
Abstract
Depression carries enormous global morbidity and is 1.5–7 times likelier to occur in individuals with chronic illness than in the general population. Idiopathic pulmonary fibrosis (IPF) has a rising incidence with a severe impact on quality of life. An indication of the prevalence of depression in this group is therefore of paramount interest. A prospective study was performed. A total of 118 participants with IPF who attended the interstitial lung disease clinic in Ninewells Hospitals, Dundee, Scotland, from May 2010 to September 2011 were recruited. Informed consent was obtained. The male to female ratio was 60:58. The Wakefield Self-assessment of Depression Inventory was used (scores ≥15 denote a depressed state). Pulmonary function tests were measured to correlate disease severity with depression scores. Of them, 58 patients had significant depressive symptoms scoring ≥15; only nine were taking antidepressant medication. The mean depression score of female participants was 15.0 ± 0.77 (SD 5.9), compared with a mean male score of 13.1 ± 0.99 (SD 7.5). Disease severity, age, duration since diagnosis and number of co-morbidities were not significantly correlated with depression. The study population had a high prevalence of depressive symptoms. Medical therapy for pulmonary fibrosis is limited and therefore palliation of symptoms and pulmonary rehabilitation form the main strategy for management. Depression should be actively screened in patients with IPF.
Introduction
Idiopathic pulmonary fibrosis (IPF) is a diffuse parenchymal lung disease characterised by a devastating distortion of pulmonary structure by abnormally proliferating fibroblasts. 1 The median duration of symptoms before diagnosis is 1–2 years with most patients referred to cardiology for exertional dyspnoea prior to a respiratory referral. 2 A small minority are asymptomatic at diagnosis; in the remainder, symptoms typically develop 2.7 years after radiographic detection of pulmonary abnormality. 2
Several causes for IPF have been proposed, including metal particles, smoking, sawdust and diabetes mellitus. 1,3,4 Reflux of gastric contents in gastro-oesophageal reflux disease (GORD) has also long been associated with IPF, 5 and more recent studies have promisingly corroborated this link. 6,7 Tobin et al. reported 17 IPF patients with 16 having abnormal oesophageal acid exposure 8 and indeed, there are at least four reported cases in the literature, where treatment of GORD in patients with IPF showed improvement in pulmonary function. 9 There is therefore indication of the role of GORD in the pathogenesis and prognosis of IPF.
The association of IPF with multiple co-morbidities, including pulmonary hypertension and emphysema, is well documented. 8,10 –12 It is also well established that major depressive illness is an extremely burdensome global morbidity. 13 –18 Depression in individuals with chronic illness is 1.5–7 times likelier to occur than in the general population. 19 –21 There is some evidence of the increased incidence of depressive symptoms in IPF patients in studies investigating the quality of life (QoL) status of these patients. 22,23 However, there remains a prominent paucity of large prospective studies addressing the diagnosis and management of depression in patients with IPF and its impact on the health status of these individuals. With the incidence of IPF at 7.4/100,000 person years, a figure which is seeing an annual increase, 24 an indication of the prevalence of depression in this group is of paramount interest.
Pulmonary rehabilitation remains the main strategy for this group of patients. It has an established role in the management of chronic obstructive pulmonary disease (COPD) and has been previously shown to reduce symptoms of anxiety and depression in these patients. 25 It is also associated with reduced breathlessness, improved health-related QoL and fewer hospital admission. 26
The aim of this study was to assess the presence of depressive symptoms in patients suffering from IPF and to investigate whether functional severity of disease correlated with the depression score. Current treatment strategies are also discussed.
Materials and methods
Participants
A total of 118 patients suffering from IPF who attended the interstitial lung disease clinic at Ninewells Hospital, Dundee, Scotland, from May 2010 to September 2011 were recruited for this study. The diagnosis of pulmonary fibrosis was based on high-resolution computerised tomography of the chest and surgical and transbronchial biopsies of the lung. Patients were excluded if they refused consent, had a lack of competency in completing the questionnaire, had depression prior to a diagnosis of pulmonary fibrosis or whose notes could not be found.
All participants gave informed consent and ethical approval was obtained from the local ethics committee. References for the study are 12/ES/0014 (NHS Tayside Research Ethics Committee reference).
