
Abstract
Previous studies have shown that vitamin D has beneficial effects on respiratory health. The role of inflammation as a possible mediator between vitamin D and respiratory health is not well understood. We used National Health and Nutrition Examination Survey 2001–2006 data (unweighted N = 12,856) to examine the mediating effects of biomarkers of inflammation on associations between vitamin D and respiratory health. Vitamin D was measured by serum 25 hydroxy vitamin D test. Respiratory health was measured by self-reported respiratory symptoms and chronic obstructive pulmonary disease (COPD). Biomarkers included C-reactive protein (CRP), alkaline phosphatase (AP), and five leukocyte measures. Models controlled for season, age, sex, race/ethnicity, body mass index, and current and former smoking. Lower levels of vitamin D were significantly associated with respiratory symptoms (linear trend p < 0.01) and with COPD (linear trend p < 0.0002) after adjusting for covariates. Adding biomarkers to the models to test for mediation, the vitamin D effect on respiratory health was not a consequence of any single marker but was partially attenuated as a combined result of leukocytes, AP, and CRP. Vitamin D is beneficial to improve respiratory health. Its benefits do not appear to be mediated by any single biomarker examined in this study; rather, benefits of vitamin D may act broadly through multiple mediating mechanisms.
Introduction
Vitamin D is essential for bone mineralization and calcium homeostasis. Evidence more recently has established that vitamin D has beneficial effects on immune function and control of inflammation 1,2 and that it is related to lower risks of cancer, diabetes, cardiovascular disease, and infectious disease. 3 –5 The benefits of vitamin D extend to improve respiratory health as well. 6 –8 For example, vitamin D has been found to correlate inversely with inflammatory forms of respiratory disease. 9,10 Black and Scragg 7 analyzed National Health and Nutrition Examination Survey (NHANES) 1988–1994 data and found significant associations between vitamin D and spirometry measures of lung function. In a controlled trial, Laaksi et al. 11 found that vitamin D supplementation was effective in prevention of acute respiratory tract infection in a sample of healthy men.
The specific mechanisms by which vitamin D supports respiratory health are unclear. One explanation for the respiratory health benefits of vitamin D is found in its anti-inflammatory properties. 2,12 –16 Vitamin D is thought to regulate many cellular processes including immunomodulating the activity of monocytes, macrophages, lymphocytes, and epithelial cells. 10 Both acute and chronic forms of respiratory disease occur in conjunction with inflammation. 17 –19 In an analysis of NHANES III data, Mannino et al. 20 found higher levels of C-reactive protein (CRP) and fibrinogen in persons with restrictive or obstructive lung disease.
There is evidence to support each of the three hypothesized links. Studies have found associations between (A) vitamin D and respiratory health, 7,13 (B) vitamin D and various biomarkers of inflammation, 15,16,21,22 and (C) biomarkers and respiratory health. 20 However, a direct test of the mediating role of inflammatory biomarkers in the vitamin D–respiratory health link within a single study has not been undertaken. There have been recent calls for research to understand how the relationship between vitamin D and respiratory health may be mediated through systemic inflammation. 23,24 The purposes of this study were to test for relationships between vitamin D and respiratory health using recent survey years from the NHANES and to determine whether there was evidence that the effect of vitamin D on respiratory health may be mediated through a set of tested biomarkers.
Methods
Design
The study was a cross-sectional analysis of NHANES data. 25 We included three survey periods conducted over 6 years (2001–2002, 2003–2004, and 2005–2006). Each sampling period included different persons, and each person was measured on all variables at one time observation. These years were selected because they are the most recent years in which the vitamin D status has been assessed in the NHANES. Variables from the laboratory, examination, demographic, and questionnaire data were combined for analysis. Pregnant women and persons less than 20 years of age were excluded.
Dependent variables
The primary dependent variables of interest were self-report measures of respiratory symptoms and chronic respiratory disease. Participants were asked if they had ever been told by a doctor or health-care professional that they had emphysema or chronic bronchitis; these two conditions were combined to form a dichotomous measure of the presence or absence of chronic obstructive pulmonary disease (COPD).
