
Abstract
Chronic lower airway diseases, including chronic obstructive pulmonary disease (COPD) and asthma, are currently the third leading cause of death in the United States. We aimed to evaluate changes in prevalence of and risk factors for COPD and asthma among the US adult population. We evaluated changes in prevalence of self-reported doctor-diagnosed COPD (i.e. chronic bronchitis and emphysema) and asthma and self-reported respiratory symptoms comparing data from the 1988–1994 and 2007–2010 National Health and Nutrition Examination Surveys. To investigate changes in the severity of each outcome over the two periods, we calculated changes in the proportions of spirometry-based airflow obstruction for each outcome. Prevalence of doctor-diagnosed chronic bronchitis and emphysema decreased significantly mainly among males, while asthma increased only among females. The self-reported disease and the respiratory symptoms were associated with increased prevalence of airflow obstruction for both periods. However, the prevalence of airflow obstruction decreased significantly in the second period among those with shortness of breath and doctor-diagnosed respiratory conditions (chronic bronchitis, emphysema, and asthma). COPD outcomes and asthma were associated with lower education, smoking, underweight and obesity, and occupational dusts and fumes exposure. Chronic lower airway diseases continue to be major public health problems. However, decreased prevalence of doctor-diagnosed chronic bronchitis and emphysema (in males) and decreased prevalence of airflow obstruction in those with respiratory symptoms and doctor-diagnosed respiratory diseases may indicate a declining trend and decrease in disease severity between the two periods. Continued focus on prevention of these diseases through public health interventions is prudent.
Introduction
Asthma and chronic obstructive pulmonary disease (COPD) are common conditions characterized by airway obstruction. Asthma is marked by episodic chest tightness, wheezing, coughing, and breathlessness associated with variable and reversible airflow obstruction. 1 COPD includes chronic bronchitis, defined by the presence of recurring symptoms of chronic productive cough for a minimum of 3 months in two or more consecutive years, and emphysema, characterized by destruction of the alveolar walls and permanently enlarged terminal air spaces. 2 Airflow obstruction in COPD is not fully reversible. 3
In 2008, direct health-care costs in the United states related to COPD and asthma totaled US$53.7 billion; indirect costs due to lost productivity amounted to an additional US$14.3 billion. 4 Recent reports indicate that deaths from chronic lower airway diseases, which include COPD and asthma, are on the rise and are currently the third leading cause of death in the United States. 5
Smoking is recognized as the primary cause of emphysema 6 and as the most common risk factor for chronic bronchitis and COPD; however, occupational and environmental exposures also contribute to the increased risk of these diseases. 6 –8 Studies have demonstrated that occupational exposure can contribute to the development of small airways disease 9 and emphysema. 10,11 About 15% of COPD and 15% of asthma cases are estimated to be attributed to occupational exposures. 12 –16 However, the contribution of occupational and environmental exposures to COPD and asthma is often difficult to discern in individual patients; this applies especially to COPD among smokers. 17 Additionally, about 2% of COPD cases 18 are associated with a genetic mutation causing α1-antitrypsin deficiency. 19
The most recent estimate of the prevalence of respiratory symptoms and doctor-diagnosed COPD and asthma in the US population using the National Health and Nutrition Examination Survey (NHANES) was reported using data from NHANES III (1988–1994). 20,21 Estimated prevalence of COPD, among US adults aged 25 and older, was 15.1% based upon lung function testing by spirometry and 5.2% based upon doctor diagnosis of COPD (either chronic bronchitis, emphysema, or both). 22 The estimated prevalence of doctor-diagnosed current asthma among those 20 years and older was 4.5%. However, the prevalence of wheezing was higher, with a prevalence of 16.4%. 23 The most recent NHANES 2007–2010 study included a respiratory component and provides an opportunity to evaluate changes in the prevalence of respiratory symptoms and doctor-diagnosed obstructive airway diseases in the US population since 1988–1994 and an opportunity to evaluate the contribution of individual and occupational risk factors to chronic lower airway diseases.
The objective of our study was to investigate trends in the prevalence of chronic lower airway disease in the US population focusing on self-reported doctor-diagnosed COPD and asthma, respiratory symptoms, and airflow obstruction measured by spirometry. For this purpose, we compared prevalence of these diseases and conditions using NHANES data obtained from 1988 to 1994 and from 2007 to 2010 surveys. In addition, we investigated the associations between occupational risk factors and chronic lower airway diseases (self-reported symptoms, self-reported doctor diagnosis, and airflow obstruction) using the most recent NHANES 2007–2010 data.
Methods
Study population
NHANES is a series of cross-sectional health interview and health examination surveys designed to select and study a representative sample of the US population and is conducted by the National Center for Health Statistics at the Centers for Disease Control and Prevention. Study participants completed an interview followed by a physical assessment at a mobile examination center. Participants answered questions about respiratory symptoms and doctor-diagnosed respiratory diseases. For this report, we used data collected during 1988–1994 and 2007–2010 surveys. Informed consent was obtained from all participants and the National Center for Health Statistics Research Ethics Review Board approved the protocol. National Health and Nutrition Examination Survey data are publically accessible from the US Centers for Disease Control and Prevention National Center for Health Statistics Web site http://www.cdc.gov/nchs/nhanes.htm.
