
Abstract
A small percentage of asthmatics have ‘severe refractory asthma’, where there is suboptimal response to currently available therapies. A number of novel therapies targeting key biological targets are becoming available. Asthma is a heterogeneous disease, and systematic evaluation of patients is important to target therapies to the underlying inflammatory subtype and clinical features. This review article outlines new and emerging treatments for severe asthma, including monoclonal antibodies targeting eosinophilic disease, anti-neutrophil strategies, novel bronchodilators and bronchial thermoplasty. We highlight the importance of individualized investigation, treatment and management of severe asthmatics.
Keywords
Introduction
Asthma is a disease that is largely managed in primary care. The British Thoracic Society/Scottish Intercollegiate Guideline Network recommends therapy in a stepwise fashion from steps 1 to 5, increasing treatment until good asthma control is achieved. 1 ‘Severe refractory asthma’ is defined in patients with persistent symptoms, exacerbations and/or airflow obstruction, despite treatment at step 4 (i.e. high-dose inhaled steroids and trials of other treatments including long-acting β2 agonists, leucotriene receptor antagonists and oral theophylline) and includes asthmatics requiring maintenance systemic steroid therapy to maintain control (step 5). Severe refractory asthma accounts for 5%–10% of all asthmatics. 2 It is estimated that this group of patients use up to 50% of the health-care budget for asthma due to high medication requirements, hospitalizations and health-care utilization 3 and as such represent a major unmet need in terms of treatment options.
Patients with asthma who remain symptomatic despite optimum therapy should be assessed in a specialist severe asthma centre. 1 The current philosophy of these centres is to perform a systematic evaluation in all referred patients in order to accurately characterize the disease in each individual. 4
Assessment of treatment-resistant asthma
A thorough assessment of asthmatics who are symptomatic, despite conventional treatment, will determine whether they fall into one of the three following categories:
5
Potentially treatable asthma – this is asthma that should respond better to treatment, but there is a barrier preventing this, for example, continued smoking, continued avoidable allergen exposure or non-adherence to treatment. Asthma with co-morbidities, where there are other factors contributing to the patient’s overall symptoms, for example, dysfunctional breathing, chronic rhinosinusitis, nasal polyps, bronchiectasis, obesity-related breathlessness or airway obstruction, uncontrolled gastro-oesophageal reflux disease (GORD), vocal cord dysfunction or tracheo-bronchomalacia. Severe refractory asthma – this is asthma that is genuinely poorly responsive to standard guideline-based asthma therapy, in particular to the effects of steroids.
In the first two categories, the focus of treatment is education and treating co-morbidities. However, this review will focus on the third group (those with severe refractory asthma).
Asthma phenotyping and inflammation
Asthma is a chronic inflammatory disease of the lungs that is caused by abnormal inflammatory cells in the airways. 6 The inflammatory response occurs secondary to the body’s immune system encountering an allergen such as house dust, mite or grass pollen (allergic asthma) or other irritants, such as chemicals or cigarette smoke (non-allergic asthma). If this inflammation is uncontrolled over a long period of time, changes occur in the airway walls, leading to hypertrophy of airway smooth muscle, thickening of the basement membrane and narrowing of the airways. This leads to wheezing and coughing; classically, the airway narrowing is reversible in asthma. However, over many years and with increasing severity of disease, the airways can become stiff and fixed airflow obstruction can develop where there is no reversibility. 7 The mainstay of asthma treatment is controlling abnormal inflammation with drugs such as corticosteroids preferably prior to the onset of any fixed airway obstruction.
