
Abstract
The aim of the present study is to conduct a social media content analysis of chronic obstructive pulmonary disease (COPD) patient education videos on YouTube. A systematic search protocol was used to locate 223 videos. Two independent coders evaluated each video to determine topics covered, media source(s) of posted videos, information quality as measured by HONcode guidelines for posting trustworthy health information on the Internet, and viewer exposure/engagement metrics. Over half the videos (n = 113, 50.7%) included information on medication management, with far fewer videos on smoking cessation (n = 40, 17.9%). Most videos were posted by a health agency or organization (n = 128, 57.4%), and the majority of videos were rated as high quality (n = 154, 69.1%). HONcode adherence differed by media source (Fisher’s exact test = 20.52, p = 0.01), however with user-generated content receiving the lowest quality scores. Overall level of user engagement as measured by number of “likes,” “favorites,” “dislikes,” and user comments was low (median range = 0–3, interquartile range = 0–16) across all sources of media. Study findings suggest that COPD education via YouTube has the potential to reach and inform patients; however, existing video content and quality varies significantly. Future interventions should help direct individuals with COPD to engage with high-quality patient education videos on YouTube that are posted by reputable health organizations and qualified medical professionals. Patients should be educated to avoid and/or critically view low-quality videos posted by individual YouTube users who are not health professionals.
Introduction
Chronic obstructive pulmonary disease (COPD) is now the third leading cause of death in the United States, with more than 12 million people diagnosed and another 12 million likely to have the disease unknowingly. 1 Individuals with COPD are challenging to treat effectively, often because they require complex treatment regimens prescribed by different clinicians. Health information provided to COPD patients during medical consultations has been cited as poor and confusing. 2 Researchers have documented the need for better communication strategies to help COPD patients learn how to cope with exacerbations and avoid costly hospitalizations and emergency room visits. 3 –6 Patient education is an approach to teach individuals about daily behaviors and skills to manage and control physical, emotional, and social functioning in the context of their lives. With the increase in consumption of online health care information among adults with chronic disease, 7,8 there are now opportunities to use applied information and communication technologies on the Internet to increase access to patient education.
YouTube™ (www.youtube.com) is one of the most popular social media Web sites on the Internet and is often used to share patient education materials with large numbers of individuals with chronic disease. 9,10 YouTube is a free online video streaming service that allows users to view, upload, and post ratings/comments on posted videos. Globally, YouTube is the third most frequently visited Web site on the Internet, behind Google and Facebook. 11 Over 800 million users watch over 4 billion hours of YouTube videos each month, and approximately 100 million people take a social action on YouTube every week by liking, sharing, or commenting on videos that they watch. 12 Social actions are tracked using exposure and engagement metrics that are publically accessible under the “Video Statistics” function on YouTube. Health-related topics on YouTube range from general health education, to the latest medical treatments, to homemade videos produced and uploaded by individuals. 13 Any registered user may post videos to YouTube, which often leads to videos becoming available that may contain scientific misinformation on health-related matters. 14
Research on YouTube and its public health implications is still in its infancy. 15 The quality of patient education videos on YouTube is unclear, calling into question how best to incorporate YouTube within health promotion interventions. 13,16 –21 To our knowledge, no prior studies have examined the content, quality, and viewer exposure and engagement of COPD patient education videos on YouTube. Therefore, we conducted research to determine the extent to which these videos were posted, viewed, rated, and commented on by YouTube users.
Research questions
Which topics are covered in YouTube COPD patient education videos? What are the primary media sources of YouTube COPD patient education videos? What is the quality of YouTube COPD patient education videos from posted by different media sources? What are the exposure and engagement metrics of YouTube COPD patient education videos by media source? What is the relationship between the exposure and engagement statistics attached to YouTube COPD patient education videos?
