
Abstract
Pulmonary rehabilitation (PR) is recommended for people with interstitial lung disease (ILD); however, the educational content of PR was not designed for this group. This study explored the perspectives of patients and ILD clinicians regarding the educational content of PR for ILD. A qualitative study using individual semi-structured interviews was undertaken. Transcripts were coded independently by two investigators and themes established by consensus. Participants were 18 people with ILD (9 idiopathic pulmonary fibrosis, diffusing capacity for carbon monoxide 54 (20)% predicted) and 14 clinicians from 5 countries and 5 disciplines. Major themes from patient interviews were the importance of knowing what the future might bring and the need for honesty from clinicians. Most were happy to attend standard PR education sessions but wanted ILD-specific content. Patients wanted information about end-of-life planning and most were happy to discuss it in a group. Among clinicians, there was no consensus regarding whether prognosis should be discussed in PR. Most clinicians supported discussion of advanced care planning, however, some thought it should not be discussed in a group. We conclude that people with ILD have specific educational needs that may not be met in the current PR format. Patients and clinicians have some discordant views about programme content.
Introduction
The interstitial lung diseases (ILDs) are a highly disabling group of pulmonary disorders that include idiopathic pulmonary fibrosis (IPF), ILDs of known cause such as pneumoconiosis and drug-related ILD and ILD associated with connective tissue disease, such as rheumatoid arthritis and systemic sclerosis. The ILDs are characterized by exercise limitation, distressing dyspnoea, reduced ability to undertake daily activities and poor quality of life. 1,2 Treatment options are limited, and for some ILDs, life expectancy is markedly reduced. 3
Pulmonary rehabilitation (PR) is a cornerstone intervention to increase exercise tolerance and reduce symptoms in patients with chronic lung disease. 4 Most of the evidence supporting the efficacy of PR comes from studies involving people with chronic obstructive pulmonary disease (COPD); 5 however, growing evidence supports its use in ILD. 6 Two randomized controlled trials reported that PR had positive effects on dyspnoea, functional exercise capacity and quality of life. 7,8 Guidelines for ILD management now recommend that PR should be offered to the majority of patients. 3
PR includes exercise training, education and behaviour change. 4 The educational content of PR was originally designed for patients with COPD and includes topics that may not be relevant to those with other pulmonary conditions. 9 In patients with ILD, the physiological basis of exercise limitation, symptoms, treatment, disease progression and outcomes differ substantially from COPD. 2 It has been suggested that educational programmes for people with ILD should cover oxygen therapy, exacerbation management, energy conservation, symptom management, mood disorders, medications, lung transplantation and end-of-life care. 10 It is not known whether these topics fulfil the educational needs of people with ILD.
The aim of this study was to explore the perspectives of patients and clinicians regarding the topics that should be included in the educational component of PR for patients with ILD.
Methods
A qualitative study using semi-structured interviews and thematic analysis was undertaken, informed by the principles of grounded theory. 11 The study was approved by the Human Research Ethics Committees of Alfred Health and La Trobe University.
Interviews were undertaken with two groups of participants, namely, people with ILD and clinicians who care for people with ILD. A purposive sample was recruited to ensure the participation of a range of clinicians and patients that reflect the breath of potential experiences in those groups. Other strategies used to enhance rigour included use of field notes to demonstrate decision-making, researcher–participant corroboration, researcher triangulation, multiple coding and negative case analysis. 12 Informed consent was obtained from all participants.
Adults diagnosed with ILD were recruited from a tertiary hospital with a specialist ILD clinic. Participants with both IPF and non-IPF ILDs were recruited, as these groups may differ according to prognosis and disease experience. Purposive sampling was used to ensure inclusion of participants of both genders, with varying diagnoses and disease severity, both with and without previous experience in PR. ILD clinicians were identified via two sources, namely, Australian clinicians were identified via the Australian IPF network and international expert clinicians were identified in the peer-reviewed literature on PR and/or ILD. Purposive sampling was used to ensure inclusion of clinician participants from a range of disciplines (nursing, physiotherapy, exercise physiology, respiratory therapy and medicine) and a range of geographic locations. An email inviting participation was sent by the chief investigator. Demographic information about the participating clinicians was collected during the interview, including years of experience in ILD care and/or PR.