Our study sample was limited to adults aged 40–79 years. The 1988–1994 survey classified participants as non-Hispanic White, non-Hispanic Black, Mexican American, or other. ‘Other Hispanic’ was an additional race/ethnicity category added in the 2007–2010 survey.
Variable definition
Self-reported symptoms
Chronic Bronchitis
Participants were considered to have symptoms of chronic bronchitis if they responded affirmatively to the following questions about chronic cough and chronic phlegm: “Do you usually cough on most days for 3 consecutive months or more during the year?”; “Do you usually bring up phlegm on most days for 3 consecutive months or more during the year?” and reported an answer greater than or equal to 2 years to the following questions: “For how many years have you had this cough?”; “For how many years have you had this trouble with phlegm?”.
Wheezing
No questions were asked consistently between the two surveys, which could develop a case definition for asthma based upon diagnostic symptoms recommended by the National Asthma Education and Prevention Program. 24 One question about wheezing was consistently asked in both surveys, therefore we report on the prevalence of recent wheezing. Participants were classified as having symptoms of wheezing if they answered affirmatively to “Have you had wheezing or whistling in your chest at any time in the past 12 months?”.
Shortness of breath
A question examining shortness of breath on exertion was also asked in both surveys. Participants in the 1988–1994 survey were classified as having shortness of breath if they responded affirmatively to “Are you troubled by shortness of breath when hurrying on level ground or walking up a slight hill?”. Participants in the 2007–2010 survey were classified as having shortness of breath if they responded affirmatively to “Have you had shortness of breath either when hurrying on the level or walking up a slight hill?”.
Self-reported doctor and/or health professional diagnosed conditions
When comparing the two surveys, questions assessing the presence of doctor-diagnosed conditions were asked in a slightly different manner. In the 1988–1994 survey, participants were asked “Has a doctor ever told you that you had…”, whereas in the 2007–2010 survey participants were asked “Has a doctor and/or other health professional ever told you that you had…” For simplicity purposes, we will refer to responses from both surveys regarding diagnosed conditions as “doctor-diagnosed.”
Doctor-diagnosed chronic bronchitis
Participants were considered to have doctor-diagnosed chronic bronchitis if they responded positively to “Has a doctor (and/or health professional in the case of the 2007–2010 survey) ever told you that you had chronic bronchitis?” and “Do you still have chronic bronchitis?”.
Doctor-diagnosed emphysema
Participants were considered to have doctor-diagnosed emphysema if they responded positively to “Has a doctor (and/or health professional in the case of the 2007–2010 survey) ever told you that you had emphysema?”.
Doctor-diagnosed asthma
Participants were considered to have doctor-diagnosed current asthma if they responded positively to “Has a doctor (and/or health professional in the case of the 2007–2010 survey) ever told you that you had asthma?” and “Do you still have asthma?”.
Airflow obstruction
The severity of the self-reported symptoms of chronic bronchitis as well as self-reported doctor diagnoses of chronic bronchitis and emphysema were compared for each period by evaluating the prevalence of airflow obstruction measured by spirometry. We used the American Thoracic Society (ATS) criteria of mild or worse (mild+) airflow obstruction 25 defined as the ratio of forced expiratory volume in 1 second (FEV1) to the forced vital capacity (FVC) less than the lower 5th percentile (i.e. lower limit of normal (LLN) 26 ; FEV1/FVC < LLN). Moderate or worse (moderate+) airflow obstruction was defined as FEV1/FVC < LLN plus FEV1 < 70% predicted based on the ATS criteria. 25 Further descriptions of methods for spirometry testing, interpretation, and defining airflow obstruction have been described previously. 27
Demographics
Demographic variables and risk factors investigated were age, race, education, smoking status, body mass index (BMI), and occupational exposure. Smoking status was categorized by never smokers (those who had smoked less than 100 cigarettes in their entire life), ex-smokers (those who had smoked more than 100 cigarettes in their entire life, but did not currently smoke), and current smokers. The pack-years variable was estimated by multiplying current number of packs smoked by the number of years the participant reported smoking. For ex-smokers, pack-years was determined using the number of packs they reported smoking when they last smoked.
Occupational variables
Occupational exposure variables were created from responses to the occupational questionnaire module administered in the 2007–2010 survey. Participants between the ages 16 and 79 who indicated that they were employed, either currently or at one point in their lives, were asked occupational exposure questions. Occupational exposure to mineral dust was classified as an affirmative answer to “In any job, have you ever been exposed to dust from rock, sand, concrete, coal, asbestos, silica or soil?”. Occupational exposure to organic dust was classified as an affirmative answer to “In any job, have you ever been exposed to dust from baking flours, grains, wood, cotton, plants, or animals?”. Occupational exposure to exhaust fumes was classified as an affirmative answer to “In any job, have you ever been exposed to exhaust fumes from trucks, buses, heavy machinery, or diesel engines?”. Occupational exposure to other fumes was classified as an affirmative answer to “In any job, have you ever been exposed to any other gases, vapors, or fumes? Examples are vapors from paints, cleaning products, glues, solvents, and acids; or welding/soldering fumes.”. These variables were also combined into the following variables “ever dust and/or fume exposure,” “ever dust exposure,” and “ever fume exposure.”
