
Abstract
Chronic obstructive pulmonary disease (COPD) is a multisystem disease. Established comorbidities include cardiovascular disease, osteoporosis, loss of muscle mass and function, depression, and impaired quality of life. The natural history is not well understood. The Assessment of Risk in Chronic Airways Disease Evaluation (ARCADE) is a longitudinal study of comorbidities in COPD. The primary aims are to delineate the progression and interrelationships of cardiovascular disease and associated comorbidities. Each year ARCADE aims to recruit 250 patients diagnosed with COPD and 50 comparators (free from respiratory disease). Assessments include spirometry, body composition, blood pressure, aortic stiffness (pulse wave velocity (PWV)), noninvasive measures of cardiac output, systemic inflammatory mediators, blood and urine biochemistry, and physical and health outcomes. These will be repeated at 2 and 5 years. In the first year of recruitment, 350 patients and 100 comparators were recruited. The reproducibility of aortic PWV, cardiac output, stroke volume, and cardiac index was evaluated and accepted in 30 patients free from overt cardiovascular disease. The preliminary data from ARCADE have demonstrated acceptable reproducibility of hemodynamic outcome measures. Further longitudinal data collection will increase knowledge of the progression and interactions between cardiovascular risk factors and other comorbidities in COPD.
Introduction
Unlike other common chronic diseases in the United Kingdom, the prevalence of chronic obstructive pulmonary disease (COPD) has not declined, 1 and by 2020 it is estimated to become the third leading cause of mortality worldwide. 2 Smoking remains the major cause of COPD, leading to an accelerated age-related decline in lung function and loss of exercise capacity. However, COPD is a multisystem disorder with important extra-pulmonary comorbidities and associated clinical consequences such as increased cardiovascular (CV) risk, loss of skeletal muscle mass and function, osteoporosis, insulin resistance, and diabetes mellitus. 3 –7 The underlying mechanism(s) and evolution of comorbidities remain unclear, as most studies have been small and cross-sectional in design. However, potential causative factors include the nonrespiratory effects of smoking, continuous systemic inflammation, loss of physical capacity, and disease-related adaptations in lifestyle.
The Assessment of Risk in Chronic Airways Disease Evaluation (ARCADE) study will focus on CV risk and outcomes in COPD. CV disease is a major cause of mortality, accounting for 30–50% of the deaths in COPD, independent of cigarette smoking status. 8 It has been suggested that premature vascular aging causes increased arterial stiffness, which is a factor in the CV disease in COPD. 9 In the general population, increased aortic stiffness is an independent risk factor for CV disease and is inversely related to a decline in the forced expiratory volume in 1 second (FEV1). 10,11 Increased aortic stiffness disturbs physiological ventricular–vascular coupling causing an increase in mid to late central systolic pressure and left ventricular afterload, which increases myocardial oxygen demand, while reducing diastolic pressure augmentation of myocardial perfusion. This ischemia leads to progressive myocardial fibrosis, ventricular stiffening, and left ventricular diastolic failure, which are observed even in mild severity airflow obstruction in COPD. 12 Aortic pulse wave velocity (PWV) is the accepted “gold standard” measure of aortic stiffness, which is increased in COPD, 9 though no measure of arterial stiffness has been validated as a prognostic predictor of CV risk in COPD as studies so far have only been cross-sectional.
A number of other comorbidities may be related to CV risk in COPD. Cross-sectional studies have demonstrated near continuous systemic inflammation, increased insulin resistance, risk of developing diabetes mellitus, 4,7 a low fat-free mass (FFM) and bone mineral density are related to aortic stiffness in COPD. 9 A unifying hypothesis for the development of comorbidities in COPD is that similar deficits in physiological systems are seen in natural aging, where they are considered to represent degenerative changes with time, and that COPD causes premature aging or is itself an outcome of a predisposition to premature aging.