Individual semi-structured interviews were conducted using an interview schedule designed by the study authors (Table 1). Questions covered topics related to the educational needs of people with ILD and drew from a previous evaluation of information needs in PR for people with COPD 13 as well as suggested education topics for ILD in an expert review. 10 Interviews were digitally recorded. Descriptive and reflective field notes were taken by the interviewer. Investigator triangulation was employed with interviews conducted by one of two researchers (JF or AH). The recorded interviews were transcribed verbatim by a research assistant. All transcripts were de-identified.
Interview questions.
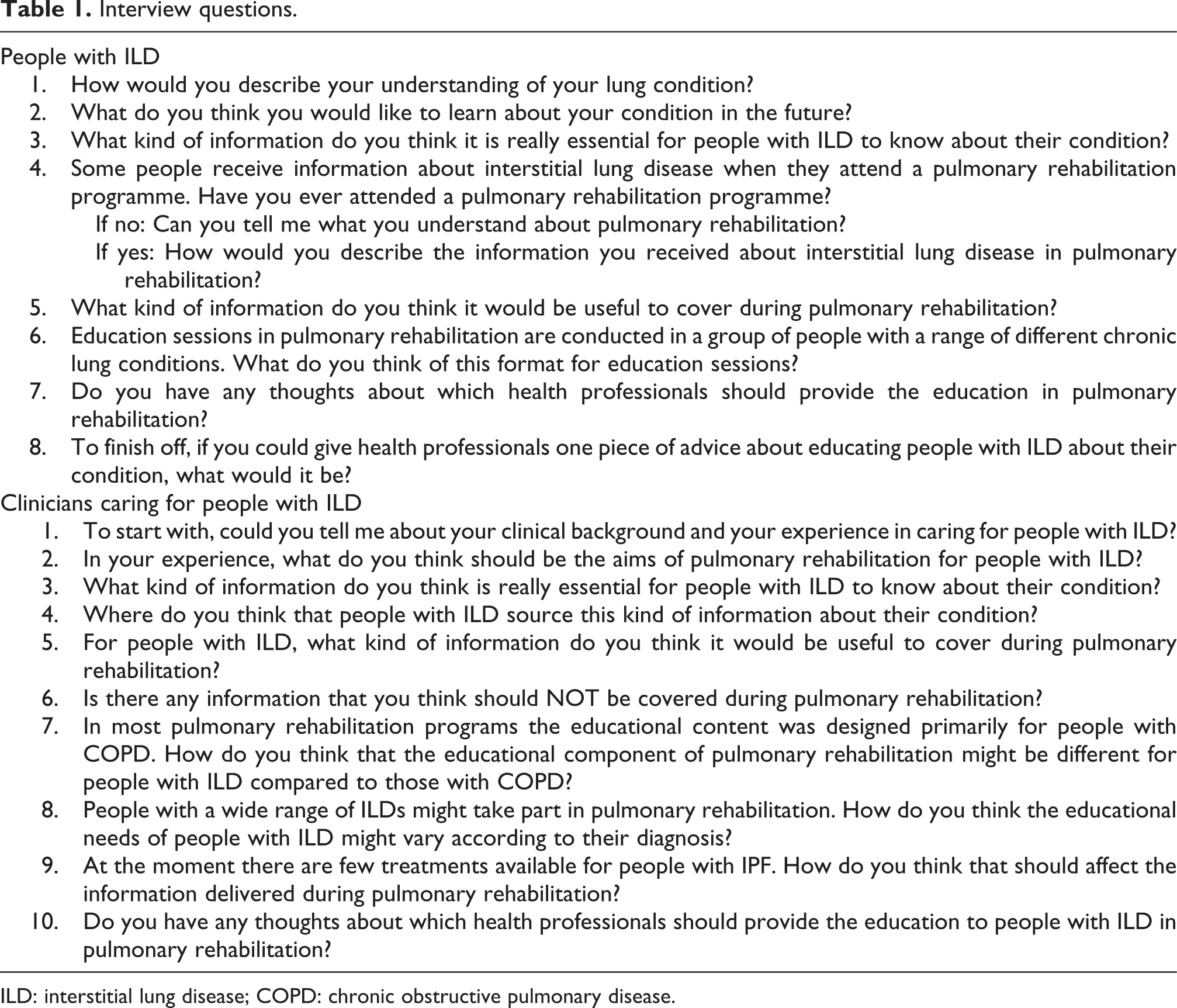
ILD: interstitial lung disease; COPD: chronic obstructive pulmonary disease.