Methods
A COPD patient education video was defined as any posted video to YouTube providing information on self-management strategies that patients could undertake themselves. On 3 August 2012, we searched YouTube for English language content using the following search terms: Chronic Obstructive Pulmonary Disease, COPD, COPD management, and COPD self-management. To meet our inclusion criteria, video content needed to be audible and related to COPD patient education on self-management strategies. Non-English videos without sound were excluded from the analysis. Studies of users behavior on Internet search engines indicate that over 90% of users click on results within the first three pages of search results, 22 yet 79% of users will search through multiple pages if they do not find what they want on page one. 23 Therefore, we screened the first seven pages of results for each search term, assuming that users would be unlikely to scan beyond these pages.
Video searches were conducted independently by two research team members who were trained to follow the same standards for locating and evaluating videos. Coder training involved independently watching and coding 10 representative videos not included in the final analysis. Blind coding was used so that coders would understand the study’s general goals, without having advanced knowledge of specific research questions, which may have biased codes. Each coder saved videos meeting inclusion criteria into four separate YouTube Favorites playlists corresponding to each search term. Eligible videos were then selected from each coder’s playlists. The two coders saved a total of 339 videos. Duplicate videos (n = 63) from these saved lists were eliminated and videos with content that did not relate to this study’s purpose (n = 32) were also removed. Disagreements between coders on whether saved videos met inclusion criteria (n = 5) were resolved by consensus or by adjudication from a third member of the research team with experience studying COPD self-management. Video clips that were part of a multi-segment video were reduced down to the most recent upload (n = 5). Videos not in English (n = 1) or without sound (n = 15) were also excluded. A total of 223 unique YouTube videos were saved for analysis.
The following data were extracted from each video in the final sample: Title of the video, uniform resource locator, date of upload, duration of video (in seconds), source of video upload (health agency or organization such as a medical center, health/medical foundation, or professional organization; medical professional; news program; television commercial; user-generated content (UGC); or other), patient education topic on COPD self-management (e.g. smoking cessation; breathing retraining; energy conservation/stress management; performing activities of daily living (ADLs); medication management (e.g. self-management of exacerbations with rescue inhalers); infection control; nutrition; and physical activity), and number of HONcode principles followed. 24
HONcode is the oldest and most used ethical and trustworthy code for presenting medical and health-related information on the Internet. Research has indicated that Web sites following HONcode principles provide health care consumers with quality health information. 25,26 We used eight adapted HONcode principles to evaluate the quality of videos (Table 1). Each rater indicated whether each principle was adhered to in each video (1 = yes; 0 = no), and we computed a summated adherence score to quantify the total number of HONcode principles followed.
Eight adapted HONcode principles and frequency of adherence in reviewed videos (total n = 223).

COPD: chronic obstructive pulmonary disease; HTML: hypertext markup language.
aCriteria did not apply to all videos. Videos believed to not have financial advertiser/sponsorship support were scored as not applicable (N/A) and awarded one point for meeting the criteria.
Each coder also reported video views (i.e. exposure) by recording overall video view counts and the extent to which viewers left ratings and feedback (i.e. engagement). For each video, engagement was measured by recording the number of “favorites,” “likes,” “dislikes,” and presence of viewer-posted comments. To determine whether the majority of video comments (≥70%) affixed to each video were positive, neutral, or negative in tone, each coder recorded an ordinal rating of the slant of comments (positive = 1, neutral = 0, negative = −1). Coders reviewed examples of each type of comment during coder training to determine how viewer comments were to be evaluated. All comments were screened for relevance, and irrelevant comments (e.g. comments with inappropriate language) were removed.
Using Statistical Package for Social Sciences Version 21 software (SPSS Inc., Chicago, Illinois, USA), basic frequency and descriptive statistics were calculated to describe video characteristics such as media source, topics covered, number of views, and number of days posted to YouTube. Fisher’s exact test was used to test for differences in the number of videos adhering to HONcode principles by media source. Level of HONcode adherence was determined using the following adherence scheme: 0–2 principles (low); 3–5 principles (medium); and 6–8 principles (high). Central tendency engagement statistics were computed to determine the median number of days posted to YouTube, favorites, likes, dislikes, and comments by media source. One-way nonparametric Kruskal–Wallis test determined whether differences existed in the median number of days videos had been posted to YouTube and median number of video views by media source. Pearson’s correlation statistics determined relationships between viewer exposure and engagement metrics. The value of p < 0.05 was considered statistically significant.
