
Abstract
In recent years, several studies have shown that whole body vibration training (WBVT) may be a beneficial training mode in a variety of chronic diseases and conditions such as osteoporosis, fibromyalgia, multiple sclerosis, or chronic low back pain. However, a systematic review on the effects of WBVT in patients with chronic obstructive pulmonary disease (COPD) has not been performed yet. An extensive literature search was performed using various electronic databases (PubMed, Embase, LILACS, and PEDro). They were searched from inception until September 20, 2014, using key words like “COPD” and “whole body vibration training.” A total of 91 studies could be identified and were screened for relevance by two independent reviewers. Six studies were included in a qualitative analysis. Trials studied either the effects of WBVT versus an inactive control group, versus sham WBVT, during an acute COPD exacerbation or as a modality on top of conventional endurance and strength training. All randomized trials reported a significantly superior benefit on exercise capacity (6-minute walking distance) in favor of the WBVT group. Although there are only few studies available, there is some preliminary evidence that WBVT may be an effective exercise modality to improve functional exercise capacity in patients with COPD.
Introduction
In 1881, JM Granville was the first to postulate therapeutic effects of treating pain by mechanical vibration. It was only in the 1980s that whole body vibration training (WBVT) was used as a training modality in athletes. However, scientific articles reporting on WBVT studies usually end with the phrase “further research is needed”, which still reflects the limited knowledge on WBVT. Furthermore, a large number of general WBVT studies suffer from methodological weaknesses and included only small sample sizes. 1 Also, heterogeneous study populations and a large variety of different WBVT protocols and approaches have led to inconclusive results of WBVT effects so far. 2
In general, WBVT is characterized by an external stimulation inducing an oscillation vibration to a subject standing on a vibrating platform. Nowadays numerous different WBVT devices are available, which use various mechanical principles of inducing WBV. Most platforms rely on one or both of the two most commonly used energy transfer systems (Figure 1) but also vary by technical quality. One type of devices transfers vibration to both feet synchronously (also known as vertical vibration), while the other one uses a side alternating mode similar to standing on a seesaw. Thus, these two techniques address two completely different neurophysiologic movement patterns. There is an ongoing debate regarding which approach might be more beneficial or superior. Thus, WBVT should not be seen as a unique term for one specific exercise modality.