As a large longitudinal study, ARCADE will extend earlier cross-sectional findings and increase knowledge of the rate of central arterial stiffening and its interaction with other CV risk factors and comorbidities in COPD (Table 1). It will also permit a study of the reliability of outcome measures including arterial stiffness, which has not yet been established in patients with COPD. In addition, ARCADE will include an assessment of indicators of aging, such as assessment of frailty and the accumulation of physiological deficits. 13,14 The aim of this publication was to describe the protocol and demographics of the patients with COPD and comparators recruited in the first year of the study as well as to evaluate the reproducibility of key outcome measures.
Aims of the ARCADE study.

CV: cardiovascular; COPD: chronic obstructive pulmonary disease.
Methods
Study design
The ARCADE is a prospective longitudinal observational study of patients with prior physician-diagnosed COPD, being undertaken in Cardiff, United Kingdom. Potential subjects are notified to researchers and invited to participate in the study. Those participants diagnosed with COPD, confirmed or refuted by determination of post-bronchodilator spirometry, and other suitability were recruited into the study (Figure 1). Participants are assessed at baseline and the assessments will be repeated at 2 and 5 years (Table 2). All subjects continue to receive their normal prescribed medications throughout the study and no medications are excluded. A between-day reproducibility reliability study of key outcome measures including aortic PWV, cardiac output (CO), cardiac index (CI) and stroke volume (SV), which have not been established in COPD, has been undertaken in a subset of patients. The study is conducted in accordance with the Declaration of Helsinki and Good Clinical Practice Guidelines and has been approved by the South East Wales Ethics Committee, part of the National Research Ethics Service (UK).

Flow chart of the first year of recruitment. *Excluded based on inclusion/exclusion criteria table 2.
Inclusion and exclusion criteria.
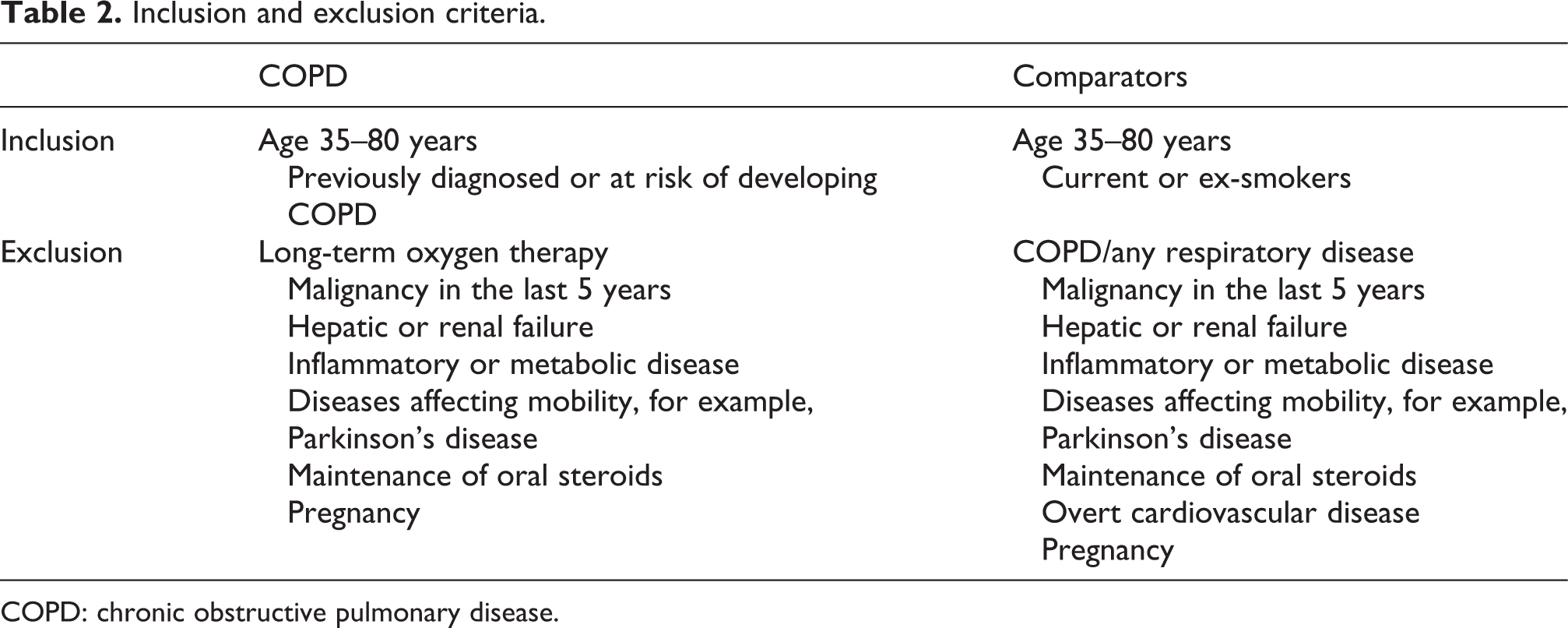
COPD: chronic obstructive pulmonary disease.