Statistical data analysis
Age-standardized prevalence were estimated using Statistical Analysis System (SAS), version 9.3 software, procedure PROC SURVEYREG, 28 which accounted for the study design and NHANES examination weights assigned to each participant. Age standardization to the US population of 2000 was applied to the estimated prevalence for the 1988–1994 and 2007–2010 periods using national Current Population Survey population size tables. 29 –31 The weighted frequencies and means were derived using SAS procedure PROC SURVEYFREQ and PROC SURVEYMEANS, accounting for the study design and examination weights. To compare the prevalence estimates from NHANES 1988–1994 and 2007–2010, PROC SURVEYLOGISTIC was used to calculate the Wald statistic and p values evaluation if the distribution of demographic characteristics between the two time periods was statistically different. PROC SURVEYREG was used to calculate a t statistic and assess whether the mean pack-years among smokers in the two survey periods was statistically different.
Demographic-specific prevalence of symptoms of chronic bronchitis, wheezing, and shortness of breath, as well as doctor-diagnosed emphysema, chronic bronchitis, and asthma, were calculated for both survey periods. Additionally, age-standardized prevalence of ATS mild+ and moderate+ airflow obstruction according to the presence or absence of respiratory symptoms or doctor-diagnosed respiratory diseases was calculated for the participants who completed spirometry testing. Multiple logistic regression using PROC SURVEYLOGISTIC was used to estimate odds ratios (ORs) (and 95% confidence intervals (CIs)) for the association of respiratory symptoms, as well as doctor-diagnosed chronic bronchitis, emphysema, and asthma and airflow obstruction with education, smoking status, BMI, and self-reported occupational exposure to dusts and fumes, adjusting for the effect of age, sex, and race, for NHANES 2007–2010 respondents who reported ever employment.
Results
Table 1 shows descriptive statistics for NHANES 1988–1994 and NHANES 2007–2010 participants aged 40–79. In this age range, mean age (55.8 vs. 55.5 years, p = 0.32) and age distribution were similar for the two study samples. Proportions of males and females sampled in the two surveys were not statistically different (p = 0.22). Compared to the 1988–1994 survey, the 2007–2010 sample had a higher proportion of non-Hispanic Black and Mexican American participants and had a significantly higher level of education reported among participants (some college 16.8% vs. 27.5%.; college graduate 21.3% vs. 27.9%; p < 0.0001). The mean BMI was significantly higher in the 2007–2010 survey (27.4 vs. 29.2 kg/m2; p < 0.0001). The frequency of obesity, defined as BMI of 30 kg/m2 or greater, increased by nearly 10 percentage points in 2007–2010 (27.2% vs. 37.7%; p < 0.0001). Conversely, the proportion of participants with normal BMI (18.5–24.9 kg/m2) decreased by almost the same amount in 2007–2010 (34.8% vs. 25.1%; p < 0.0001). The 2007–2010 sample had a significantly higher proportion of never smokers (39.9% vs.51.2%; p < 0.0001) and significantly decreased mean pack-years of smoking (29.4 vs. 24.5 pack-years; p < 0.0001) when the ex-smoker and current smoker categories were combined.
Descriptive statistics for NHANES 1988–1994 and NHANES 2007–2010 data for 40–79-year-olds.a

NHANES: National Health and Nutrition Examination Survey; NH: non-Hispanic; N/A = data not available; BMI: body mass index.
a“Other Hispanic” classification was not available in NHANES III.
bCurrent Population Survey.
cData presented as mean pack-years with standard error in brackets.
Age-standardized estimated prevalence of symptoms of chronic bronchitis (Table 2) did not differ significantly between the two sample periods among any of the demographic categories. Significant decreases in the estimated prevalence of wheezing were observed among several demographic categories in 2007–2010 (ages 40–79, males, non-Hispanic Whites, Mexican Americans, and current smokers (data not shown)). Prevalence of shortness of breath significantly increased in 2007–2010 among non-Hispanic Blacks but decreased among Mexican Americans.
