duration. Overall, subjects were able to attain and remain within their target HR range. Mean HR attained, expressed as a percentage of the target, was 99.9 ± 3.5% for CTHI, 99.8 ± 2.4% for CTVT and 89.6 ± 7.2% for IT (average of high and low interval). Mean HR attained, expressed as a percentage of the ventilatory threshold, was 109.3 ± 7.0% for CTHI, 100.8 ± 2.9% for CTVT and 108.0 ± 7.4% for IT.
The time course for absolute and relative physiological parameters for which significant between-group differences were observed is shown in Figures 1 and 2, respectively. For symptomatic responses, the only significant between-group difference observed was for perceived leg fatigue, expressed in absolute terms, which was significantly less in CTVT than CTHI and IT (F = 4.37, p = 0.01). PANAS results revealed a significant time effect from rest to post-exercise for positive (F = 9.74, p < 0.001) and negative (F = 6.43, p = 0.005) affect scores, but no time by intervention group interaction. GVA results indicated a significant time effect from rest to post-exercise for both global affect (F = 8.47, p < 0.001) and vigour (F = 9.79, p < 0.001). Additionally, a time by intervention group interaction was observed (see Figure 3).

Time course values for (a)
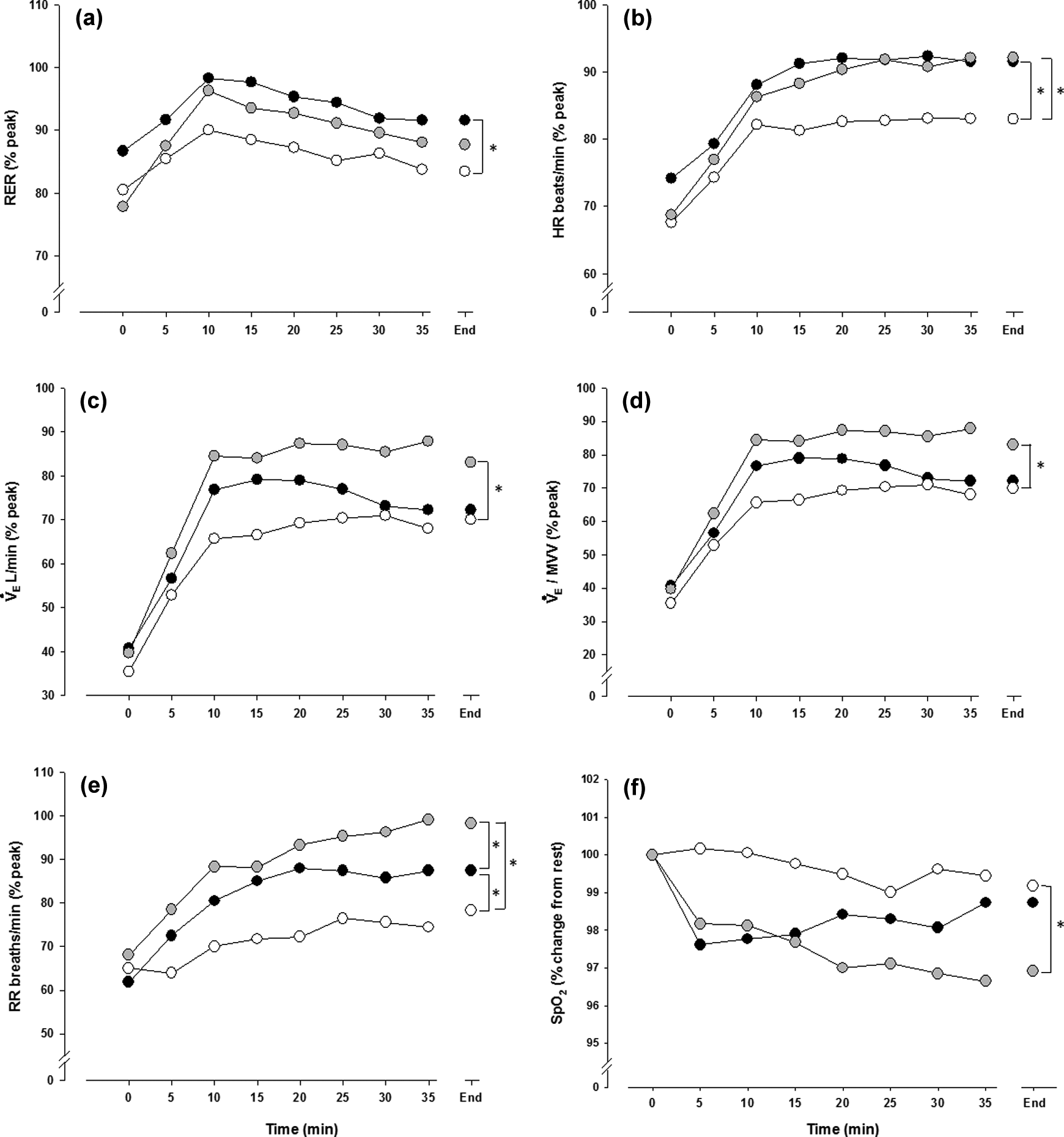
Time course values for (a) RER (% peak), (b) HR (% peak), (c)
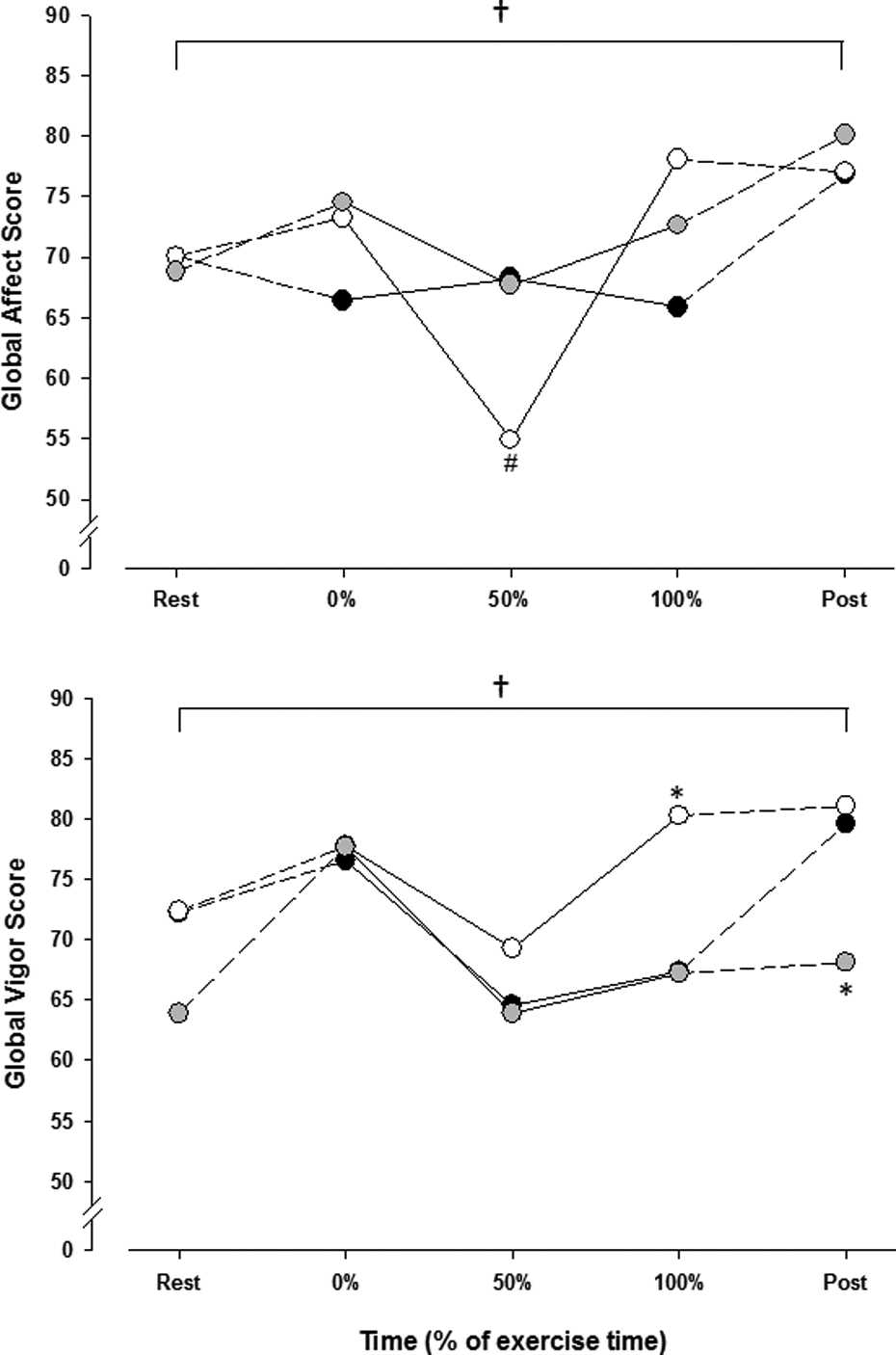
Global affect and global vigour, as measured by the GVA, for CTHI (black circles), CTVT (white circles) and IT (grey circles). †p < 0.001: significant difference; #p < 0.05: significant difference from CTHI. *p < 0.05: significant difference from other groups; GVA: global vigour and affect Instrument; CTHI: continuous training at high intensity; CTVT: continuous training at ventilatory threshold; IT: interval training.