Symptoms of respiratory illness included eight items regarding cough and wheezing. All participants were asked two questions, whether or not they had experienced a dry cough at night in the past year and whether or not they had experienced wheezing or whistling in the chest during the past year. Participants who said yes to the wheezing question were asked follow-up questions regarding the number of such attacks in the last year (dichotomized for this study into one versus more than one) and whether the wheezing episodes resulted in medical attention, chest sounds, sleep disturbance, medications being prescribed, or activity limitations. Participants received a score from 0 to 8 based on the number of symptoms; this distribution was positively skewed and was dichotomized into persons who reported 0 to 2 symptoms versus persons who reported more than 2 symptoms.
Independent variables and mediators
The primary independent variable of interest was vitamin D measured by serum 25 hydroxy vitamin D (25(OH)D) test in nanomoles per liter. The vitamin D distribution was divided into quintiles consistent with a previous NHANES study of vitamin D and lung function. 7
Seven blood biomarkers were included based on their availability from the same persons as the data on vitamin D and respiratory symptoms. Markers included CRP (milligrams per deciliter), alkaline phosphatase (AP; units per liter), and five leukocytes measured as 1000 cells/µL including basophils, lymphocytes, monocytes, eosinophils, and segmented neutrophils. The distributions of biomarkers were examined and were found to be positively skewed; we converted all biomarkers to natural log values for analysis.
Covariates
We included covariates to control for possible confounding influences on the relationships among variables. Covariates included season, sex, age, race/ethnicity, smoking, and overweight and obesity. Season was recorded as fall–winter (November 1 through April 30) or spring–summer (May 1 through October 31) according to the time when the laboratory samples were obtained. Age in years was categorized into ages 20–39 (used as the referent), 40–59, and 60 and over. Race/ethnicity was categorized into non-Hispanic White (used as the referent), non-Hispanic Black, and other. Smoking was categorized into lifetime never smokers (used as the referent), former smokers, and current smokers. Body mass index (BMI) was used to distinguish participants who were normal weight (BMI < 25; used as the referent), overweight (25–29.9), and obese (30 and over.)
Analysis
We conducted an analysis based on Baron and Kenny 26 guidelines to determine whether associations between vitamin D and respiratory health may be mediated by the biomarkers in the study. Evidence for mediation is observed in multiple regression analysis if a significant vitamin D–respiratory outcome coefficient becomes nonsignificant when a significant biomarker–respiratory outcome coefficient is added to the model. Partial mediation could occur if the vitamin D effect remained significant but the magnitude of the effect was reduced. In the mediation models, we first examined the effect of biomarkers individually and then examined whether there was evidence for mediation when biomarkers were combined.