Traditionally, inflammation in asthma has been thought of as being characterized by the presence of eosinophils in the airways. Targeting airway eosinophils with steroid therapy has been shown to improve asthma control. 8 Certain inflammatory cytokines are important in the recruitment of eosinophils to the airway, for example, interleukin (IL)-4 and IL-5 (Figure 1) and these are attractive targets for drug development. However, it is now clear that many asthmatics, particularly those with severe or non-allergic disease, do not have eosinophils in the airways. 9,10 There may be different reasons for this, for example, past steroid use, smoking or recurrent infection, but in a subgroup, it may be that the neutrophil is the primary inflammatory cell. 11

In allergic asthma, Th2 lymphocytes release cytokines such as IL-4, -5 and -13 in response to allergens, resulting in the recruitment of eosinophils, mast cells and CD4+ lymphocytes into the airways. Non-allergic stimuli (e.g. cigarette smoke and viruses) activate Th1 lymphocytes via epithelial cells and dendritic cells. This results in production of IL-8 and IL-12 and recruitment of neutrophils, monocytes and CD8+ lymphocytes to the airway. In allergic asthma, the balance is tipped to a predominantly Th2 (eosinophilic) response and, in non-allergic asthma, to a Th1 (neutrophilic) response; the former being more responsive to the effects of steroids. Treatment strategies are being developed to target these specific pathways. IL: interleukin; Th: T helper cells.
The complex spectrum of asthma may be divided into subgroups or ‘phenotypes’ depending on either aetiology (cause), type of inflammation or clinical symptoms.
Stepwise asthma treatment is based on clinical features alone, but over the last 10 years, there has been a drive to personalize asthma treatment by targeting specific clinical/inflammatory phenotypes. There is no international consensus on how to divide asthma into these specific phenotypes, but recent work has focussed on ‘cluster analysis’, a method that groups people together with similar symptoms, signs and inflammatory features (Figure 2). 12,13 This method is useful to guide treatment according to how proportional symptoms are to the degree of airway inflammation. However, it is limited, in that specific aetiological factors will not be identified, for example, a patient can be put into the category of ‘allergic asthma’ but it will not be clear whether the allergy is to environmental, occupational or food allergens. Therefore, careful clinical assessment by an experienced asthma physician is required in conjunction with measurement of airway inflammation, physiology, radiology, immunology and clinical characteristics (presence of mucous/recurrent infection (Table 1). In addition to assessment of disease, markers of co-morbidity are actively sought, for example, obesity, reflux, nasal disease, vocal cord dysfunction, hyperventilation, osteoporosis, steroid-induced diabetes and sleep apnoea syndrome.