Direction of vibration movement during vertical and side-alternating whole body vibration training. Source. Adapted from Rauch et al. 3
For a useful interpretation of a WBVT intervention, it is necessary to take a closer look at the WBVT parameters like frequency, peak-to-peak displacement, duration, exercises, and so on. In order to help improving the quality of study reports on WBV interventions, the International Society of Musculoskeletal and Neuronal Interactions has provided suggestions on how to describe WBVT interventions adequately. 3 Table 1 shows an overview on relevant items that should be addressed in WBVT studies.
Checklist of items that should be addressed in reports of a WBV treatment study.
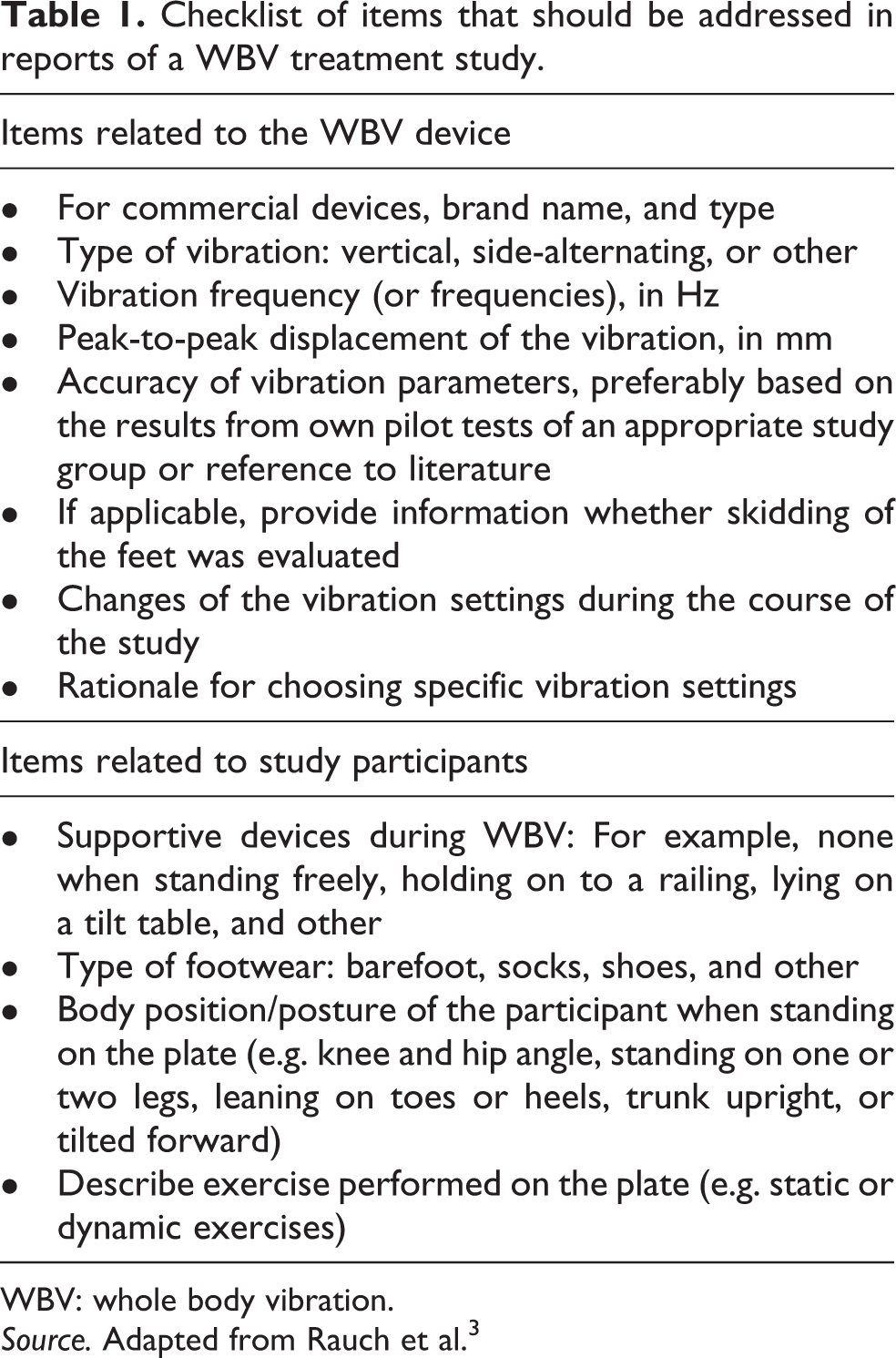
WBV: whole body vibration.
Source. Adapted from Rauch et al. 3
The general effects of WBVT
Effects of WBVT can be divided into acute and chronic effects. An activation of lower extremity blood circulation, 4 improvement of muscle performance and balance 5 as well as an increase in human growth hormone output 6 have been observed after just a single bout of WBVT. Chronic effects of WBVT have been reported in various physiological systems. A central mechanism of WBVT is elicited by the “tonic vibration reflex” that provokes muscle contractions especially in the lower extremities. 7 This reflex caused by mechanical vibration induces a higher rate of motor unit recruitment in skeletal muscles by stimulating muscle spindles and Golgi cells. It is supposed that the most important structural benefits of WBVT are of neurophysiological origin. 8 Other possible mechanisms of WBVT benefits include enhanced postural control and improved intermuscular coordination like the complex interplay of agonists and antagonists. 9 WBVT has also been shown to be an effective training modality to counteract immobility-related muscle atrophy and loss of bone density. 10
In recent years, several studies have reported inconclusive results of WBVT. However, many reviews have concluded that WBVT may be a beneficial training mode in a large variety of chronic diseases and conditions such as osteoporosis, fibromyalgia, cystic fibrosis, multiple sclerosis, type 2 diabetes, pelvic floor weakness, and chronic low back pain.