The interview transcripts were independently examined by two investigators (AH and JF). The transcripts were first read line-by-line and fragmented into descriptive codes to represent the data (open coding). 14 Codes were then organized hierarchically to form themes and the original transcripts were searched to refine the relationship between themes and codes (axial coding). The final themes were agreed through iterative discussion between the two investigators. Quotations were extracted from the transcripts to provide supportive data for each theme. Data analysis commenced during the period when interviews were being conducted, so that the preliminary analysis could inform the ongoing interview process. Data collection continued until saturation was achieved in each group. 15 The final themes were compared between IPF and non-IPF participants as well as between clinicians and individuals with ILD.
Results
Participants with ILD
Eighteen people with ILD took part (nine with IPF). Their demographic characteristics are presented in Table 2. Participants had a wide range of disease severity (diffusing capacity for carbon monoxide range 28–94% predicted) and functional capacity (6-min walk distance range 270–663 m). Nine participants had previously undertaken a PR programme. Three major themes were identified from the interviews (Table 3).
Characteristics of participants with ILD.
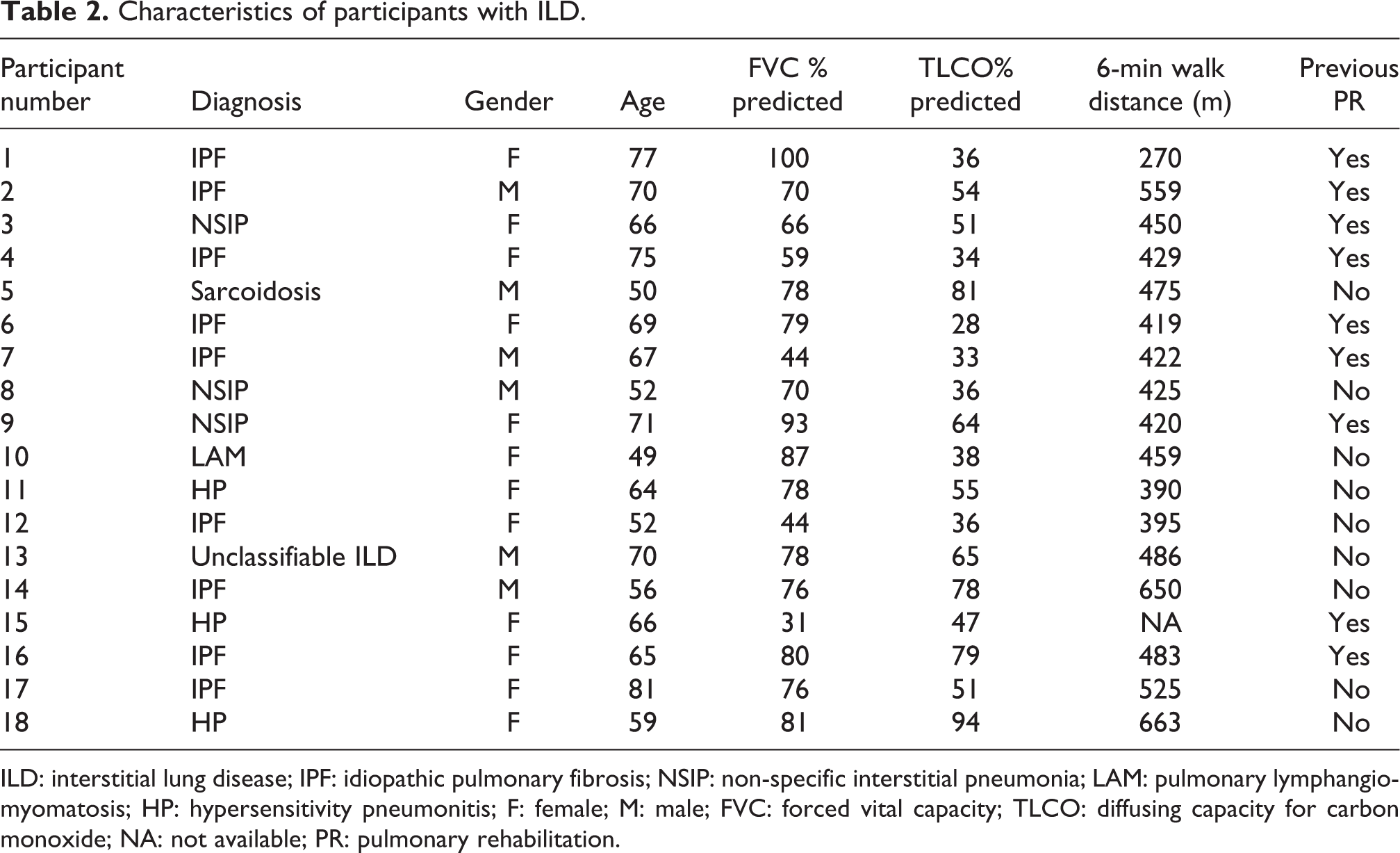
ILD: interstitial lung disease; IPF: idiopathic pulmonary fibrosis; NSIP: non-specific interstitial pneumonia; LAM: pulmonary lymphangiomyomatosis; HP: hypersensitivity pneumonitis; F: female; M: male; FVC: forced vital capacity; TLCO: diffusing capacity for carbon monoxide; NA: not available; PR: pulmonary rehabilitation.