The US population age-standardized prevalence of self-reported respiratory symptoms among ages 40–79, 1988–1994 and 2007–2010.a
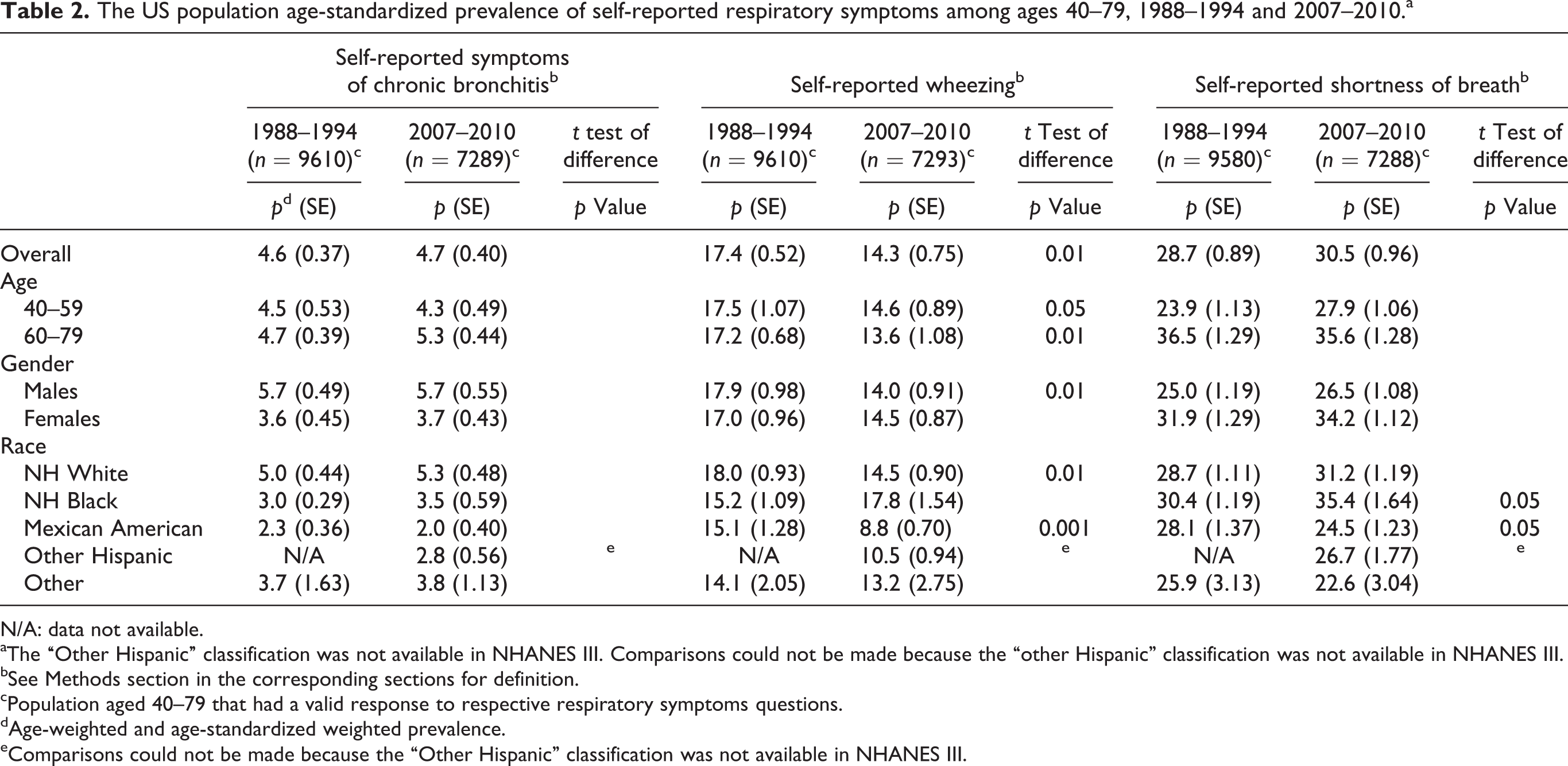
N/A: data not available.
aThe “Other Hispanic” classification was not available in NHANES III. Comparisons could not be made because the “other Hispanic” classification was not available in NHANES III.
bSee Methods section in the corresponding sections for definition.
cPopulation aged 40–79 that had a valid response to respective respiratory symptoms questions.
dAge-weighted and age-standardized weighted prevalence.
eComparisons could not be made because the “Other Hispanic” classification was not available in NHANES III.
Age-standardized estimated prevalence of doctor-diagnosed conditions is summarized in Table 3. Prevalence of doctor-diagnosed chronic bronchitis decreased significantly in 2007–2010 overall and specifically among several demographic categories (ages 50–59 and 70–79, males, non-Hispanic Whites, Mexican Americans, and current smokers (data not shown)). Prevalence of doctor-diagnosed emphysema remained stable between the two sample periods, except for males where the prevalence decreased significantly in 2007–2010 (4.7% vs. 2.7%; p < 0.001). The prevalence of doctor-diagnosed current asthma significantly increased in 2007–2010 overall and among several demographic categories (ages 60–69, 70–79, females, non-Hispanic Whites, non-Hispanic Blacks, and among never smokers, ex-smokers, and current smokers).