The rationale for WBVT in patients with COPD
Within the past decades, endurance and strength training have been established as the major components of exercise training programs in patients with chronic obstructive pulmonary disease (COPD). 11 Nevertheless, there is still an unmet need regarding the evaluation of further and complementary exercise modalities to encounter the extrapulmonary manifestations of COPD on various levels. The rationale for applying WBVT in patients with COPD is almost self-evident when considering the general indications for the use of WBVT such as improving muscle power, balance, and bone density. 12 All these aspects are highly relevant in COPD patients. Therefore, WBVT might be considered a worthwhile attempt to be included in exercise training programs for subjects with COPD. However, a review on WBVT in patients with COPD has not been performed yet. Therefore, aim of this systematic review was to identify and analyze all available studies that investigated exercise training on WBV platforms in patients with COPD. Outcome parameters of interest were 6-minute walking distance (6MWD), sit-to-stand tests, peak knee extension force, and quality of life.
Methods
Data sources and search strategy
An extensive literature search was performed on September 20, 2014 and updated on February 20, 2015. Electronic databases (PubMed (MEDLINE), Embase, LILACS, and PEDro) were searched from inception until now. Search terms were based on a combination of the following key words: “COPD” OR “chronic obstructive pulmonary disease” OR “chronic bronchitis” OR “emphysema” and “whole body vibration training” OR “whole body vibration” OR “vibration training” OR “vibration”. In addition, we performed a manual search of references in published studies on the subject. This systematic review was performed in compliance with the preferred reporting items for systematic reviews according to the PRISMA guidelines. 13
Inclusion and exclusion criteria
Articles were included if they (i) were full papers published as original articles and (ii) were written in English. Articles were excluded when they studied any kind of chest wall vibration for the purpose of mucus clearance. Book chapters, letters to the editor, unpublished work, and study protocols were also excluded from this review.
Selection of studies
Two members of the review team (RG and IH) independently screened title and abstract of each study identified from the search. All potentially relevant articles were then retrieved in full-text form for a secondary screen. Agreements on inclusion were decided unanimously. A list of excluded studies and reasons for their exclusion is maintained in Figure 2.