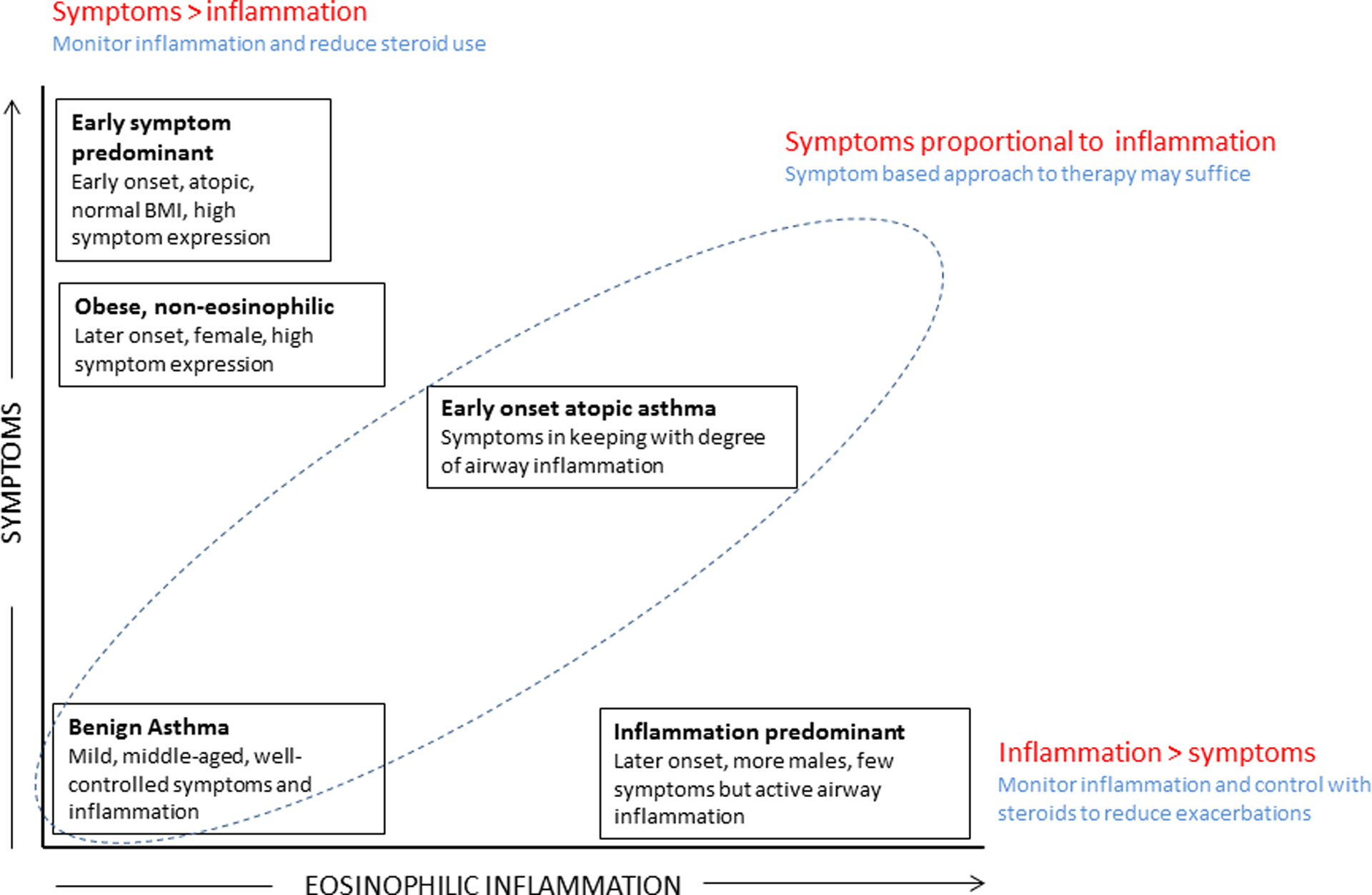
Clinical phenotypes of asthma identified by cluster analysis, adapted from Haldar et al. 12 Clusters are plotted and divided into three categories (red) based on how proportional symptoms are to airway inflammation. Treatment strategies are suggested based on levels of concordance (blue).
Investigations performed in detailed assessment of patients with severe asthma.

IgE: immunoglobulin E; CXR: chest X-ray; HRCT: high-resolution computed tomography; DEXA: dual-energy X-ray absorptiometry.
Steroid-related side effects
A key challenge for patients with steps 4 and 5 asthma and their physicians is minimization of oral corticosteroid (OCS) use and side effects. The change in body shape associated with OCS use can, in some, bring feelings of self-loathing and loss of self-worth and may, ultimately, lead to depression and isolation. 14
The prevalence of co-morbid conditions attributed to OCS increases with the frequency of use. In the recently published UK severe asthma registry of patients attending national severe asthma centres, the prevalence of common OCS-related conditions was high compared with patients having moderate asthma. For example, prevalence of GORD was 41% in the UK severe asthma population compared with 9% in the general population, and obesity (body mass index >28) was 40% in patients in the severe asthma registry study, but it is between 24% and 30% in the general population. 15
The comparative prevalence of other co-morbid conditions (such as diabetes, osteoporosis, steroid-related eye disease, hypertension, etc.) is much harder to confirm and depends on diagnostic criteria used in severe asthma studies compared with those used in general population studies.
Existing approaches used at or beyond step 5
Existing therapies, available beyond step 5 asthma, include Omalizumab, which is used for a specific sub-group of allergic patients who meet the National Institute for Clinical Excellence (NICE) guidelines criteria. 16 This is an example of a therapy that has emerged from research over the last 10 years to change the management for a small proportion (estimated between 10% and 15%) 17 of all patients with severe asthma. Recent real-life studies, both in the UK and internationally, have demonstrated that, in clinical practice, the observed benefits and response rates (approximately 70%) are higher than was experienced during clinical trials. 18
Bronchial thermoplasty has also recently received a licence for treatment. Clinical trials have shown improvements in health status, exacerbations, Accident and Emergency (A&E) attendances and hospital admissions, 19 as well as direct cost savings because of reduced exacerbation rates. Data also shows reduced days off work and school, which has significant economic cost saving implications that are not considered in the current NICE appraisal. 20 The same may be true for Omalizumab, but data are sparse.