Data were analyzed using SAS software version 9.3. The procedures ‘surveyreg’ and ‘surveylogistic’ were used depending on the response variable scale. Strata and cluster variables as provided in the NHANES data were used to account for the sampling design, and the data were weighted according to NHANES guidelines. 27
Results
A descriptive summary of unweighted study variables is provided in Table 1. The total N was 12,856; missing values reduced available sample sizes by less than 1%. COPD was reported by 7.4% of the sample and three or more respiratory symptoms by 11.7%. The mean value for vitamin D was 58.5 nmol/L (SD = 22.4); the values that approximated a quintile split are shown in Table 1.
Summary of unweighted (N = 12,856) study variable descriptive statistics.
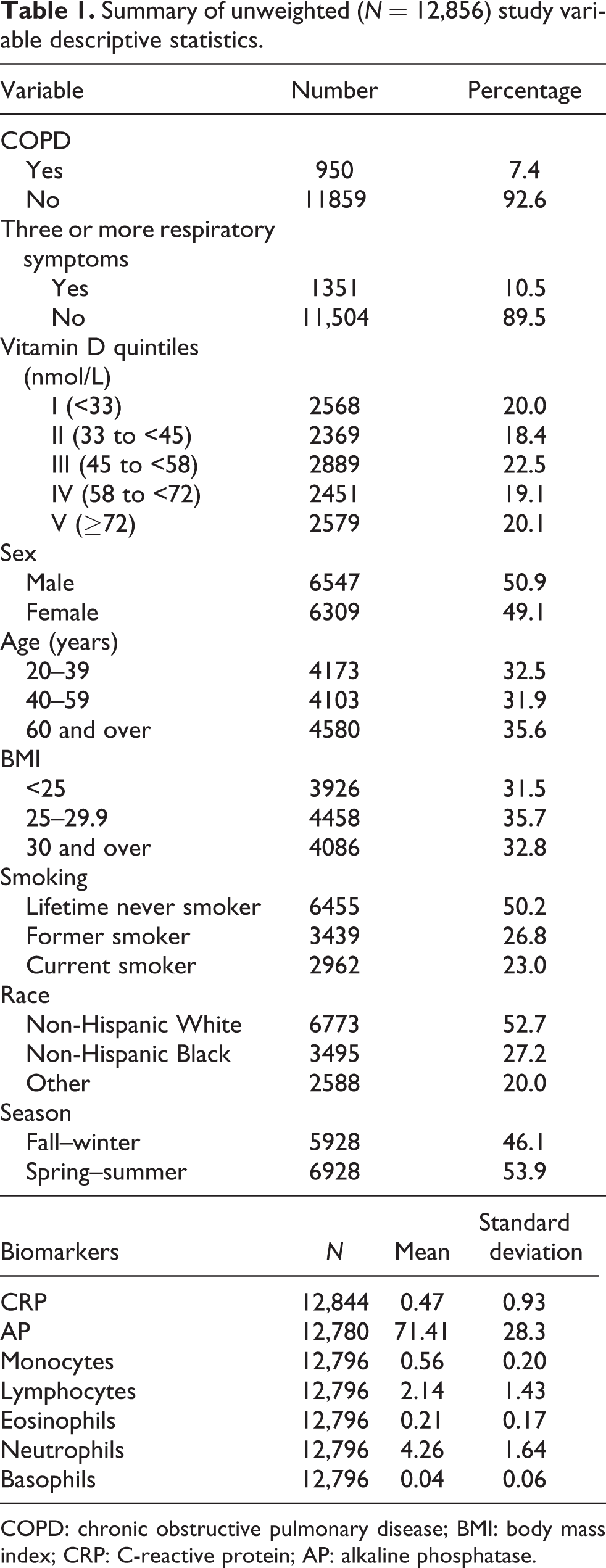
COPD: chronic obstructive pulmonary disease; BMI: body mass index; CRP: C-reactive protein; AP: alkaline phosphatase.
Bivariate correlations between the markers of inflammation and oxidative stress were examined. The highest correlation was r = 0.38 between monocyte and neutrophil counts; monocytes and lymphocytes were correlated at r = 0.32. Other correlations were smaller. We interpreted these correlations to mean that multicollinearity was not a serious concern and we therefore included multiple markers as separate independent variables in final models.
The relationships between respiratory health measures as the dependent variables and vitamin D as the primary independent variable are summarized in Table 2. Lower levels of vitamin D were significantly associated with respiratory symptoms (p < 0.01) and with COPD (p < 0.0002). The effects were strongest for the lower vitamin D quintiles.
ORs, 95% CIs, and p values for linear trends testing the associations between vitamin D and respiratory health measures.a
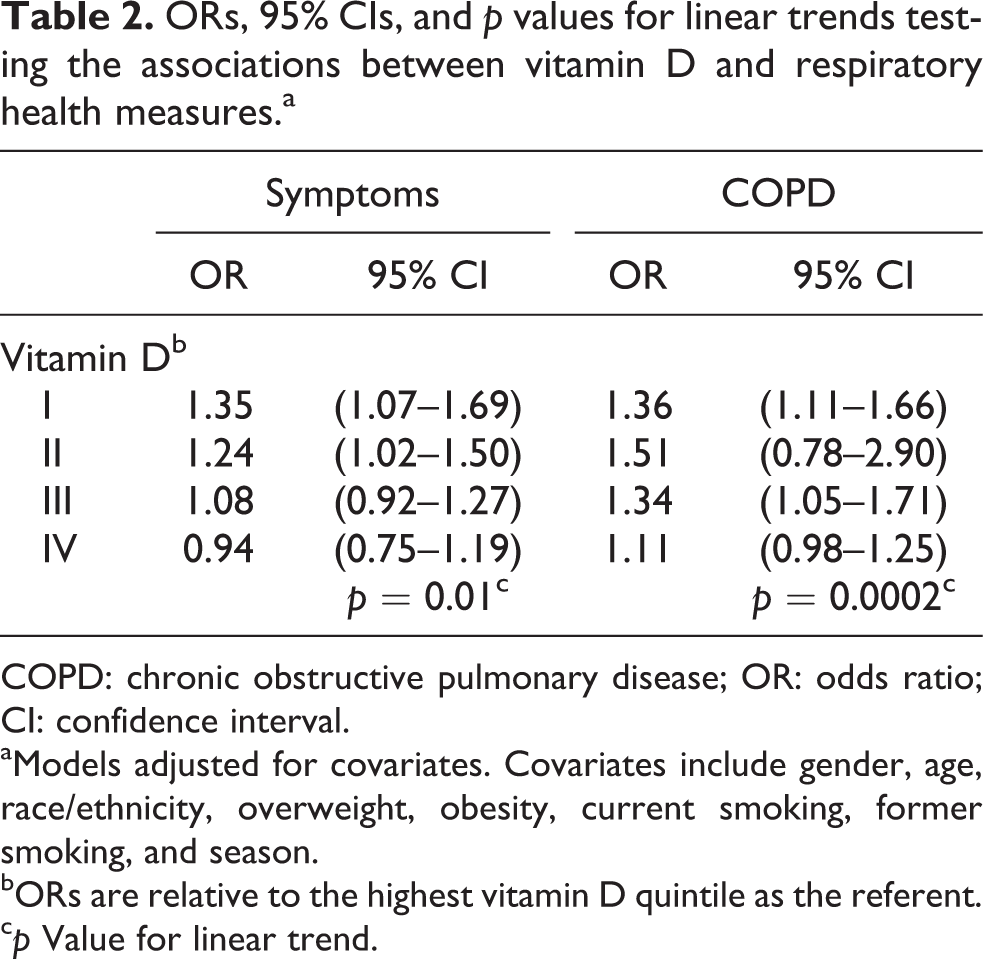
COPD: chronic obstructive pulmonary disease; OR: odds ratio; CI: confidence interval.
aModels adjusted for covariates. Covariates include gender, age, race/ethnicity, overweight, obesity, current smoking, former smoking, and season.
bORs are relative to the highest vitamin D quintile as the referent.
c p Value for linear trend.
Table 3 confirms that most tested biomarkers were significantly associated with respiratory measures. Two of the leukocytes, basophils and lymphocytes, were not related to the measures of respiratory health and so, per Baron and Kenny 26 guidelines, were not used in the mediation analysis. All remaining biomarkers were significantly related to vitamin D level (data not shown).