The US population age-standardized prevalence of self-reported doctor-diagnosis among persons 40–79 years, 1988–1994 and 2007–2010.a
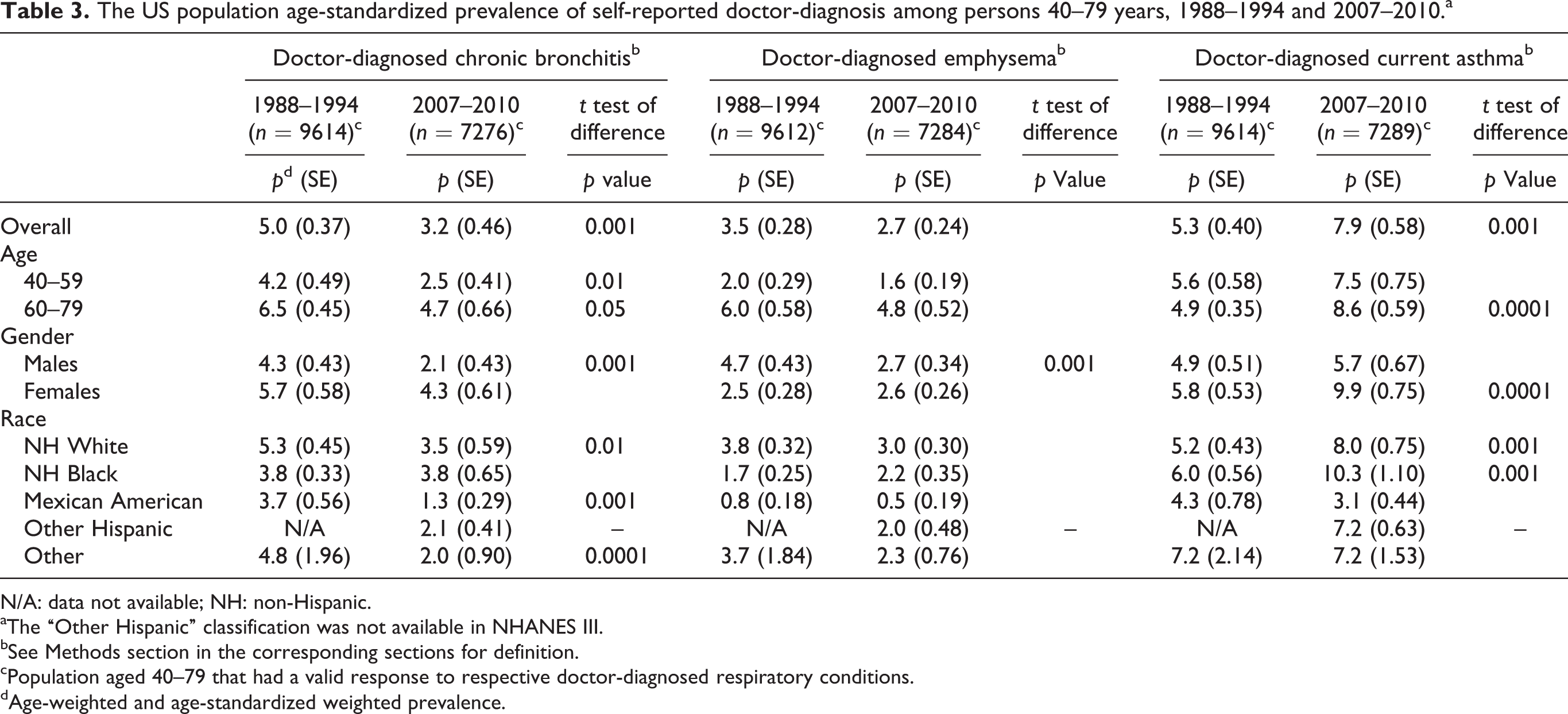
N/A: data not available; NH: non-Hispanic.
aThe “Other Hispanic” classification was not available in NHANES III.
bSee Methods section in the corresponding sections for definition.
cPopulation aged 40–79 that had a valid response to respective doctor-diagnosed respiratory conditions.
dAge-weighted and age-standardized weighted prevalence.
From the 1988–1994 survey, 90% of those aged 40–79 and from the 2007–2010 survey 77% of those aged 40–79 had valid spirometry and sufficient biometric data to evaluate lung function. 27 Table 4 shows the prevalence of mild+ and moderate+ airflow obstruction measured by spirometry, as defined by ATS criteria, for the two study periods, by the presence of respiratory symptoms, and doctor-diagnosed respiratory diseases among individuals aged 40–79 years. For example, among those with doctor-diagnosed emphysema in the 1988–1994 survey, 59.41% had mild+ airflow obstruction. Conversely, among those who did not report a doctor diagnosis of emphysema during the same period, 15.13% had mild+ airflow obstruction. Overall, the prevalence of mild+ and moderate+ airflow obstruction significantly decreased in 2007–2010. Table 4 also demonstrates that the presence of self-reported respiratory symptoms and doctor-diagnosed disease (chronic bronchitis, emphysema, and asthma) was significantly associated with increased prevalence of airflow obstruction as determined by spirometry for both periods. However, the prevalence of mild+ and moderate+ airflow obstruction decreased significantly among those with shortness of breath and the doctor-diagnosed conditions of chronic bronchitis, emphysema, and asthma in 2007–2010.
The US population age-standardized prevalence of airflow obstruction according to the presence or absence of self-reported respiratory symptoms and diseases among persons 40–79 years with valid spirometry.

ATS: airflow obstruction.
aNHANES III (1988–1994) total participation with valid data n = 20,050.
bNHANES 2007–2010 total participation with valid data n = 20,686.
cAge-weighted and age-standardized weighted prevalence.
dSee Methods section for definition.
eSignificant at α = 0.01.
fPrevalence of airflow obstruction in those with self-reported symptoms/doctor-diagnosed condition are significantly higher than those without symptoms/condition among the same survey period at α = 0.0001.
gPrevalence of airflow obstruction in those with self-reported symptoms/doctor-diagnosed condition are significantly higher than those without symptoms/condition among the same survey period at α = 0.01.
Table 5 shows associations (OR) between selected risk factors and chronic lower airways disease. The associations with lower education, current and ex-smoking status, and BMI outside the range of 18.5–29.9 kg/m2 (normal + overweight BMI categories) showed an increasing trend. Participants reporting occupational exposure had significantly higher odds of all respiratory symptoms and doctor-diagnosed conditions than participants not reporting exposure. In particular, those reporting ever dust and/or fume exposure and ever dust exposure had twice the odds of chronic bronchitis symptoms compared with those not reporting these exposures (ever dust and/or fume exposure OR = 2.03, 95% CI: 1.44–2.87; ever dust exposure OR = 2.13 CI: 1.49–3.04). There were no significant associations between occupational exposure and airflow obstruction. Participants who reported occupational exhaust fume exposure had 20% greater odds of airflow obstruction than other participants, but this difference did not reach statistical significance.