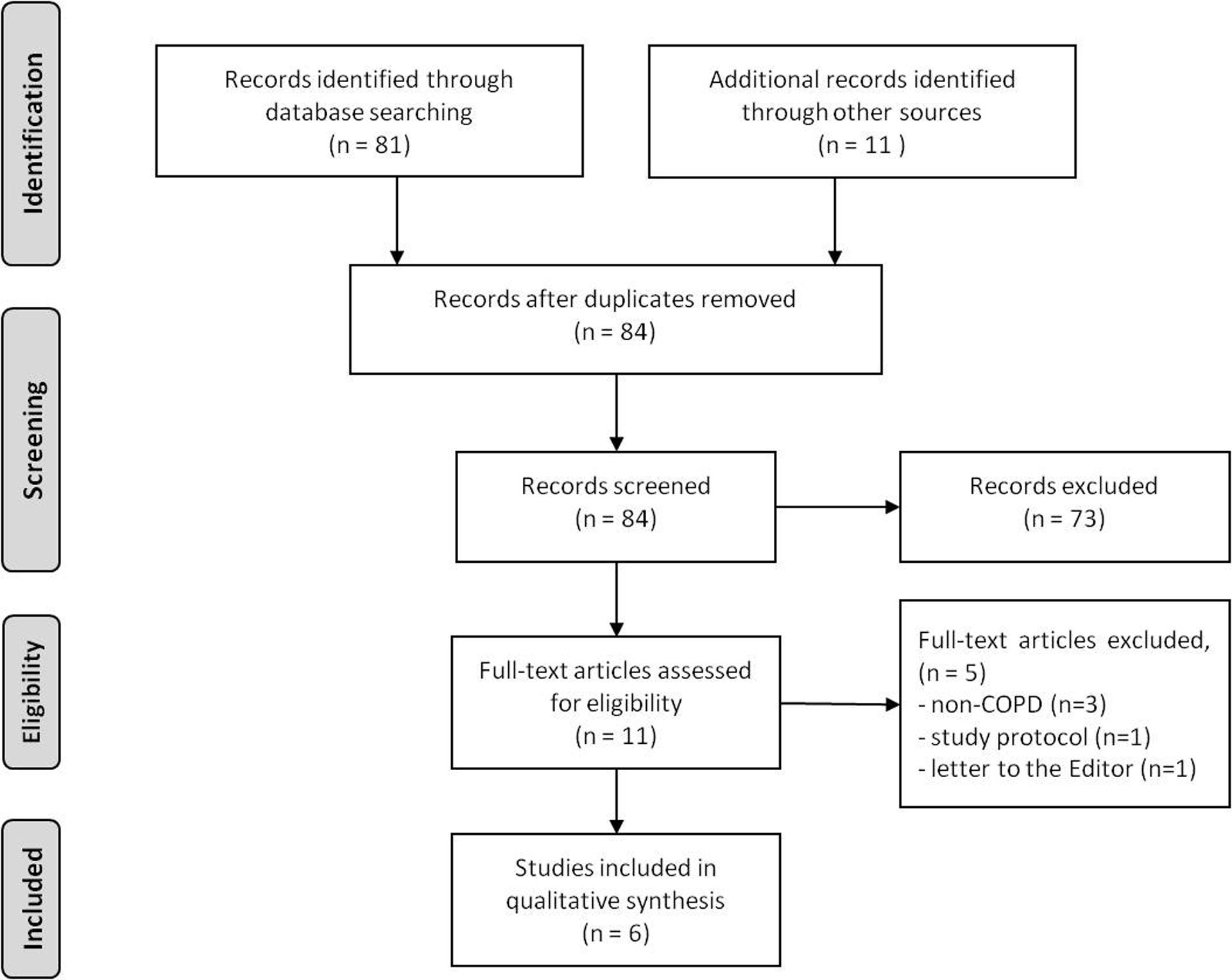
PRISMA flow chart.
Data extraction and quality assessment
Data were extracted using a standardized form by one member of the review team (RG) and double-checked by another team member (IH) to ensure accuracy. Data included study method and design, sample size, withdrawal rate, patient characteristics, WBVT settings, intervention-related adverse events, WBVT training regime, and major results.
The methodological quality of each study was rated individually by two reviewers (RG and IH) using Grading of Recommendations Assessment, Development and Evaluation (GRADE) guidelines 14 (see Table 2). Disagreement on the quality rating was resolved by achieving a consensus.
Characteristics of studies that investigated WBVT in patients with COPD.

1RM: one repetition maximum; 5-SST: 5-repetition-sit-to-stand test; 6MWD: 6-minute walking distance; AECOPD: acute exacerbation of the chronic obstructive pulmonary disease; CON: control; COPD: chronic obstructive pulmonary disease; CAT: COPD Assessment Test; CRDQ: Chronic Respiratory Disease Questionnaire; DLCO: lung diffusion capacity; FEV1: forced expiratory volume in 1 second; IL-8: interleukin 8; LTOT: long-term oxygen therapy; n.a.: not available; PR: pulmonary rehabilitation; SGRQ: St George Respiratory Questionnaire; QF: quadriceps force; RCT: randomized controlled trial; RT: resistance training; SWBVT: sham whole body vibration training; TUG: timed up and go test; W: % withdrawal; WBV: whole body vibration; WBVT: whole body vibration training; SpO2: oxygen saturation.
a p < 0.05; b p < 0.001.
Data analysis
Since the included studies were very heterogeneous with regard to their methodology and objective, it was not possible to perform a meta-analysis. Therefore, a qualitative analysis of the different studies was performed (Table 2).
Results
Study selection
The study selection process is outlined in Figure 2. A total of 92 titles were screened, resulting in the retrieval of 11 full-text articles for review. Five studies were excluded with reasons, and the remaining six articles were included in the review (for study details see Table 2).
Quality assessment
The quality of the included studies, using the GRADE recommendations, is presented in Table 2. All included studies had an appropriate research design and used objective measures. In all studies, blinding patients or therapists who performed the exercise intervention was not possible. Four studies were performed as randomized controlled trials using an adequate quality of methodology. 15,17,19,20 Two studies performed by the same work group used a nonrandomized study design with crossover to sham 16,19 that yielded lower methodological quality ratings.