Interview themes.

PR: pulmonary rehabilitation; ILD: interstitial lung disease.
Tell me about the future
Most participants with IPF understood their condition to be progressive and eventually fatal. In contrast, participants with non-IPF ILDs expected a variable clinical course. It’s a progressive lung disease and there is no known treatment except it slowly gets worse. (P4, IPF) …the progression of the disease is sort of an unknown thing and it may not get any worse. (P9, non-IPF)
The strongest theme across the participant interviews was the desire for PR clinicians to be honest about their future. Regardless of underlying diagnosis, the vast majority of participants expressed a need for clinicians to listen to their concerns, provide information about what they should expect over the natural course of the disease and be honest about their prognosis. Oh, just to listen to the patient and their concerns about the future. (P4, IPF) In my situation I would like to know if it was terminal. (P11, non-IPF) Well I haven’t got a very long future so ah, I suppose I’d like a bit of honesty from them…I’ve been sort of kept in the dark a little. (P1, IPF)
The overwhelming majority of participants were also interested in hearing information on planning for the end of life during PR. One other thing I am interested in is when you reach the end stage and you’re struggling to breathe and all these things, what can be done about it to reduce my anxiety level? No one has talked to me about that. (P7, IPF)
Almost all participants were happy to hear information about end-of-life planning in a group and for many this was their preferred setting. …they’re small groups and everybody’s anxious, everybody has the same issues so I think it (a group setting) is a good place to have it. (P9, non-IPF)
The exception was a very small number of participants who preferred to receive such information in private; none of these participants had previously undertaken PR.
Seeking information from multiple sources
Whilst participants described their specialist respiratory doctor as their primary source of disease information, almost all had also looked for information on the Internet. The majority had used the Internet to confirm information received at their medical appointments. A smaller number reported that the information on the Internet could be confusing and it was difficult to know what to trust. Others reported that they used the Internet primarily to make contact with others who had a similar disease. It (the internet) was helpful but I already know the information because the doctors at the hospital already told me. (P3, non-IPF) It’s good to touch base with other women who have the disease and you feel like family I guess. (P10, non-IPF)
Most participants were happy to receive information about their lung condition from any suitably qualified health professional, with a small minority preferring to speak only with a physician. I would be comfortable (receiving information) as long as you were experienced in the job. (P3, non-IPF) I’d prefer to speak to the specialist I guess. They’re the ones that have all the answers. (P5, non-IPF)
Education in PR
Participants who had previously undertaken PR recalled the value of the education programme. Several participants reported receiving information about COPD, some of which was not directly applicable to their condition. Some of it (the education) was really good, some of it was common to all of us, but there wasn’t anything that was specific to interstitial lung disease. (P9, non-IPF)
A few participants felt that education topics such as transplantation and oxygen therapy were not relevant for them, either because they were too early or too late in their disease stage.