Association between risk factors and self-reported respiratory symptoms, self-reported doctor-diagnosed conditions, and airflow obstruction among 40–79-year-olds, NHANES 2007–2010.
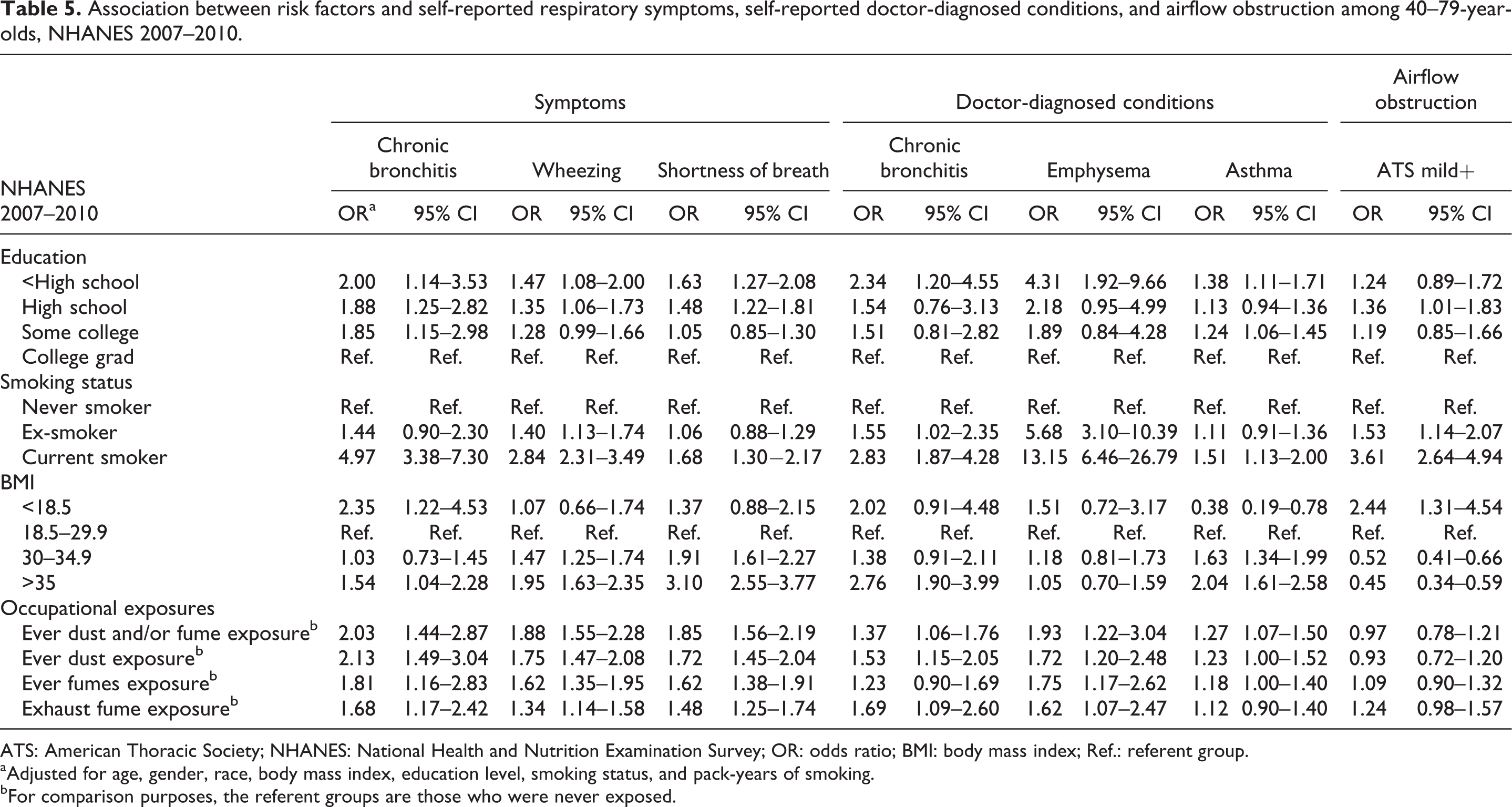
ATS: American Thoracic Society; NHANES: National Health and Nutrition Examination Survey; OR: odds ratio; BMI: body mass index; Ref.: referent group.
aAdjusted for age, gender, race, body mass index, education level, smoking status, and pack-years of smoking.
bFor comparison purposes, the referent groups are those who were never exposed.
Discussion
Our objectives were to investigate whether there was a change in the prevalence of COPD and asthma outcomes and/or a change in the severity of the conditions as reflected by the presence of airflow obstruction over time and evaluate the effect of individual and occupational risk factors on the prevalence of these conditions.