Outcome measures
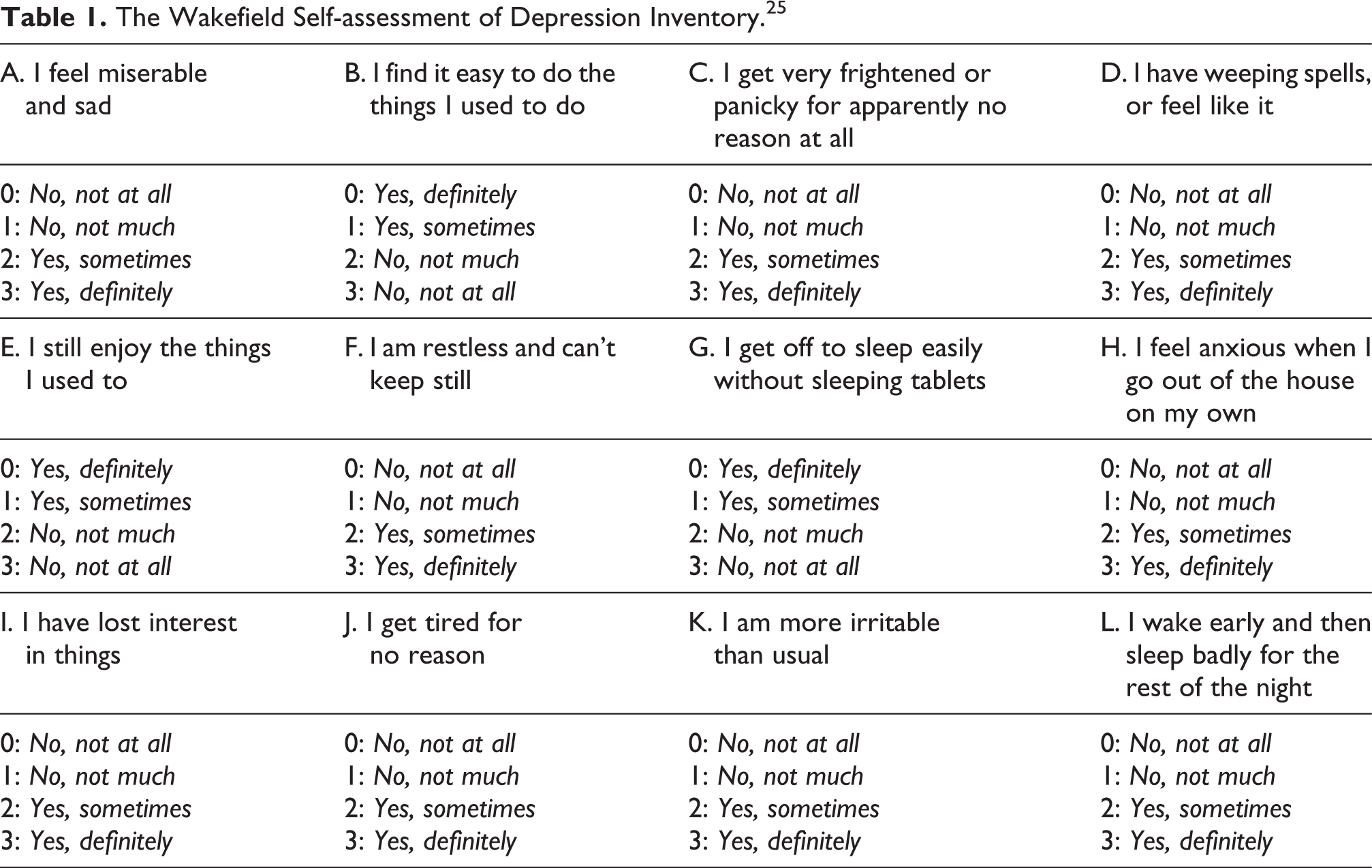
The Wakefield Self-assessment of Depression Inventory (WDI; Table 1) was used to assess depression status. 27 This consists of 12 questions with 4 possible answers each; participants are asked to read each question carefully, one at a time, and underline or circle the response that best indicates how they feel at the time of completion. Each answer is scored on a scale of 0–3; collating each answer generates a depression rating score of 36. A score of ≥15 suggests a high frequency and intensity of the symptoms often associated with depression (e.g. lethargy, anorexia, low self-esteem, anxiety, etc.), though it does not imply a diagnosis of the condition, similar to alternative depression rating scales. 28 The WDI has previously been used with success in studies investigating depression in patients with other pathologies 29,30 and, furthermore, can independently be completed by the patient, reducing investigator bias.