Most participants favoured PR programmes that included people with a variety of lung conditions, recognizing the opportunities for learning that could occur regardless of underlying diagnosis. However, most also felt that ILD-specific education should be provided. …If it’s a respiratory disease, it’s a respiratory disease. And to me they’re all one and the same.…you can learn from one another as to how it impacts you and sometimes someone develops strategies to handle things. (P17, IPF) That’s up to the facilitator really to make sure, he should know what people sitting there have got…so they could tailor the talk. (P9, non-IPF)
Specific topics that participants identified as particularly relevant to ILD were managing cough, how to manage medications and their side effects and strategies to limit disease progression. What I still need to find out is how to manage that cough, so that it’s not something that embarrasses me and other people when I’m in public…there might be strategies that you can use to control it. (P17, IPF) I’m not on a lot but I am on warfarin for instance. And that’s a very complex thing, that wasn’t covered…. I’d like to have known more about that. (P9, non-IPF) I want to know what should I do to prevent it from getting worse and what is the good exercise for this situation. (P12, IPF)
A smaller number of participants favoured an education group that only included people with ILD. There was no relationship between previous participation in PR and preference for disease-specific education groups.
Apart from differences in their expectations of disease trajectory, there were no differences in themes emerging from IPF and non-IPF interviews. There were no differences in themes from participants with more severe compared to less severe disease.
Clinician participants
Fourteen clinicians from five countries took part, including five nurses, four physicians, three physiotherapists, one respiratory therapist and one exercise physiologist. Experience in delivering PR and/or caring for people with ILD ranged from 4 to 30 years. All were practicing in developed countries. Three themes were identified from the interviews (Table 3).
PR for ILD improves function, reduces symptoms and provides social support
Clinicians were enthusiastic about the role of PR in improving exercise capacity, symptoms and day-to-day functioning in ILD. Exercise training was seen as critical to achieving these goals. The role of the group environment in providing social support was also emphasized. The group makes something different, okay? So they see 15 other patients with the same symptoms, the same disease, so they start to talk about their disease and so on. Then after, they start laughing about who has higher desaturation during exercise. So I think it helps them. (C11, exercise physiologist)
Content of PR
The majority of clinicians identified areas where the educational needs of people with ILD differed from those with COPD. If they’re not taking inhalers, I’m not sure it’s very helpful for them to hear about it. (C4, nurse) An exacerbation of ILD wouldn’t be relevant to somebody with COPD because the causes can be quite different. And the treatment is quite different. (C6, nurse)
Topics consistently identified as being critical to ILD education were management of cough and use of oxygen therapy. The cough is a huge burden for them, so tips and strategies on how they can, or if they can, manage their cough. (C3, physiotherapist)
Many clinicians also felt that education in PR should be tailored according to the type of ILD. …connective tissue related ILD is linked to joint pain, joint problems, restricted mobility…having an awareness of oxygen needs in the IPF group…. (C10, physiotherapist)
However, a minority of clinicians felt that it would not be possible to tailor the education program according to the underlying diagnoses of people with ILD. …there are so many types of ILD, I think you’ll struggle to provide educational resources that cover them all in one program. (C13, respiratory physician)
Most clinicians thought it was helpful for patients to understand the types of treatments available, even where options were limited. This included the role of clinical trials. …for many ILDs there’s not a lot of treatment options at the moment and I think in those cases it would be useful to know where the state of the science is at, and to understand why their doctors would perhaps be encouraging them to participate in clinical trials. (C1, physiotherapist)
A small number of clinicians expressed concern about the capacity of PR staff to lead such a discussion, given the complex and rapidly changing nature of medical treatments. Well it depends on the competence of those administering the rehabilitation programme and what sort of credentials they have to discuss pharmacotherapeutics. (C13, respiratory physician)
Discussing the future in PR
Some clinicians felt that prognosis should be discussed in PR education sessions and perceived this information as important to patients. Patients always need to know what their outlook is, what the expected disease behaviour will be with time. What symptoms they are likely to experience and because of their disease and what disability they can expect. (C9, respiratory physician)
However the difficulties inherent in providing this information were acknowledged, either because it conflicted with the perceived role of PR, or because prognosis was uncertain. That is really a tricky area because you know, in rehab…we’re there to help patients improve their function, improve their symptoms, improve their mood…and to have a discussion about the high mortality and the lack of treatment is difficult you know. (C4, nurse) I think with COPD it’s much more straightforward with the disease trajectory. I think with ILD there isn’t a set prognosis…. (C7, respiratory physician)
Other clinicians did not feel that it was appropriate to provide information about prognosis in PR. In a pulmonary rehab program, you’re not the primary treating physician, so it’s not really your role to be telling them what their likely prognosis is or how the disease normally plays out. (C3, physiotherapist)
There was no consensus on discussion of end-of-life care in PR. Some clinicians felt that PR was a good location for discussing end-of-life planning and that the group setting was advantageous. …if you do it in a group as part of a lecture I think that’s actually less daunting…It’s actually good to have it in a group discussion without being specific to any individual. (C8, respiratory physician)
However, others felt strongly that discussions about end-of-life care should only happen in private. I think it’s extremely difficult for a person who is responsible for a group’s therapy to individualize a discussion about end of life. So I don’t think that’s a natural context for that very important discussion. (C9, respiratory physician)
Others felt that end-of-life planning was useful only to those patients with the worst prognosis. …planning for end of life measures…might not be relevant to all people with ILD. (C2, nurse)
Discussion
This is the first study to explore the perspectives of patients and clinicians regarding the role and content of education during PR for ILD. These results indicate that although people with ILD value participation in PR programmes that include people with other lung diseases, they have specific educational needs that may not be met by the current educational content. Some clinicians expressed significant reservations regarding inclusion of information on prognosis and end-of-life care, topics that were highly valued by patients.