For patients dependent on OCS not suitable for Omalizumab or bronchial thermoplasty, old-fashioned immune suppressive treatments are occasionally used, such as methotrexate, azathioprine, ciclosporin, mycophenolate, gold and, sulphasalazine as steroid-sparing agents. In the recent American Thoracic Society (ATS)/European Respiratory Society (ERS) guideline on the management of severe asthma, 21 these therapies were classified as ‘do not use’, as there are insufficient data to support beneficial effects. Small studies have suggested a modest steroid-sparing benefit. 22,23 UK severe asthma centres will still use these treatments if all other treatments have been exhausted and patients remain desperate to withdraw or reduce OCS. 4 Further research is needed on the benefits versus risks in severe asthma.
Anti-fungal therapy
A single placebo-controlled trial has supported the use of itraconazole in patients with severe asthma with fungal allergy. 24 The magnitude of the response in this study was high with an Asthma Quality of Life Questionnaire (AQLQ) benefit over placebo of 0.8, which is higher than any individual treatment in asthma. A more recent placebo-controlled trial of voriconazole did not match the findings with itraconazole. 25 The duration of the voriconazole study may have been too short at 3 months, as the itraconazole study by Denning et al. 24 demonstrated no response at two months, but clinically and statistically meaningful benefits at 4 months.
Anti-neutrophil therapies
Evidence for the use of macrolides in asthma has been conflicting 26 ; however, there is some emerging evidence of a possible benefit in neutrophilic asthma. A study in 45 severe refractory asthmatics showed that two months of treatment with clarithromycin 500 mg twice daily reduced airway neutrophils with improvement in AQLQ scores; the effect was greater in a subgroup of patients with non-eosinophilic asthma. 27 A recent randomized control trial of azithromycin as an add-on therapy for 6 months in exacerbation-prone severe asthma showed that the rate of severe exacerbations reduced in non-eosinophilic asthma. 28 The recent ERS/ATS guidelines on severe asthma do not recommend the routine use of azithromycin for severe asthma. 21 In specialist centres, however, it is considered as a treatment in patients with a history of recurrent culture-proven chest infections, especially those with concomitant bronchiectasis or immune deficiency.
New small molecule inhibitors aimed at targeting neutrophilic inflammation are under development. Direct inhibition of airway neutrophils via blockade of the chemokine receptor CXCR2 reduced sputum neutrophils and demonstrated small improvements in asthma control and non-severe exacerbations. 29 Anti-IL-17 is important in promoting neutrophilic inflammation. A clinical trial has shown that Brodalumab, a human anti-IL-17 receptor monoclonal antibody, is safe in moderate to severe asthma, but, overall, no treatment effect was observed. 30 A possible improvement in asthma control was seen in a predefined subgroup with highly reversible airways disease warranting further study.
Mucolytics
There is no current evidence to support the use of mucolytics in asthma per se. However, studies have shown a benefit of using hypertonic saline and oral mucolytics (cisteines) in bronchiectasis. 31 –33 A very small clinical trial showed benefit from mannitol inhalation in mucocilliary clearance in asthmatics. 34 Bearing in mind the high prevalence of bronchiectasis observed in patients with severe asthma (33%; Menzies et al. 4 ), these therapies may have a role in patients with severe asthma with bronchiectasis; this merits further research.