ORs, 95% CIs, and p values for linear trends, testing the associations between biomarkers, respiratory symptoms, and COPD. Models adjusted for covariates.a

COPD: chronic obstructive pulmonary disease; OR: odd ratio; CI: confidence interval; CRP: C-reactive protein; AP: alkaline phosphatase.
aCovariates include gender, age, race/ethnicity, overweight, obesity, current smoking, former smoking, and season.
Tables 4 and 5 show the final mediation analysis results for respiratory symptoms and COPD, respectively. The top lines of each table show the vitamin D effect before adding biomarkers; this is copied from Table 2 but is repeated for ease of comparison. The next lines show the odds ratios (ORs) and linear trends for vitamin D when it was included in the models with each of the five biomarkers individually. The findings indicated little difference between the significant vitamin D effects before adding the biomarkers and the effects when adding each marker individually; vitamin D ORs remained almost identical. There was some evidence for a partial mediating effect through AP for both respiratory symptoms and COPD.
ORs, 95% CIs, and p values for linear trends testing the associations between vitamin D and respiratory symptoms before and after inclusion of biomarkers.a

CI: confidence interval; OR: odds ratio; CRP: C-reactive protein; AP: alkaline phosphatase.
aModels adjusted for covariates. Covariates include gender, age, race/ethnicity, overweight, obesity, current smoking, former smoking, and season.
bORs are relative to the highest vitamin D quintile as the referent.
Odds ratios, 95% CIs, and p values for linear trends testing the associations between vitamin D and COPD before and after inclusion of biomarkers.a

COPD: chronic obstructive pulmonary disease; CI: confidence interval; CRP: C-reactive protein; AP: alkaline phosphatase; OR: odds ratio.
aModels adjusted for covariates. Covariates include gender, age, race/ethnicity, overweight, obesity, current smoking, former smoking, and season.
bORs are relative to the highest vitamin D quintile as the referent.
The last model results in Tables 4 and 5 show the vitamin D ORs when adding all five markers simultaneously. In each of these final models (one for respiratory symptoms and one for COPD), the vitamin D effect appeared to be partially attenuated. The ORs were altered in particular for vitamin D levels at the lowest quintiles. For respiratory symptoms, the p values for the linear trends for the vitamin D effects changed from p = 0.01 without biomarkers to p = 0.07 with combined biomarkers. For COPD, the corresponding change in the linear trend was from p = 0.0002 without biomarkers to p = 0.03 with combined biomarkers. Although not shown in the table, the biomarkers in the final model with the strongest associations to COPD were CRP and AP; the biomarkers with the strongest associations to respiratory symptoms were CRP, AP, and eosinophil count.