The Wakefield Self-assessment of Depression Inventory. 25
Procedures
Patients were asked to read carefully the instructions on the questionnaire and to complete it as accurately and honestly as possible. The questionnaires were administered by the primary author. Participants were instructed to indicate how they felt at the time of completion, rather than how they were in the past, or how they would hope to be. After completion, questionnaires were handed to a receptionist in an unmarked envelope. Throughout the study, confidentiality was maintained. Functional severity of disease was assessed by various measurements including forced expiratory volume in 1second (FEV1), the forced vital capacity (FVC), the ratio of FEV1 to FVC, the gas transfer factor and the gas constant. Ethical approval was obtained.
Data analysis
The prevalence of depression was calculated by assessing the percentage of participants scoring ≥15 on the WDI. The relationship between depression scores and lung function measurements was investigated by the Pearson’s product-moment correlation coefficient. An unpaired t test was used to assess significance between male and female mean depression scores. Basic analyses were conducted using the software Microsoft Excel 2007. The level of significance was set at 0.05.
Results
Demographic summary
The study population comprised of 118 patients (60 males and 58 females). Baseline characteristics are summarised in Table 2. Age ranged between 34 and 96 (68.1 ± 11.35) years. The duration since diagnosis varied from 1 month to 30 years (3.9 ± 4.1 years). Over half of the patients were either current (15) or ex-smokers (59).
Demographic summary of study population.

COPD: chronic obstructive pulmonary disease; GORD: gastro-oesophageal reflux disease.
aRepresented as mean ± SD.
Of them, 16 patients (13.6%) had GORD and 27 (22.9%) were using proton pump inhibitors due to complaints of indigestion. There was significant co-morbidity in the study population, with 92.4% of participants having at least one co-morbidity (Figure 1); the commonest co-morbidities were connective tissue disease (23), COPD (19), GORD (16), diabetes (14), obesity (12), depression (9) and sarcoidosis (7).

Frequency of co-morbidities.
Prevalence of depression
A high prevalence of depressive symptoms was found in the sample. The mean depression score was 14.1 ± 0.63 (SD 6.8). A total of 58 patients (49.2%) scored ≥15. Depression scores were subsequently correlated with various parameters including age, duration since diagnosis, number of co-morbidities and lung function measurements (Table 3). Correlation coefficients between depression score and FEV1 (r = −0.20), FVC (r = −0.20), gas transfer factor (r = −0.23) and the gas constant (r = −0.05) were significant (all p < 0.05). Correlation between depression score and duration since diagnosis (r = −0.11), FEV1–FVC ratio (r = 0.05), age (r = −0.08) and number of co-morbidities (r = −0.08) was not significant (all p > 0.05).
Correlation coefficients between depression score and various parameters.

FEV1: forced expiratory volume in 1second; FVC: forced vital capacity.
The mean depression score of female participants was 15.0 ± 0.77 (SD 5.9), compared with a mean male score of 13.2 ± 0.99 (SD 7.6; Figure 2). This difference was not statistically significant (t = −1.39, p = 0.17). Of the 58 patients scoring ≥15, only the nine patients with previously diagnosed depression were started with the anti-depression therapy. No patient was offered pulmonary rehabilitation due to lack of availability of a rehabilitation programme at the time of the study.

Gender-specific frequency of depression scores.