Adherence and response to 12-week exercise training program
One subject from CTHI was excluded after completing the acute bout for medical reasons. Mean attendance was not significantly different between groups (CTHI: 70.1 ± 32.9% (range: 49.3–91.0); CTVT: 81.9 ± 17.2% (range: 71.0–92.9); IT: 73.3 ± 28.6% (range: 52.9–93.8), F = 0.61, p = 0.55). Mean 12-week adherence to the target training intensity was significantly lower in IT compared to CTHI and CTVT (CTHI: 85.6 ± 15.0% (range: 76.0–95.1); CTVT: 85.4 ± 15.8% (range: 75.3–95.5); IT: 49.0 ± 42.8% (range: 18.4–79.7), F = 6.69, p = 0.004). Adherence rates to the target training intensity were high and slightly negatively skewed. Standardization attempts failed to normalize adherence data; thus, original values were used.
At baseline, mean endurance cycling time, as measured by the constant-load cycling test, was 306.3 ± 131.8 seconds for CTHI, 300.9 ± 119.7 seconds for CTVT and 266.3 ± 109.6 seconds for IT. Post 12-week training, mean endurance cycling time was 615.5 ± 400.0 seconds for CTHI, 633.5 ± 445.8 seconds for CTVT and 629.1 ± 304.5 seconds for IT. Analyses revealed a significant time effect (F = 28.49, p < 0.001), yet no time by intervention group interaction.
Relationship between acute responses and adherence to target training intensity
After adjusting for percent attendance rate, mean achieved W (r = −0.429, p = 0.014),
The mediation model was not supported by our data. When moderation was tested with

(a) Conceptual moderation model and (b) statistical moderation model with
Discussion
Summary of main findings
The findings can be summarized as follows: (i) affect generally improved from rest to post-exercise; (ii) CTVT was less physiologically demanding than CTHI and IT, was associated with a more pronounced drop in global affect mid-exercise, but with less leg fatigue and better end-exercise vigour; (iii) IT was associated with a more pronounced ventilatory response than CTHI and CTVT, lower levels of post-exercise vigour and reduced 12-week adherence; (iv) pre-training mean
How and why it agrees or disagrees with the existing literature
Results on the acute physiological response to IT compared to CTHI differ from previous reports, showing reduced metabolic strain with IT compared to CTHI. 4,6 Inconsistencies between our results and those from Sabapathy and colleagues 4 are likely attributable to disparities in IT protocols. In our study, IT consisted of shorter intervals (30 seconds vs. 1 minute) of a higher relative intensity (100% vs. 70% W peak) alternated with active recovery (versus rest). These differences likely translated into less time for recovery with our IT protocol, thereby making it more physiologically demanding. As for Vogiatzis et al., 6 our findings possibly differed from theirs due to disparities in continuous training protocols. Their subjects were asked to maintain a W corresponding to 80% W peak 6 ; in the present study, subjects were asked to remain within ±5 beats/minute of the HR reached at 80% W peak on the incremental test, corresponding to approximately 60% W peak (data not shown). Thus, our CTHI protocol was less physiologically demanding than theirs. It seems reasonable to conclude that, depending on the protocols used, IT can be similarly, slightly more, or slightly less physiologically demanding than CTHI. Also, based on the present study, IT may be associated with lower levels of vigour or alertness post-exercise.