People with ILD expressed a strong desire to receive information about disease trajectory during PR education sessions. Whilst a small number of clinicians also thought this was important to allow patients to prepare for the future, a larger number of clinicians did not think that this information could be adequately conveyed in this setting. The natural history of ILD can be highly variable, as some patients may remain stable for extended periods of time, whilst others have a rapidly progressive clinical course. 16 This variability contributed to the reluctance of clinicians to broach this subject. However, given the value that patients placed upon this topic, it may be difficult for PR clinicians to avoid it entirely. It could be argued that this dilemma is common to COPD, which is now recognized as a disease of variable prognosis with phenotypes that have differing risks for morbidity and mortality. 17 The role of clinicians in PR may be to acknowledge variability in prognosis whilst emphasizing the health behaviour changes that are thought to impact on long-term outcome, such as optimizing peripheral muscle function and aggressive management of co-morbidities. 4
Clinicians and patients agreed that information on current ILD treatments should be provided in PR. Similar to the discussions of treatment options for COPD that currently occur during PR, 4 neither group suggested that PR was a place where specific treatments should be recommended for individuals, rather that a clearer understanding of the purpose and side effects of treatments would be beneficial. Staffing for PR programmes varies according to local resources and such information may be delivered by a doctor, pharmacist, nurse, physiotherapist or respiratory scientist. 18 Inclusion of treatment information specific to ILD is not addressed in recent guidelines for PR. 4 If PR clinicians are to be well equipped for such discussions, consideration must be given to how ongoing, up-to-date professional development can be delivered.
People with ILD valued the opportunity to be included in existing PR programmes, but identified specific needs that may not be currently addressed in education programmes. This included management of cough, a frequent and distressing symptom with few evidence-based treatments. 3 Both patients and clinicians thought that sharing their strategies for cough management in a group environment would provide useful support. Many participants with ILD were enthusiastic about discussing end-of-life care in PR, although there were some dissenting voices who would prefer to have the discussion in private, whilst clinicians were much less certain about the merit of including this topic at all. The patient perspectives are consistent with a previous study showing that people with a range of chronic respiratory diseases valued the opportunity to take part in a structured, group-based session on advance care planning in PR. 19 Currently, the only education topic for ILD that is specifically mentioned in PR guidelines is the benefits of exercise. 20 The broad educational needs of people with ILD, along with the lack of consensus between clinicians and patients regarding the important topics, suggests that more work should be done to determine a relevant, acceptable curriculum for PR education in ILD.
The strengths of this study are that it is the first to systematically examine the educational needs of people with ILD in PR; we included the perspectives of both individuals with ILD and clinicians; we included patient participants with a wide range of disease severity and we included participants with both IPF and non-IPF diagnoses. The weaknesses include the small sample size and the absence of an international sample of participants with ILD, such that the perspectives documented here may not reflect the full range of perspectives of people with ILD, particularly those managed in other locations. In addition, this study did not document the perspectives of PR participants with other diagnoses (e.g. COPD, asthma and bronchiectasis) on the inclusion of ILD-specific content in PR.
Conclusion
People with ILD value the opportunity to attend PR education sessions but identify topics specific to their needs that are not currently included. Patients and clinicians do not agree on the most important topics for inclusion. Development of a comprehensive PR curriculum for ILD should consider how to incorporate information that is important to patients, along with strategies to support clinicians in its delivery.
Footnotes
Funding
This research was supported by a grant from the American Thoracic Society Foundation and the Pulmonary Fibrosis Foundation.