Discussion
There is a paucity of literature with respect to the prevalence of depression in pulmonary fibrosis. In contrast, several studies have attempted to demonstrate the incidence of depression in COPD patients, with rates varying from 6 to 50% in various reported series. 28,31,32 We have shown in a large prospective study that 49.2% of individuals with IPF scored ≥15 on the WDI, suggesting a high frequency and intensity of depressive symptoms in these patients. This is higher than trends seen in the general UK population (i.e. a 2.6% national point prevalence of depression, 11.4% of ‘mixed depression and anxiety’ and a 6% annual and 15% lifetime incidence of an episode of depression) 33,34 but similar to the levels reported with COPD. In keeping with the literature, 17 –19 female participants were more depressed than their male counterparts, though this was not statistically significant. Further work to elucidate the significance of social support and home circumstances as depressive correlates is needed. Statistically significant negative correlations were found between depression scores and gas transfer factor measurements, FEV1 and FVC. However, the weakness of the correlations (r = −0.20, −0.20 and −0.23, respectively) and the lack of statistically significant correlation with the gas constant and FEV1–FVC ratio suggest these are unlikely to be of a significantly pertinent nature. There was also no significant correlation between depression score and duration since diagnosis, age and number of co-morbidities.
Though this questionnaire cannot be used to diagnose depression, it is a valuable screening tool and an effective correlate for depressive symptoms. 27,30 There is a possibility that some patients scoring high on the questionnaire may have other physical or psychological illness. Conversely, scores <15 may still warrant psychiatric consultation if the stress or dysfunction is substantial.
Many IPF patients faced with a gradual and progressive realisation of the severity and poor prognosis of their condition. Worsening lung function means that daily living is severely affected, which has numerous social and psychological implications. There is presently very limited medical treatment for IPF. The Idiopathic Pulmonary Fibrosis International Group Exploring N-Acetylcysteine I Annual (IFIGENIA) trial recommends a triple therapy consisting of N-acetyl cysteine, azathioprine and prednisolone,
36
though initial findings from the ongoing phase III Prednisone, Azathioprine, and N-acetylcysteine: A Study That Evaluates Response in IPF (PANTHER-IPF) study suggests increased mortality, poor compliance and lack of therapeutic benefit.
37
The European Respiratory Society further recommends lung transplantation;
35
this appears to be the sole therapeutic treatment at present. 5-year survival rates following lung transplantation have been shown to be as high as 72%.
38
Presently, however, most patients undergoing lung transplantation have other forms of fibrotic lung diseases and eligibility and timing of transplantation that vary from centre to centre.
35
The waiting time for lung transplantation coupled with a median survival of 2–3 years for these patients makes this a difficult option to utilise for many patients. It appears, therefore, that for the present, the World Health Organization’s advice to initiate best supportive care (BSC) remains the most effective strategy to alleviate symptoms and QoL indicators.
39
For IPF patients, BSC must take into account a number of aspects. Appropriate analgesia and O2 supplementation; oral opiates to control cough and dyspnoea and control of GORD symptoms, if present; pulmonary rehabilitation; cessation of smoking; optimisation of drug therapy; physical, psychosocial and spiritual care.
There is currently little evaluation of the efficacy of the various aspects of BSC for IPF patients. However, the value of pulmonary rehabilitation in managing COPD is well documented. 25 Deconditioning, severe breathlessness, impaired QoL, nutritional deficit, fatigue and social isolation are common both in patients with COPD and IPF and hence pulmonary rehabilitation may be beneficial in IPF also. Nevertheless, there is a lack of large, well-controlled trials investigating the benefits of pulmonary rehabilitation in this subpopulation. A few observational studies have demonstrated improvement in exercise tolerance and QoL measures over several weeks of pulmonary rehabilitation in IPF patients. 40 –42 Although the severity, disablement and shortened life expectancy of IPF patients might be comparable with other serious illnesses such as cancer and COPD, the disease has met with limited focus, and few rehabilitation programmes have been prepared for patients suffering from IPF. A larger study is needed in order to define the benefits of IPF-specific pulmonary rehabilitation. It is recommended that for now, pulmonary rehabilitation be carried out based on the same criteria as COPD.
The high burden of depression in IPF should not be ignored; in our study, nearly half the patients had high WDI scores. Patients on antidepressants still had high scores for depression suggesting a role for other therapeutic interventions such as cognitive behavioural therapy. Depression should be actively screened in patients with pulmonary fibrosis and appropriate supportive treatment, including antidepressant medication and psychological counselling, be therefore offered.
Footnotes
Conflict of Interest
The authors declared no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.