Results
Data reliability
To determine agreement between coders, a subsample of 50 videos were analyzed to determine the κ statistic or coefficient of agreement. 27 A subsample size of 50 meets guidelines for conducting reliability analyses in media content analyses (i.e. at least 50 cases or 10 to 20% of the sample). 28,29 The coefficient of agreement (κ) between coders for identifying video source was 0.78, slant of comments was 0.70, and mean κ for identifying patient education topics was 0.75 (SD = 0.09; Table 2). The values of κ were at or near the recommended cutoff value of 0.70. 30 Interrater reliability of the number of HONcode principles followed per video was assessed using Lin’s concordance correlation coefficient (ρ c), 31 which measures agreement between two observers when variables are continuously scaled. 32 The reliability of HONcode principle ratings was satisfactory, ρ c = 0.771.
Intercoder reliability scores for identifying COPD topics in subsample of reviewed videos (n = 50).
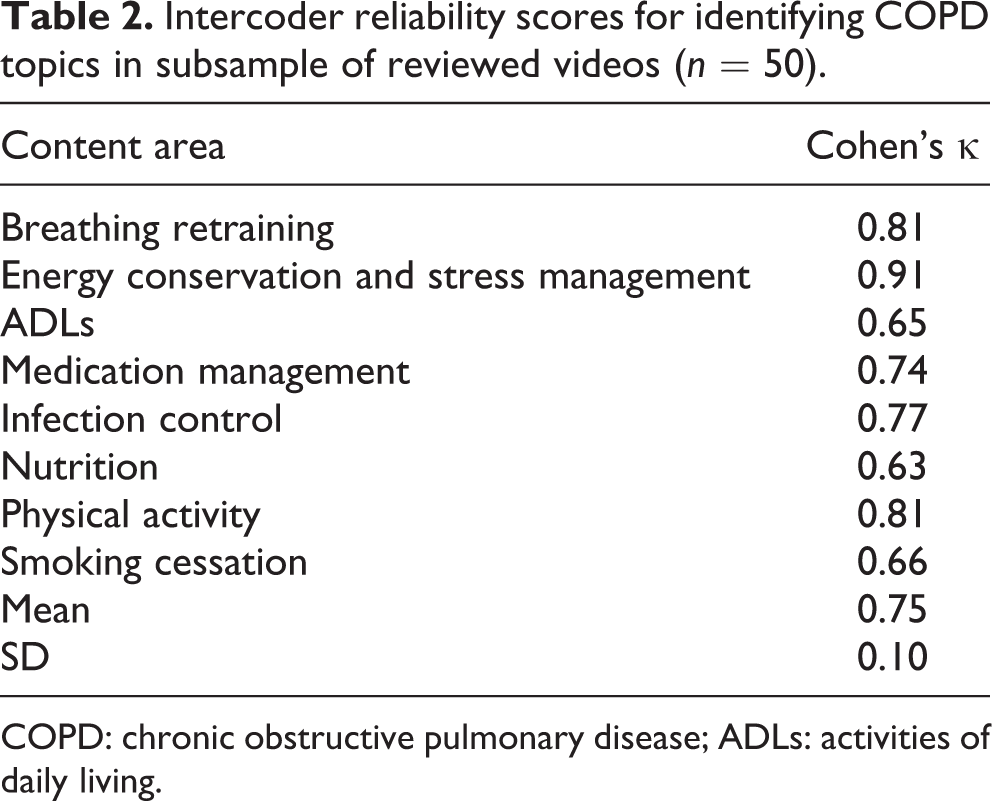
COPD: chronic obstructive pulmonary disease; ADLs: activities of daily living.
Research Question #1: Which topics are covered in YouTube COPD patient education videos?