Comparing CTHI and CTVT, our results support Vallet et al.’s 5 findings suggesting that CTVT is more tolerable physiologically for COPD patients than continuous training at a standardized intensity. CTVT was also shown, for the first time in COPD, to be associated with higher levels of end-exercise alertness. This approach may thus be associated with better long-term adherence than CTHI and IT. CTVT was associated with lower leg fatigue ratings, but the difference disappeared when expressed in relative terms. Furthermore, CTVT was not associated with reduced dyspnoea, as previously reported by Vallet et al. 5 Ratings of perceived breathlessness have previously been suggested as unresponsive to increases in exercise performance 37 and declines in lung function over time. 38 The presence of a dyspnoea threshold in COPD has been proposed, which when surpassed may not be well tolerated. 37 Subjects may therefore consciously or unconsciously select a level of dyspnoea not to surpass. 37 Our findings may reflect this phenomenon.
Positive changes in affective state (increase in positive and/or global affect and decrease in negative affect) observed from rest to post-exercise across training protocols is consistent with previous findings in healthy populations, which show acute exercise-induced improvements in affect with varying training intensities. 9,13,17 However, our group results are not in line with the contention that affect improves or remains stable during exercise performed at the ventilatory threshold, and worsens when the intensity is above the ventilatory threshold. Indeed, CTVT, which exercised at 100% of the ventilatory threshold, experienced the greatest dip in affect mid-exercise, while CTHI and IT, which exercised above the ventilatory threshold (109% and 108%, respectively, data not shown), experienced less or no dip. Perhaps COPD patients, who face discomfort on a regular basis, react differently from healthy individuals to different intensities. Elevated rates of psychological and cognitive impairments have been documented in COPD. 39,40 These factors have been shown to variably alter the affective response to exercise; this may explain discrepancies between our findings and those in healthy individuals. 11,12
Adherence to the target training intensity was measured using continuous data tracking technology. Using this precise measure, subjects from the IT group were found to have spent a significantly lower percentage of time at the target intensity (49%) compared to CTHI (86%) and CTVT (85%); yet, the training effect appeared to be similar across groups. These findings, however, need to be interpreted with caution since this study was not powered to detect differences in adherence rates or training effects between protocols. Rather, it emphasized on the relationship between acute responses and subsequent adherence to different protocols to validate/invalidate previously proposed conceptual models from healthy populations. To that extent, our results suggest that acute measures of exercise intensity, more specifically
Strengths and limitations of this study
This study needs to be interpreted in the context of some limitations. Sample size was small, which may have affected our power, and groups were unequal in size. Furthermore, based on the general response to the incremental cycling test, it is likely that the test was symptom-limited, as opposed to maximal, in a number of subjects. This may have translated into an underestimated exercise prescription. Methodology used to ascertain target training intensity (via HR) may not be in line with previous literature, however, this approach was selected to reflect common practice in community-based rehabilitation programs.
In conclusion, CTHI, CTVT and IT improved affective valence from rest to post-exercise and induced a significant 12-week exercise training effect. However, they elicited different acute physiological responses, which in turn were associated with differences in 12-week adherence to the target training intensity. This association was moderated by acute end-exercise vigour.
Footnotes
Acknowledgements
The authors would like to acknowledge the Respirology Unit at l’Hôpital du Sacré-Coeur de Montréal. More specifically, we thank respirologists Dr François Beaucage and Dr Simon Parenteau, as well as Lucie Jolicoeur and Bernadette Tardivel for their invaluable help. We also thank Éric Nadreau for his assistance and expertise with the metabolic equipment and Jean Paquet for his help with certain elements of the statistical analyses. Finally, we thank the participants who made this study possible.
Conflict of interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: SLB has received honoraria from Kataka Medical Communications for consultancy for the development of behaviour change CME. KLL has received speaker or consultancy fees from Abbvie, Takeda, Merck-Frost and Boehringer Ingelheim. AKR, RW, EC-T and VP have no potential conflicts of interest with any companies or organizations whose products or services are discussed in this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the operating grants from the Fonds de recherche du Québec – Santé (FRQ-S; grant number 12505), and Canadian Lung Association – Canadian Respiratory Health Professionals (no assigned grant number).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.