Subjects
As there has been no data regarding the annual change in PWV in COPD, the sample size was based on the annual increase of 0.25m/s in PWV reported in hypertensive patients. To detect a 25% difference in the rate of progression with 95% power at p = 0.01 level, it was estimated that 1500 patients would be required for the full study. The aim is to recruit clinically stable patients with a confirmed diagnosis of COPD with mild, moderate, severe or very severe airflow obstruction 15 and a comparator group of up to 300 current or ex-smokers free of COPD and other exclusion criteria (Table 1). Patients with other inflammatory disease or on long-term oxygen therapy were excluded to avoid the known CV complications and the possible effects on arterial wall and amplification of CV risk.
Recruitment sources include general practice databases, respiratory outpatient clinics, pulmonary rehabilitation and smoking cessation referrals, and previous participants in respiratory research at Cardiff University.
Outcome measures
All outcome measures will be repeated at 2 and 5 years post baseline in all available subjects (Table 2). Mortality data including cause of death will be collected from the National Office for Statistics and the NHS Information Service Center. The following methods are included in the longitudinal study: body composition, physical performance, hemodynamic, and metabolic data for the preliminary data analysis.
Methods
Anthropometry and pulmonary function
Height and weight were determined barefoot in lightweight indoor clothing. FFM and fat mass (FM) were measured by bioelectrical impedance (Tanita BC-418, MA). The FFM and body mass index (BMI) were expressed as a height square index, FFMI kg/m2 and BMI kg/m2, respectively. A stretch-resistant tape was used to measure the waist and hip circumference.
Postbronchodilator spirometry was performed after inhalation of salbutamol 200 μg (Vitalograph, UK). According to the American Thoracic Society/European Respiratory Society guidelines, the best of three blows within 5% of each other was recorded including FEV1, forced vital capacity (FVC), and their ratio (FEV1/FVC). 16
Physical performance
All subjects undertook the 6-minute walking distance (6MWD) postbronchodilator according to the guidelines. 17 Pre- and posttest resting heart rate and oxygen saturation were recorded by pulse oximetry with the subjects breathing air. The mean maximum handgrip strength (HGS) was measured using a hand dynamometer (Takei Scientific Instruments Co Ltd item 5401, grip-D, Tokyo, Japan) based on four determinations, two in each hand.
Questionnaires
Patients completed the COPD-specific St George’s Respiratory Questionnaire (SGRQ-c) 18 and COPD assessment test (CAT). 19 Patients were asked to report breathlessness using the the modified Medical Research Council (mMRC) scale, the number of exacerbations, defined as an acute worsening beyond the normal day-to-day respiratory symptoms, which necessitated a change in regular medication, in the last year. In addition, patients were asked to report their history of cigarette smoking.
CV measurements
Aortic PWV
CV assessments were undertaken in all subjects having abstained from caffeine, tobacco, and inhaled short-acting β2 agonists for at least 6 and 12 hours following long-acting β2 agonists or long-acting muscarinic antagonists (Table 3). Prior to the physical performance assessments and after resting for 10 minutes, peripheral systolic and diastolic blood pressure (BP) were determined in both seated and supine positions and the mean arterial pressure (MAP) calculated (OMRON Corporation, Kyoto, Japan). Applanation tonometry was used to measure pulse waveforms at the radial, carotid, and femoral sites using a high-fidelity micromanometer (Millar instruments, Houston, Texas, USA). Aortic PWV was calculated as the speed of the pulse wave traveling between the carotid and femoral pulses using the R wave of a simultaneous electrocardiogram (ECG) recording (SphygmoCor; AtCor Medical, Sydney, Australia). 20
ARCADE outcome measures in COPD and comparator group.