Approximately half of the videos covered medication management (113 of 223 videos, 50.7%). Other content areas were addressed far less often: smoking cessation (n = 40; 17.9%); physical activity (n = 39; 17.5%); performing ADLs (n = 37; 16.6%); inflection control (n = 26; 11.7%); breathing retraining (n = 22; 9.8%); nutrition (n = 11; 4.9%); and energy conservation/stress management (n = 10; 4.4%; Figure 1).

Topics featured in reviewed YouTube videos (n = 223). Total numbers (n) combined equal more than the sample because videos could contain content from more than one topic category.
Research Question #2: What are the primary media sources of YouTube COPD patient education videos?
The majority of videos were posted by a health agency or organization (128 videos, 57.4%). Videos posted by medical professionals (25 videos, 11.2%), as UGC (19 videos, 8.5%), from news programs (11 videos, 4.9%) and television commercials (7 videos, 3.1%) were identified far less often. Videos assigned to the “other” category (33 videos, 14.8%) primarily contained messages from more than one media source that could not be reasonably classified under one single category (e.g. medical professional representing a sponsoring health organization on a news program).These videos included news reports with patients describing the use of government health services to care for COPD using vignettes from medical professionals.
Research Question #3: What is the quality of YouTube COPD patient education videos posted by different media sources?
The number of videos in compliance with each HONcode principle is reported in Table 1. A majority of videos (n = 182, 82%) met criteria #1, which required medical and health advice to come from a qualified health professional, unless clearly stated otherwise. In all, 79% (n = 179) of sampled videos met criteria #2, providing patient education on COPD self-management without the intention to replace the patient–physician relationship. Most videos also maintained the right to confidentiality and respect of patients featured (n = 146, 65%) and contained references to source data on information presented (n = 142, 64%). Additional contact information and/or a Web site link for further information was provided by 61% of videos, while 45% (n = 110) clearly identified funders and contributors of information presented in the video or within video descriptions. The two HONcode criteria with the fewest videos in compliance were criteria #5 (n = 62, 28%), requiring claims to be supported by evidence through references or hypertext markup language (HTML) links, and criteria #8 (n = 30, 13%), that only applied to videos supported by funding from advertisers.
Table 3 reports the number and proportion of YouTube videos posted from each media source according to the level of HONcode adherence (low, medium, and high). Due to low expected counts of less than 5 in 10 cells (55.6% of total cells), Fisher’s exact test was conducted to compare the number of videos in each HONcode category by media source. Results indicated that level of HONcode adherence differed significantly by media source (Fisher’s exact test = 20.52, p = 0.01). While the majority of videos across all media categories were rated as high quality (n = 154, 69.1%), 17% were judged to be low quality and 13.9% were judged to be medium quality. More than two-thirds of videos from health agencies and organizations were judged to be of high quality (86 of 128 videos, 67.2%), with the largest proportion of low-quality videos in the UGC category (7 of 19 videos, 36.8%).The largest proportions of low- (71.1%), medium- (56.7%), and high- (67.2%) quality HONcode ratings were for videos posted by health agencies or organizations, demonstrating variable quality in COPD patient education videos produced by organizations as well as by individuals.