Anti-TNF α
Tumour necrosis factor α (TNF–α) promotes airways inflammation, and its levels are raised in many chronic inflammatory diseases including severe asthma. 35 However, whilst early small trials of therapy with anti-TNF-α in refractory asthma suggested possible benefits, 36,37 subsequent larger randomized controlled trials failed to show clear benefits whilst raising serious concerns regarding toxicity that have discouraged further study. 38,39
PDE-4 inhibitors
Phosphodiesterase 4 (PDE-4) is a pro-inflammatory enzyme; hence, its inhibition could potentially reduce airways inflammation. Roflumilast is a PDE-4 inhibitor that has been shown to have anti-inflammatory effects in asthma 40 and, subsequently, to improve lung function at high dose, at least, in mild to moderate asthmatics. 41 Its use has not yet been investigated in severe refractory asthma, but possible benefits in patients with COPD with frequent exacerbations 42 may lead to further studies in this group.
New and emerging therapies for severe asthma
Monoclonal antibodies
Anti-IL-5
A small proportion of patients with severe allergic asthma have persistently raised eosinophils levels in the sputum and blood, despite adequate treatment with corticosteroids after accounting for patient adherence to treatment. 43,44 IL-5, a cytokine that promotes eosinophil production and trafficking into the lungs, 45 has been identified as a potential anti-inflammatory target in allergic asthma. Mepolizumab, a monoclonal antibody against IL-5, significantly reduced exacerbation rates and improved quality of life in patients with severe refractory eosinophilic asthma. 46,47 This was associated with a reduction in sputum and blood eosinophils but did not improve symptoms, forced expiratory volume in 1 second (FEV1) or airway hyperresponsiveness.
Resilizumab, another anti-IL-5 monoclonal antibody, reduced sputum eosinophil levels and lung function with a non-significant trend towards reduced exacerbations in a placebo-controlled trial of poorly controlled asthmatics with eosinophilic inflammation. 48
Benralizumab is a novel agent that binds to the IL-5 receptor. A recent phase II study showed a reduction in exacerbations and improvement in lung function and asthma control in moderate to severe asthmatics with raised blood eosinophil counts. 49
These are promising new treatments for a highly selected group of severe asthmatics, with predominantly eosinophilic disease and multiple exacerbations. Larger multi-centre trials of treatment with anti-IL-5 agents are ongoing.
Anti IL-4 and IL-13
IL-4 and IL-13 are cytokines that drive allergic inflammation, and both share a common receptor. 50,51 IL-13 concentrations are increased in the airways of patients with asthma. 52 Various approaches to inhibiting IL-13 and/or IL-4 have been developed:
specific monoclonal antibodies against the individual cytokines (e.g. tralokinumab and lebrikizumab against IL-13);
soluble cytokine receptors that ‘mop up’ individual cytokines (e.g. altrakincept against IL-4); or
IL-4Rα blockade, which targets the common IL-13 and IL-4 receptor and inhibits binding of both cytokines (e.g. pitrakinra and dupilumab).
IL-13 monoclonal antibodies have shown a good safety profile in asthmatics. 53,54 A study of lebrikizumab in 219 poorly controlled asthmatics showed a significant improvement in FEV1, particularly in patients with high serum periostin levels (a biomarker of eosinophilic inflammation). As per the anti-IL-5 antibody mepolizumab, this agent only demonstrated clinical effectiveness when the population was stratified for their eosinophilic pattern of airway inflammation. 55 Pitrakinra reduced allergen-induced late asthmatic responses and the need for rescue medication with minimal side effects. 56 Dupilumab has recently been demonstrated to have an effect in preventing exacerbations and treatment failure in a novel study design when inhaled steroid treatment was actively withdrawn to induce early exacerbations. 57 A number of phase II trials in anti-IL-4 and IL-13 drugs are ongoing in severe asthma, the results of which are eagerly anticipated.