CUBA: Contact Ultrasound Bone Analyzer; 6MWD: 6-minute walking distance; HGS: handgrip strength; TUG: Timed Up and Go; SGRQ: St Georges Respiratory Questionnaire; CAT: COPD assessment test; CGA: Comprehensive geriatric assessment.
aDescribed and reported separately.
CO and SV
Non-Invasive Cardiac Output Monitoring (NICOMTM) (Cheetah Medical, Wilmington, DE) was used to measure the CO, SV, and CI by chest bioreactance. Four electrodes were placed on the thorax, mid-left and right clavicles, and mid-left and right-last rib. Data were automatically and continuously recorded using a computer data logger on a minute-by-minute basis. 21
Blood analysis
Venous blood was obtained for determination of lipids, glucose, insulin, glycosylated hemoglobin A1c (HbA1c), fibrinogen and high-sensitivity C-reactive protein (hs-CRP) by Cardiff and Vale University Hospital biochemistry laboratory according to the standard procedure. Blood was stored at −80°C for future analysis including deoxyribonucleic acid (DNA).
Reproducibility protocol
The between-day reproducibility was determined for aortic PWV, CO, SV, and CI by a single operator in 30 patients. The PWV was based on a comparison of the mean of double recordings on each day.
Statistical analysis
Analysis was undertaken using the statistical software package SPSS 18.0 (Chicago, Illinois, USA) with a significance level of p < 0.05. Data were checked for normality prior to analysis. Parametric data were presented as mean and standard deviation (SD) and compared by t test. Nonparametric data were expressed as median (range). Categorical data were analyzed using the chi-square test. For the reproducibility study, the mean differences between the readings were compared by paired t test. Intraclass correlation coefficients (ICCs) were calculated and Bland Altman plots generated to evaluate the limits of agreement within 2 SDs of the mean differences, thus expressing the expected variation in 95% of the cases. 22
Results
Demographics of the first-year recruitment
At the end of the first year of recruitment, 350 fully evaluable patients and 100 comparators were included in the baseline analysis. Although a large proportion of patients were approached from primary care COPD registers, approximately 50% were either unavailable or excluded prior to recruitment due to the failure to meet inclusion/exclusion criteria (Table 2).
In the patient group, the inhaled therapy comprised short-acting β2-agonist (n = 192), long-acting β2-agonist (n = 25), long-acting muscarinic antagonist (n = 204), and inhaled corticosteroid alone or in combination (n = 197). No comparator subject received inhaled therapy. Of the 350 patients, 125 reported CV disease including angina, myocardial infarct, or cerebrovascular accident. CV medication included angiotensin-converting enzyme inhibitors for 79 patients and 4 comparators, angiotensin receptor blockers for 34 patients and 1 comparator, Beta Blockers for 26 patients and 2 comparators, and calcium channel blockers for 75 patients and no comparators. In addition, 135 patients and 19 comparators had been prescribed statins for hypercholesterolemia. Bisphosphonates were prescribed for 53 patients and 5 comparators.
Patients and comparators were similar for gender, however, the patients were older (mean difference 95% CI 2.9 (1.2-4.7 p = 0.001)) and had more smoking pack-years than comparators. Patients had lower mean (SD) FEV1/FVC 0.52 (0.11), FEV1 predicted 56.3 (20%) and FVC 85.0 (20.9) and lower resting oxygen saturations (p < 0.001).
The severity of airflow obstruction in the patients was GOLD 1 (n = 40), GOLD 2 (n = 173), GOLD 3 (n = 109), and GOLD 4 (n = 28). According to the more recent combined COPD classification which includes risk of exacerbations and symptoms, we grouped patients using the CAT score and frequency of exacerbations as GOLD A (n = 22), GOLD B (n = 15), GOLD C (n = 74), and GOLD D (n = 239). 23 The mMRC breathlessness scale in patients was mMRC 0 (n = 43), mMRC 1 (n = 106), mMRC 2 (n = 70), mMRC 3 (n = 97), and mMRC 4 (n = 34). Of the patients, 127 reported less than two exacerbations per year and 223 reported two or more exacerbations per year.