HONcode adherence level in YouTube COPD patient education videos by media source.a
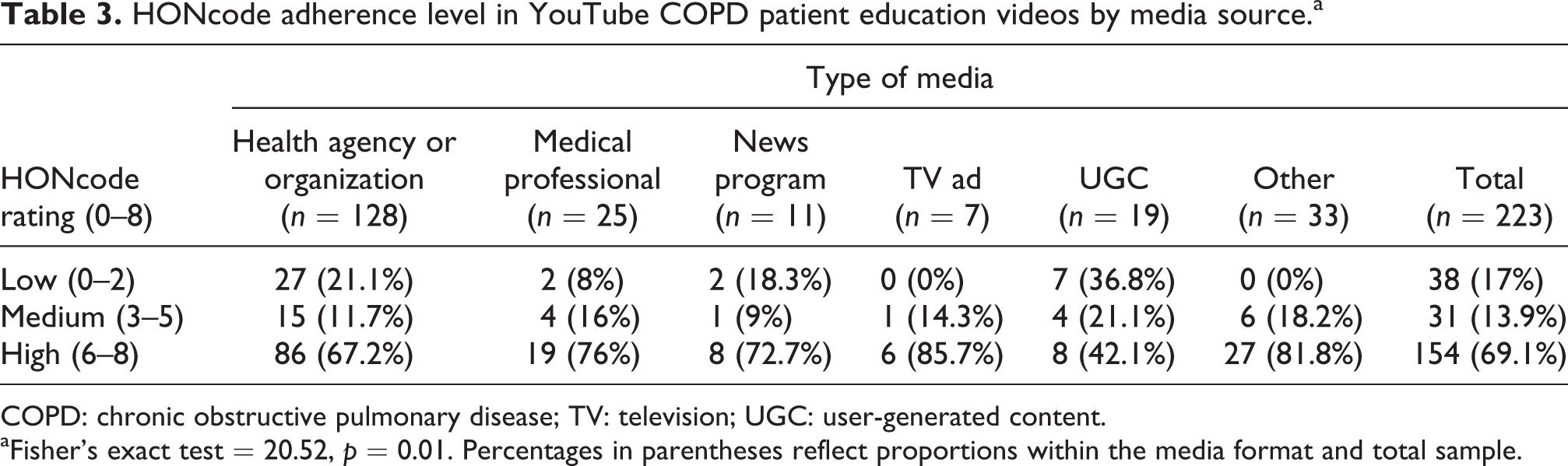
COPD: chronic obstructive pulmonary disease; TV: television; UGC: user-generated content.
aFisher’s exact test = 20.52, p = 0.01. Percentages in parentheses reflect proportions within the media format and total sample.
Research Question #4: What are the exposure and engagement metrics of YouTube COPD patient education videos by media source?
Table 4 presents descriptive exposure and engagement metrics by media source. An exploratory data analysis revealed that data on the number of days posted to YouTube and number of views were not normally distributed (Shapiro–Wilk statistics (degrees of freedom = 223) = 0.24–0.95, p = 0.001); therefore, we report nonparametric statistics including median values. Results from one-way Kruskal–Wallis tests indicated no statistically significant differences in the number of days videos were posted to YouTube, χ 2(5, n = 223) = 5.58, p = 0.349), or in the number of video views, χ 2(5, n = 223) = 1.887, p = 0.865), across all media sources. Videos posted by news sources were available for the longest amount of time (median (mdn) = 1176 days, interquartile range (IQR) = 841–1512 days), receiving the largest number of views (mdn = 3126 views, IQR = 616–6771 views). Videos posted as television advertisements had the second highest viewership (mdn = 1927 views, IQR = 47–2899 views). Videos posted by medical professionals were available for the least amount of time (mdn = 646 days, IQR = 205–1189 days), receiving the least number of views (mdn = 745 views, IQR = 82.5–3067.5 views).
Descriptive exposure and engagement metrics by media source.