Bronchodilators
Long-acting muscarinic antagonists have attracted attention as potential novel therapy in asthma, as they have several potentially beneficial effects that are complementary to standard inhaled therapy, such as bronchodilation, inhibition of mucus secretion and reduction in hyperinflation. 58 They have been shown to reduce exacerbation frequency and slow lung function decline in COPD; therefore, current research is investigating whether these benefits may also be seen in asthma. 59 Peters et al. 60 showed that the addition of tiotropium to inhaled corticosteroids (ICS) resulted in a superior outcome to doubling ICS dose and was similar to adding salmeterol, as assessed by morning peak flow measurements. Kerstjens et al. 61 subsequently reported the results of two identical trials, showing a small bronchodilator effect and a 21% reduction in severe exacerbations in symptomatic asthmatics with persistent airflow obstruction when added to step 3/4 therapy. A recent systematic review concluded that tiotropium may have a beneficial role in moderate to severe asthma that remains uncontrolled despite ICS and long-acting beta-agonists; no safety concerns were raised. 62
A recent clinical trial investigating the addition of vilanterol, a novel ultra-long-acting β-agonist, to ICS showed a reduction in risk of severe exacerbations and improved lung function in uncontrolled asthmatics compared with ICS alone. 63 A number of other bronchodilators are in development for both asthma and COPD. 64
Bronchial thermoplasty
Bronchial thermoplasty, as mentioned above, is a novel therapy that targets airway smooth muscle. Therapy involves three protracted bronchoscopy procedures, and patients are at risk of exacerbations of asthma immediately thereafter (for one week in most cases, but up to 4 weeks post-procedure overall). During the treatment, thermal energy is applied to all accessible airways. Current studies have suggested that the procedure removes up to 50% of smooth muscle mass from the bronchial tree. Clinical benefits witnessed in a sham-controlled trial included not only AQLQ improvement (primary endpoint) but also large improvement in exacerbation frequency, A&E attendances and hospital admissions, which, in open-label follow-up, persisted for up to five years. 19,65,66 In all the clinical trials published to date, there have been no long-term sequelae of airway strictures or bronchiectasis as originally feared.
The major issue with this treatment, to date, is the lack of knowledge or certainty regarding its true mechanism of action and patient population best served. As such, all patients undergoing therapy should be enrolled in long-term data collection ‘studies’ or ‘registries’ to improved understanding and knowledge.
Future targets
Many inflammatory pathways have been identified as potential targets in asthma. A new inhaled dual PD-3 and PD-4 inhibitor has undergone phase 1 trials, including in mild asthmatics, showing a good safety and efficacy profile. 67 There is a large body of work ongoing, identifying small molecules that are important in the transcription of inflammatory genes, such as p38 mitogen-activated protein kinase and nuclear factor-κB, as potential novel targets for drugs. 68,69 Drugs that act on these pathways are in the early stages of development and have not yet reached phase I trials.
Because of the side effects of steroids, there has been an interest in the development of ‘dissociated glucocorticoids’. These are drugs that can suppress inflammation but theoretically have a reduced side effect profile because of a different mechanism of interaction with genes. However, separating desired from undesired effects has been challenging for scientists. 70 A randomized controlled clinical trial of inhaled GW870086, a novel selective glucocorticoid, in mild–moderate asthmatics disappointingly showed no effect on lung function or rescue medication use. 71
Conclusion
In conclusion, we are currently in an exciting era in the field of severe asthma. A large national collaboration of data collection in the UK (The Severe Asthma Registry) and international research programmes are developing our understanding of individual patterns of disease. Linking real-life studies, detailed phenotyping and genetics will aid us in tailoring treatments in patients with asthma. Many new treatments are on the horizon, which will help make personalized asthma a reality. The ultimate goal is the almost complete elimination of the dependence on OCS. This will be critical to a small percentage of asthmatics that represent a population with a huge unmet need in the UK.
Footnotes
Funding
The authors have received the following support from the pharmaceutical industry of relevance to this article: BK has received lecture fees from Astrazeneca and Novartis. SJF has research grant support from AstraZeneca and GlaxoSmithKline (GSK); lecture fees from GSK and Novartis; scientific advisory board participation fees from GSK, Boehringer Ingelheim and Novartis and conference attendance support from GSK, Boehringer Ingelheim and Novartis. RMN has received lecture fees and conference attendance support from GSK, Chiesi, Boston Scientific and Novartis.