Body composition and physical performance
Mean BMI and FFMI were similar in patients and comparators. However, HGS, 6MWD, and resting oxygen saturations were lower and the waist girth was greater in patients than in comparators (p < 0.05; Table 4).
Subject characteristics.a

6MWD: 6-minute walk distance; BMI: body mass index; FFMI: fat-free mass index; FEV1: forced expiratory volume in 1 second; FFM: fat-free mass; FVC: forced vital capacity; CAT: COPD assessment test; SGRQ-c: St George’s Respiratory Questionnaire; O2: oxygen.
aAll data mean (SD) unless otherwise indicated.
bMedian (range).
Hemodynamic and metabolic data
Aortic PWV, peripheral and central systolic BP, and pulse pressure and heart rate were greater in patients, while SV was less in the comparators (p < 0.05; Table 4). While central and peripheral diastolic and MAP were not different between the groups. Circulating hs-CRP and fibrinogen were greater, but the total cholesterol was lower in patients than in comparators (Table 5).
Hemodynamic and biochemical data in patients and comparators.a

BP: blood pressure; hsCRP: high-sensitivity C-reactive protein; PWV: pulse wave velocity.
aAll data mean (SD) unless otherwise indicated.
bGeometric mean.
Reproducibility
The between-day reproducibility interval was a median (range) 7 (6–8) days (Table 6). There was no difference in the repeated assessments for PWV, CO, CI, or SV and their ICCs were all greater than 0.936. Bland-Altman plots showed the mean differences were all close to 0, with no systematic bias in that the mean difference was not dependent on the underlying mean values (supplementary material). A total of five data points (for aortic PWV three data points and for CO two data points) fell outside the 95% CI but did not adversely affect the ICCs.
Demographics and reproducibility of PWV, CO, SV in patients with COPD.a

BP: blood pressure; FEV1: forced expiratory volume in 1 second; FVC: forced vital capacity; ICC: intraclass correlation coefficient; PWV: pulse wave velocity.
aData presented as mean (SD).
Discussion
Summary of the main findings
The ARCADE is the first prospective longitudinal study designed to determine the potential role of CV risk factors and their relationship to CV outcomes including death. This can be achieved using a patient group representative of the greater COPD population in terms of the spectrum of severity of the airway disease, exacerbation frequency, physical impairment, and disability. The first year of recruitment has yielded a population across the range of disease severities GOLD 1–4 and the combined COPD assessment, which includes symptoms and exacerbations, GOLD A–D. 23 In this stratification, more patients were in the severe disease category, GOLD D, due to frequent exacerbations, than in those with severe airflow obstruction, GOLD 4.
In all cohort studies, the issue of subjects not included in the study needs to be considered. It was to address this and the representative potential of our patient group (the first year recruitment cohort) that we undertook this review. The main reasons for not entering the study included unavailability of subjects or participation declined by subjects, which may reflect aspects of the impact of COPD on the lifestyle of patients, while only 19.7% were excluded at this stage. A further 27 (7.2%) were excluded at the confirmation of the presence of airflow obstruction.
The hallmark of COPD is poorly reversible airflow obstruction, which is expressed as the FEV1, predicts mortality but is a poorer predictor of symptoms or functional outcomes. 24 This limitation of the utility of pulmonary function and the multiple extra-pulmonary associations, which contribute to morbidity and mortality and the cost of care, emphasizes the need for alternative assessments, such as inflammatory biomarkers, symptoms, physical impairment, and health status to guide future interventions. Our year 1 patient cohort demonstrated, as would be expected, impaired physical function with a reduced 6MWD and HGS, compared to comparators. Such reductions in physical function were supported by the findings of the SGRQ-c and CAT scores, indicating a reduced health-related quality of life and spectrum of symptomatic impact. Our patients did not show marked differences in mean body composition compared with the comparator group.