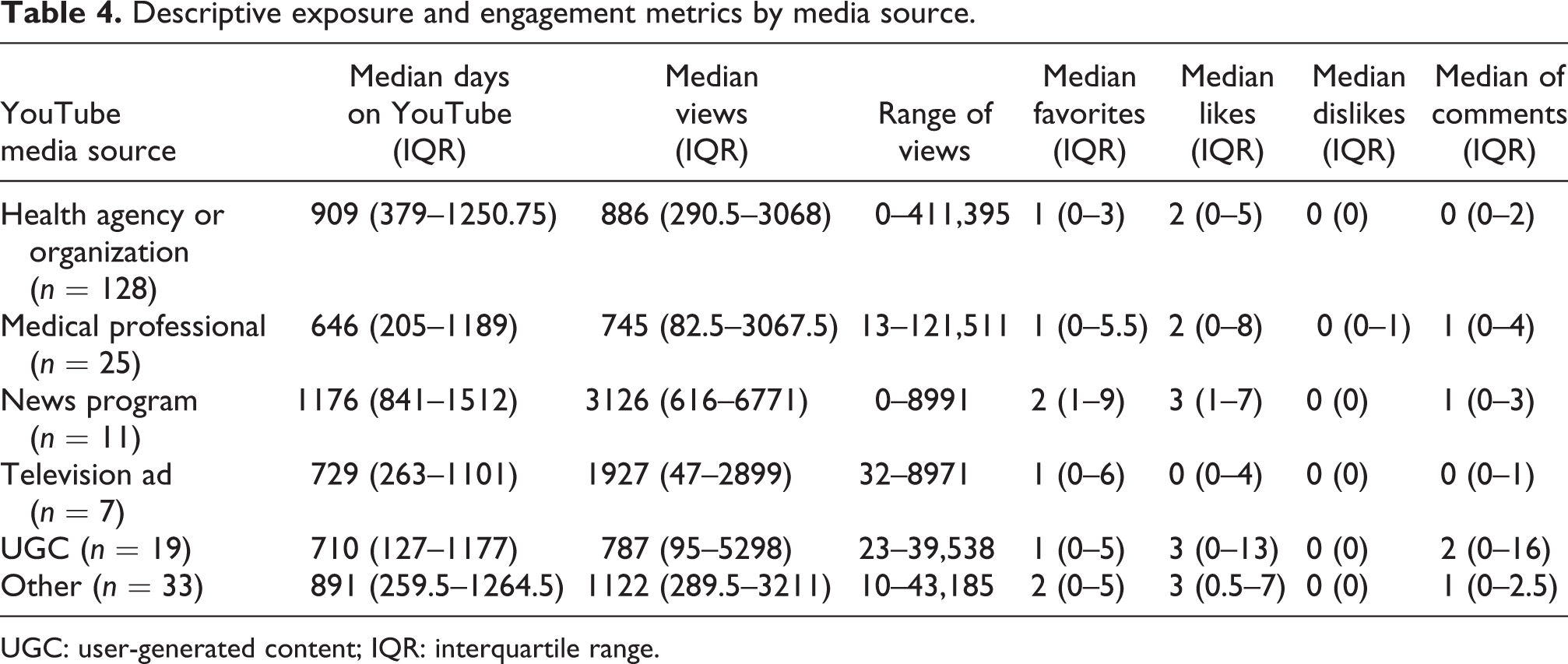
UGC: user-generated content; IQR: interquartile range.
Of the reviewed videos, 139 (58.7%) were marked as a favorite,145 videos (65%) were liked by at least one viewer, and 101 videos (45.2%) had at least one viewer comment. The majority of videos contained comments that were judged to be neutral in tone (n = 144; 62.1%); however, over 30% of videos had comments rated as positive (n = 71). While the number of comments per video ranged from 0 to 170, the median number of comments per video was 0 (IQR = 0–2). Overall, there was very little video viewer engagement across each media source regardless of length of time videos were uploaded to YouTube or the number of times videos had been viewed. The median number of likes, favorites, and dislikes were all <5 in all media categories (Table 4). Only one media category, UGC, had, on average, more than one comment posted by viewers (mdn = 2, IQR = 0–16).
Research Question #5: What is the relationship between the exposure and engagement statistics attached to YouTube COPD patient education videos?
As would be expected, there were positive relationships between the total number of views and number of days videos were available to view on YouTube (r = 0.31, p < 0.01), number of likes (r = 0.80, p < 0.01), number of favorites (r = 0.66, p < 0.01), and number of viewer-posted comments (r = 0.73; p < 0.01). Number of overall views was also positively associated with the slant of posted comments, with videos that were viewed more often receiving more positive comments, Spearman’s ρ = 0.43, p < 0.01.