Summary of main findings
To explain changes in disease prevalence between the two surveys, we evaluated the changes in prevalence of individual risk factors such as smoking, BMI, and education over the two periods. We found decreased prevalence of current smoking (p < 0.0001) and decreased mean pack-years (p < 0.0001) among smokers in the 2007–2010 survey. Prevalence of obesity (BMI > 30 kg/m2) increased by more than 10% (p < 0.0001), while correspondingly the prevalence of the normal BMI category (BMI 18.5–24.9 kg/m2; p < 0.0001) decreased. In the 1988–1994 survey, over 62% of the population reported completing some high school or graduating from high school; however, in the 2007–2010 survey a majority reported attending some college or graduating from college (55%; p < 0.0001).
Occupational risk factors were evaluated using questions asked during the 2007–2010 survey about occupational dust and fume exposure among participants who reported they had ever worked. We found significantly increased ORs for the association between exposure to dusts and fumes and almost every respiratory symptom and doctor-diagnosed respiratory condition category. Most notably, the OR for ever dust exposure among those with chronic bronchitis was 2.13 (CI: 1.49–3.04). Interestingly, significant relationships between occupational exposure and airflow obstruction were not observed. However, it is possible that this could be attributed to the healthy worker effect. 32 Previous research has suggested that workers who take up and remain in jobs with exposure to dusts and other respiratory irritants tend to have increased initial levels of lung function when compared to workers who do not work in these conditions. 33,34
Disease-specific findings and relations to the literature
Chronic bronchitis
Chronic bronchitis was evaluated using two outcomes. The first outcome was the presence of chronic bronchitis symptoms as ascertained using a standard ATS-recommended definition and questions on chronic cough and phlegm. The second outcome was the self-reported doctor-diagnosed chronic bronchitis, also ascertained by questionnaire. Prevalence of chronic bronchitis symptoms did not change between the two surveys; however, we observed a decrease in the prevalence of self-reported doctor diagnosis of chronic bronchitis. Chronic bronchitis is a potentially disabling condition, and both outcomes were associated with higher prevalence of mild and moderate airflow obstruction. For both periods, the prevalence of airflow obstruction (mild+) was higher for those who reported chronic bronchitis symptoms than for the doctor-diagnosed chronic bronchitis, suggesting a substantial proportion of those with obstructive chronic bronchitis may be undiagnosed. However, when comparing the two surveys we observed a decrease in the prevalence of mild+ airflow obstruction in 2007–2010 among those with symptoms and/or doctor-diagnosed chronic bronchitis, which may indicate a decrease in disease severity between the two periods (Table 2). Additionally, significant decreases in the prevalence of doctor-diagnosed chronic bronchitis were observed among all age-groups and specifically among males, non-Hispanic Whites and Mexican Americans. Even though we have observed a decrease in the prevalence of doctor-diagnosed chronic bronchitis, the fact that prevalence of self-reported symptoms of chronic bronchitis has not changed since the NHANES III survey indicates that chronic bronchitis is still a major respiratory illness in the older US population. However, it is unclear whether factors like overreporting of symptoms by individuals or underdiagnosis by healthcare professionals are affecting the prevalence of reported disease.
Smoking is the most common risk factor for chronic bronchitis, and we observed that current smokers had higher odds of chronic bronchitis than others (OR = 4.97, CI: 3.38–7.30; Table 5). Smoking rates decreased between the two surveys which may have contributed to the reduced prevalence of doctor-diagnosed chronic bronchitis and the reduced prevalence of airflow obstruction in those with the disease. However, smoking is not the only risk factor for chronic bronchitis. We observed higher odds of chronic bronchitis for those with lower education status (OR = 2.00, CI: 1.14–3.53) and those who were underweight (BMI < 18.5 kg/m2; OR = 2.35, CI: 1.22–4.53) or severely obese (BMI > 35 kg/m2; OR = 1.54, CI: 1.04–2.28), in models that included smoking (Table 5).
Increases in symptoms of chronic bronchitis have been demonstrated among workers with exposure to dusts (biologic and mineral dust), gas, and fumes. 35 –40 COPD and airflow obstruction are also associated with exposure to biologic and mineral dusts, gases, and fumes 41 as well as working in specific industries (i.e., rubber, plastic, leather, textile, food products manufacturing, health care, sales, construction, smelting, and agriculture). 42,43 We observed that individuals with chronic bronchitis symptoms had the highest odds of exposure to dusts and fumes compared with all other respiratory symptoms and conditions evaluated. Ever dust and/or fume and ever dust exposures had among the highest ORs with 2.03 (CI:1.44–2.87) and 2.13 (1.49–3.04), respectively. This suggests that workers continue to be exposed to dusts and fumes at concentrations or at frequencies that are negatively impacting their respiratory health. Future research should focus on further identifying specific jobs at risk for exposures and chronic bronchitis.
Emphysema
We found that the overall prevalence of doctor-diagnosed emphysema decreased only in males. Smoking is the primary risk factor for emphysema. Not surprisingly we observed a strong association between doctor-diagnosed emphysema and being a smoker or ex-smoker (ORs = 13.15 and 5.68, Table 5). The significantly reduced prevalence of doctor-diagnosed emphysema in males may be due to the significant reduction in smoking rates and mean pack-years. In addition, reduced prevalence of mild+ airflow obstruction was observed among those with emphysema, suggesting a reduction in disease severity.