The results at the end of first year of recruitment demonstrated that the primary outcome measure of CV risk, aortic PWV, was greater in the patients than in the comparators, confirming previous smaller cross-sectional studies. 9 Systolic BP was greater in the patients, while both peripheral and central MAP were similar in patients and comparator subjects, indicating increased central vascular stiffness, increased pulse pressure, and premature vascular aging in the patients. Increased pulse pressure alters the cyclical dynamics of the arterial wall connective tissues, promoting vascular remodeling and arterial stiffness. 25 Thus, arterial stiffness may be both a marker for and a cause of CV disease. In natural aging, central elastic arteries stiffen due to progressive collagen cross-linkage, reduced elastic fiber content, calcification, and increased muscle tone because of endothelial cell senescence induced by oxidative stress. 26 In older individuals, PWV reflects the physical functioning and functional limitation components of frailty, independent of age, but physical disability may precede in COPD. 27 Thus, the increased aortic PWV in COPD could be interpreted as premature vascular aging and probably indicates subclinical CV disease. 9,12 Other risk factors including the biomarkers of systemic inflammation, hsCRP, and fibrinogen were greater in the patient group, however, there was no difference in glucose, and cholesterol was lower in patients than in comparators, which is likely due to statin use. Longitudinal follow-up of such risk factors coupled with the ability to review causes of death will ensure the ability of the ARCADE study to identify predictive CV risk factors and other aspects of COPD that may predict CV outcomes. CO and CI were similar, though SV was lower in patients than in comparators, which may be a consequence of altered ventilatory dynamics or cardiac dysfunction. 28 The results to date may be criticized for differences in smoking status and overt CV disease between the groups. This is common in research studies and represents the difficulty in identifying healthy smoker comparators. The ARCADE study was not designed as a control-matched study but to describe a representative COPD group and a comparator group, which will allow the study to determine the differences in the accrual rate of CV disease between groups.
The reproducibility of outcome measures is fundamental to any longitudinal study, and preliminary analysis from the year 1 cohort of the ARCADE study has demonstrated acceptable reproducibility for noninvasive measures of PWV, CO, CI, and SV. The subset of patients included in the reproducibility study were representative of the larger group studied to date with similar lung function, BMI, and hemodynamic measures. We estimated the between-day reproducibility using the ICC to calculate the consistency based on the contribution of patient variance to the total variance. 22 This approach is limited in heterogeneous samples, and, therefore, Bland-Altman plots were constructed and confirmed the consistency of the outcome measures and their suitability for the ARCADE study.
Strengths and limitations
The ARCADE builds on previous longitudinal studies with the inclusion of CV risk factors and their reliability. These were absent from Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE), a study which highlighted the importance of phenotypes such as frequent exacerbators. 29 The recent understanding of the number and impact of comorbidities on morbidity and mortality suggests possible other phenotypic subgroups. Examples of other probable clinical phenotypes include marked alterations in body composition, which is a predictor of increased mortality and morbidity. 6 There is an association between an accelerated decline in FEV1, the presence of type 2 diabetes mellitus, hypertension, and CV disease with an increased risk of death in COPD. 7 In order to minimize the effect of confounders, we excluded other inflammatory states, cancer, and metabolic disorders. The present data are limited by its cross-sectional nature; however, the planned follow-up assessment may allow the delineation of comorbidity-related phenotypes and their development. Although PWV was slightly less than that reported by Sabit et al., 9 the SDs and BP were similar, and both were significantly greater than comparators; therefore, this was thought not to risk the future longitudinal analysis which will provide further informative results. It will provide a potentially valuable insight into COPD and may indicate important areas for therapeutic intervention.
Conclusions
ARCADE will extend knowledge of CV risk and outcomes in patients with COPD and close an important gap in the highly successful ECLIPSE study, which demonstrated the value of a medium term, longitudinal observational cohort study in COPD.
Footnotes
Clinical trials
This study is registered at Clinical Trials. Govt. with the identification number: NCT01656421.
Conflict of interest
The authors declared no conflicts of interest.
Funding
This work was supported by GlaxoSmithKline [grant number SCO115218].
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.