Discussion
Topic and media source
This exploratory study illustrated that COPD patient education videos are available on YouTube; however, the number of videos on COPD is underrepresented compared with other leading causes of death. A general YouTube search query of COPD may yield users with <50,000 total results, which is far less than “heart disease” (approximately 3,000,000 hits) or “diabetes” (approximately 1,000,000 hits). 33 –35 The most common COPD patient education topic on YouTube was on medication use. Given the high prevalence of inhaler misuse in COPD, 36 there is great need for low-literate educational materials that show patients (especially those with poor vision) how to appropriately use different types of inhalers such as rescue, long-lasting, and steroid-metered dose inhalers. 37 Planned inhaler training programs in COPD have decreased attack frequency and exacerbations, while improving health-related quality of life. 38 Videos to support COPD patient education related to proper medication use and breathing techniques have been evaluated as acceptable and effective in previous studies. 39,40 Of the reviewed videos in this study, we noted very few posted by pharmaceutical companies (less than five videos). The majority of videos were posted by reputable health agencies and organizations. An illustrative example on YouTube is the Channel, WipeCOPD (Web-based Interactive Professional Education in Chronic Obstructive Pulmonary Disease), which offers a wide variety of instructional videos on how to use different inhaler devices. These types of high-quality, low-literate videos on effective medication use should be made available to patients with COPD, their informal caregivers, and clinicians.
Videos on topics other than medication management were lacking in the sample. For example, the number of YouTube videos on smoking cessation (n = 40) was surprisingly low given that smoking causes the progression of COPD and is a vitally important topic to include in COPD self-management programs. 5 Over 50% of videos were posted by formal health agencies and organizations, such as medical centers (e.g. University of Nebraska Medical Center, Floyd Medical Center), foundations (e.g. COPD Foundation, British Lung Foundation), and professional organizations (e.g. American College of Physicians, Annals of Internal Medicine). It will be important that these types of leading health and medical organizations promote smoking cessation in COPD more often on their YouTube Channels.
Quality
Our study confirms the findings of Garbarron et al. 16 that quality indicators used to develop patient education videos on YouTube are inconsistently adopted. While we found that the majority of YouTube COPD patient education videos (almost 70%) showed high adherence to HONcode principles for presenting quality and trustworthy health information on the Internet, it was interesting to note that nearly 20% of posted videos were rated as low quality. This finding underscores the importance of operationalizing quality indicators for patient education on YouTube, even among health agencies and organizations where video quality was shown to variable in this study.
Patients with COPD should be directed to videos containing high-quality medical advice that is posted to YouTube channels operated and updated by clearly identified health professionals and/or reputable health-related organizations. In this study, most of the sampled videos provided medical and health advice from qualified health professionals and the video clearly indicated that qualified professionals were not involved with producing the video. More COPD patient education videos on YouTube should promote peer-reviewed content that describes evidence on the potential benefits and harms of available treatments and intervention strategies. 16 Of the videos examined in this study, very few included evidence through references to support claims on benefits, skills/behaviors, interventions, treatments, and/or products discussed. Posted videos should contain source citations and include external HTML links whenever possible to help patients locate and verify the source(s) of health information presented in videos. Fewer than half of sampled videos in this study informed viewers of sources of funding for video production. Sources of funding for video production and potential conflicts of interest should be made transparent to viewers, so that advertising and educational messages are easily discernable. 41 In this study, UGC videos were judged to have the lowest quality, likely because individual users have limited technical expertise that limits their ability to produce high-quality educational content. UGC availability on YouTube increases the potential for disseminating inaccurate health information to users searching for COPD patient education. Patients should be warned to limit exposure to such content to inform their medical decision making.
Exposure and engagement
Not surprisingly, COPD patient education videos receiving more exposure also received greater levels of viewer engagement. However, the levels of viewer engagement in COPD patient education videos on YouTube were notably low overall. Using the power of YouTube to develop disease-specific video resource centers to improve communication and understanding in chronic disease management may provide patients with valuable resources for patient education. 42 –45 Online patient education programs with minimal supervision, including open-access video portals complemented by support plans for living a healthy lifestyle (e.g. smoking cessation and physical activity), can be provided to patients at a low cost with potential for high returns. Future studies should investigate how to more effectively develop and promote social media-based resources to engage patients in the chronic disease self-management process. Interventions such as these are likely to improve comprehensive COPD patient education programs.