All studies provided methodological information closely related to the guidelines on reporting WBVT intervention studies. 3 However, only one study 15 reported on the rationale for choosing a specific vibration frequency.
Study characteristics
Acute response during WBVT
An Australian study by Furness et al. 16 investigated the acute effects of WBVT by profiling subjective and objective responses. Seventeen patients with moderate COPD (forced expiratory volume in 1 second (FEV1): 52 ± 18% predicted (pred.)) performed two sessions, WBVT and sham WBVT (SWBVT). Each session consisted of 5 × 1-minute bouts of standing on a side-alternating vibration platform (Amazing Super Heatlh, Melbourne, Australia) with a 20° knee flexion at 2 mm peak-to-peak displacement (WBVT) or 0 mm peak-to-peak displacement (SWBVT). Participants were told that the SWBVT intervention was an “ultralow frequency” vibration intervention that is “very different” to the WBVT intervention. Oxygen saturation reduced by 1% during WBVT and did not change during SWBVT. Changes in perceived dyspnea remained stable from “very slight” to “slight” among WBVT and SWBVT. Acute changes in subjective and objective responses during WBVT were clinically meaningless. It was concluded that short bouts of standing on a vibration platform might be seen as a mode of dyspnea-free exercise modality in people with COPD.
WBVT versus control
A randomized controlled trial (RCT) by Pleguezuelos et al. 17 investigated the effects of WBVT with regard to changes in muscular force and functional capacity parameters in patients with COPD. Sixty stable male patients with COPD (FEV1: 35 ± 10% pred.) were randomized to a WBVT group or a control group without any intervention. Patients in the WBVT exercised on a vertical vibration platform (Fitvybe®, Gymnauni, Belgium) for 3 sessions/ week and a total duration of 6 weeks. The training was designed to perform static squatting position at a frequency of 35 Hz and 6 series of 4 × 30-seconds duration at each session. After 6 weeks, patients in the WBVT group showed a highly significant and clinically relevant improvement in 6MWD of 81 ± 9 m (p < 0.001), whereas patients in the control group remained at baseline 6MWD. Nevertheless, the primary outcome parameter of isokinetic knee flexor and extensor force did not change significantly in any group.
Braz Junior et al. 20 performed a similar approach using a randomized controlled crossover design in a small group of 11 patients with COPD (FEV1: 15 ± 11% pred.). Patients underwent a 12-week WBVT program (three supervised sessions/week) on a vertical platform (Powerplate, London, UK). Subjects stood in a static semi-squatting position at a knee angle of 120°–130°. Training was applied using short bouts of 30–60 seconds of WBVT for 10–20 minutes at 35 Hz. Patients in the control group did not receive any intervention. At 12 weeks, patients in the WBVT group were able to increase 6MWD significantly by 64 m, whereas the control group walked 15 m less compared to the baseline. Also quality of life (measured by St George Respiratory Questionnaire) improved significantly only in the WBVT group.
Furness et al. performed an efficacy trial using a non-randomized, crossover design to sham. 18 Sixteen COPD patients (FEV1: 59 ± 19% pred.) performed home-based, supervised WBVT sessions on a side-alternating platform (Amazing Super Health) twice a week for 6 weeks. Patients stood on the vibration platform with the knees flexed to 53 ± 19° at a frequency of 25 Hz and a 2-mm peak-to-peak displacement (duration per session not reported). At 6 weeks, it was found that functional performance had significantly (p < 0.05) improved (timed up and go test: from 11.3 ± 1.9 seconds to 9.8 ± 1.9 seconds, 5-repetition sit-to-stand test: from 18.5 ± 3.4 seconds to 15.1 ± 2.4 seconds). It was also reported that various kinematic variables of gait-like stride length, stride time, and stride velocity had significantly improved. After a 2-week washout phase, patients performed another 6 weeks of SWBVT also using 25 Hz but 0 mm peak-to-peak displacement. Functional performance did not further change within this period.