Discussion
The results of this study add to the research evidence that vitamin D is correlated to better respiratory health. We observed significant linear trends from the highest to the lowest quintile levels between vitamin D and increased risk for reported COPD and respiratory symptoms.
Results of the mediation analysis suggest that the apparent respiratory benefits of vitamin D occur broadly and at best could be partially mediated through anti-inflammatory mechanisms that are expressed through leukocyte counts, CRP, and AP. Any one indicator could not account for the benefits of vitamin D, but combined, they appeared to partially mediate the vitamin D–respiratory health relationships. Even with this partial mediation, the benefits of vitamin D appeared to be broader than those that we could capture with the biomarkers under study.
AP is an enzyme that dephosphorylates endotoxins and counters pro-inflammatory responses. It has been proposed as a possible therapeutic agent for such conditions as sepsis, acute kidney injury, or brain injury. 28 –30 It has also been examined as a diagnostic tool for pulmonary tuberculosis 31 and as a marker of fibrosis in chronic interstitial lung disorders. 17 Our evidence suggests that AP is elevated in persons who report more frequent respiratory symptoms or COPD and that vitamin D may operate to help control serum levels of this enzyme.
CRP is a pro-inflammatory cytokine. It is synthesized primarily in the liver and kidney in response to interleukins and other agents and can increase rapidly in concentration in the blood after infection or inflammation. 32 CRP plays a powerful and broad role in anti-inflammatory, anti-infection, and immune responses in a wide variety of disease states. CRP may also be produced at lower levels in response to ongoing chronic conditions including subclinical inflammation. 32 Some studies have suggested that exposure to particulate matter air pollution causes increases in CRP, which lends support to its potential role as a marker in respiratory disease. 33,34
It appears, however, that vitamin D may impact measures of respiratory health through control of systemic inflammation broadly, or possibly through other mechanisms, rather than through these specific markers as isolated paths. It is an oversimplification to attempt to treat inflammatory markers as though they acted independently of each other. Leukocytes and CRP, for example, are interdependent. 32
Our findings are limited by the particular biomarkers that were available for study. The NHANES data did not include measures of some markers that have been found to be related to vitamin D levels in prior research, particularly the cytokine tumor necrosis factor α (TNF-α) and interleukins (ILs) such as IL-1 and IL-6.
Other limitations of the study concern the cross-sectional design, the self-report nature of the outcome data, and the limited covariate data included in the analysis. The cross-sectional design restricts the ability to test for temporal relationships between vitamin D, biomarker response, and subsequent occurrence of symptoms and disease. This may be especially limiting when considering that self-reported COPD diagnosis took place prior to NHANES data collection, and respiratory symptoms were asked for occurrence within the previous year. However, the fact that we observed significant associations between vitamin D and these respiratory measures, and between many biomarkers and the respiratory measures, makes it plausible to examine whether there may be evidence for mediation. Nevertheless, we cannot exclude the possibility of reverse causation. Independent assessments of lung function such as through spirometry were not available during the 2001–2006 period when vitamin D was assessed. Respiratory symptom self-report measures were restricted to the eight available items. Measures of respiratory symptoms may represent persons with a variety of respiratory diseases such as COPD, asthma, or other clinical or subclinical lung disorders. For example, the relationships observed between vitamin D, eosinophils, and respiratory symptoms may reflect effects for persons with asthma. Measures of dietary variables or medications that might influence vitamin D levels, mediators, or outcome measures were not included; medications, for example, that work to improve respiratory symptoms may obscure the impacts of vitamin D, or diets high in anti-inflammatory properties may affect measures of biomarkers independently of vitamin D.
Further research is necessary to better understand how vitamin D exerts beneficial effects on respiratory health. The broad physiological importance of vitamin D to autoimmune, infectious, and inflammatory processes across multiple organ systems is increasingly recognized but, as yet, incompletely understood. Although this study did not isolate single biomarkers that might account for links between vitamin D and respiratory health, it would perhaps have been more surprising had we found such evidence, and instead, the results are perhaps more properly reflective of the broader roles that vitamin D plays in maintaining optimal health through its impact on multiple processes.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.