Even though smoking is regarded as the major risk factor for emphysema, occupational risk factors have been identified. Emphysema, caused by inhalation of dust, especially among coal and gold miners, is well documented. 10,44 –49 Furthermore, tobacco smoking, when combined with vapors, gases, dusts, and/or fumes, has been shown to have, at a minimum, an additive effect when contributing to the development of COPD 38 and emphysema alone. 38,45 Consistent with the published literature, we observed significant increased odds for exposure to dusts and/or fumes among those with doctor-diagnosed emphysema (ORs range 1.72–1.93) when adjusting for smoking.
Asthma
Interestingly, we observed a decreasing prevalence of symptoms for wheezing but increasing prevalence of doctor-diagnosed asthma between the two survey periods. Significant decreases in wheezing were observed among almost every age category, among males, and among non-Hispanic Whites and Mexican Americans. Conversely, increases in doctor-diagnosed asthma were observed among every age category, among females, non-Hispanic Whites and Blacks. This inverse relationship suggests that potentially more asthmatic individuals are seeking care and being diagnosed and therefore are potentially receiving appropriate treatment to reduce their wheezing symptoms. The observed increased prevalence of doctor-diagnosed asthma could also be potentially influenced by the increase in awareness of asthma among healthcare professionals and their patients. 50 –52 However, due to the limited nature of the survey questions asked and because the questions changed slightly between the two survey periods, it is unclear what exactly is driving this inverse observation.
Individual factors may be contributing to the increased prevalence of doctor-diagnosed asthma. Obesity, considered BMI greater than 30 kg/m2, has been associated with an increased prevalence of asthma. 53 –55 We found that individuals from the 2007–2010 survey with asthma had an incrementally and significantly increased ORs for obesity (BMI of 30–34.9 kg/m2; OR = 1.63) and severe obesity (BMI > 35 kg/m2; OR = 2.04) compared to BMI 18.5–29.9 kg/m2. Therefore, the increase in prevalence of obesity we observed in the 2007–2010 survey is potentially contributing to the increased prevalence of doctor-diagnosed asthma during the same time period.
Increased asthma prevalence and symptoms of wheezing have previously been associated with occupational dust and gas exposure. 40,56,57 We observed occupational exposures to dusts and fumes to have an effect on the prevalence of doctor-diagnosed asthma with the most substantial exposure category being the aggregated ever dusts and/or fumes category (OR = 1.27; CI: 1.07–1.50). However, exposure to dusts and fumes had a more substantial effect on the prevalence of wheezing with the aggregated ever dusts and/or fumes category having the highest OR (OR = 1.88 CI: 1.55–2.28).
Strengths and limitations
NHANES is a comprehensive, nationally representative study, designed to assess the health status of the US population. Therefore, utilization of NHANES data for this study is a strength. This study is subject to several limitations. All information on survey participant’s symptoms and doctor-diagnosed respiratory diseases was self-reported and subject to recall bias and misclassification. Intensive efforts to increase awareness of COPD symptoms, diagnosis, and disease management were started in the 1990s. 58 This increased awareness may have affected diagnoses of COPD in the general US population and thus impacted prevalence estimates in our study. Furthermore, as mentioned previously, awareness of asthma also increased between the two survey periods which could have contributed to the increased prevalence of doctor-diagnosed asthma we observed. In the 2007–2010 survey, the phrase “and/or health professional” was added to questions that was previously asked about doctor-diagnosed conditions. It is possible that this addition may have changed how diagnosed conditions were reported by participants in the 2007–2010 survey. Occupational exposures were self-reported. Individuals may be more likely to recall exposures if they have respiratory symptoms or a doctor-diagnosed respiratory disease. Furthermore, the lack of associations between occupational exposures and airflow obstruction may be due to the healthy worker effect. Workers, in general, tend to be healthier, fitter, and have increased lung function compared to nonworkers in the same population. This is especially true for workers with occupational exposures to dust. 33,34
In conclusion, the results of this study provide an update on prevalence of chronic respiratory symptoms and doctor-diagnosed chronic lower airway diseases in the United States. The public health implications of this study are highlighted by the findings that from the 1988–1994 to the 2007–2010 survey period, prevalence of chronic bronchitis symptoms and doctor-diagnosed emphysema were generally stable, doctor-diagnosed chronic bronchitis and self-reported wheezing decreased and doctor-diagnosed asthma increased. Further evidence for the association between occupational dust and fume exposure and chronic lower airway diseases and symptoms is provided. This study demonstrates that COPD and asthma continue to be major public health problems and emphasizes individual and occupational risk factors that could be targeted in efforts to prevent and reduce the prevalence of chronic lower airway diseases.
Footnotes
Acknowledgments
The authors thank Gretchen White and Drs Kristin Cummings and Eileen Storey for providing helpful comments and critique of the manuscript and Dr Lu-Ann Beeckman-Wagner for overseeing training, data collection, and quality assurance of spirometry data.
Agency Disclaimer
The findings and conclusions of this report are those of the authors and do not necessarily represent the views of the United States Centers for Disease Control and Prevention National Institute for Occupational Safety and Health.
Authors’ Note
CH and EH conceived the study. CH, BD, and EH analyzed the data and interpreted the results. CH, BD, and EH wrote the manuscript. All authors have read and approved the final manuscript.
Funding
This work was performed by US Federal Government employees as part of their work; no non-governmental funding supported this work. The Centers for Disease Control and Prevention National Institute for Occupational Safety and Health supported the salaries of the authors.