One potentially valuable aspect of using social media for COPD patient education is the ability to help people who would otherwise be hard to reach and engage. People with severe COPD are often isolated by their breathlessness. 46 –48 Online health communication forums centered around social objects like patient education videos could facilitate social networking and peer support among hard-to-reach patients with COPD. In this study, the largest numbers of comments were affixed to YouTube videos that were posted by individual users (i.e. UGC), which received the lowest quality ratings. The largely unregulated YouTube video sharing environment leaves patients vulnerable to inaccurate or misleading health information that may not be evidence based or peer reviewed by health care professionals. Individuals with COPD who may search for patient education on YouTube should be cautioned to interpret UGC messages with extreme caution and skepticism. Because of the potential for misinformation in UGC videos on YouTube, it is recommended that potentially harmful COPD patient education videos on YouTube be flagged by watchdog groups with comments warning potential viewers about the risks of harmful health information. 49 All media sources should develop and enforce policies that adhere to best practice standards for creating, communicating, and delivering quality patient education content. 50
Limitations
Although our search strategy was extensive, we may have missed videos that were not properly tagged with matching search terms. The proprietary algorithm used by YouTube to determine which content (e.g. title, description, and metatags) and engagement (e.g. views, ratings, embeds, and social shares) factors influence search queries is unknown, but likely had an impact on the number of engagement metrics reported in this study. Videos that have been uploaded to YouTube since the date of our search may currently be available but not included in our study. In addition, some videos that were retrieved in our study may now be deleted since the time of our analysis. There was also potential for videos to be judged as quality and trustworthy based on compliance with HONcode principles, yet still contain biased or inaccurate information. While we attempted to avoid this threat by training raters on how to apply HONcode principles uniformly, our adapted principles did not comprehensively assess the accuracy of clinical information included in videos. This type of assessment would require coders with sufficient experience in pulmonary medicine and/or rehabilitation, which was not feasible given the limited resources available for this exploratory study.
Additionally, more longitudinal and field-based studies on how patients are using YouTube for COPD patient education are needed. These studies can consider demographic data of viewers and what devices (i.e. desktop computer, mobile smartphone, or tablet computer) are being used to access videos on COPD patient education over time. The present analysis also may not necessarily reflect how YouTube videos are perceived by individuals with COPD. While we were able to determine audience responses to videos to a certain extent (using public access YouTube metrics), valid patient self-reports of responses to YouTube videos could not be ascertained from this data. Additional research should address how and why individuals with COPD and their informal caregivers use social media for COPD patient education. To increase relevance to clinical practice, future studies should also consider whether patients who view YouTube COPD patient education videos show greater improvements in outcomes such as patient activation and satisfaction.
Conclusion
The lack of public knowledge about COPD has been highlighted in the literature. 51 –53 YouTube and other online video resources may make an important contribution to promoting public health awareness regarding how patients can cope with and self-manage COPD. Findings from this study indicate that YouTube may represent a viable social media channel for translating and disseminating COPD patient education on topics such as medication management; however, more needs should be analyzed to motivate those with COPD to engage video content on other important topics such as smoking cessation. Researchers and practitioners in pulmonary medicine and rehabilitation should consider using and promoting high-quality YouTube videos posted by reputable health organizations and qualified medical professionals to augment patient–provider communication and improve overall COPD patient education. Before doing so, however, there is need for a greater understanding of the costs and benefits associated with using this type of social media for patient education in chronic diseases like COPD. 54 Caution should be applied when viewing and responding to low-quality videos, particularly those posted by individual YouTube users who are not health professionals. The current study highlights the need to conduct additional research to identify quality indicators for COPD patient education on YouTube, which is likely to improve its utility as a COPD patient education resource.
Footnotes
Conflict of interest
The authors have no consulting and/or personal relationships with other people or organizations that influenced this work. The project was conducted by authors listed on the title page.
Funding
This work was supported by the NIH (NCATS) CTSA awards to the University of Florida UL1TR000064 and KL2TR000065.