WBVT versus training on the floor
Another RCT by Gloeckl et al. 15 studied the effects of WBVT as an additional exercise modality on top of a multidisciplinary short-term pulmonary rehabilitation (PR) program. Eighty-two patients with severe COPD (FEV1: 38 ± 11% pred.) enrolled in a 3-week inpatient PR program performed conventional endurance and strength training on 5 days/week for about 60 minutes/day. Additionally, patients were randomly assigned to one of two intervention groups: (1) 3 × 3-minutes of bilateral dynamic squatting exercises on a side-alternating vibration platform (Galileo®, Novotec Medical, Germany) at a high intensity (24–26 Hz) three times per week or (2) a control group performing the same amount of squatting exercises on the floor without WBV. The increase in 6MWD was significantly higher in the WBVT group compared with the control group (64 m versus 37 m; p < 0.05). The time required for a functional exercise performance test (5-repetition sit-to-stand test) also improved to a clinically 21 relevant extent in patients performing WBVT (−4.0 ± 4.8 seconds versus −2.0 ± 3.1 seconds; p = 0.067). The benefits on health-related quality of life (HRQL; measured by the Chronic Respiratory Questionnaire) were comparable within both groups. It was concluded that WBVT seems to be an effective and feasible exercise modality for patients with advanced COPD that may enhance the effects of a comprehensive PR program.
WBVT during AECOPD
Another RCT by Greulich et al. 19 investigated the use of WBVT in COPD patients during hospitalization due to an acute exacerbation of COPD (AECOPD). Beyond a similar medical treatment, 40 COPD patients (FEV1: 36 ± 16% pred.) were randomly assigned to one of two different interventions. Both groups received 30 minutes of daily chest physiotherapy focusing on breathing exercises to improve mucus clearance. A WBVT group additionally exercised on a side-alternating vibration platform (Galileo, Novotec Medical, Germany) at a high frequency (26 Hz) for 3 × 2 minutes daily. Although patients stayed in hospital for 1 week only, authors of this study reported very large and remarkable effects for patients in the WBVT group. Patients in the control group showed worsened exercise capacity and HRQL at discharge, whereas patients in the WBVT group significantly improved in these outcomes (6MWD: −5 m versus +96 m; p < 0.01; COPD Assessment Test: CON group: 24 ± 9 points to 23 ± 7; p = not significant and WBVT group: 29 ± 6 to 25 ± 6; p = 0.02). Another important finding of this trial was that the decrease in interleukin 8 was significantly more pronounced in the WBVT group (p = 0.04).
Discussion
This systematic review provides an overview on all currently published studies on WBVT in patients with COPD. The six included studies focused on very different aspects of WBVT.
One study that investigated the acute effects of a single bout of WBVT 16 only included patients with moderate COPD. It remains unknown to what extent oxygen saturation or other parameters may be influenced during WBVT in patients with a more severe disease that become hypoxemic during exercise. This important safety issue has to be investigated in future trials. Also potential differences in cardiorespiratory response between static and dynamic squatting position should be studied.
One WBVT study 17 measured quadriceps force. No difference could be found following a 6-week WBVT intervention. The use of an isokinetic measurement procedure of determining muscular force in this study might have been an inadequate approach since exercise training was performed in an isometric fashion. This might have underestimated a potential change in muscle force. However, this study clearly showed a meaningful benefit of WBVT in COPD patients on 6MWD and this may support the hypothesis that a large proportion of WBVT effects may be referred to neuromuscular adaptations rather than to muscle hypertrophy (especially when training is performed without additional load). 8,22
Also the study by Gloeckl et al. supports this hypothesis since WBVT was even able to additionally increase exercise capacity on top of endurance and strength training which themselves yield a very strong benefit on exercise capacity. It was speculated that these effects were related to an increase in neuromuscular activation as well as in intra- and intermuscular coordination.
The study by Greulich et al. provided another important aspect that well dosed and controlled exercise during an acute exacerbation can be a beneficial and an effective additional therapeutic option 23 to counteract the devastating deconditioning of patients during this phase.
WBVT in the clinical practice in COPD patients
No conclusive WBVT protocol for its use in patients with COPD emerged throughout the reviewed literature. Available studies used different vibration devices (vertical or side-alternating), different vibration frequencies, and peak-to-peak displacements as well as various types of exercises. Therefore, it is not yet possible to derive the most efficient parameters for WBVT in COPD patients yet. However, according to the functional principle of WBV devices, an exercise frequency of >20 Hz for side-alternating and <35 Hz for vertical platforms should be aimed in order to improve muscle strength and function. These frequencies have been shown to increase neuromuscular activation of lower limb muscles the most. 24 Several sets of 30–180 seconds of WBVT duration seemed to be appropriate depending on the specific training target. The most commonly used exercise for WBVT in patients with COPD was the squatting exercise either in a dynamic or in a static fashion (Figure 3). It has not been investigated yet if one squatting modality is superior to another. It might be speculated that a combination of both static and dynamic exercises may be most beneficial to improve leg muscle function. However, a recently published study showed that a combination of (i) high vibration frequencies, (ii) the use of additional training load, and (iii) the mechanical principal of a side-alternating vibration platform induced the highest electromyographic activities of knee extensors. 25 Regarding the body position used, a knee flexion of 60° and forefoot stance appeared to be most effective for activating knee extensors and plantar flexors. 25 Some WBVT devices also offer vibrating handle bars or straps that are fixed to the platform and enable isometric exercises for the upper extremities. Whether these applications of vibration training for the upper body are useful or effective in patients with COPD has still to be investigated.

A patient with severe COPD during squatting position on a WBV platform (the patient gave written consent for the use of this photograph). COPD: chronic obstructive pulmonary disease; WBV: whole body vibration.
However, it is known that larger benefits of an exercise program can be reached if training contents are varied in order to prevent a certain ceiling effect of training effects. Therefore, it might be useful to vary vibration parameters, exercises, and the use of additional load in WBVT programs that last for a longer period.
In patients with COPD, WBVT might be used in all stages of disease severity. Patients with mild COPD and well-preserved functional status as well as patients with end-stage COPD and considerably reduced exercise capacity may successfully use WBVT. However, clinical practice shows that there is a minority of COPD patients who does not feel comfortable being exposed to WBV and therefore refuses WBVT.
Since mechanical vibration techniques have also been shown to increase sputum expectoration, it might also be conceivable that certain positions on a WBV platform transferring vibrations to the thoracic structures may improve mucus clearance. However, also this approach has not been investigated yet.
Beyond increasing functional capacity, WBVT can also be applied for other purposes. COPD patients often suffer from an increased risk for falls or comorbidities like, for example, sarcopenia or osteoporosis. WBVT may be a beneficial exercise strategy to counteract and improve these issues. Furthermore, WBVT frequencies used for joint mobilization and muscle relaxation could be applied to improve flexibility of the patient’s musculoskeletal system and the mobility of the spine and rib cage.
Study limitations
This systematic review has some limitations that need to be considered. The literature search was performed in four electric databases (PubMed, Embase, LILACS, and PEDro), and thus other articles may have been missed. Nevertheless, as the search strategy was thorough and further complemented with the review of reference lists from articles included, it is believed that this review contains all currently relevant studies on the topic. In addition, the inclusion of articles solely written in English may eliminate results from non-English publications. Also a potential risk of publication bias cannot be excluded since studies with inconclusive or even negative findings on WBVT might not have been published.
Conclusion
Although WBVT is not a new approach in medical exercise therapy, there is only a scarce number of studies currently available that have investigated WBVT in patients with COPD. Up to now, a meta-analysis and reliable comparison of these studies is not possible due to inhomogeneous study protocols and settings (study period, WBV device, WBV parameters, exercises performed on the WBV platform, disease severity, etc.). Nevertheless, there seems to be some preliminary evidence that WBVT may be an effective and promising additional exercise method beyond traditional training regimes in patients with COPD. With regard to the different pathways of inducing muscle contractions during WBVT (involuntary reflex) in comparison with traditional training (voluntary muscle contraction), WBVT could evolve as a worthwhile complementary approach to enhance training effects in patients with COPD.
Footnotes
Conflict of interest
The authors declared no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.